High-Energy Talar Neck Fracture: Diagnostic Insights & Crucial MRI Sagittal Analysis

Key Takeaway
MRI sagittal views are crucial for high-energy talar neck fractures, offering indispensable insights beyond CT. They exquisitely detail soft tissue injuries, including ligamentous integrity (deltoid, calcaneofibular, interosseous talocalcaneal ligaments) and articular cartilage status. This comprehensive assessment aids in surgical planning, prognostication, and evaluating avascular necrosis risk.
A 38-year-old male presents following a 15-foot fall. He has severe hindfoot pain. Clinical exam shows a tense, swollen ankle. Plain films reveal a displaced talar neck fracture. Describe your initial assessment and the radiographic findings shown in Figure 3-61.
Candidate: I would start by confirming hemodynamic stability and performing a thorough neurovascular exam, as this is a high-energy injury. I would note the skin status, as these are prone to soft tissue compromise. The lateral X-ray shows a displaced talar neck fracture. I would classify this using the Hawkins system, which correlates displacement with the risk of AVN. I would request a CT scan to look for comminution, articular step-off, and to finalize operative planning.
The candidate fails to address the "tense" soft tissue exam, misses the urgency of fracture-dislocations (which are orthopaedic emergencies), or neglects to mention the specific importance of the Hawkins sign or the risk of varus malunion in their management plan.
The candidate immediately identifies the need for urgent reduction if there is skin tenting or neurovascular compromise. They systematically describe: 1) Clinical status (soft tissue envelope, NV status). 2) Radiographic findings (displacement, comminution, joint involvement). 3) Classification (Hawkins). 4) Definitive plan (CT scan for surgical planning, early ORIF using dual incisions, and mentioning the avoidance of varus malunion as the key to long-term success).
The patient has been taken to theatre for a displaced talar neck fracture. You are planning the surgical approach. Why is a single approach insufficient, and what does the image in Figure 2-77 illustrate regarding your fixation strategy?
Candidate: A single approach is rarely sufficient because you cannot adequately visualize both the medial and lateral cortices to prevent varus malunion. I would use dual (anteromedial and anterolateral) approaches. Figure 2-77 shows the use of lag screws for compression. I must ensure these are countersunk to avoid articular cartilage damage.
Ignoring the vascular anatomy. Failing to mention that the deltoid branches of the posterior tibial artery are at risk if the medial dissection is carried too far inferiorly, which significantly increases the risk of AVN.
The candidate highlights that dual approaches are the "Gold Standard" to avoid the common pitfall of medial comminution leading to varus collapse. They explicitly mention protecting the deltoid arterial supply medially and the necessity of the Canale view intraoperatively to confirm the reduction of the talar neck in both planes.
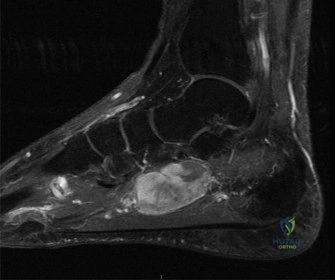
Post-operatively, you are reviewing the patient's progress. We discussed the significance of MRI in this case. Looking at the sagittal T1-weighted image below, what are you looking for, and how does this change your management?

Candidate: I am looking for signs of avascular necrosis (AVN). In a T1-weighted MRI, a drop in signal intensity in the talar body relative to normal fatty marrow suggests vascular compromise. If present, it influences our weight-bearing status, although I know the Hawkins sign on plain film remains a key clinical indicator of revascularization.
Equating the absence of a Hawkins sign purely to AVN. A candidate who fails to mention that the Hawkins sign is a hyperemic change in *living* bone, and thus its absence is suspicious but not diagnostic of necrotic bone.
The candidate explains that while MRI is highly sensitive, we distinguish between transient edema and established AVN using T2-weighted/STIR sequences. They correctly note that the "Hawkins sign" (subchondral osteopenia) is the definitive sign of *viability* and that management for AVN, if asymptomatic, remains protected weight-bearing to prevent structural collapse of the talar dome.
