Ankle Fractures Dislocations: Expert Diagnosis, Treatment & Outcomes
Key Takeaway
We review everything you need to understand about Ankle Fractures Dislocations: Expert Diagnosis, Treatment & Outcomes. Ankle fractures dislocations are common skeletal injuries, frequently involving the lateral malleolus, and typically result from external rotation with the foot supinated. Achieving anatomic reduction is the most crucial factor for a satisfactory outcome. Operative intervention for posterior malleolar fractures is often indicated if there is >25% involvement or >2mm step-off, which is vital for joint stability.
Introduction and Epidemiology
Ankle fractures and fracture-dislocations represent one of the most common skeletal injuries encountered by orthopedic surgeons, accounting for nearly 10% of all fractures. The incidence is approximately 187 per 100,000 people annually, exhibiting a bimodal distribution. Peak incidences occur in young males secondary to high-energy trauma or sports-related injuries, and in older females secondary to low-energy falls associated with osteoporosis.
The lateral malleolus is the most commonly fractured osseous structure in the ankle. Fractures of the malleoli are predominantly caused by rotational mechanisms, with the most common mechanism being external rotation with the foot in a supinated position. Achieving anatomic reduction is universally considered the most critical factor for ensuring a satisfactory long-term clinical and radiographic outcome. Even minor deviations in the anatomic restoration of the ankle mortise can lead to significantly altered contact stresses across the tibiotalar joint, precipitating early-onset post-traumatic osteoarthritis.
Classification Systems
Understanding fracture morphology and the mechanism of injury is essential for preoperative planning. The two primary classification systems utilized are the Danis-Weber classification and the Lauge-Hansen classification.
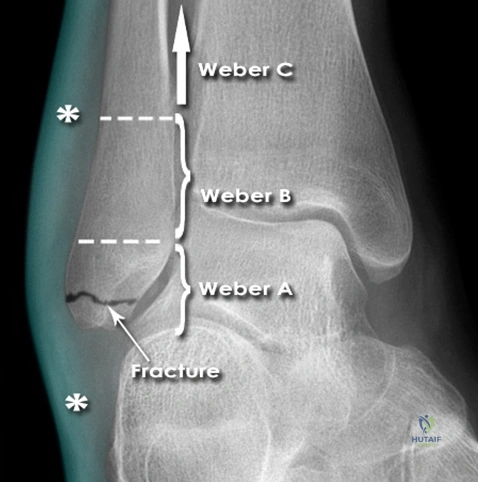
The Danis-Weber classification is based entirely on the location of the fibular fracture relative to the syndesmosis.
* Weber A fractures occur distal to the level of the tibial plafond and are typically avulsion injuries.
* Weber B fractures occur at the level of the syndesmosis and often involve partial or complete syndesmotic disruption.
* Weber C fractures occur proximal to the syndesmosis and are universally associated with syndesmotic disruption.
The Lauge-Hansen classification is based on the position of the foot at the time of injury (supination or pronation) and the direction of the deforming force (external rotation, adduction, or abduction). The Supination-External Rotation (SER) pattern is the most common, accounting for 40% to 70% of all ankle fractures. The sequence of failure in an SER injury progresses from the anterior inferior tibiofibular ligament (AITFL), to a short oblique/spiral fracture of the lateral malleolus, followed by the posterior inferior tibiofibular ligament (PITFL) or posterior malleolus, and finally the medial malleolus or deltoid ligament.
Radiographic Presentation of Weber A Fractures
To illustrate a classic low-energy rotational injury, consider the presentation of a twisting ankle injury. The anteroposterior (AP) radiograph demonstrates characteristic findings of a Weber A fracture.
In this presentation, there is a transverse fracture of the fibular tip located strictly distal to the ankle joint line. Significant soft tissue swelling is typically noted laterally. Because the fracture is distal to the syndesmosis, the ankle mortise remains anatomically aligned, and the syndesmotic ligaments remain intact.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous and ligamentous anatomy of the ankle is prerequisite for anatomic reduction and stable internal fixation. The ankle joint is a highly congruent, modified hinge joint composed of the distal tibia, distal fibula, and the talus.
Osseous Anatomy
The distal tibia forms the superior and medial borders of the ankle mortise. The distal tibial articular surface, or plafond, articulates with the talar dome. The medial malleolus is the medial projection of the distal tibia and is divided into an anterior colliculus and a posterior colliculus, separated by the intercollicular groove. The anterior colliculus is larger and extends further distally than the posterior colliculus. The posterior malleolus is the posterior flare of the distal tibia, and its integrity is vital for posterior joint stability and preventing posterior subluxation of the talus.
The distal fibula forms the lateral malleolus, which functions as the lateral buttress of the ankle mortise. The lateral malleolus exhibits a lateral flare and is positioned more posterior and distal than the medial malleolus. The medial surface of the distal fibula articulates with the lateral aspect of the talus. The incisura fibularis is a concave groove along the distal lateral tibia in which the fibula lies, forming the syndesmotic articulation.
Ligamentous Anatomy
The stability of the ankle mortise relies heavily on its ligamentous complexes. The medial collateral ligament, or deltoid ligament, is divided into superficial and deep components. The superficial deltoid ligament originates primarily from the anterior colliculus and resists hindfoot eversion. The deep deltoid ligament originates from the posterior colliculus and the intercollicular groove, inserting heavily onto the medial talus; it is the primary medial stabilizer against lateral talar shift and external rotation of the talus.
The lateral collateral ligament complex consists of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). These structures resist inversion and anterior translation of the talus.
The syndesmotic ligamentous complex stabilizes the distal tibiofibular articulation and consists of four primary structures. These include the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the transverse tibiofibular ligament (TTFL), and the interosseous ligament (IOL), which is the distal continuation of the interosseous membrane.
Compartmental Anatomy of the Leg
Surgical approaches to the ankle require navigating the muscular and neurovascular compartments of the lower leg. The leg is divided into four distinct compartments.
* Anterior Compartment contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius, innervated by the deep peroneal nerve and supplied by the anterior tibial vessels.
* Lateral Compartment contains the peroneus longus and peroneus brevis, innervated by the superficial peroneal nerve.
* Superficial Posterior Compartment contains the gastrocnemius, soleus, and plantaris muscles.
* Deep Posterior Compartment contains the flexor digitorum longus, flexor hallucis longus, and tibialis posterior, innervated by the tibial nerve and supplied by the posterior tibial vessels.
Biomechanics of the Ankle Mortise
The biomechanics of the ankle joint are dictated by the unique trapezoidal shape of the talar dome, which is wider anteriorly than posteriorly. During dorsiflexion, the wider anterior portion of the talus engages the mortise, forcing the fibula laterally and into external rotation to accommodate the talus. Conversely, in plantarflexion, the narrower posterior talus occupies the mortise, and the talar dome rotates internally due to the checkrein action of the intact deltoid ligament.
Normal range of motion (ROM) of the ankle joint encompasses 30 degrees of dorsiflexion and 45 degrees of plantarflexion. The minimum functional ROM required for a normal gait cycle is 10 degrees of dorsiflexion to 20 degrees of plantarflexion. The axis of rotation of the ankle joint is not purely coronal; it is externally rotated approximately 20 degrees compared to the coronal axis of the knee.
Indications and Contraindications
The decision to proceed with operative versus non-operative management hinges on the stability of the ankle mortise, patient comorbidities, and the specific fracture pattern. Anatomic reduction is the paramount goal, as a talar shift of merely 1 millimeter decreases the tibiotalar contact area by 42%, exponentially increasing peak contact stresses and the risk of post-traumatic arthritis.
| Parameter | Operative Indications | Non Operative Indications |
|---|---|---|
| Fracture Displacement | Any displacement of the medial malleolus; lateral malleolus displacement > 3mm. | Undisplaced fractures with an intact and stable mortise. |
| Mortise Stability | Talar shift; widened medial clear space (> 4mm); syndesmotic diastasis. | Normal medial clear space; symmetric mortise on stress radiographs. |
| Posterior Malleolus | Involvement of > 25% of the articular surface; > 2mm articular step-off; posterior talar subluxation. | Small avulsion fractures (< 25%) with a congruent joint and no step-off. |
| Fracture Pattern | Bimalleolar fractures; Trimalleolar fractures; Bosworth fracture-dislocations; Weber C fractures. | Isolated, undisplaced Weber A or Weber B fractures with no deltoid injury. |
| Soft Tissue Status | Open fractures (emergent); impending skin necrosis from dislocation. | Severe peripheral vascular disease; active localized infection; non-ambulatory patient (relative). |
Contraindications to immediate internal fixation include severe soft tissue compromise (fracture blisters, gross edema), active local infection, and critical limb ischemia. In cases of severe soft tissue swelling, temporary spanning external fixation is indicated until the soft tissue envelope improves, typically evidenced by the return of skin wrinkles (the "wrinkle sign").
Pre Operative Planning and Patient Positioning
Thorough preoperative planning requires high-quality orthogonal radiographs, including weight-bearing views when feasible, and advanced imaging for complex fracture patterns.
Radiographic Evaluation
Standard radiographic evaluation includes Anteroposterior (AP), Lateral, and Mortise views. The mortise view is obtained with the leg internally rotated 15 to 20 degrees to profile the tibiotalar articulation.
Critical radiographic measurements must be assessed to determine mortise integrity. The tibiofibular clear space should be measured 1 cm above the joint line; a normal clear space is < 6 mm on both AP and mortise views. The medial clear space, measured between the lateral border of the medial malleolus and the medial border of the talus, should be < 4 mm and symmetric with the superior clear space. The tibiofibular overlap should be > 6 mm on the AP view and > 1 mm on the mortise view.
Advanced Imaging
Computed Tomography (CT) is highly recommended for all trimalleolar fractures to assess the size, comminution, and articular impaction of the posterior malleolus. CT is also invaluable for identifying occult osteochondral lesions of the talus, marginal impaction of the tibial plafond, and the presence of intra-articular loose bodies.
Patient Positioning and Preparation
Patient positioning is dictated by the planned surgical approaches.
* Supine Positioning with a bump under the ipsilateral hip is standard for lateral, medial, and anterior approaches. This position internally rotates the leg, bringing the lateral malleolus into profile while allowing access to the medial malleolus.
* Prone Positioning is strongly preferred when direct reduction and fixation of a large posterior malleolar fragment are required via a posterolateral approach.
* Lateral Decubitus Positioning can also be utilized for isolated posterolateral and lateral access but limits access to the medial malleolus.
A thigh tourniquet is routinely applied to maintain a bloodless surgical field, though its inflation should be minimized in patients with known peripheral arterial disease. Prophylactic intravenous antibiotics are administered 30 minutes prior to incision.
Detailed Surgical Approach and Technique
Surgical management of ankle fractures demands meticulous handling of the delicate soft tissue envelope and rigid internal fixation to allow for early range of motion.
Lateral Malleolus Fixation
The lateral approach to the fibula is the workhorse for lateral malleolar fractures. The incision is made directly lateral or slightly posterolateral over the fibula. The internervous plane lies between the peroneus tertius (deep peroneal nerve) anteriorly and the peroneus brevis (superficial peroneal nerve) posteriorly. Care must be taken to identify and protect the superficial peroneal nerve, which crosses the surgical field anteriorly in the distal third of the leg.
For Weber B fractures (short oblique or spiral), the fracture is reduced anatomically using reduction forceps. Fixation is typically achieved using a 3.5 mm cortical lag screw placed perpendicular to the fracture plane to provide interfragmentary compression. This is followed by the application of a neutralization plate (usually a one-third tubular plate or a 3.5 mm locking compression plate) applied to the lateral or posterolateral surface of the fibula. Posterolateral anti-glide plating is biomechanically superior for resisting the posterior displacement forces acting on the distal fibula and avoids intra-articular screw penetration.
For Weber C fractures, a longer plate is required to span the comminuted or diaphyseal segment. Bridge plating techniques may be employed to preserve the fracture hematoma and periosteal blood supply in highly comminuted patterns.
Medial Malleolus Fixation
The medial approach utilizes a longitudinal or gently curved incision centered over the medial malleolus. The saphenous nerve and great saphenous vein must be identified and retracted anteriorly.
The fracture site is debrided of interposed periosteum or organizing hematoma. The medial malleolus is reduced and provisionally held with smooth Kirschner wires. Fixation is most commonly achieved with two parallel 4.0 mm partially threaded cancellous screws. The screws should be directed perpendicular to the fracture line. In cases of small avulsion fragments or severe comminution, a tension band wiring technique or a small medial hook plate may be utilized to provide stable fixation.
Posterior Malleolus Fixation
A posterior malleolar fracture with > 25% articular involvement or > 2 mm step-off is an operative indication. The posterolateral approach is performed with the patient prone. The incision is made between the lateral border of the Achilles tendon and the posterior border of the fibula. The sural nerve and lesser saphenous vein must be protected.
The deep dissection involves retracting the peroneal tendons laterally and the flexor hallucis longus (FHL) medially. This exposes the posterior tibia. The posterior malleolar fragment is typically attached to the PITFL. Direct reduction of the articular surface is performed, and fixation is achieved using anteriorly directed lag screws or a posterior buttress plate. Posterior plating provides superior biomechanical stability compared to anterior-to-posterior lag screws.
Syndesmotic Evaluation and Fixation
Following osseous fixation, the syndesmosis must be evaluated for instability. Intraoperative stress testing is performed using the external rotation stress test or the lateral pull test (Cotton test) under fluoroscopy. Widening of the tibiofibular clear space or medial clear space indicates syndesmotic incompetence.
If unstable, the syndesmosis is reduced with the ankle in neutral dorsiflexion. Reduction forceps are applied across the medial and lateral malleoli. Fixation is achieved using one or two 3.5 mm or 4.5 mm cortical screws placed parallel to the joint line, engaging three or four cortices. Alternatively, dynamic fixation using suture button constructs (e.g., TightRope) has gained popularity. Suture buttons allow for physiologic micro-motion of the syndesmosis, potentially reducing the risk of malreduction and eliminating the need for routine hardware removal.
Complications and Management
Despite meticulous surgical technique, complications following ankle fracture fixation remain a significant clinical challenge. The delicate soft tissue envelope and the high articular congruency of the mortise contribute to specific post-operative morbidities.
Osteochondral Lesions of the Talus
Osteochondral lesions of the talus (OLT) are frequently missed concomitant injuries. They are believed to occur after 2% to 6% of all ankle sprains and a significantly higher percentage of rotational ankle fractures. The shearing forces generated during talar subluxation cause impaction or avulsion of the talar articular cartilage and subchondral bone.
Consider the clinical scenario of a patient presenting with persistent, unexplained chronic ankle pain following a seemingly healed or "negative" initial injury.

In this presentation, there is a distinct loss of the normal talar dome cortex contour due to an osteochondral fracture. Patients with unexplained chronic ankle pain have been shown to have osteochondral lesions in up to 81% of cases when evaluated with advanced imaging (MRI or CT).
Treatment initially is non-operative, focusing on immobilization, non-steroidal anti-inflammatory drugs (NSAIDs), and physical therapy. Non-operative treatment has a reported success rate of 45% to 50%. Persistent symptoms are treated operatively, yielding better results. Arthroscopic procedures involving fragment excision, debridement, and bone marrow stimulation (microfracture) have been shown to have an 87% success rate for lesions smaller than 1.5 cm squared. Larger or cystic lesions may require osteochondral autograft transfer (OATS) or matrix-induced autologous chondrocyte implantation (MACI).
Summary of Common Complications
| Complication | Estimated Incidence | Salvage and Management Strategy |
|---|---|---|
| Post Traumatic Osteoarthritis | 10% - 40% | Initial conservative management (bracing, injections). Surgical salvage includes ankle arthrodesis or total ankle arthroplasty for end-stage disease. |
| Wound Dehiscence and Infection | 2% - 5% | Superficial infections managed with oral antibiotics. Deep infections require aggressive surgical debridement, hardware removal (if fracture is healed or unstable), and targeted IV antibiotics. |
| Syndesmotic Malreduction | Up to 16% | Revision open reduction and internal fixation (ORIF) if identified early. Late presentations may require syndesmotic arthrodesis. |
| Nonunion | 1% - 3% | Optimization of host factors (smoking cessation, glycemic control). Revision ORIF with autologous bone grafting and rigid fixation. |
| Sural or Superficial Peroneal Nerve Injury | 5% - 10% | Often transient neuropraxia. Persistent symptomatic neuromas may require surgical excision and burying of the nerve stump into adjacent muscle or bone. |
Post Operative Rehabilitation Protocols
Rehabilitation following ankle fracture fixation is phased, balancing the need for tissue healing with the prevention of joint stiffness and muscle atrophy. Protocols vary based on fracture stability, bone quality, and patient compliance.
Phase One Immediate Post Operative
The primary goals in the first 0 to 2 weeks are wound healing, edema control, and pain management. The patient is typically placed in a well-padded short leg splint or a bulky Jones dressing. The patient is instructed to remain strictly non-weight-bearing (NWB) on the operative extremity. Elevation of the limb above the level of the heart is emphasized to mitigate swelling and reduce the risk of wound dehiscence.
Phase Two Early Mobilization
At the 2-week postoperative mark, sutures are removed provided the surgical incisions are fully healed. For patients with stable fixation and reliable compliance, the splint is transitioned to a removable controlled ankle motion (CAM) boot.
Active range of motion exercises out of the boot are initiated. Patients are instructed to perform dorsiflexion and plantarflexion exercises, aiming to restore the minimum functional ROM (-10 to 20 degrees). Inversion and eversion are generally restricted if a syndesmotic repair or medial malleolar fixation was performed. Weight-bearing status remains restricted, typically NWB or touch-down weight-bearing (TDWB) depending on surgeon preference and fracture comminution.
Phase Three Weight Bearing and Strengthening
At 6 weeks postoperatively, radiographic evaluation is performed to assess for callus formation and maintenance of mortise reduction. If clinical and radiographic signs of healing are present, patients are progressively transitioned to full weight-bearing (FWB) in the CAM boot, and eventually to standard supportive footwear by 8 to 10 weeks.
Physical therapy is intensified during this phase. Strengthening exercises for the peroneal, tibial, and gastrocnemius-soleus complexes are initiated. Proprioceptive training using balance boards is critical for restoring dynamic ankle stability and preventing recurrent falls.
Phase Four Return to Activity
Return to high-impact activities, heavy labor, or competitive sports is generally permitted between 4 to 6 months postoperatively. Clearance is contingent upon the restoration of symmetric ankle ROM, lower extremity strength > 90% of the contralateral side, and the ability to perform sport-specific agility drills without pain or reactive effusion.
Summary of Key Literature and Guidelines
The foundational principles of ankle fracture management are heavily derived from classical biomechanical and clinical studies.
The Lauge-Hansen classification, published in 1950, remains the cornerstone for understanding the mechanism of injury and predicting the sequence of ligamentous and osseous failure. Although its inter-observer reliability has been debated, it provides an invaluable framework for closed reduction maneuvers, which reverse the mechanism of injury.
The biomechanical imperative for anatomic reduction was definitively established by Ramsey and Hamilton in 1976. Their seminal cadaveric study demonstrated that a lateral talar shift of merely 1 mm results in a 42% decrease in tibiotalar contact area. This foundational data underscores the strict operative indications for any displacement that compromises the medial clear space.
Recent literature has heavily focused on the management of the syndesmosis. The traditional paradigm of rigid cortical screw fixation followed by routine hardware removal has been challenged by the advent of dynamic suture button constructs. Multicenter randomized controlled trials have demonstrated that suture button fixation yields equivalent, if not superior, functional outcomes compared to screw fixation, with a significantly lower rate of symptomatic hardware requiring secondary removal operations. Furthermore, the use of intraoperative 3D fluoroscopy or CT has been shown to significantly reduce the unacceptably high historical rates of syndesmotic malreduction.
Clinical & Radiographic Imaging
