Medial Subtalar Dislocation: A Comprehensive Clinical Case & Imaging Guide
Key Takeaway
Medial subtalar dislocation is diagnosed via detailed clinical examination revealing characteristic hindfoot valgus, lateral calcaneal displacement, and a palpable medial talar head. Plain radiographs confirm complete talocalcaneal and talonavicular disarticulation with an intact tibiotalar joint. CT scans are crucial post-reduction to detect occult fractures or incarcerated fragments and ensure concentric reduction.
Patient Presentation and History
A 32-year-old male, otherwise fit and healthy, presented to the Emergency Department following a high-energy motor vehicle accident as a restrained passenger. He reported significant immediate pain and deformity in his left ankle and foot, rendering him unable to bear weight. The mechanism described was an axial load through a plantarflexed foot with a severe inversion component, consistent with the foot being trapped under the dashboard during the frontal collision.
He denied any significant past medical history, noting no prior foot or ankle injuries, no diabetes mellitus, no peripheral vascular disease, and no neuropathic conditions. His only regular medication was a daily multivitamin. He is a non-smoker and consumes alcohol socially. His tetanus immunization status was up to date.
To understand the pathomechanics of this specific injury, it is critical to review the peritalar anatomy. The subtalar joint complex relies heavily on strong ligamentous restraints, primarily the interosseous talocalcaneal ligament, the cervical ligament, and the robust joint capsules. In a medial subtalar dislocation, the mechanism typically involves forced inversion on a plantarflexed foot. The sustentaculum tali acts as a bony fulcrum. As the deforming force continues, the talonavicular capsule fails first, followed by the disruption of the interosseous and cervical ligaments. The calcaneus and the rest of the foot displace medially, leaving the talus locked in the ankle mortise. The tibiotalar and calcaneocuboid articulations remain remarkably intact, defining the classic "peritalar" dislocation. The high-energy nature of this dashboard injury raises immediate concerns for concomitant osteochondral shearing injuries and severe soft tissue compromise.
Clinical Examination Findings
Upon initial assessment in the trauma bay, the patient was alert and oriented. His vital signs were stable, and the primary ATLS survey revealed no other life-threatening injuries. Attention was immediately directed to the isolated left lower extremity injury.
Inspection of the Extremity
The left hindfoot and midfoot displayed a marked and obvious deformity, classically described in orthopedic literature as an "acquired clubfoot." There was significant varus angulation of the hindfoot with prominent medial displacement of the calcaneus relative to the talus. The foot was locked in supination and plantarflexion. Conversely, the talar head was prominently palpable dorsolaterally, resting superficial to the navicular and cuboid.
The skin overlying the dorsolateral talar head appeared stretched and was under significant tension, displaying focal pallor and early signs of impending necrosis due to the underlying bony prominence. There was no gross skin breach, but the soft tissue envelope integrity was severely compromised. Swelling was rapidly increasing around the ankle and midfoot, obliterating normal anatomical landmarks. No obvious signs of open injury were noted, though careful circumferential scrutiny was performed given the high-energy mechanism.
Palpation and Bony Landmarks
Marked tenderness was elicited diffusely over the ankle joint and subtalar joint complex, extending distally into the midfoot. The talar head was distinctly palpable dorsolaterally, confirming the medial displacement of the distal foot segment. The calcaneus was displaced medially and slightly anteriorly. Gross bony crepitus was not appreciated, though the severe deformity made deep palpation difficult.
Range of Motion Assessment
Active and passive range of motion of the ankle and foot was severely restricted due to pain and mechanical blockade from the peritalar dislocation. The subtalar and talonavicular joints were entirely locked. Attempted movements exacerbated the patient's discomfort significantly and were deferred to prevent further soft tissue damage and neurovascular compromise.
Neurological and Vascular Assessment
A thorough neurological examination of the left lower extremity revealed no focal deficits. Sensation was intact to light touch and pinprick in all dermatomes encompassing L4, L5, S1, and S2. Motor function was grossly intact in all major muscle groups, including ankle dorsiflexion, plantarflexion, inversion, eversion, and toe flexion and extension, though limited by pain.
Crucially, the dorsalis pedis and posterior tibial pulses were strong and bilaterally symmetrical. Capillary refill in all toes was brisk at under two seconds. Despite the severe distortion of the medial neurovascular bundle and the tension over the dorsalis pedis artery laterally, vascular status remained excellent. However, given the evolving soft tissue envelope and high-energy mechanism, continuous serial monitoring of the neurovascular status and skin integrity was paramount until definitive reduction could be achieved.
Imaging and Diagnostics
Following the initial clinical assessment, emergent plain radiographs of the left foot and ankle were obtained in the trauma bay to confirm the direction of the dislocation and identify any gross concomitant fractures before attempting reduction.
Initial Radiographic Findings
Standard orthogonal views including anteroposterior, lateral, and oblique views of the foot, alongside anteroposterior and lateral views of the ankle, were reviewed.
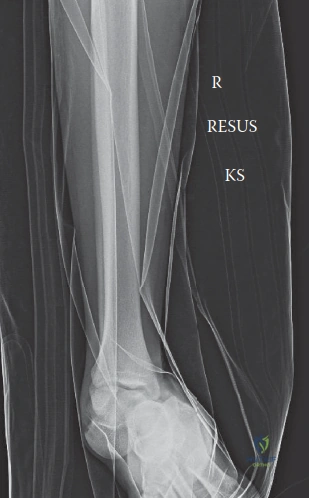
The lateral view demonstrated a complete loss of articulation between the talus and calcaneus at the subtalar joint, as well as a complete disarticulation between the talus and navicular. The talus remained perfectly congruent with the distal tibia within the ankle mortise, confirming a true subtalar dislocation rather than a tibiotalar or pantalar dislocation. The calcaneus was displaced medially and anteriorly relative to the talus. The talar head was seen dislocated dorsolaterally from the navicular.
The anteroposterior view of the foot confirmed the medial displacement of the entire foot relative to the talus. The talonavicular joint was completely incongruent, with the navicular resting medial to the talar head. The ankle views demonstrated no concomitant tibiotalar subluxation, widening of the syndesmosis, or obvious malleolar fractures. This radiographic pattern is the hallmark of a medial subtalar dislocation.
Advanced Imaging Indications
While plain radiographs are sufficient for diagnosing the dislocation and guiding the immediate closed reduction, computed tomography is an absolute requirement following the reduction of any subtalar dislocation. High-energy peritalar dislocations are associated with a high incidence of periarticular fractures that are frequently occult on plain radiography.
A post-reduction non-contrast CT scan of the foot and ankle with fine axial, coronal, and sagittal reformats is mandatory. The primary indications for this CT scan include evaluating for osteochondral shear fractures of the talar dome, talar head, or navicular. Furthermore, it is critical for identifying fractures of the lateral process of the talus, the posterior process of the talus, and the sustentaculum tali. Identifying these fractures is essential, as displaced intra-articular fragments can block concentric reduction and lead to rapid post-traumatic arthrosis if left unaddressed. Magnetic Resonance Imaging is rarely indicated in the acute setting but may be utilized in the subacute or chronic phases to evaluate for avascular necrosis of the talus or to map complex ligamentous disruptions if chronic instability develops.
Differential Diagnosis
When evaluating a severe deformity of the hindfoot following high-energy trauma, the differential diagnosis must include other complex peritalar injuries. Accurate diagnosis dictates the reduction maneuvers and surgical planning.
| Pathology | Mechanism of Injury | Clinical Deformity | Key Radiographic Feature | Management Priority |
|---|---|---|---|---|
| Medial Subtalar Dislocation | Inversion of plantarflexed foot | Foot in varus and supination, talar head prominent dorsolaterally | Talonavicular and talocalcaneal disarticulation, foot displaced medially | Emergent closed reduction to prevent skin necrosis |
| Lateral Subtalar Dislocation | Eversion of dorsiflexed foot | Foot in valgus and pronation, talar head prominent medially | Talonavicular and talocalcaneal disarticulation, foot displaced laterally | Emergent closed reduction, high rate of open reduction required |
| Talar Neck Fracture with Dislocation | High-energy axial load with forced dorsiflexion | Variable hindfoot deformity, severe swelling | Fracture line through talar neck, subluxation or dislocation of subtalar/tibiotalar joints | Emergent reduction, high risk of talar body avascular necrosis |
| Chopart Joint Dislocation | Direct crush or high-energy twisting | Midfoot shortening, severe midfoot swelling | Disarticulation at talonavicular and calcaneocuboid joints, subtalar joint intact | Reduction and stabilization of the transverse tarsal joint |
| Pantalar Dislocation | Extreme high-energy trauma | Gross instability of the entire hindfoot and ankle | Dislocation of tibiotalar, subtalar, and talonavicular joints simultaneously | Emergent reduction, extremely high risk of soft tissue compromise and AVN |
Surgical Decision Making and Classification
The immediate management of a medial subtalar dislocation is governed by the status of the soft tissue envelope. The prominent talar head places the overlying skin at imminent risk of pressure necrosis. Therefore, emergent closed reduction is the absolute first step in the surgical decision-making algorithm. Delaying reduction to obtain advanced imaging or waiting for optimal operating room availability is contraindicated if the skin is blanching or tented.
Classification of Subtalar Dislocations
Subtalar dislocations are anatomically classified based on the direction in which the distal segment the foot and calcaneus displaces relative to the talus.
* Medial Dislocations: Account for approximately 80 to 85 percent of all subtalar dislocations. The foot displaces medially. They are typically lower energy than lateral dislocations and have a higher success rate for closed reduction.
* Lateral Dislocations: Account for 15 to 20 percent of cases. The foot displaces laterally. These are often higher-energy injuries and are frequently associated with open wounds and a much higher rate of irreducibility due to soft tissue interposition.
* Anterior and Posterior Dislocations: Exceedingly rare, representing less than 1 percent of cases, usually resulting from severe direct trauma.
Indications for Operative Intervention
The primary indication for operative intervention in the acute setting is an irreducible dislocation. Approximately 10 to 15 percent of medial subtalar dislocations cannot be reduced closed. In medial dislocations, the most common blocks to closed reduction include the buttonholing of the talar head through the extensor digitorum brevis muscle belly, the extensor retinaculum, or the talonavicular joint capsule. Less commonly, the deep peroneal nerve or anterior tibial vessels can become entrapped.
If closed reduction is successful, the subsequent decision-making relies on the post-reduction CT scan and clinical stability. Operative intervention is indicated if there is persistent gross instability of the subtalar joint following reduction, which may require percutaneous transarticular Kirschner wire fixation. Furthermore, any displaced intra-articular fractures identified on the post-reduction CT, such as a displaced lateral process of the talus fracture or an osteochondral fragment within the subtalar or talonavicular joint space, necessitate open reduction and internal fixation or fragment excision.
Surgical Technique and Intervention
The initial intervention for this patient involves an emergent attempt at closed reduction in the emergency department under conscious sedation.
Closed Reduction Technique
Adequate muscle relaxation is critical for a successful closed reduction. The patient is placed under deep conscious sedation or general anesthesia. The knee must be flexed to 90 degrees to completely relax the gastrocnemius-soleus complex, which otherwise exerts a massive deforming force on the calcaneus via the Achilles tendon.
The reduction maneuver requires a coordinated, multi-step approach. First, an assistant applies counter-traction at the flexed knee. The surgeon grasps the heel and the forefoot, applying sustained longitudinal traction in the line of the deformity. To disengage the locked talonavicular and subtalar joints, the deformity must initially be exaggerated; for a medial dislocation, this means further plantarflexing and inverting the foot. Once the joints are disengaged, the surgeon applies direct manual pressure over the prominent dorsolateral talar head while simultaneously everting, abducting, and dorsiflexing the foot. A palpable and audible "clunk" typically signifies a successful concentric reduction. Following reduction, the foot is immediately assessed for stability by taking it through a gentle range of motion, and a well-padded short leg posterior splint with a U-stirrup is applied in a neutral position.
Open Reduction Technique
If closed reduction fails after two well-executed attempts with adequate sedation, the patient must be taken emergently to the operating room for an open reduction. For an irreducible medial subtalar dislocation, an anterolateral approach is utilized.
The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg, providing excellent access to the anterolateral hindfoot. A longitudinal incision is made starting from the tip of the lateral malleolus and extending distally toward the base of the fourth metatarsal, directly over the prominent talar head. Careful blunt dissection is performed through the subcutaneous tissues, meticulously identifying and retracting the branches of the superficial peroneal nerve and the sural nerve.
The extensor digitorum brevis muscle belly is identified. In irreducible medial dislocations, the talar head is frequently found buttonholed through the extensor retinaculum or the EDB muscle belly. The obstructing tissue is carefully incised or retracted to free the talar head. The talonavicular capsule may also be interposed and require longitudinal incision. Once the block is removed, the reduction maneuver described above longitudinal traction, eversion, and dorsiflexion is performed under direct visualization.
Fixation Construct and Joint Stabilization
Once reduced, either closed or open, the stability of the subtalar joint is assessed under live fluoroscopy. Most medial subtalar dislocations are inherently stable once concentrically reduced due to the congruency of the bony anatomy. However, if there is recurrent subluxation or gross instability, temporary percutaneous fixation is required.
This is achieved using smooth 2.0 mm or 2.4 mm Kirschner wires. Typically, one or two wires are driven from the plantar aspect of the calcaneus, across the subtalar joint, and into the talar body. An additional wire may be placed from the navicular into the talar head to stabilize the talonavicular joint if necessary. These wires are left protruding through the skin, bent, and capped for easy removal in the clinic setting. If open reduction was performed, the wound is irrigated copiously and closed in layers, ensuring a tension-free skin closure.
Post Operative Protocol and Rehabilitation
The post-reduction rehabilitation protocol is designed to protect the healing ligamentous structures while mitigating the long-term risks of joint stiffness and post-traumatic arthrosis.
Phase One Acute Immobilization
Immediately following reduction, the patient is placed in a bulky, well-padded short leg splint. Strict non-weight-bearing status is enforced. The primary goals during the first two weeks are edema control, wound healing if an open reduction was performed, and prevention of re-dislocation. Deep vein thrombosis prophylaxis is initiated based on patient risk factors and institutional protocols, given the immobilization.
Phase Two Transition and Early Motion
At the two-week mark, the patient returns to the clinic. If percutaneous K-wires were utilized, they are typically maintained for a total of four to six weeks. The splint is transitioned to a rigid short leg cast or a controlled ankle motion boot. The patient remains strictly non-weight-bearing. If the joint was stable and no K-wires were used, gentle active range of motion exercises of the ankle and subtalar joint may be initiated out of the boot to prevent severe arthrofibrosis, though passive stretching and inversion/eversion are strictly avoided.
Phase Three Weight Bearing Progression
At six weeks post-injury, any remaining K-wires are removed. Radiographs are obtained to confirm maintenance of concentric reduction and to evaluate for any early signs of avascular necrosis of the talus, which would appear as relative sclerosis of the talar body. The patient is transitioned to progressive partial weight-bearing in the CAM boot, advancing to full weight-bearing over the next four weeks. Formal physical therapy is initiated, focusing on aggressive active and active-assisted range of motion, peroneal muscle strengthening to enhance dynamic lateral stability, and proprioceptive training.
Phase Four Long Term Rehabilitation
By ten to twelve weeks, the patient is typically transitioned out of the CAM boot into a supportive shoe with a rigid heel counter or an ankle brace. High-impact activities and sports are generally restricted for a minimum of four to six months. Patients must be counseled that maximal medical improvement may take up to a year, and some degree of permanent restriction in subtalar inversion and eversion is expected.
Clinical Pearls and Pitfalls
Successfully managing a medial subtalar dislocation requires vigilance and an understanding of the subtle nuances associated with peritalar trauma.
- Pearl Knee Flexion is Mandatory: The most common reason for a failed closed reduction in the emergency department is inadequate relaxation of the gastrocnemius-soleus complex. Always flex the knee to 90 degrees during the reduction maneuver to eliminate this massive deforming force.
- Pearl The Post Reduction CT is Non Negotiable: Plain radiographs are notoriously poor at identifying osteochondral shearing injuries and subtle periarticular fractures. A post-reduction CT scan must be obtained in every case to rule out intra-articular fragments that will destroy the joint if left behind.
- Pitfall Missing the Snowboarders Fracture: The lateral process of the talus is highly susceptible to fracture during the inversion/dorsiflexion moments of peritalar trauma. Missing a displaced lateral process fracture will lead to rapid subtalar arthrosis and chronic lateral-sided foot pain.
- Pitfall Delaying Reduction for Imaging: The skin overlying the dislocated talar head is under extreme tension. Delaying reduction to obtain a CT scan or waiting for an orthopedic team to arrive can result in full-thickness skin necrosis, converting a closed injury into a disastrous open joint injury requiring complex soft tissue coverage.
- Pearl Understanding the Nomenclature: Subtalar dislocations are named by the direction the foot travels, not the talus. In a medial dislocation, the foot is medial, but the most prominent bony landmark is the talar head, which sits dorsolaterally. This counterintuitive clinical picture often leads to misdiagnosis in initial trauma bay documentation.
- Pitfall Underestimating Long Term Complications: While the avascular necrosis rate of the talus is significantly lower in isolated subtalar dislocations compared to talar neck fractures, it is not zero. The artery of the tarsal canal is frequently torn. Furthermore, post-traumatic subtalar arthritis occurs in up to 50 percent of high-energy cases, regardless of the quality of reduction, due to the initial chondral insult. Patients must be appropriately counseled regarding these long-term prognoses.
