Operative Management of Hallux Sesamoid Pathology: Sesamoidectomy and Bone Grafting Techniques
Key Takeaway
Hallux sesamoidectomy is a precise surgical intervention indicated for recalcitrant sesamoiditis, fractures, or nonunions that fail conservative management. The procedure demands meticulous soft tissue handling, particularly the protection of the proper medial plantar nerve, and robust repair of the flexor hallucis brevis tendon to prevent postoperative hallux valgus or varus deformities. Careful patient selection and adherence to strict postoperative rehabilitation protocols are paramount for optimal functional recovery.
INTRODUCTION TO HALLUX SESAMOID PATHOLOGY
The hallux sesamoids play a critical biomechanical role in the function of the first metatarsophalangeal (MTP) joint. Embedded within the tendons of the flexor hallucis brevis (FHB) muscle, the tibial (medial) and fibular (lateral) sesamoids function similarly to the patella in the knee. They absorb weight-bearing forces, reduce friction, protect the flexor hallucis longus (FHL) tendon, and increase the mechanical advantage of the intrinsic musculature during the push-off phase of gait. During normal ambulation, the sesamoids transmit forces equivalent to three times the body weight, which can escalate exponentially during athletic activities.
Because of these immense biomechanical demands, the sesamoids are susceptible to a variety of pathologies, including acute fractures, stress fractures, nonunions, osteonecrosis (Treves disease), osteoarthritis, and recalcitrant sesamoiditis. While the majority of these conditions can be managed nonoperatively through offloading, orthotics, and activity modification, surgical intervention becomes necessary when conservative measures fail.
Sesamoidectomy—whether partial or complete—is the historical gold standard for recalcitrant sesamoid pathology. However, the procedure is not without significant risks, primarily the disruption of the delicate intrinsic balance of the first MTP joint, which can lead to iatrogenic deformities. Consequently, joint-preserving techniques, such as autogenous bone grafting for nonunions, have gained traction, particularly in high-demand athletes.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the plantar anatomy of the first MTP joint is mandatory before undertaking sesamoid surgery.
The sesamoids are encapsulated within the plantar plate and the two heads of the FHB.
* Tibial (Medial) Sesamoid: Typically larger and bears more weight than its fibular counterpart. It is embedded in the medial head of the FHB and receives attachments from the abductor hallucis.
* Fibular (Lateral) Sesamoid: Embedded in the lateral head of the FHB and receives attachments from the adductor hallucis.
* Intersesamoid Ligament: A strong fibrous band connecting the two sesamoids, forming a tunnel through which the FHL tendon glides.
⚠️ Surgical Warning: The Iatrogenic Deformity Risk
Excision of the tibial sesamoid inherently weakens the medial intrinsic restraints. If the medial head of the FHB and the plantar capsule are not meticulously repaired, the unopposed pull of the adductor hallucis (attached to the fibular sesamoid) will inevitably lead to an iatrogenic hallux valgus deformity. Conversely, excision of the fibular sesamoid without proper repair risks iatrogenic hallux varus.
Neurological Considerations
The proper medial plantar nerve to the hallux courses intimately with the medial aspect of the tibial sesamoid. It emerges plantarly at the musculotendinous junction of the abductor hallucis muscle. Iatrogenic injury to this nerve results in painful neuromas and numbness along the medial aspect of the great toe, a complication that is often more debilitating than the original sesamoid pathology.
INDICATIONS FOR SURGERY
Surgical intervention is indicated only after a rigorous trial of conservative management (typically 6 to 12 months) has failed. Indications include:
* Recalcitrant Sesamoiditis: Chronic inflammation unresponsive to offloading and corticosteroid injections.
* Sesamoid Fractures: Acute or stress fractures with persistent pain.
* Symptomatic Nonunions: Particularly in athletes where prolonged immobilization is detrimental.
* Osteonecrosis (Avascular Necrosis): Often presenting with fragmentation and collapse of the sesamoid.
* Intractable Plantar Keratosis (IPK): Secondary to a hypertrophic or plantar-flexed sesamoid.
* Osteoarthritis: Localized degenerative joint disease between the sesamoid and the metatarsal head.
PREOPERATIVE PLANNING
Standard weight-bearing anteroposterior, lateral, and axial sesamoid radiographs are essential. The axial view is particularly useful for assessing the crista (the bony ridge on the plantar aspect of the metatarsal head separating the sesamoids) and evaluating joint space narrowing or subluxation.
Magnetic Resonance Imaging (MRI) is the modality of choice for differentiating between a symptomatic bipartite sesamoid (which will show bone marrow edema) and an asymptomatic bipartite sesamoid. Computed Tomography (CT) may be utilized to assess the exact fracture pattern or the extent of a nonunion.
SURGICAL TECHNIQUE: TIBIAL SESAMOIDECTOMY
The following technique details the approach for a tibial (medial) sesamoidectomy. The principles of soft tissue preservation and meticulous repair apply equally to fibular sesamoidectomies, though the surgical approach differs (typically a plantar or dorsal web-space approach).
1. Patient Positioning and Anesthesia
The patient is placed in the supine position on the operating table. A regional ankle block or general anesthesia may be utilized, depending on patient and surgeon preference. A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying and protecting the neurovascular structures.
2. Incision and Exposure
- Make a medial longitudinal incision, approximately 4 to 5 cm in length, centered just plantar to the midline of the first MTP joint.
- The incision should parallel the plantar-medial border of the foot, avoiding the weight-bearing plantar skin.
- Deepen the incision through the subcutaneous tissue. Meticulous hemostasis is maintained using bipolar electrocautery to avoid thermal injury to adjacent nerves.
- Incise the joint capsule longitudinally, strictly in line with the skin incision.
3. Intra-articular Evaluation
- Before proceeding with excision, evaluate the intra-articular portion of the tibial sesamoid.
- Assess the quality of the articular cartilage on both the sesamoid and the corresponding plantar surface of the first metatarsal head.
- Check the mobility of any fracture fragments. If the cartilage on the metatarsal head is severely denuded, the patient must be counseled postoperatively regarding the potential for persistent pain or the future need for MTP arthrodesis.
4. Extracapsular Approach and Nerve Protection
- Approach the sesamoid through an extracapsular plane to minimize disruption of the joint mechanics.
- Crucial Step: Identify and protect the proper medial plantar nerve to the hallux. This nerve emerges plantarly at the musculotendinous junction of the abductor hallucis muscle and courses directly over the medial aspect of the capsule.
- Gently dissect the nerve free from the surrounding fascia and retract it plantarly using a blunt retractor or a vessel loop.
💡 Clinical Pearl: Nerve Retraction
Avoid excessive traction on the proper medial plantar nerve. Neurapraxia from aggressive retraction is a common cause of postoperative dysesthesia. Keep the nerve under direct visualization throughout the excision.
5. Excision (Partial vs. Complete)
- Make a precise incision over the plantar aspect of the sesamoid, splitting the fibers of the medial head of the FHB.
- Partial Sesamoidectomy: If only the proximal or distal pole is fragmented or necrotic, a partial excision is preferred to preserve the biomechanical function of the remaining FHB tendon. Use a scalpel to sharply excise the diseased pole, leaving the healthy bone and its tendinous attachments intact.
- Complete Sesamoidectomy: If the entire sesamoid is necrotic, severely comminuted, or arthritic, a complete excision is warranted. Use a small scalpel (e.g., a #15 blade) to carefully shell the sesamoid out of its tendinous envelope. Keep the blade directly on the bone to avoid severing the FHL tendon, which lies immediately adjacent to the lateral border of the tibial sesamoid.
6. Flexor Brevis Defect Repair (The Most Critical Step)
The excision of the sesamoid leaves a significant void in the medial head of the FHB and the plantar plate. Failure to repair this defect will result in a loss of medial soft-tissue tension, leading to hallux valgus.
* For Complete Excision: Repair the defect in the FHB and plantar plate using a robust, 2-0 nonabsorbable polyethylene or polyester suture. Employ a figure-of-eight or Krackow suturing technique to imbricate the tendon ends, restoring the resting tension of the medial structures.
* For Partial Excision: If a portion of the sesamoid is retained, the detached portion of the FHB tendon must be secured to the remaining bone. Use a rongeur or burr to expose the cancellous surface of the remaining sesamoid fragment. Secure the FHB tendon to this cancellous bed using transosseous sutures or a mini-suture anchor (e.g., 2.0 mm or 2.4 mm).
7. Closure
- Once the tendon repair is complete, assess the resting alignment of the hallux. It should sit neutrally without a tendency to drift into valgus.
- Repair the medial joint capsule with 2-0 absorbable sutures (e.g., Vicryl).
- Close the subcutaneous layer with 3-0 absorbable sutures.
- Close the skin with 4-0 nylon or a subcuticular closure, depending on surgeon preference.
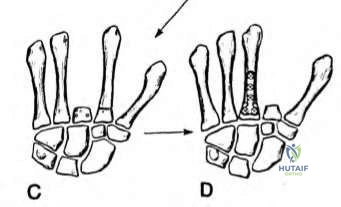
ALTERNATIVE TECHNIQUE: AUTOGENOUS BONE GRAFTING FOR NONUNIONS
While sesamoidectomy is highly effective for pain relief, the loss of the sesamoid alters the biomechanics of the first ray. In high-demand patients, such as elite athletes or dancers, preserving the sesamoid is highly desirable.
Anderson and McBryde reported their seminal experience with autogenous bone grafting for nonunions of the hallux sesamoid in 21 patients. They reported successful bony union in all but two patients, noting that most patients obtained complete pain relief and successfully returned to their preinjury level of athletic activity. These authors demonstrated that biological restoration of the sesamoid is a viable and often superior alternative to excision in the athletic population.
Bone Grafting Technique Overview
- Approach: The surgical approach is identical to that of a sesamoidectomy, utilizing a medial incision for the tibial sesamoid.
- Preparation of the Nonunion: Instead of excising the fragments, the nonunion site is carefully opened. A small curette or a 2.0 mm burr is used to debride the fibrous nonunion tissue down to bleeding, healthy cancellous bone on both the proximal and distal fragments. The articular cartilage must be preserved.
- Graft Harvesting: Autogenous cancellous bone graft is harvested. The ipsilateral calcaneus or the proximal tibia are excellent local donor sites that provide highly osteogenic cancellous bone with minimal donor-site morbidity.
- Graft Placement: The cancellous graft is densely packed into the prepared nonunion defect.
- Fixation (Optional): Depending on the size of the fragments, internal fixation may be achieved using a single, headless compression screw (e.g., 1.5 mm or 2.0 mm) placed from proximal to distal. If the fragments are too small or comminuted for screw fixation, the intact plantar plate and FHB tendon often provide sufficient stability once the defect is grafted and the soft tissues are repaired.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for soft tissue healing (particularly the FHB repair) with the prevention of MTP joint stiffness.
Phase 1: Protection and Healing (Weeks 0 to 3)
- Immediately postoperatively, a bulky compressive dressing is applied.
- The patient is placed in a short-leg cast with a toe plate extending past the hallux to prevent accidental dorsiflexion, which would stress the FHB repair.
- Weight Bearing: Strict non-weight-bearing (NWB) status is maintained for 2 to 3 weeks to allow the initial phase of tendon healing to occur without disruption.
Phase 2: Transition and Early Motion (Weeks 3 to 6)
- At 2 to 3 weeks, the cast and sutures are removed.
- The patient is transitioned to a rigid-soled walking boot or a postoperative hard-soled shoe.
- Weight Bearing: Progressive weight-bearing as tolerated is initiated in the boot.
- Range of Motion (ROM): Active and gentle passive ROM exercises of the first MTP joint are commenced. The focus is on restoring plantarflexion and dorsiflexion while avoiding aggressive passive stretching that could elongate the tendon repair.
Phase 3: Strengthening and Return to Activity (Weeks 6 to 12+)
- At 6 weeks, the patient is transitioned to standard, supportive athletic footwear, often utilizing a rigid carbon-fiber insert or a custom orthotic with a sesamoid cutout to offload the surgical site.
- Physical therapy focuses on intrinsic foot strengthening, proprioception, and gait retraining.
- Return to Sport: The resumption of light jogging and low-impact activities is generally allowed at 8 weeks. Return to full, unrestricted high-impact sports (e.g., sprinting, jumping, dancing) may take 3 to 6 months, depending on the patient's recovery of strength and the resolution of localized edema.
COMPLICATIONS AND PITFALLS
Despite meticulous surgical technique, complications can arise following sesamoid surgery. Surgeons must be prepared to manage these effectively.
- Iatrogenic Hallux Valgus/Varus: As previously discussed, this is the most significant biomechanical complication. It results from failure to adequately repair the FHB tendon or from over-resection of the capsule. Management of a severe postoperative deformity may require secondary soft-tissue reconstruction or, in severe cases, MTP joint arthrodesis.
- Nerve Injury: Injury to the proper medial plantar nerve results in neuroma formation or anesthesia. Prevention through careful extracapsular dissection is paramount. If a neuroma develops and fails conservative management, surgical excision and burying of the nerve stump into the intrinsic musculature may be required.
- MTP Joint Stiffness: Arthrofibrosis is common due to the proximity of the surgery to the joint capsule. Adherence to the postoperative ROM protocol starting at 2 to 3 weeks is critical to mitigating this risk.
- Transfer Metatarsalgia: Removal of a sesamoid alters the load distribution across the forefoot. Patients may develop pain under the lesser metatarsal heads or under the remaining sesamoid. This is typically managed with custom orthotics and metatarsal pads.
- Infection and Wound Dehiscence: The plantar-medial skin has a tenuous blood supply. Incisions must be handled with atraumatic technique, and patients must be counseled on strict elevation during the initial postoperative period to minimize swelling and tension on the incision line.
CONCLUSION
Hallux sesamoidectomy remains a highly effective procedure for the relief of chronic, debilitating pain associated with sesamoid pathology that is refractory to conservative care. The success of the procedure hinges on a thorough understanding of the local anatomy, meticulous protection of the neurovascular structures, and a biomechanically sound repair of the flexor hallucis brevis tendon complex. For the athletic population, joint-preserving techniques such as autogenous bone grafting for nonunions offer an excellent alternative that maintains the structural integrity and mechanical advantage of the first ray. Strict adherence to a phased postoperative rehabilitation protocol is essential to optimize functional outcomes and facilitate a successful return to preinjury activity levels.
