AAOS Sports Medicine MCQs (Set 3): Knee & Shoulder Ligament Trauma | OITE & ABOS Review

Key Takeaway
This high-yield Sports Medicine MCQ set (Set 3) for AAOS/ABOS exams covers critical topics in knee and shoulder pathology. Questions delve into the diagnosis, imaging, and management of ACL tears, meniscal injuries, shoulder instability, and rotator cuff pathology, aiding comprehensive board preparation.
AAOS Sports Medicine MCQs (Set 3): Knee & Shoulder Ligament Trauma | OITE & ABOS Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
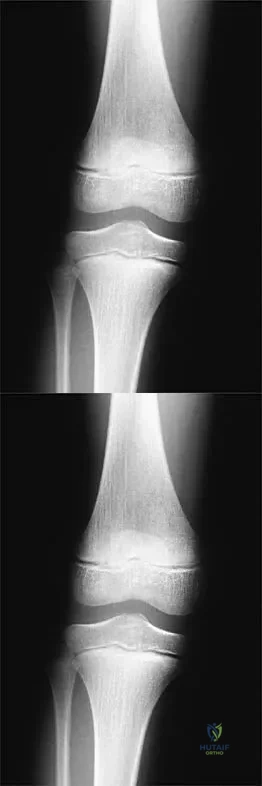
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of
Explanation
Question 2
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
Question 3
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Question 4
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Question 5
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Question 6
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Question 7
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
Question 8
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Question 9
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
Question 10
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Question 11
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
Question 12
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Question 13
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
Question 14
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
Question 15
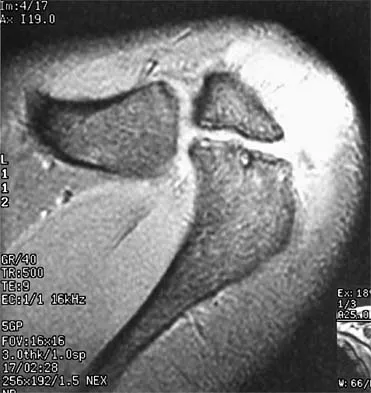
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
Question 16
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
Question 17
A cortisone injection in the subacromial space will most likely result in
Explanation
Question 18
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
Question 19
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45 degrees of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25 degrees of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
Question 20
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
Question 21
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Question 22
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
Question 23
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
Explanation
Question 24
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
Question 25
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
Question 26
A 25-year-old rugby player sustains a direct blow to the anteromedial aspect of his knee. Examination reveals increased external rotation of the tibia at 30 degrees of knee flexion, but symmetric external rotation at 90 degrees compared to the contralateral side. Which structure is the primary deficient restraint responsible for this examination finding?
Explanation
Question 27
A 22-year-old competitive rugby player presents with recurrent anterior shoulder dislocations. CT imaging demonstrates a 25% anterior glenoid bone loss and a deep, engaging Hill-Sachs lesion. What is the most appropriate surgical management?
Explanation
Question 28
A 16-year-old elite female soccer player sustains an acute ACL tear. She is considering graft options for reconstruction. Compared to hamstring autograft, bone-patellar tendon-bone (BTB) autograft has been consistently associated with which of the following outcomes?
Explanation
Question 29
A 25-year-old rugby player presents with a twisting knee injury. On examination, the dial test demonstrates 15 degrees of increased external rotation compared to the contralateral normal knee at 30 degrees of knee flexion, but symmetrical external rotation at 90 degrees of flexion. Which structure is most likely injured?
Explanation
Question 30
A 34-year-old male is brought to the emergency department after a motorcycle accident. He has a visibly deformed knee that spontaneously reduces. Examination reveals a gross multiligamentous knee injury. His pedal pulses are palpable, but an ankle-brachial index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 31
A 22-year-old collegiate linebacker presents with recurrent anterior shoulder instability. Preoperative CT imaging reveals a 28% anterior glenoid bone loss and an engaging Hill-Sachs lesion. Which of the following is the most appropriate surgical management?
Explanation
Question 32
A 19-year-old male presents to the trauma bay after a rugby tackle. He complains of severe medial clavicle pain, dysphagia, and a choking sensation. Clinical examination demonstrates a palpable depression at the medial end of the clavicle. What is the most appropriate definitive management?
Explanation
Question 33
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon uses fluoroscopy to identify the femoral attachment site. According to Schöttle's method, where is the anatomic femoral origin of the MPFL located?
Explanation
Question 34
A 24-year-old athlete undergoes an anterior cruciate ligament (ACL) reconstruction. Postoperatively, he demonstrates an absent Lachman test but a persistently positive pivot shift test. What is the most likely technical error made during the procedure?
Explanation
Question 35
A 21-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 25% anterior glenoid bone loss. Which of the following is the most appropriate definitive management?
Explanation
Question 36
A 28-year-old man sustains a twisting injury to his knee. Examination reveals 15 degrees of increased external rotation on the dial test at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is equal bilaterally. Which structure is most likely injured?
Explanation
Question 37
A 22-year-old collegiate football player sustains a non-contact pivoting knee injury. MRI confirms an isolated ACL tear. He elects for reconstruction using a bone-patellar tendon-bone autograft. During the procedure, the femoral tunnel is drilled too anteriorly. Which complication is most likely postoperatively?
Explanation
Question 38
A 28-year-old skier sustains an acute knee injury and presents with a positive dial test at 30 degrees of flexion, which normalizes to the contralateral side at 90 degrees of flexion. Which of the following structures is most likely injured?
Explanation
Question 39
A 25-year-old overhead athlete presents with anterior shoulder pain. He describes a "dead arm" sensation when throwing. Physical exam reveals a positive O'Brien's active compression test. Which of the following MRI arthrogram findings is most consistent with a Type II SLAP tear?
Explanation
Question 40
A 20-year-old male sustains a traumatic anterior shoulder dislocation. After closed reduction, CT scan demonstrates a 25% anterior glenoid bone loss. What is the most appropriate definitive surgical management?
Explanation
Question 41
A 35-year-old laborer falls directly on the lateral aspect of his shoulder and is diagnosed with a grade III acromioclavicular (AC) joint separation. Which ligaments are completely disrupted in this injury?
Explanation
Question 42
A 16-year-old female experiences recurrent patellar dislocations. Physical exam reveals apprehension with lateral patellar translation. What is the primary soft-tissue restraint to lateral patellar translation at 20 degrees of knee flexion?
Explanation
Question 43
A 30-year-old male sustains a posterior knee dislocation. After reduction, his ankle-brachial index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 44
Which bundle of the anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation when the knee is in 90 degrees of flexion?
Explanation
Question 45
A 24-year-old gymnast presents with a painful shoulder. Examination demonstrates generalized ligamentous laxity, positive sulcus sign, and apprehension with anterior and posterior translation. She has failed 6 months of physical therapy. What is the most appropriate surgical treatment for her multidirectional instability?
Explanation
Question 46
During an ACL reconstruction using a hamstring autograft, the surgeon uses a suspensory fixation device on the femur and an interference screw on the tibia. What is the most common mechanism of graft failure in the first 3 months postoperatively?
Explanation
Question 47
A 19-year-old football player sustains a valgus blow to his knee. Exam reveals a grade III MCL injury and an ACL tear. What is the recommended treatment strategy?
Explanation
Question 48
A 30-year-old baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. Physical examination reveals a loss of 25 degrees of internal rotation compared to the contralateral side, while external rotation is increased. What is the most likely diagnosis?
Explanation
Question 49
A patient presents with a chronic posterolateral corner (PLC) deficient knee resulting in a varus thrust during gait. Radiographs show mechanical axis falling medial to the knee center and no advanced osteoarthritis. What is the most appropriate initial surgical management?
Explanation
Question 50
In performing an arthroscopic repair of a Bankart lesion, the surgeon places suture anchors at the 3, 4, and 5 o'clock positions on the glenoid (in a right shoulder). Which nerve is most at risk if the drill penetrates the anteroinferior glenoid neck too deeply?
Explanation
Question 51
A 21-year-old athlete undergoes revision ACL reconstruction. Preoperative CT scan shows an expanded tibial tunnel measuring 16 mm in diameter. What is the preferred surgical strategy in this setting?
Explanation
Question 52
A 22-year-old collegiate soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Compared to a quadruple-stranded hamstring autograft, what is the most likely long-term complication associated with this graft choice?
Explanation
Question 53
A 25-year-old man presents with knee pain after a twisting injury. Physical examination reveals an asymmetric increased external rotation of the tibia of 15 degrees at 30 degrees of knee flexion, but no difference compared to the contralateral knee at 90 degrees of flexion. Which of the following structures is most likely injured?
Explanation
Question 54
A 20-year-old rugby player undergoes a Latarjet procedure for recurrent anterior shoulder instability with significant glenoid bone loss. Postoperatively, he presents with weakness in elbow flexion and decreased sensation over the lateral forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 55
A 30-year-old male is evaluated in the trauma bay after a high-speed motorcycle accident. He has a grossly deformed knee which is quickly reduced and splinted. His ankle-brachial index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 56
A 24-year-old skier sustains an isolated Grade III injury to the medial collateral ligament (MCL). Magnetic resonance imaging reveals an avulsion of the MCL from its tibial insertion with the distal end flipped superficial to the pes anserinus. What is the most appropriate management?
Explanation
Question 57
A 45-year-old male manual laborer complains of deep shoulder pain and mechanical clicking. MRI demonstrates a Type II Superior Labrum Anterior to Posterior (SLAP) tear. Nonoperative management has failed. What is the most appropriate surgical treatment in this patient demographic?
Explanation
Question 58
A 35-year-old man presents to the emergency department complaining of shoulder pain after a first-time generalized tonic-clonic seizure. On examination, his arm is locked in adduction and internal rotation. Radiographs reveal a posterior shoulder dislocation with an anteromedial humeral head defect involving 20% of the articular surface. What is this defect termed?
Explanation
Question 59
During an anterior cruciate ligament (ACL) reconstruction, the surgeon evaluates the anatomy of the native ACL footprint. Which of the following statements correctly describes the biomechanics of the two main bundles of the ACL?
Explanation
Question 60
A 28-year-old dashboard-injury victim presents with a positive posterior drawer test and a posterior sag sign. MRI confirms an isolated Grade II posterior cruciate ligament (PCL) tear. What is the most appropriate initial management?
Explanation
Question 61
A 35-year-old man presents with a locked shoulder after a generalized seizure. Radiographs demonstrate a posterior shoulder dislocation with an anterior humeral head defect involving 25% of the articular surface as shown in Figure 1.
What is the most appropriate surgical management?
Explanation
Question 62
A 22-year-old football player undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Six months postoperatively, he complains of anterior knee pain and a persistent 10-degree extension lag. A sagittal MRI reveals graft impingement against the intercondylar notch roof. Which of the following technical errors most likely caused this complication?
Explanation
Question 63
A 26-year-old male is brought to the emergency department after a high-speed motorcycle accident. Examination reveals a grossly unstable knee with a suspected multi-ligamentous injury (knee dislocation). Distal pulses are palpable, but the ankle-brachial index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 64
An 8-year-old girl (Tanner stage 1) sustains a midsubstance anterior cruciate ligament (ACL) tear. She experiences recurrent instability despite bracing and physical therapy. What is the most appropriate surgical technique to minimize the risk of physeal growth arrest?
Explanation
Question 65
A 22-year-old collegiate soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Which of the following is the most common complication uniquely associated with this specific graft choice compared to hamstring autograft?
Explanation
Question 66
A 19-year-old female gymnast presents with bilateral shoulder pain and a sensation of the shoulders "slipping" out of joint. Examination reveals positive sulcus signs bilaterally and generalized ligamentous laxity (Beighton score 7/9). Initial management should consist of:
Explanation
Question 67
A 26-year-old rugby player sustains a direct blow to the proximal tibia with the knee flexed at 90 degrees. Examination demonstrates a posterior sag sign and 8 mm of posterior translation of the tibia on the femur at 90 degrees of flexion, but normal translation at 30 degrees. The dial test is negative. What is the most appropriate initial management?
Explanation
Question 68
A 24-year-old throwing athlete undergoes an arthroscopic Type II SLAP repair. What is the most common postoperative complication that prevents a return to the previous level of overhead competition?
Explanation
Question 69
A 35-year-old man sustains an ultra-low velocity knee dislocation after a misstep. Following closed reduction in the emergency department, his ankle-brachial index (ABI) is measured at 0.7. What is the most appropriate next step in management?
Explanation
Question 70
A 29-year-old cyclist falls directly onto his shoulder point. Radiographs confirm a 150% superior displacement of the distal clavicle relative to the acromion, and the coracoclavicular distance is increased by 150% compared to the contralateral side. This represents which type of acromioclavicular (AC) joint injury according to the Rockwood classification?
Explanation
Question 71
A 31-year-old soccer player sustains a hyperextension and varus injury to his knee. On examination, he has 15 degrees of increased external tibial rotation at 30 degrees of knee flexion compared to the contralateral side. This asymmetry completely resolves when tested at 90 degrees of flexion. Which structure is most likely injured?
Explanation
Question 72
A 22-year-old football player sustains a recurrent anterior shoulder dislocation.
Advanced imaging demonstrates an engaging Hill-Sachs lesion and anterior glenoid bone loss of 28%. What is the most appropriate surgical management to minimize the risk of recurrence?
Explanation
Question 73
A 40-year-old recreational skier presents with medial knee pain after catching an inside edge. Examination reveals 4 mm of medial opening to valgus stress at 30 degrees of flexion with a firm endpoint, but no opening at 0 degrees. MRI confirms a partial tear of the superficial MCL at its femoral attachment. What is the recommended treatment?
Explanation
None
