Acute Ankle Fractures in Diabetic Patients: Advanced Surgical Management and Fixation Strategies

Key Takeaway
The operative management of acute ankle fractures in diabetic patients demands rigorous preoperative optimization and augmented surgical fixation. Due to the high risk of Charcot neuroarthropathy and wound complications, surgeons must employ robust constructs, including locking plates, multiple syndesmotic screws, and transarticular tibiotalar pinning. Postoperative protocols require extended immobilization and strict glycemic control to achieve a stable, plantigrade foot and prevent devastating morbidity or amputation.
Comprehensive Introduction and Patho-Epidemiology
The management of acute ankle and foot fractures in patients with diabetes mellitus represents one of the most formidable and unforgiving challenges in modern orthopedic traumatology. As the global prevalence of diabetes continues to surge, orthopedic surgeons are increasingly confronted with complex lower extremity trauma in this highly vulnerable patient population. Because operative treatment inherently carries precipitously higher complication rates in diabetic patients—especially those with compounding comorbidities such as peripheral arterial disease (PAD), peripheral neuropathy, and chronic kidney disease—it is frequently tempting for the uninitiated surgeon to treat these fractures nonoperatively. However, this conservative approach is fraught with peril. The "diabetic paradox" in ankle trauma dictates that while surgical intervention carries an undeniably high risk of wound complications and deep infection, nonoperative management in the presence of peripheral neuropathy carries a near-certainty of devastating mechanical failure, progressive deformity, and ultimately, limb loss.
Acute ankle fractures in the neuropathic diabetic patient must therefore be approached with a resolute bias toward operative fixation, utilizing biomechanical principles that are vastly more robust than those applied to nondiabetic patients. Nonoperative treatment frequently leads to catastrophic loss of reduction, insensate skin sloughing, deep ulceration, and the rapid, unchecked onset of Charcot neuroarthropathy. The pathophysiology underpinning this phenomenon is multifactorial. Peripheral neuropathy strips the patient of protective sensation and proprioception, leading to unrecognized repetitive microtrauma and the inability to effectively offload the injured extremity. Autonomic neuropathy shunts blood away from the nutrient capillaries through arteriovenous anastomoses, causing a hyperemic state that paradoxically starves the bone of essential nutrients while simultaneously increasing osteoclastic activity and driving profound localized osteopenia.
Furthermore, the cellular environment in the diabetic patient is fundamentally hostile to both bone and soft tissue healing. Chronic hyperglycemia leads to the accumulation of advanced glycation end-products (AGEs), which detrimentally cross-link type I collagen in bone and soft tissues, rendering the bone brittle and the soft tissue envelope inelastic and prone to necrosis. Impaired leukocyte function, specifically diminished chemotaxis and phagocytosis, exponentially increases the risk of surgical site infections. Consequently, the orthopedic surgeon must view the diabetic ankle fracture not merely as a mechanical disruption of the osseous mortise, but as a complex systemic emergency requiring meticulous preoperative optimization, aggressive and augmented surgical stabilization, and prolonged, highly specialized postoperative care.
The epidemiological data surrounding diabetic ankle fractures underscore the gravity of the condition. Diabetic patients with ankle fractures experience complication rates that are three to five times higher than their non-diabetic counterparts. The risk of major limb amputation following an operatively treated ankle fracture in a diabetic patient with neuropathy and nephropathy can approach 15-20% in some series, compared to less than 1% in healthy patients. Recognizing these stark realities, the contemporary standard of care demands an evolution from traditional AO techniques to advanced, augmented fixation strategies designed to withstand the unique biomechanical and biological demands of the diabetic lower extremity.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of both the vascular anatomy and the altered biomechanics of the diabetic lower extremity is an absolute prerequisite for successful surgical intervention. The soft tissue envelope surrounding the ankle mortise is notoriously thin, with the distal tibia and fibula lying strictly subcutaneous. In the diabetic patient, this tenuous envelope is further compromised by microvascular disease. Surgical approaches must therefore be meticulously planned according to the angiosome concept. The medial malleolus and medial soft tissues are supplied primarily by the posterior tibial artery via its calcaneal and malleolar branches, while the lateral malleolus is supplied by the peroneal artery. Transgressing these angiosomes with poorly planned incisions, or elevating extensive subcutaneous flaps that shear the delicate perforating vessels, will inevitably precipitate full-thickness wound necrosis. Full-thickness fasciocutaneous flaps, elevated directly off the periosteum without undermining, are mandatory to preserve the dermal capillary plexus.
Biomechanically, the diabetic ankle presents a perfect storm of structural compromise. Standard AO principles of internal fixation, which rely on the compression of healthy cortical bone and the patient's compliance with weight-bearing restrictions, are frequently insufficient. The combination of profound osteopenia, impaired cellular healing, and the patient's absolute inability to protect the extremity due to loss of proprioception and pain sensation demands augmented fixation techniques. The forces transmitted across the tibiotalar joint during normal ambulation can exceed four to five times body weight; in the insensate patient, these forces are often magnified by an altered, uncoordinated gait pattern and early, inadvertent weight-bearing.
To counteract these immense destructive forces, the "Diabetic Construct" must be engineered with maximal rigidity and fatigue resistance. Locking plate technology is the cornerstone of this approach. Fixed-angle constructs are essential to prevent screw toggle, sequential screw pullout, and catastrophic construct failure in osteopenic bone. Furthermore, the working length of the plate must be significantly increased. Plates should be substantially longer than standard, utilizing multiple cortices well proximal to the fracture zone to dissipate stress over a larger area of the tibial or fibular diaphysis, thereby preventing peri-implant fractures at the proximal terminus of the hardware.
Equally critical is the management of the distal tibiofibular syndesmosis. Even in the absence of frank syndesmotic instability on preoperative imaging, the syndesmosis in a neuropathic diabetic patient should be prophylactically stabilized. The standard paradigm of utilizing one or two tricortical screws is inadequate. Augmented fixation requires multiple (typically three or four) quadricortical screws to rigidly reinforce the mortise and prevent late diastasis. Unlike in healthy patients, these syndesmotic screws are generally not removed, serving as permanent internal splints. In severe fracture-dislocations or in highly noncompliant neuropathic patients, supplemental transarticular fixation with heavy Kirschner wires, Steinmann pins, or even retrograde intramedullary nails driven across the tibiotalar and subtalar joints provides critical temporary or permanent stability, neutralizing the deforming forces of the Achilles tendon and protecting the tenuous internal fixation.
Exhaustive Indications and Contraindications
The decision-making matrix for treating acute ankle fractures in diabetic patients requires a delicate balancing act between the imperative for rigid mechanical stability and the severe risks of soft tissue necrosis and deep infection. The indications for surgery are significantly broader in this population due to the unacceptable natural history of nonoperative management. However, the contraindications must be strictly respected to avoid precipitating an iatrogenic amputation.
| Clinical Scenario / Parameter | Indications for Operative Intervention (Augmented Fixation) | Absolute or Relative Contraindications |
|---|---|---|
| Fracture Pattern | Displaced bimalleolar, trimalleolar, or syndesmotic equivalent fractures; any fracture with mortise widening; acute Charcot mimicking fracture. | Nondisplaced, stable unimalleolar fractures in compliant patients (Relative contraindication for surgery; requires close TCC monitoring). |
| Neurologic Status | Presence of peripheral neuropathy (requires augmented/super-construct fixation due to insensate limb). | Severe, unmanageable psychiatric illness or absolute refusal to adhere to postoperative non-weight-bearing protocols (Relative). |
| Vascular Status | Palpable pulses, ABI > 0.9, TBI > 0.3, Toe pressure > 40 mmHg, transcutaneous oxygen (TcPO2) > 40 mmHg. | Uncorrectable severe ischemia (ABI < 0.5, TBI < 0.2, TcPO2 < 20 mmHg). Revascularization must precede bone fixation. |
| Soft Tissue Envelope | Intact skin, manageable fracture blisters (blood-filled blisters require delayed approach or percutaneous techniques). | Active deep infection, gross purulence, osteomyelitis, or uncorrectable severe soft tissue necrosis (Absolute contraindication for internal fixation). |
| Glycemic Control | Perioperative glucose 140-180 mg/dL. HbA1c < 8.0% is ideal but acute fractures cannot wait for long-term HbA1c correction. | Extreme, uncontrolled diabetic ketoacidosis or hyperosmolar hyperglycemic state (Must be medically corrected prior to OR). |
| Charcot Neuroarthropathy | Acute fracture in a pre-existing Charcot foot, or acute Charcot collapse threatening the viability of the limb. | Active, untreated deep space infection in the setting of Charcot (Requires staged external fixation and debridement). |
The indications for augmented internal fixation encompass nearly all displaced ankle fractures in the diabetic population. The presence of neuropathy is not a contraindication to surgery; rather, it is the primary indication for upgrading the surgical construct from standard AO fixation to a "super-construct." Percutaneous fixation techniques are indicated when the soft tissue envelope is too compromised to permit standard incisions, yet the fracture demands stabilization to prevent pressure necrosis from displaced bone fragments. Primary tibiotalocalcaneal (TTC) arthrodesis is indicated in cases of severe, highly comminuted fractures in elderly neuropathic patients where the articular cartilage is unsalvageable, or in cases of acute-on-chronic Charcot neuroarthropathy where massive bone loss precludes standard ORIF.
Contraindications center primarily on inadequate perfusion and active infection. Operating on a dysvascular limb without prior vascular surgical consultation and intervention is a direct path to wound dehiscence and amputation. An Ankle-Brachial Index (ABI) can be falsely elevated in diabetics due to medial arterial calcification (Mönckeberg's sclerosis); therefore, Toe-Brachial Indices (TBI) and transcutaneous oxygen tension (TcPO2) are mandatory for accurate risk stratification. Internal fixation in the presence of active osteomyelitis or an infected ulcer is strictly contraindicated; these scenarios mandate staged reconstruction utilizing radical debridement, temporary external fixation, and culture-directed antibiotic therapy before any definitive internal stabilization can be considered.
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative optimization and meticulous surgical planning are critical to mitigating the exceptionally high complication rates in this patient cohort. Before proceeding to the operating room, a rapid but exhaustive assessment of the patient's vascular, neurologic, and metabolic status is mandatory. The vascular assessment must go beyond the simple palpation of pulses, as microvascular disease can profoundly impair wound healing despite palpable macrovascular flow. As previously noted, TBI and TcPO2 are the most reliable indicators of healing potential. If the TBI is less than 0.3 or the toe systolic pressure is below 40 mm Hg, emergent vascular surgery consultation for endovascular or open bypass revascularization is required prior to definitive fracture fixation. Temporary stabilization with a spanning external fixator may be necessary while awaiting revascularization.
Neurologic assessment via Semmes-Weinstein monofilament testing dictates the biomechanical strategy. A patient who cannot feel the 5.07 (10-gram) monofilament has lost protective sensation and will inevitably load the surgical construct prematurely. This finding mandates the use of augmented fixation techniques, including longer locking plates and multiple syndesmotic screws. Glycemic control must be aggressively managed by a multidisciplinary team. While the long-term HbA1c is a known predictor of postoperative complications, the acute perioperative glucose management is paramount. Intravenous insulin protocols should be utilized to maintain perioperative blood glucose levels strictly between 140 and 180 mg/dL, as hyperglycemia severely impairs neutrophil function and exponentially increases the risk of surgical site infection.
Radiographic evaluation must include orthogonal views of the ankle, full-length tibia/fibula radiographs to rule out proximal extension, and dedicated foot radiographs to assess for concomitant midfoot Charcot arthropathy. A preoperative Computed Tomography (CT) scan is highly recommended for all diabetic ankle fractures to fully appreciate the extent of articular comminution, identify occult impaction injuries (such as marginal plafond fractures), and accurately template screw trajectories. Templating is a critical step; the surgeon must pre-select locking plates that are significantly longer than those used for standard fractures. For a typical lateral malleolar fracture, a plate that allows for a minimum of five to six bicortical or locking screws proximal to the fracture zone should be templated.
Patient positioning in the operating room must facilitate both precise surgical execution and the protection of the insensate contralateral limb. The patient is typically positioned supine on a radiolucent table with a bump under the ipsilateral hip to internally rotate the leg, bringing the fibula into a neutral position. The contralateral heel and bony prominences must be meticulously padded to prevent iatrogenic pressure ulcers during the procedure. A sterile tourniquet is typically applied to the proximal thigh, but its use should be minimized or entirely avoided in patients with severe peripheral arterial disease to prevent ischemic reperfusion injury. Fluoroscopy must be positioned to allow unobstructed orthogonal views of the entire lower leg, ankle, and foot, ensuring that the extensive hardware required for augmented fixation can be visualized in its entirety.
Step-by-Step Surgical Approach and Fixation Technique
Standard Open Reduction and Internal Fixation
For the typical bimalleolar or trimalleolar equivalent fracture in a diabetic patient without prohibitive soft tissue compromise, a meticulous, soft-tissue-respecting open approach is paramount. The surgical technique must flawlessly integrate augmented fixation principles to prevent construct failure.
Step 1: Positioning and Approach
Following meticulous sterile prep and drape, the standard lateral approach to the fibula and medial approach to the medial malleolus are utilized. The incisions must be carefully planned to avoid transgressing angiosomes. Full-thickness fasciocutaneous flaps are sharply elevated directly off the periosteum. The surgeon must absolutely avoid undermining the subcutaneous tissues, as this shears the delicate perforating vessels and guarantees marginal skin necrosis. Retraction must be gentle, utilizing blunt retractors, and the tissues should be frequently irrigated to prevent desiccation.
Step 2: Fibular Fixation
The fibular fracture is anatomically reduced using pointed reduction forceps, taking care not to crush the osteopenic bone. A long, pre-contoured lateral or posterolateral locking plate is applied. The "diabetic construct" requires that the plate span significantly proximal to the fracture zone, typically utilizing a 7-hole or 9-hole plate for a standard Weber B fracture. At least four to five locking screws must be placed proximal to the fracture to ensure adequate pullout strength and distribute the bending moment across a larger segment of the diaphysis.
Step 3: Medial Malleolar Fixation
The medial malleolus is notoriously difficult to fix in the diabetic patient due to profound cancellous osteopenia. Standard partially threaded cancellous screws frequently fail to achieve adequate purchase and will pull out. Therefore, the medial malleolus is fixed using fully threaded, solid cortical screws that engage the dense bone of the lateral tibial plafond, or ideally, a medial buttress plate (such as a 1/3 tubular plate or dedicated medial distal tibia plate) applied in an antiglide fashion.
Step 4: Syndesmotic and Transarticular Augmentation
Regardless of preoperative stress testing, the syndesmosis in a neuropathic diabetic patient is routinely stabilized to reinforce the mortise. Multiple (three or four) 3.5mm or 4.5mm quadricortical screws are placed parallel to the joint line. If the construct feels tenuous, or if the patient is known to be highly noncompliant, retrograde transarticular pins (heavy Steinmann pins) are driven from the plantar aspect of the calcaneus, through the talus, and into the distal tibia to provide massive temporary stability.
The following preoperative and postoperative radiographs demonstrate the successful application of augmented fixation in a young diabetic patient with a severe bimalleolar fracture-subluxation:


FIGURE 85-25 A and B: Preoperative radiographs of a highly unstable bimalleolar ankle fracture-subluxation in a 19-year-old man with a 12-year history of insulin-dependent diabetes mellitus.

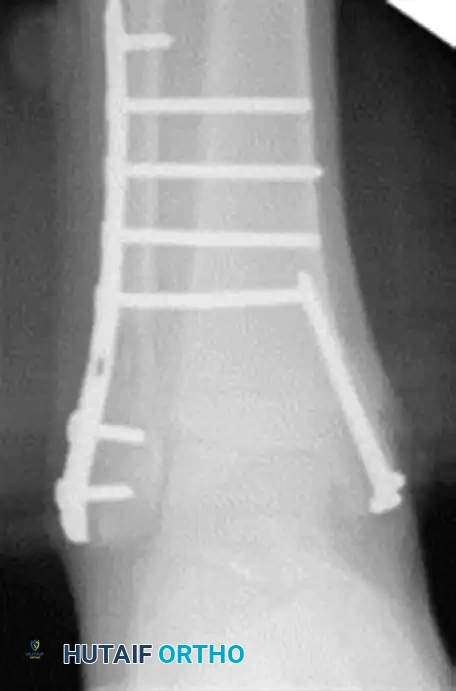
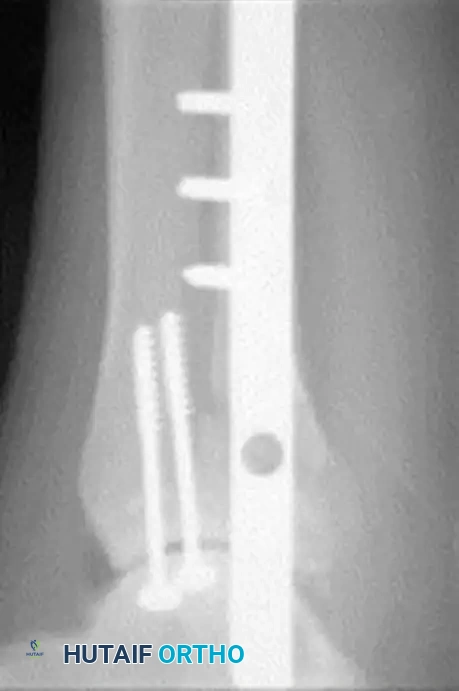
FIGURE 85-25 C-E: Postoperative fixation demonstrating robust fibular plating, medial malleolar screw fixation, and critical supplemental syndesmotic screws to reinforce the mortise.
Percutaneous Fixation Strategies
In patients presenting with severe soft tissue compromise, massive fracture blisters, profound vascular disease, or multiple medical comorbidities where prolonged open incisions carry an unacceptable risk of necrosis or anesthetic death, percutaneous fixation is a highly valuable alternative. This technique prioritizes the preservation of the biological envelope over absolute anatomic reduction of the osseous fragments.
The procedure relies on closed reduction maneuvers under live fluoroscopy. Once an acceptable, length-stable reduction is achieved, strategic placement of percutaneous screws or transarticular pins is performed. Cannulated screw systems are heavily utilized. Small stab incisions are made, and the soft tissues are bluntly spread to the bone to protect neurovascular structures (specifically the superficial peroneal nerve laterally and the saphenous nerve and vein medially). Guide wires are placed across the fracture sites and the syndesmosis, followed by the insertion of fully threaded screws to maximize purchase in osteopenic bone.
While this technique sacrifices the rigid, fixed-angle stability of locking plates, it provides sufficient stability to prevent gross motion, thereby allowing the highly compromised soft tissue envelope to heal without the insult of a massive surgical exposure. Postoperatively, these patients require even more rigorous immobilization, frequently utilizing circular external fixation or immediate total contact casting to supplement the percutaneous hardware.


FIGURE 85-26 A-C: Percutaneous fixation of an ankle fracture in a diabetic patient, utilizing minimally invasive screw placement to stabilize the fracture while respecting a highly compromised soft tissue envelope.
Management of Charcot Neuroarthropathy
Acute fractures in diabetic patients can rapidly degenerate into Charcot neuroarthropathy if not rigidly stabilized. The profound inflammatory cascade associated with the trauma triggers massive osteoclastogenesis, leading to rapid bone resorption and joint destruction. Conversely, patients may present with acute-on-chronic Charcot breakdown mimicking an acute fracture. A critical surgical warning must be heeded: misdiagnosing an acute Charcot event as a simple ankle sprain or standard fracture will lead to catastrophic, irreversible joint destruction. Any diabetic patient presenting with a red, hot, swollen foot must be presumed to have Charcot arthropathy or deep infection until proven otherwise.
Tibiotalocalcaneal (TTC) Arthrodesis
When the ankle joint is unsalvageable due to severe Charcot destruction or massive comminution in an elderly neuropathic patient, realignment and extended fusion are required. A primary Tibiotalocalcaneal (TTC) arthrodesis utilizing a rigid, retrograde intramedullary nail provides a load-sharing construct that is biomechanically far superior to plate fixation in the neuropathic patient.
Surgical Steps for TTC Nailing:
1. Preparation: Through a lateral transfibular or anterior approach, the remaining articular cartilage of the tibiotalar and subtalar joints is aggressively debrided down to bleeding subchondral bone. The fibula is often resected and used as autograft.
2. Alignment: The foot is meticulously positioned in neutral dorsiflexion, 5 degrees of valgus, and 10 to 15 degrees of external rotation. Malalignment in any plane will lead to abnormal pressure distribution and subsequent ulceration.
3. Implantation: A rigid retrograde intramedullary nail is introduced through a plantar incision in the calcaneus, traversing the subtalar and tibiotalar joints, and driven into the tibial canal. Multiple locking screws are placed proximally and distally to secure the construct. Internal compression is applied if the system allows.

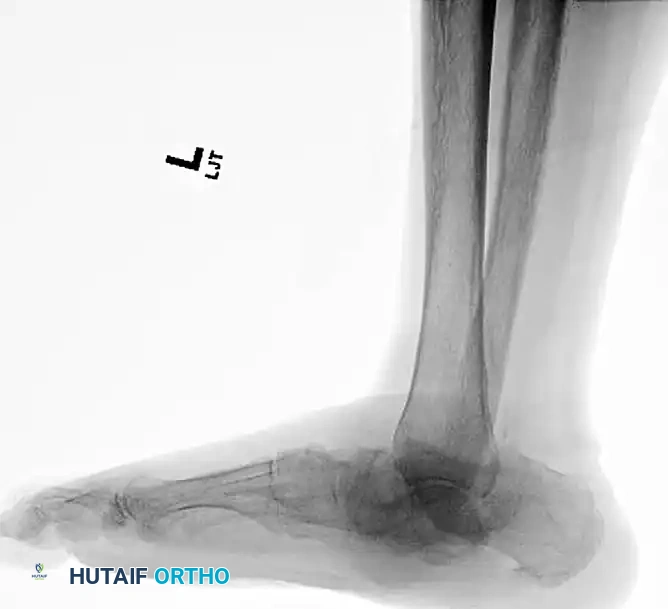
FIGURE 85-20 A and B: Severe Charcot arthropathy of the ankle with profound deformity and joint destruction.

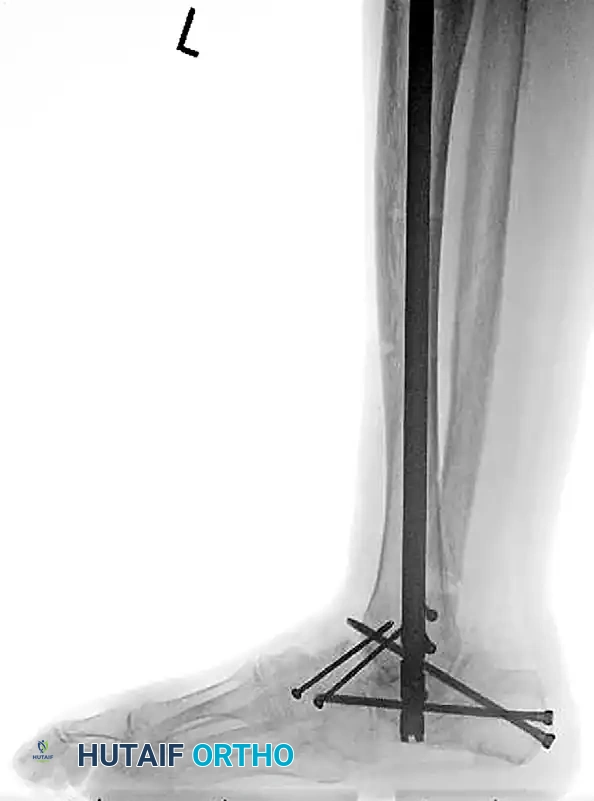
FIGURE 85-20 C and D: Postoperative radiographs following successful tibiotalocalcaneal (TTC) arthrodesis with a rigid retrograde intramedullary nail, restoring a plantigrade alignment.
Charcot Arthropathy with Superimposed Osteomyelitis
The presence of an open ulcer with underlying osteomyelitis in a Charcot ankle is a limb-threatening emergency. Internal fixation is strictly contraindicated in the setting of active infection, as the hardware will inevitably become colonized, leading to a chronic biofilm infection and ultimately, amputation.
Staged Reconstruction Protocol:
1. Radical Debridement: All infected bone, devitalized soft tissue, and sinus tracts must be radically excised. This frequently requires a complete talectomy if the talus is necrotic, fragmented, or heavily infected. The goal is complete source control.
2. External Fixation: Following debridement, a hybrid or Ilizarov fine-wire external fixator is applied. This device spans the massive bone defect, provides rigid stability necessary for soft tissue healing, and allows for daily wound care, vacuum-assisted closure (VAC) application, and eventual soft tissue reconstruction (e.g., free tissue transfer). Once the infection is eradicated (often 6-12 weeks later), definitive internal fusion can be considered.


FIGURE 85-21 A and B: Charcot arthropathy of the ankle complicated by severe osteomyelitis.

FIGURE 85-21 C: Clinical appearance of the foot demonstrating a deep, probing medial ulcer.

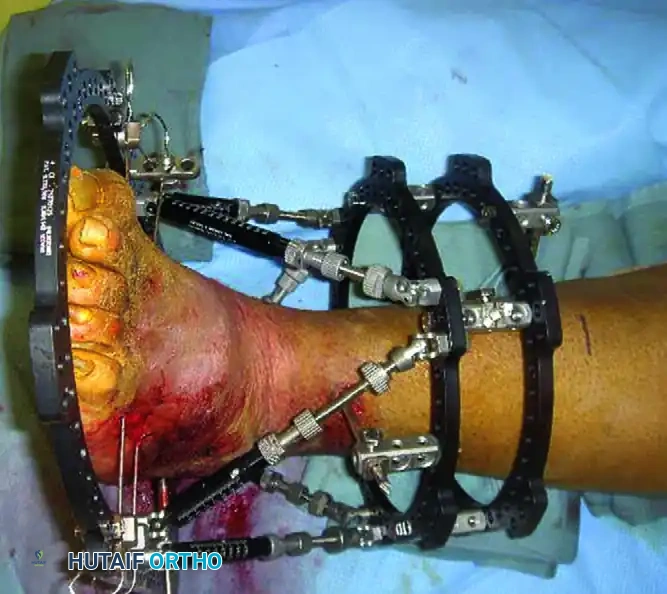
FIGURE 85-21 D and E: Intraoperative removal of the infected, necrotic talus (talectomy) to achieve source control.
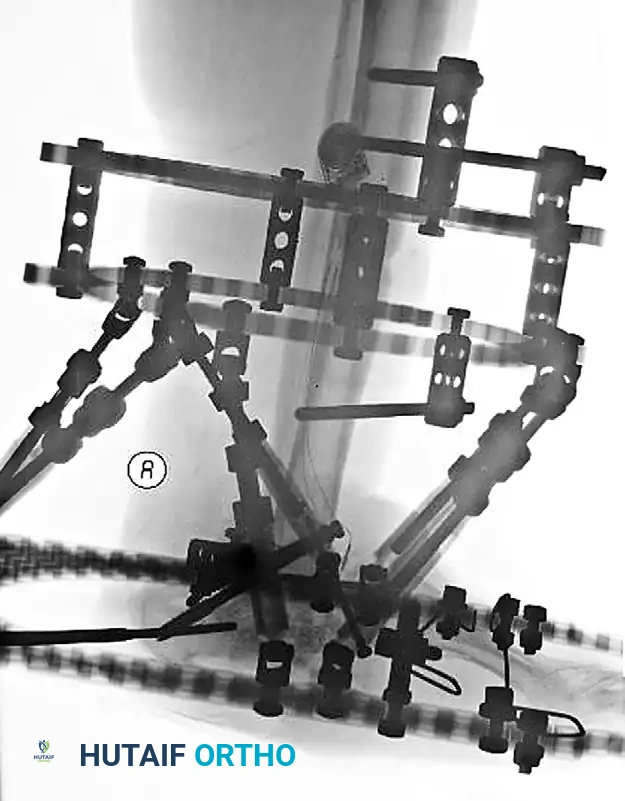
FIGURE 85-21 F: Application of a hybrid external fixator to stabilize the limb and maintain length following talectomy.

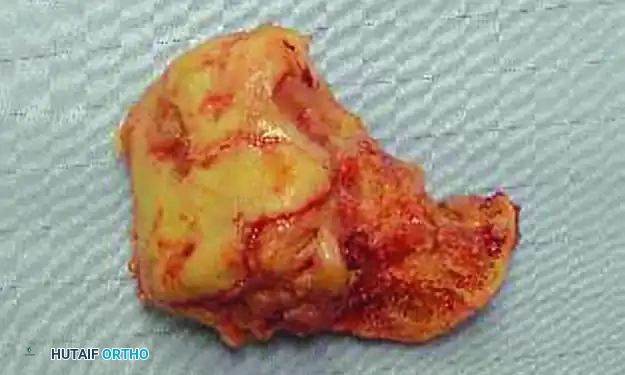
FIGURE 85-21 G and H: Postoperative radiographs showing the hybrid fixator in place, providing rigid stabilization while the soft tissue envelope heals.
Midfoot and Forefoot Charcot Reconstruction
Charcot breakdown is not limited to the ankle mortise; midfoot collapse (producing the classic rocker-bottom deformity) and forefoot destruction are extremely common and frequently accompany hindfoot pathology. Surgical reconstruction in the midfoot is highly complex and often relies on the tension band principle to counteract the massive deforming forces
Clinical & Radiographic Imaging Archive




