Step-by-Step Medial Side of the Ankle Approach Guide
Key Takeaway
For anyone wondering about Step-by-Step Medial Side of the Ankle Approach Guide, The medial approach to the ankle is a surgical technique designed to expose the medial side of the ankle joint. It's used for procedures such as arthrodesis, excision or fixation of osteochondral fragments from the talus, and removal of loose bodies. The approach involves a 10-cm incision centered on the medial malleolus, with careful dissection.
Introduction and Epidemiology
The medial approach to the ankle joint represents a fundamental exposure in orthopedic surgery, providing direct access to the medial malleolus, the medial aspect of the tibiotalar joint, and associated soft tissue structures. Its utility spans a broad spectrum of pathologies, ranging from traumatic injuries such as medial malleolar fractures to degenerative conditions like ankle arthritis, and specific issues such as osteochondral lesions of the talus or soft tissue impingement. The approach is favored for its relatively straightforward dissection, inherent safety profile due to the subcutaneous nature of the underlying bone, and minimal disruption of critical neurovascular bundles when performed meticulously.
Historically, surgical approaches to the ankle have evolved with advancements in anatomical understanding and surgical instrumentation. The medial approach, being largely extensile, allows for precise visualization and management of complex pathologies. The epidemiology of conditions requiring this approach is diverse. Ankle fractures, particularly those involving the medial malleolus, are common, with an incidence rate estimated between 100 and 150 per 100,000 person-years, varying by age and activity level. Osteochondral lesions of the talus (OCLTs) also frequently present on the medial dome, often following traumatic events, with reported prevalence as high as 70% in symptomatic ankles. End-stage ankle arthritis, while less common than hip or knee arthritis, often necessitates surgical intervention, including arthrodesis, for which the medial approach is a viable option. Understanding the indications, detailed anatomy, and meticulous technique is paramount for successful patient outcomes.
Surgical Anatomy and Biomechanics
A comprehensive understanding of the regional anatomy is critical for executing a safe and effective medial ankle approach. The ankle joint is a complex hinge joint formed by the articulation of the distal tibia and fibula (forming the mortise) with the talus. The medial structures play a pivotal role in ankle stability and function.
Bony Landmarks
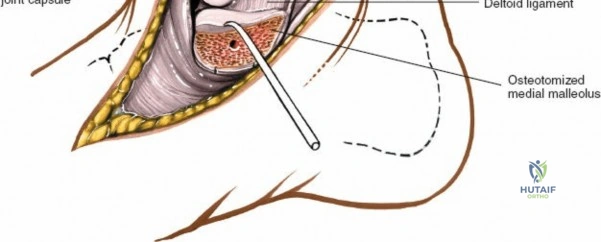
The primary bony landmark for this approach is the medial malleolus, which is the palpable distal end of the tibia. This prominent structure serves as the origin for the deltoid ligament and forms the medial boundary of the tibiotalar joint. Other critical bony structures exposed or navigated include the medial talar dome, the body of the talus, and the sustentaculum tali of the calcaneus, particularly during more extensile exposures or subtalar joint involvement. The subcutaneous nature of the medial malleolus facilitates both palpation and direct surgical access.
Ligamentous Structures
The deltoid ligament complex is the primary static stabilizer of the medial ankle. It consists of superficial and deep layers.
* Superficial Layer: Originates from the anterior colliculus of the medial malleolus and fans out to insert onto the navicular (tibionavicular part), the sustentaculum tali (tibiocalcaneal part), and the posterior aspect of the talus (superficial posterior tibiotalar part).
* Deep Layer: Consists of the anterior deep tibiotalar ligament and the posterior deep tibiotalar ligament. These originate from the posterior colliculus and intercollicular groove of the medial malleolus and insert onto the medial aspect of the talar body. The deep deltoid ligaments are critical primary stabilizers against talar external rotation and valgus tilt.
Preservation or careful repair of these structures is essential for maintaining ankle stability.
Tendinous Structures
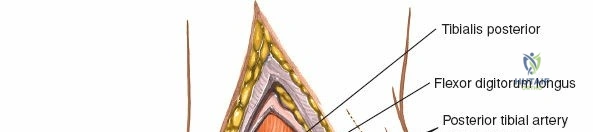
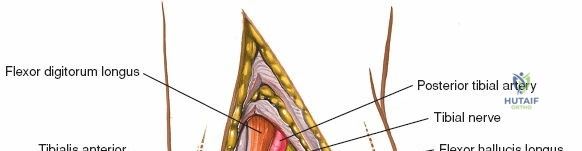
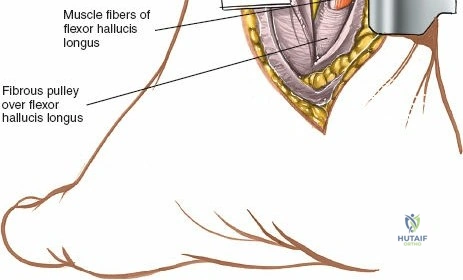
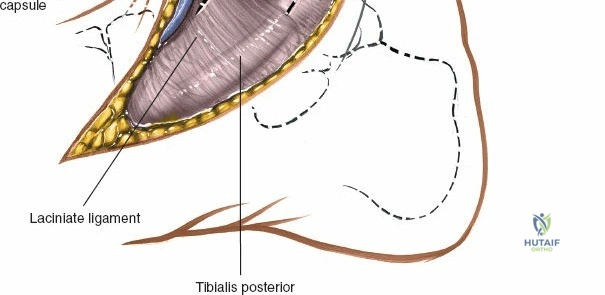
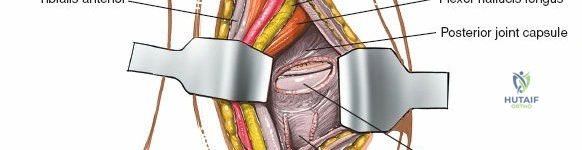
The posteromedial aspect of the ankle houses the "Tom, Dick, And Harry" tendons, which course posterior to the medial malleolus within individual fibro-osseous tunnels. From anterior to posterior, these are:
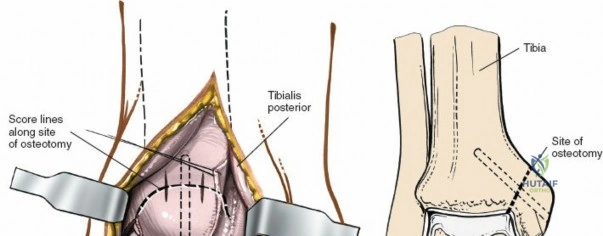
* Tibialis Posterior Tendon: This tendon is the most anterior of the three, lying immediately posterior to the medial malleolus. It is a primary inverter and plantarflexor of the foot and is vital for maintaining the medial longitudinal arch.
* Flexor Digitorum Longus Tendon: Located posterior to the tibialis posterior, this tendon is responsible for flexing the lateral four toes.
* Flexor Hallucis Longus Tendon: The most posterior of the three, this tendon lies deep and posterior to the flexor digitorum longus, passing through a groove on the posterior aspect of the talus. It is the primary flexor of the great toe.
These tendons are contained within synovial sheaths and must be identified and retracted judiciously to prevent iatrogenic injury or adhesions.
Neurovascular Structures
Several critical neurovascular structures are in proximity to the medial ankle approach:
* Posterior Tibial Artery and Tibial Nerve: These structures, along with the flexor digitorum longus and flexor hallucis longus tendons, are contained within the tarsal tunnel, situated posterior to the medial malleolus. The tibial nerve provides motor innervation to intrinsic foot muscles and sensory innervation to the sole of the foot. The posterior tibial artery is a main blood supply to the foot. The approach typically stays anterior to the tibialis posterior tendon, thus minimizing direct risk to these structures, but meticulous technique is required for deeper or more posterior dissection.
* Saphenous Nerve: A purely sensory nerve, the saphenous nerve courses anterior to the medial malleolus, often accompanied by the great saphenous vein. It provides sensation to the medial aspect of the lower leg and foot. It is susceptible to injury during skin incision and subcutaneous dissection.
* Great Saphenous Vein: Located subcutaneously, anterior to the medial malleolus, it typically runs with the saphenous nerve. It should be identified and protected, or ligated if necessary, though preservation is preferred.
Biomechanics
The medial ankle structures, particularly the deltoid ligament, are crucial for resisting excessive talar external rotation and valgus forces. Injury to the deltoid ligament can lead to gross ankle instability, especially in combination with lateral malleolar fractures. The tibialis posterior tendon is a dynamic stabilizer, supporting the medial arch and contributing to hindfoot inversion. Understanding these biomechanical functions informs the surgical strategy, particularly when addressing complex fractures or ligamentous instabilities. The approach itself minimizes disruption to the intrinsic stability mechanisms when performed along the subcutaneous border of the tibia.
Indications and Contraindications
The medial approach exposes the medial side of the ankle joint. Its versatility allows for addressing a wide range of pathologies, making it a valuable tool in the orthopedic surgeon's armamentarium.
Specific Indications
- Arthrodesis of the Ankle (Tibiotalar Arthrodesis): For end-stage ankle arthritis, particularly when a direct anterior approach is complicated by significant deformity or hardware, or when concomitant medial malleolar pathology needs addressing. The medial approach can be combined with a lateral approach for comprehensive joint preparation and fixation.
- Excision or Fixation of Osteochondral Fragments from the Medial Side of the Talus (OCL/OCD): Medial talar OCLs are common, especially after ankle sprains or direct trauma. This approach allows direct visualization and management, including fragment removal, internal fixation, microfracture, or osteochondral autograft/allograft transplantation.
- Removal of Loose Bodies from the Ankle Joint: If loose bodies are localized to the medial gutter or medial aspect of the tibiotalar joint.
- Medial Malleolar Fractures: The gold standard for open reduction and internal fixation (ORIF) of displaced medial malleolar fractures, ensuring anatomical reduction and stable fixation. This includes isolated medial malleolar fractures, as well as components of bimalleolar and trimalleolar ankle fractures.
- Deltoid Ligament Repair or Reconstruction: For acute, reparable ruptures of the deltoid ligament, often associated with pronation-external rotation (PER) ankle fractures, or for chronic instability requiring reconstruction.
- Medial Soft Tissue Releases: In cases of severe equinovarus deformities, particularly those involving contracture of the tibialis posterior tendon or deep fascial structures.
- Accessory Navicular Excision and Tibialis Posterior Advancement: For symptomatic accessory navicular leading to tibialis posterior dysfunction or painful os naviculare syndrome.
- Tarsal Tunnel Decompression: Although a separate posteromedial approach is more common, a medial approach can be modified or extended to address tarsal tunnel pathology anteriorly.
Contraindications
Absolute contraindications for the medial ankle approach are few and generally align with those for any elective surgical procedure.
* Active Local Infection: Presence of cellulitis, abscess, or osteomyelitis in the surgical field significantly increases the risk of postoperative infection and complicates healing.
* Severe Peripheral Vascular Disease: Compromised vascular supply to the limb can impair wound healing and increase the risk of complications, especially with extensive soft tissue dissection.
* Severe Soft Tissue Compromise: Prior trauma, burns, radiation, or extensive scarring over the intended incision site may necessitate alternative approaches or staged reconstruction.
* Severe Patient Comorbidities: Uncontrolled diabetes, severe cardiac or pulmonary disease, or other systemic conditions that significantly elevate surgical risk.
* Pathology Better Addressed by Other Approaches: For instance, lateral talar OCLs, posterior malleolar fractures, or global ankle arthrodesis where circumferential exposure is preferred.
Indications Summary Table
| Operative Indications (Medial Approach) | Non-Operative Indications (Conservative Management) |
|---|---|
| Displaced medial malleolar fractures | Nondisplaced, stable medial malleolar fractures |
| Symptomatic, displaced osteochondral lesions of the medial talus | Asymptomatic or small, stable osteochondral lesions of the talus |
| Symptomatic loose bodies in the medial ankle compartment | Asymptomatic loose bodies |
| End-stage ankle arthritis requiring arthrodesis | Mild to moderate ankle arthritis (NSAIDs, PT, injections, bracing) |
| Acute, complete deltoid ligament ruptures with instability | Partial deltoid ligament tears or sprains without gross instability (RICE, PT) |
| Symptomatic accessory navicular syndrome | Asymptomatic accessory navicular |
| Tarsal tunnel syndrome refractory to conservative management | Mild tarsal tunnel symptoms responsive to rest, NSAIDs, orthotics |
| Severe equinovarus deformity requiring medial soft tissue release | Mild to moderate equinovarus deformity managed with bracing, casting, physical therapy |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is critical to optimize outcomes and minimize complications associated with the medial ankle approach.
Preoperative Planning
- Clinical Assessment: A thorough history and physical examination are essential to understand the patient's symptoms, functional limitations, and to identify any relevant comorbidities. Neurovascular status of the extremity must be documented.
- Imaging Studies:
- Standard Radiographs: Anteroposterior, lateral, and mortise views of the ankle are the initial imaging modalities. These help to identify fractures, arthritic changes, bone spurs, and the location of large loose bodies or OCLs. Stress views may be helpful for assessing ligamentous instability.
- Computed Tomography (CT Scan): Indispensable for detailed evaluation of fracture patterns (e.g., medial malleolar comminution, posterior malleolar involvement), characterizing OCLs (size, depth, cystic changes), assessing malunion, or planning complex arthrodesis.
- Magnetic Resonance Imaging (MRI): Provides excellent visualization of soft tissues, including the deltoid ligament, tibialis posterior tendon, and articular cartilage. It is crucial for assessing OCL cartilage integrity, identifying loose bodies not visible on X-ray, and evaluating the extent of soft tissue injuries or impingement.
- Surgical Planning: Based on imaging, determine the exact location and extent of pathology. Plan the incision length and trajectory. For fracture fixation, select appropriate implants (screws, plates, K-wires) and consider their placement to avoid joint intrusion and maximize stability. For arthrodesis, plan bone resection and desired fusion position.
- Informed Consent: Discuss the diagnosis, proposed surgical procedure, potential benefits, risks (including specific complications like nerve injury, infection, nonunion), alternatives, and expected postoperative course with the patient.
Patient Positioning
The patient is typically placed in the supine position on the operating table.

- Limb Preparation: The entire lower extremity, from the midthigh to the toes, is prepared and draped in a sterile fashion.
- Exsanguination and Tourniquet Application: To provide a bloodless field, the limb is exsanguinated either by elevating it for 5 minutes or by applying a soft rubber bandage (e.g., Esmarch bandage) firmly from distal to proximal. A pneumatic tourniquet is then inflated to an appropriate pressure (typically 250-300 mmHg for the lower extremity, or 100 mmHg above systolic blood pressure), ensuring the tourniquet time is monitored closely.
- Leg Position: The operating table should allow the limb to be positioned with the knee slightly flexed. The natural external rotation of the leg exposes the medial malleolus optimally. The pelvis ordinarily does not have to be tilted to improve the exposure, as minor adjustments to leg rotation are usually sufficient.
The external rotation can be maintained with sandbags or positioning devices if needed, but often, simply allowing the leg to rest naturally suffices. Ensure the foot and ankle are free to be manipulated during the procedure for optimal visualization and reduction. A bump under the ipsilateral hip can further assist in internal rotation of the hip, bringing the medial malleolus into a more superior and accessible position.
Detailed Surgical Approach and Technique
The medial ankle approach is a direct and versatile method for addressing a variety of pathologies. The principle is to gain direct access to the medial malleolus and tibiotalar joint while protecting neurovascular structures.
Incision Planning and Skin Incision
The medial malleolus is the palpable distal end of the tibia, serving as the primary landmark.
The incision should be carefully planned. A straight or gently curved longitudinal incision is typically made directly over the medial malleolus.
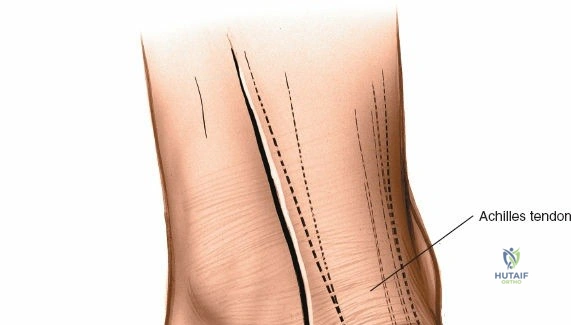
This incision usually extends from approximately 2-3 cm proximal to the tip of the medial malleolus to just distal to it, following the anterior border of the malleolus. For more extensive exposure, such as for ankle arthrodesis, the incision can be extended further proximally along the subcutaneous border of the tibia and/or distally over the talus and navicular. A common curvilinear incision starts just anterior to the tibialis anterior tendon, curving posteromedially around the malleolus.
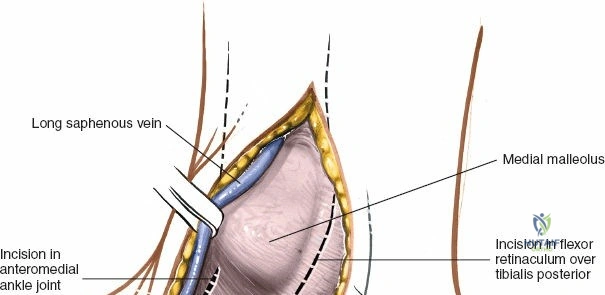
Care must be taken during the skin incision to avoid injury to the great saphenous vein and the saphenous nerve, which run subcutaneously anterior to the medial malleolus. These structures should be identified and protected, or ligated if their presence significantly obstructs exposure and their preservation is not critical for limb viability (e.g., smaller venous branches).
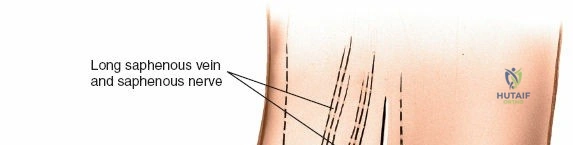
Superficial Dissection
After incising the skin and subcutaneous tissue, the great saphenous vein and saphenous nerve are typically encountered.

The saphenous nerve usually lies superficial to the great saphenous vein, or anterior to it.
These structures should be carefully identified. The nerve is a sensory branch and injury can lead to numbness or painful neuroma.
They are then gently retracted either anteriorly or posteriorly using blunt dissection and self-retaining retractors, exposing the deeper fascia overlying the medial malleolus and periosteum.
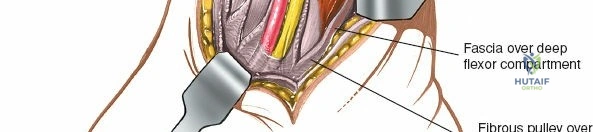
Deep Dissection and Internervous Plane
The approach uses no true internervous plane. Nevertheless, the surgery is safe because the tibia is largely subcutaneous, and dissection largely stays on bone.
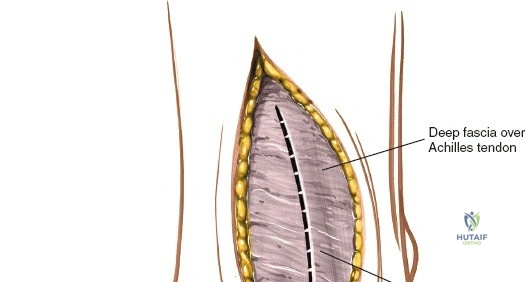
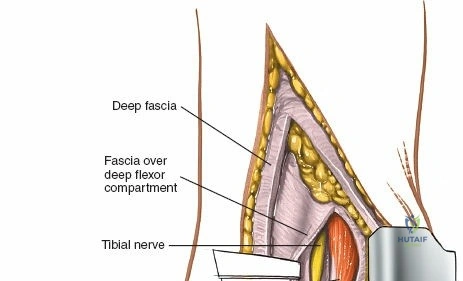
The deep fascia is incised, and the periosteum over the medial malleolus is identified.
A subperiosteal dissection is then performed using an elevator to expose the medial malleolus.

The dissection proceeds directly onto the bone, peeling the periosteum and attached deltoid ligament anteriorly and posteriorly.
It is crucial to be aware of the tibialis posterior tendon, which lies immediately posterior to the medial malleolus. This tendon, along with the flexor digitorum longus, flexor hallucis longus, posterior tibial artery, and tibial nerve, passes posterior to the medial malleolus. By performing a subperiosteal dissection on the anterior and inferior aspects of the medial malleolus, these posteromedial structures are protected.
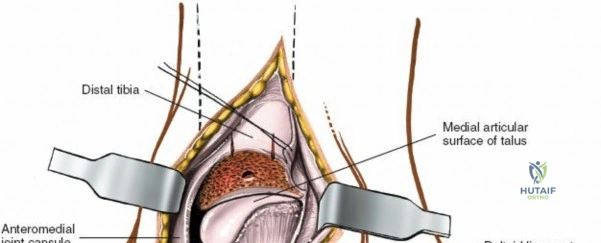
Retraction of the soft tissues, including the deltoid ligament complex, allows for clear visualization of the medial aspect of the tibiotalar joint and the talar dome.
Specific Procedure Techniques
Medial Malleolar Fracture Fixation
- Exposure: Once the medial malleolus is exposed, the fracture site is identified.
- Hematoma Evacuation: Hematoma is irrigated and evacuated to allow for clear visualization.
- Reduction: The fracture fragments are meticulously reduced anatomically. This often involves manipulating the foot and ankle, ensuring congruence of the joint surface and proper alignment of the malleolus to the tibia. Provisional fixation with K-wires may be used to hold the reduction.
- Fixation:
- Lag Screws: Typically, one or two partially threaded cancellous lag screws are inserted from the tip of the medial malleolus proximally into the tibial shaft, perpendicular to the fracture plane, to achieve interfragmentary compression.
- Tension Band Wiring: For smaller, comminuted fragments, or when strong pullout is anticipated (e.g., elderly patients), a tension band wiring technique can be employed. This involves two K-wires and a figure-of-eight wire loop.
- Antiglide Plate: Occasionally, a small antiglide plate may be used on the anterior aspect of the malleolus to prevent posterior displacement.
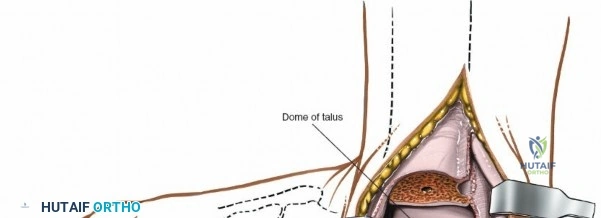
Ankle Arthrodesis
- Joint Exposure and Debridement: The medial approach allows for direct visualization of the medial tibiotalar joint. Articular cartilage is systematically resected from the distal tibia and talar dome using osteotomes, curettes, and burrs. All sclerotic bone is removed to expose bleeding cancellous bone, which is essential for fusion.

- Joint Preparation: The opposing surfaces of the tibia and talus are contoured to maximize surface area contact. Techniques include flat cuts, or creation of interlocking surfaces.

- Positioning: The ankle is positioned in neutral dorsiflexion (or slight plantarflexion, 0-5 degrees), slight valgus (0-5 degrees), and neutral rotation. This functional position optimizes gait and reduces stress on adjacent joints.
- Fixation: Typically, 2-4 large diameter cancellous screws (e.g., 6.5 or 7.3 mm) are used for compression and stability. Screws can be placed from the tibia into the talus and/or from the talus into the tibia. A medial plate may also be utilized to augment stability, especially in complex cases or revisional fusions.
Osteochondral Lesion (OCL) Management
- Lesion Identification: After gaining access to the medial tibiotalar joint, the ankle is distracted or manipulated to visualize the medial talar dome. The OCL is identified.
- Debridement and Containment: Loose or unstable cartilage fragments are debrided. The edges of the lesion are often debrided back to stable cartilage.
- Treatment Options:
- Microfracture: If the subchondral bone is viable, multiple perforations (microfractures) are made into the subchondral bone using an awl to stimulate a fibrocartilaginous healing response.
- Fragment Excision/Fixation: Small, non-viable fragments are excised. Larger, viable fragments may be fixed with small headless screws or bioabsorbable pins if amenable.
- Osteochondral Autograft/Allograft Transplantation (OATS): For larger or cystic lesions, an osteochondral cylinder may be harvested from a less weight-bearing area (e.g., ipsilateral knee) or an allograft used to resurface the defect. This requires precise drilling and impaction.
Loose Body Removal
- Systematic Search: The joint is inspected thoroughly. Loose bodies often reside in the medial gutter or within recesses of the joint.
- Removal: Loose bodies are grasped with forceps and carefully extracted. Irrigation and repeat inspection ensure all fragments are removed.
Wound Closure
- Hemostasis: Ensure meticulous hemostasis.
- Periosteum/Deltoid Repair: If the deltoid ligament or periosteum was extensively elevated or incised, it should be meticulously repaired with absorbable sutures to help restore stability and soft tissue integrity.
- Fascial Closure: The deep fascia is closed with absorbable sutures.
- Subcutaneous Closure: The subcutaneous layer is approximated to reduce dead space and tension on the skin edges.
- Skin Closure: The skin is closed with staples or non-absorbable sutures. A sterile dressing is applied.






Complications and Management
Despite being a relatively safe approach, the medial ankle exposure is not without potential complications. Awareness of these risks and strategies for prevention and management is crucial for all orthopedic surgeons.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Risk Factors | Prevention Strategies | Salvage/Management Strategies |
|---|---|---|---|---|
| Wound Infection | 1-5% | Diabetes, immunosuppression, poor vascularity, prolonged surgery | Strict aseptic technique, prophylactic antibiotics, meticulous hemostasis | Debridement, targeted antibiotics, wound VAC, flap coverage (severe) |
| Wound Dehiscence/Healing Issues | 2-10% | Smoking, diabetes, tension on closure, previous surgery, soft tissue trauma | Tension-free closure, careful soft tissue handling, smoking cessation | Local wound care, secondary closure, skin grafting, flap coverage |
| Saphenous Nerve Injury/Neuroma | 5-20% (sensory) | Direct laceration, stretch injury, entrapment in scar | Careful identification and retraction, meticulous subcutaneous dissection | Neuropathic pain management, nerve block, neuroma excision, neurolysis |
| Posterior Tibial Nerve Injury | <1% | Deep, posterior dissection, aggressive retraction | Maintain dissection anterior to TP tendon, minimize aggressive retraction | Neurolysis, pain management, tarsal tunnel release if entrapped |
| Deltoid Ligament Insufficiency | Variable | Inadequate repair, excessive release during exposure | Meticulous repair/reconstruction, judicious release of ligament | Reconstruction with autograft/allograft, bracing |
| Hardware Irritation | 5-15% | Prominent screws/plates, superficial placement | Countersinking, careful plate selection/contouring, appropriate screw length | Hardware removal after healing is complete |
| Nonunion/Malunion (Fractures/Arthrodesis) | 5-10% | Inadequate reduction/fixation, poor bone quality, infection, smoking | Anatomical reduction, stable fixation, bone grafting (if indicated) | Revision ORIF, revision arthrodesis, bone grafting, external fixation |
| Persistent Pain/Stiffness | Common, variable | Arthrosis, scar tissue, inadequate rehabilitation, complex regional pain syndrome | Early range of motion (when appropriate), comprehensive physical therapy | Physiotherapy, pain management, lysis of adhesions, manipulation under anesthesia |
| Ankle Arthrosis (Post-trauma) | 10-20% (long-term) | Inaccurate reduction, articular cartilage damage, infection | Anatomical reduction, stable fixation, early weight-bearing (when appropriate) | Arthrodesis, arthroplasty (if indicated) |
| Vascular Injury (Great Saphenous Vein) | <1% | Laceration during superficial dissection | Careful identification, gentle retraction, ligation if necessary | Ligation, direct repair (rarely needed) |
Specific Considerations
- Tarsal Tunnel Syndrome: While rare, direct injury or irritation to the tibial nerve or its branches within the tarsal tunnel can occur with aggressive posterior retraction or if dissection extends too far posteriorly. This can lead to pain, numbness, and weakness in the foot.
- Avascular Necrosis of the Talus: Although typically associated with talar neck fractures, extensive subperiosteal dissection around the talus, especially in cases of OCLs, theoretically could compromise the tenuous blood supply, although this is a rare occurrence with the medial approach itself.
- Complex Regional Pain Syndrome (CRPS): A debilitating neuropathic pain condition that can develop after any extremity trauma or surgery. Early recognition and aggressive multimodal pain management are critical.
Prevention is paramount. Meticulous surgical technique, precise anatomical identification, careful soft tissue handling, and appropriate prophylactic measures (e.g., antibiotics, DVT prophylaxis) are cornerstones in minimizing these complications. Early identification and appropriate management are key to improving patient outcomes when complications do arise.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is an integral component of successful outcomes following surgery via the medial ankle approach. Protocols are tailored based on the specific procedure performed, the stability of fixation, and the surgeon's preferences. The overarching goals are to protect the repair/reconstruction, minimize swelling and pain, restore range of motion, regain strength, and facilitate a safe return to activity.
General Principles Across Procedures
- Pain and Edema Control:
- Elevation: Continuous elevation of the limb above the heart, especially for the first 48-72 hours, to reduce swelling.
- Ice: Regular application of ice packs (20 minutes on, 20 minutes off) to the surgical site.
- Analgesia: Prescribed oral pain medications, often including NSAIDs (if not contraindicated) and acetaminophen, with short-term opioids as needed.
- Wound Care:
- Keep the incision clean and dry.
- Dressing changes as per surgeon's instructions, typically starting 2-3 days post-op.
- Monitor for signs of infection (redness, warmth, increased pain, purulent drainage).
- Deep Vein Thrombosis (DVT) Prophylaxis:
- Mechanical (foot/calf pumps) and/or chemical (low molecular weight heparin) prophylaxis as per institutional protocols and patient risk factors.
Procedure-Specific Rehabilitation Phases
1. Medial Malleolar Fracture Fixation
Phase I: Immediate Postoperative (Weeks 0-2)
* Immobilization: Short leg cast or cam walker boot, non-weight-bearing (NWB).
* Activities: Toe wiggles (within pain limits), gentle ankle pumping exercises to promote circulation.
* Goals: Protect fixation, control pain and swelling.
Phase II: Early Mobilization (Weeks 2-6)
* Immobilization: Continue cam walker boot.
* Weight Bearing: Gradual progression from NWB to partial weight-bearing (PWB) in the boot, as tolerated, often starting around week 4-6, depending on fracture stability and surgeon preference.
* Activities: Initiate gentle active and passive ankle range of motion (ROM) exercises (dorsiflexion, plantarflexion, inversion, eversion) out of the boot. Non-weight-bearing strengthening (e.g., isometric exercises).
* Goals: Restore initial ROM, prevent stiffness, initiate muscle activation.
Phase III: Strengthening and Proprioception (Weeks 6-12)
* Weight Bearing: Progress to full weight-bearing (FWB) in the boot, then transition to supportive shoe.
* Activities: Progressive strengthening exercises (thera-band, calf raises), balance and proprioceptive training (single leg stance, wobble board). Cycling, swimming.
* Goals: Restore full pain-free ROM, improve strength, enhance stability.
Phase IV: Return to Activity (Weeks 12+)
* Activities: Gradual return to impact activities and sport-specific training. Jumping, running drills. Continue strength and conditioning.
* Goals: Full return to desired activity level, minimize risk of re-injury.
2. Ankle Arthrodesis
Phase I: Immediate Postoperative (Weeks 0-6)
* Immobilization: NWB in a bulky dressing or short leg cast. Some surgeons may use an external fixator for initial stability.
* Activities: Isometric exercises of quadriceps and hamstrings, crutch training.
* Goals: Achieve solid fusion, control pain and swelling, protect surgical site.
Phase II: Progressive Weight Bearing (Weeks 6-12)
* Immobilization: Transition to a removable cast boot or brace.
* Weight Bearing: Initiate PWB in the boot/brace, gradually progressing to FWB over several weeks, guided by radiographic evidence of healing.
* Activities: Gentle gait training with assistive devices. Focus on maintaining knee and hip ROM.
* Goals: Promote bone healing, regain independence with mobility.
Phase III: Functional Recovery (Weeks 12-24+)
* Weight Bearing: FWB in supportive shoe.
* Activities: Progressive strengthening of lower extremity muscles, balance training, gait retraining to accommodate fused ankle. Emphasis on compensatory motions in adjacent joints.
* Goals: Optimize functional gait, improve strength and endurance, manage compensatory biomechanics.
* Long-term: Continue with appropriate footwear and activity modification.
3. Osteochondral Lesion (OCL) Repair/Microfracture
Phase I: Immediate Postoperative (Weeks 0-2/4)
* Immobilization: NWB in a short leg cast or cam walker boot.
* Activities: NWB ROM exercises (if stable fixation), continuous passive motion (CPM) device often used to promote cartilage healing.
* Goals: Protect the healing cartilage, minimize stiffness.
Phase II: Gradual Weight Bearing (Weeks 2/4-8)
* Weight Bearing: PWB with crutches in a boot, gradually increasing.
* Activities: Gentle, controlled active and passive ROM. Low-impact aerobic exercises (e.g., stationary bike without resistance).
* Goals: Progress weight-bearing, restore ROM without stressing repair.
Phase III: Strengthening and Proprioception (Weeks 8-16)
* Weight Bearing: FWB, transition to supportive shoe.
* Activities: Progressive strengthening, balance training. Low-impact activities, gradually increasing intensity.
* Goals: Restore strength, proprioception, and endurance.
Phase IV: Advanced Activity (Weeks 16+)
* Activities: Return to sport-specific training. Gradual progression to higher impact activities, guided by symptoms and healing.
* Goals: Full return to desired activity level while protecting the healing cartilage.
Throughout all protocols, communication between the surgeon, physical therapist, and patient is paramount to adjust the rehabilitation plan based on individual progress and any encountered challenges.
Summary of Key Literature and Guidelines
The medial ankle approach remains a cornerstone in orthopedic foot and ankle surgery, supported by a wealth of literature emphasizing its efficacy and safety when applied to appropriate indications. Recent advances have focused on refining techniques and optimizing patient outcomes, integrating evidence-based practices into rehabilitation protocols.
Key Principles from Literature
- Anatomic Reduction of Fractures: Numerous studies, dating back decades, underscore the critical importance of anatomical reduction and stable internal fixation for medial malleolar fractures. Displaced medial malleolar fractures, if not anatomically reduced, significantly increase the risk of post-traumatic ankle arthritis and instability. Early surgical intervention for displaced fractures typically yields superior long-term functional outcomes compared to non-operative management.
- Osteochondral Lesion Management: For OCLs of the medial talus, the literature supports a staged approach. Smaller, stable lesions may respond to conservative measures, but larger or symptomatic lesions often require surgical intervention. Microfracture, while effective for stimulating fibrocartilage repair, is increasingly being augmented or superseded by techniques like autologous chondrocyte implantation (ACI) or osteochondral autograft/allograft transplantation (OATS) for larger defects, aiming for hyaline-like cartilage repair and improved durability. Long-term follow-up studies continue to evaluate the durability of these various cartilage repair techniques.
- Ankle Arthrodesis: For end-stage ankle arthritis, ankle arthrodesis via the medial approach provides a reliable method for achieving pain relief and stable fusion, particularly in patients with high demand or contraindications to total ankle arthroplasty. The literature consistently reports high fusion rates (typically >90%) and significant pain reduction. Key technical considerations include thorough debridement of articular cartilage, preparation of bleeding cancellous surfaces, appropriate joint positioning (neutral dorsiflexion, slight valgus), and robust internal fixation. Outcomes may be influenced by patient comorbidities, pre-existing deformity, and bone quality.
- Deltoid Ligament Repair: The role of acute deltoid ligament repair, particularly in the context of bimalleolar or trimalleolar fractures, is debated. However, many surgeons advocate for primary repair of avulsed or severely disrupted deltoid ligaments to restore medial stability and prevent chronic instability, especially in high-demand patients. The medial approach provides excellent access for direct repair.
Professional Guidelines and Consensus Statements
- AAOS (American Academy of Orthopaedic Surgeons): Clinical practice guidelines for ankle fractures emphasize the need for anatomical reduction and stable fixation for unstable ankle fractures, including those involving the medial malleolus, to minimize the risk of post-traumatic arthritis.
- AOFAS (American Orthopaedic Foot & Ankle Society): Provides consensus statements and educational resources that guide the management of various foot and ankle pathologies, often referencing the medial approach for specific conditions. These guidelines highlight individualized patient assessment and procedure-specific rehabilitation protocols.
- International Consensus Group on Cartilage Repair of the Ankle (ICAR): Offers comprehensive recommendations for the diagnosis and treatment of osteochondral lesions of the ankle, including indications for surgical intervention via approaches like the medial malleolar osteotomy or direct medial approach, and various repair techniques.
Current Trends and Future Directions
Current trends in medial ankle surgery include a push towards minimally invasive techniques where appropriate (e.g., arthroscopic treatment of smaller OCLs, arthroscopic-assisted arthrodesis), though the open medial approach remains essential for complex trauma, larger lesions, and significant deformities. Research continues into biological augmentation strategies for OCL repair, such as scaffold-based therapies and growth factor application, as well as advancements in implant technology for fracture fixation and arthrodesis. The understanding of patient-specific outcomes and risk stratification is also continuously evolving, allowing for more tailored surgical and rehabilitation plans.
In conclusion, the medial ankle approach is a time-tested and indispensable technique in orthopedic foot and ankle surgery. Mastery of its anatomical nuances, precise surgical steps, and diligent postoperative management, guided by contemporary literature and professional guidelines, are paramount for achieving optimal clinical outcomes.
Clinical & Radiographic Imaging