Keller Resection Arthroplasty: Principles and Surgical Technique

Key Takeaway
The Keller resection arthroplasty remains a valuable procedure for older patients with moderate-to-severe hallux valgus and first metatarsophalangeal joint arthritis. By combining resection hemiarthroplasty of the proximal phalanx base with medial eminence excision, surgeons can decompress the joint and correct deformity. Careful patient selection, meticulous soft-tissue handling, and precise K-wire stabilization are paramount to preventing complications such as transfer metatarsalgia or cock-up toe deformity.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of hallux valgus encompasses a broad spectrum of interventions, ranging from isolated soft tissue rebalancing to complex osseous realignments. Among these, combined soft tissue and bony procedures hold a distinct place, particularly in the management of rigid deformities accompanied by profound degenerative joint disease. The Keller resection arthroplasty, originally described by William L. Keller in 1904, remains a foundational procedure within the orthopedic surgeon’s armamentarium. While the advent of modern joint-sparing osteotomies and reliable first metatarsophalangeal (MTP) joint arthrodesis techniques has narrowed its indications, the Keller procedure provides a reliable, reproducible, and highly effective solution for a specific subset of elderly, low-demand patients suffering from complex forefoot pathology.
The patho-epidemiology of severe hallux valgus in the geriatric population is frequently characterized by a combination of osseous deformity, soft tissue contracture, and progressive articular cartilage degradation. Over decades of abnormal biomechanical loading, the first metatarsal drifts into varus, the hallux is pulled into a valgus and pronated position by the adductor hallucis and the lateralized extensor hallucis longus (EHL), and the sesamoid complex undergoes fixed lateral subluxation. This chronic malalignment inevitably leads to asymmetric joint loading, focal chondral wear, and the development of marginal osteophytes, culminating in a rigid, painful hallux rigidus-valgus complex. For these patients, the primary source of morbidity is often twofold: intractable pain over the medial eminence due to footwear friction, and deep, intra-articular pain secondary to bone-on-bone articulation during the terminal stance phase of gait.

Figure 1: Anteroposterior radiograph of the right foot of a 65-year-old patient showing mild-to-moderate deformity and mild degenerative changes at the first MTP joint; the patient presented with both intra-articular and periarticular symptoms.
The fundamental biomechanical goal of the Keller resection arthroplasty is to decompress the joint and mobilize the hallux by removing the base of the proximal phalanx. This resection effectively shortens the bony column of the first ray, relaxing the contracted lateral soft tissue structures and allowing for marked correction of the valgus deformity without the need for a complex, healing-dependent metatarsal osteotomy. By converting a rigid, arthritic joint into a fibrous pseudoarthrosis, the procedure eliminates intra-articular pain while restoring a functional, albeit altered, range of motion.

Figure 2: Twelve years post-Keller procedure with excision of the fibular sesamoid. Note the correction of the first metatarsal varus and the maintenance of sufficient joint space to allow a functional range of motion.
However, it is critical to understand the biomechanical trade-offs inherent to this procedure. Because the varus alignment of the first metatarsal is not directly corrected via osteotomy, maintaining the correction of the hallux valgus relies heavily on meticulous soft tissue reconstruction and postoperative scar tissue formation (encapsulation). Historically, complications such as "cock-up" toe deformity, transfer metatarsalgia, and recurrent valgus have been emphasized in the literature. These historical pitfalls often stemmed from over-resection of the phalanx, failure to stabilize the joint with Kirschner wires, or poor patient selection. In contemporary orthopedic practice, when patients are selected carefully and modern technical modifications are employed, complications are uncommon, and patient satisfaction is remarkably high.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the first MTP joint is an absolute prerequisite for executing a successful Keller arthroplasty while minimizing iatrogenic complications. The first MTP joint is a highly complex diarthrodial joint stabilized by a robust capsuloligamentous complex and dynamic musculotendinous units. The proximal phalanx base serves as the critical insertion site for the intrinsic musculature of the hallux. The abductor hallucis inserts on the plantar-medial base, the adductor hallucis inserts on the plantar-lateral base, and the flexor hallucis brevis (FHB) inserts via its medial and lateral heads onto the plantar base, intimately associated with the tibial and fibular sesamoids, respectively.
When the base of the proximal phalanx is resected during a Keller procedure, these critical intrinsic attachments are inherently destabilized or entirely detached. This detachment profoundly alters the biomechanics of the first ray. The loss of the FHB insertion compromises the active plantarflexion power of the proximal phalanx and partially disrupts the windlass mechanism, which normally stabilizes the medial longitudinal arch during the propulsive phase of gait. Consequently, the load-bearing capacity of the first ray is diminished, which can lead to increased stress transfer to the lesser metatarsal heads—the pathophysiological basis for postoperative transfer metatarsalgia.
Furthermore, the resection alters the delicate balance between the extrinsic flexors and extensors of the hallux. With the intrinsic plantarflexors detached, the extensor hallucis longus (EHL) and extensor hallucis brevis (EHB) exert an unopposed dorsal pull on the distal segment of the hallux. If the joint is not adequately stabilized postoperatively, this dynamic imbalance inevitably leads to dorsal subluxation of the remaining proximal phalanx on the metatarsal head, clinically manifesting as the dreaded "cock-up" toe deformity. To counteract this, modern Keller techniques mandate temporary axial Kirschner wire fixation to hold the toe in a neutral or slightly plantarflexed position while the capsular tissues heal and fibrose, creating a stable pseudoarticulation.
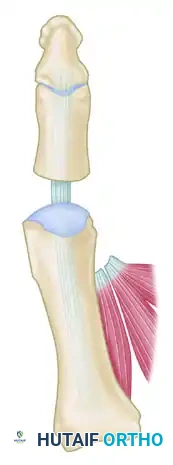
Figure 3: Anatomical diagram highlighting the course of the Flexor Hallucis Longus (FHL) beneath the concave plantar aspect of the proximal phalanx.
Equally critical is the anatomical relationship of the flexor hallucis longus (FHL) tendon to the proximal phalanx. While the dorsal, medial, and lateral cortices of the proximal phalanx are convex, the plantar surface is distinctly flat and features a central concavity that houses the FHL tendon. This tendon runs strictly along the midline, tightly bound within its fibro-osseous sheath. During the transverse osteotomy of the proximal phalanx, the surgeon must be acutely aware of this geometry. A straight cut across the bone without adequate plantar protection will inevitably lacerate the FHL, resulting in a disastrous loss of interphalangeal joint flexion and severe functional impairment.
Figure 4: Cross-sectional view noting the concave plantar aspect of the proximal phalanx housing the FHL tendon. This highlights the danger zone during the phalangeal osteotomy.
Exhaustive Indications and Contraindications
The success of the Keller procedure is inextricably linked to strict and uncompromising patient selection. It is not an operation for the young, active patient, nor is it appropriate for flexible deformities that can be managed with joint-sparing osteotomies. The ideal candidate is an elderly individual with low functional demands who presents with a rigid, painful hallux valgus deformity complicated by severe osteoarthritis of the first MTP joint. In these patients, the primary surgical goals are pain relief, facilitation of normal shoe wear, and restoration of independent ambulation, rather than the restoration of normal joint biomechanics or high-level athletic function.
Primary candidates are typically older than 65 years, though physiological age and activity level are more critical determinants than chronological age alone. The deformity is usually moderate-to-severe (hallux valgus angle of 30 to 45 degrees) with an intermetatarsal angle (IMA) that, while elevated, is often secondary to the chronicity of the deformity rather than primary metatarsus primus varus. Clinical symptoms must include intractable pain over the medial eminence that severely limits footwear options, coupled with deep, grinding intra-articular pain indicative of advanced degenerative joint disease. Radiographically, these patients demonstrate an incongruous first MTP joint with joint space narrowing, subchondral sclerosis, osteophytosis, and lateral displacement of the sesamoid apparatus.
Conversely, the Keller procedure is strictly contraindicated in young, active patients due to the inevitable loss of push-off power and the high risk of symptomatic transfer metatarsalgia. It is also contraindicated in patients with flexible deformities, where a corrective osteotomy would preserve joint function. Neuromuscular disorders characterized by spasticity or profound muscle imbalance represent an absolute contraindication, as the loss of intrinsic stability will lead to rapid and severe recurrence or secondary deformities. Furthermore, patients with an excessively long second metatarsal or pre-existing severe metatarsalgia should be approached with extreme caution, as the shortening of the first ray will predictably exacerbate lesser ray overload.
| Parameter | Indications for Keller Arthroplasty | Contraindications for Keller Arthroplasty |
|---|---|---|
| Patient Age/Demand | Elderly (>65 years), sedentary, low functional demands, limited ambulation. | Young, active, athletes, high functional demands, laborers. |
| Deformity Type | Rigid hallux valgus, combined with severe osteoarthritis (Hallux Rigidus). | Flexible hallux valgus, isolated medial eminence prominence without DJD. |
| Pathology | Advanced DJD, incongruous joint, severe lateral sesamoid subluxation. | Preserved articular cartilage, reducible deformity. |
| Neuromuscular | Intact neurological status without spasticity. | Spasticity (e.g., Cerebral Palsy), severe neuropathy (Charcot risk). |
| Lesser Rays | Asymptomatic lesser rays, normal metatarsal cascade. | Pre-existing severe transfer metatarsalgia, excessively long 2nd metatarsal. |
Expanded Indications: Technical Modifications
While the classic Keller procedure is limited to the parameters above, specific technical modifications can expand its utility to include older patients with far more severe deformities. The most critical of these modifications is the integration of a fibular sesamoidectomy. Patients presenting with 50 degrees or more of hallux valgus, complete lateral dislocation of the sesamoids, marked degenerative changes, and severe pronation of the hallux can achieve excellent functional and cosmetic outcomes when this modification is employed. The removal of the fibular sesamoid eliminates the deforming pull of the adductor hallucis and allows the first metatarsal head to translate laterally, reducing the intermetatarsal angle without the need for a proximal osteotomy.


Figure 5: Severe hallux valgus with prominent bursa formation in a 70-year-old woman. Anteroposterior and lateral clinical photographs demonstrate the profound nature of the deformity.


Figure 6: Postoperative clinical photograph and weight-bearing radiographs of the same patient demonstrating excellent correction of the deformity utilizing the modified Keller procedure with fibular sesamoidectomy.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential to anticipate anatomical challenges and ensure precise execution of the bony resections. The clinical evaluation must include a rigorous assessment of the patient's vascular status. Palpation of the dorsalis pedis and posterior tibial pulses is mandatory; if pulses are diminished, non-invasive vascular studies (ABI, toe pressures) must be obtained. A Keller procedure relies heavily on soft tissue healing to form a stable pseudoarthrosis; performing this surgery in the presence of severe peripheral arterial disease is a recipe for wound dehiscence, infection, and potential amputation. Neurological assessment is equally important to rule out profound peripheral neuropathy, which could mask postoperative complications or predispose the patient to Charcot neuroarthropathy.
Radiographic templating utilizes standard weight-bearing anteroposterior, lateral, and sesamoid axial views of the foot. The surgeon must carefully evaluate the degree of joint space narrowing, the size of the medial eminence, and the position of the sesamoids. The critical templating step involves determining the exact level of the proximal phalangeal resection. The osteotomy must be planned precisely at the metaphyseal-diaphyseal junction of the proximal phalanx. Resecting too little bone will fail to adequately decompress the joint, leading to persistent pain and restricted motion. Conversely, resecting too much bone (into the diaphysis) severely compromises the remaining intrinsic attachments, drastically increases the risk of a flail toe or cock-up deformity, and excessively shortens the toe, leading to cosmetic dissatisfaction.
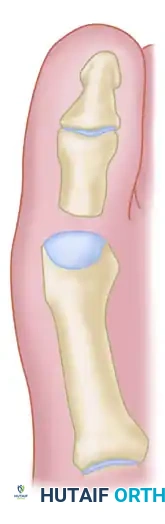
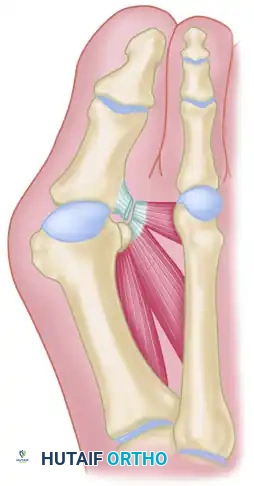
Figure 7: Diagrammatic representation of the Keller technique, illustrating the resection of the proximal phalanx, release of the adductor tendon, and resection of the medial eminence.
The procedure is typically performed under regional anesthesia, utilizing a comprehensive forefoot block or an ultrasound-guided popliteal sciatic nerve block combined with a saphenous nerve block. This approach provides excellent intraoperative anesthesia and prolonged postoperative analgesia, minimizing the need for systemic opioids in the elderly population. The patient is positioned supine on the operating table. A small bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the foot rests in a neutral position facing the surgeon.
If the vascular status is adequate, an Esmarch wrap tourniquet is applied at the ankle or calf to ensure a bloodless surgical field. This is critical for identifying and protecting delicate neurovascular structures during the deep dissection and sesamoidectomy. The foot and lower leg are prepped and draped in a standard sterile orthopedic fashion. The surgeon must ensure that the entire forefoot is freely mobile to allow for dynamic assessment of the hallux and MTP joint throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The surgical approach begins with a straight, midline medial longitudinal incision. The incision starts approximately 1 cm proximal to the interphalangeal (IP) joint of the hallux and extends proximally to the junction of the distal and middle thirds of the first metatarsal shaft. This lengthy incision is deliberately chosen to avoid excessive traction tension on the skin edges during deep retraction. The superficial tissues over the medial eminence are often thin and compromised; aggressive retraction of a small incision can easily lead to marginal skin necrosis in the elderly patient. Superficial dissection is performed bluntly to locate and protect the most medial branch of the superficial peroneal nerve, which typically courses along the proximal-dorsal edge of the medial eminence.
Deep Exposure and Capsular Flap
The dissection is carried down to the bone in the midline medially. The surgeon raises a full-thickness deep flap consisting of capsule and periosteum via sharp subperiosteal dissection. This flap is elevated dorsally, exposing up to one-third to one-half the width of the metatarsal head and neck. At the joint level, capsular elevation continues along the extensor hallucis brevis (EHB) insertion until the proximal third of the proximal phalanx is completely exposed. Having an assistant actively pronate the hallux during this stage significantly improves visualization of the lateral phalangeal base. Subperiosteal dissection must strictly expose only the portion of the proximal phalanx slated for resection to preserve the distal blood supply.
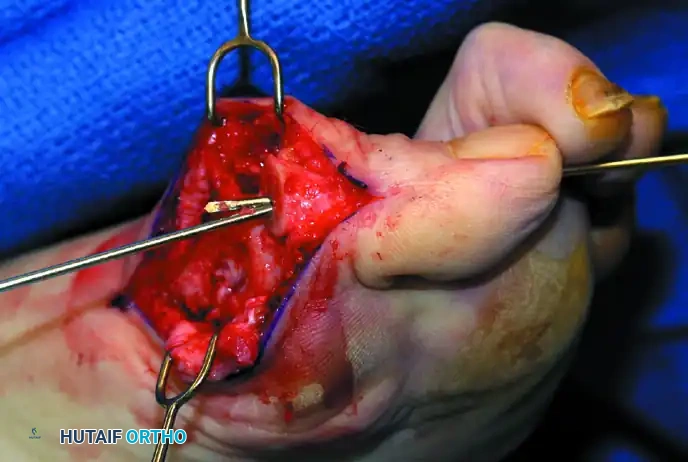
Figure 8: Intraoperative exposure demonstrating the medial capsular incision and initial elevation of the soft tissue envelope.
Plantar Dissection and FHL Protection
Plantar dissection is meticulously performed to expose the plantar aspect of the medial eminence, the tibial sesamoid, and the plantar-medial corner of the proximal phalanx. The surgeon supinates the proximal phalanx to expose its plantar corner. At this juncture, identifying and protecting the flexor hallucis longus (FHL) tendon is paramount. As previously noted, the FHL lies in a distinct concavity on the plantar aspect of the phalanx. Using a blunt instrument, the FHL is identified and retracted plantarward using a small right-angle or malleable retractor. This retractor must remain in place throughout the entirety of the phalangeal osteotomy.
Bony Resection: Medial Eminence and Proximal Phalanx
The medial eminence is resected at the sagittal groove using a 9-mm oscillating saw. The cut begins dorsally and is directed plantarward and slightly medially (5 to 10 degrees) to avoid skiving into the articular cartilage of the metatarsal head. Following this, the base of the proximal phalanx is resected exactly at the metaphyseal-diaphyseal junction, typically constituting the proximal one-third of the bone. The saw blade is carefully advanced, ensuring it does not exit the far cortex by more than 1 to 2 mm to prevent neurovascular or tendinous injury.

Figure 9: The metaphyseal-diaphyseal junction of the proximal phalanx dictates the exact level of resection.
Once the osteotomy is complete, the basilar fragment is grasped with a small Kocher clamp. By rotating the fragment and applying medial traction, the surgeon can safely release its remaining lateral attachments, which include the lateral collateral ligaments and the adductor hallucis tendinous insertion, allowing for complete excision of the fragment.
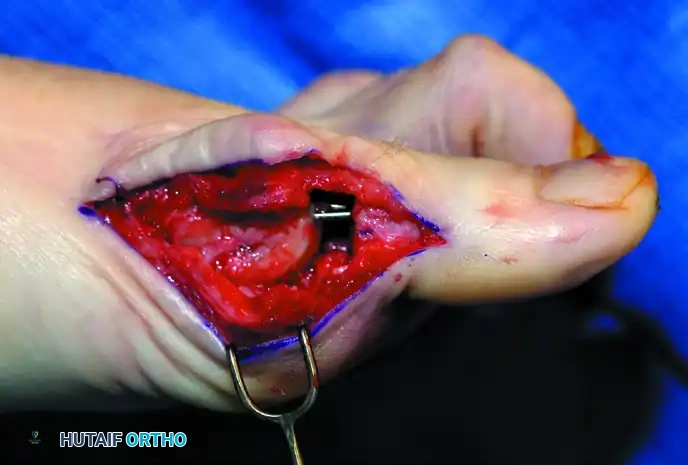

Figure 10: Intraoperative extraction of the resected proximal phalangeal base using a Kocher clamp.
Modification: Removal of the Fibular Sesamoid
In cases of severe deformity (>50 degrees valgus) with complete lateral subluxation of the sesamoid apparatus, a fibular sesamoidectomy is performed. A sturdy two-toothed retractor is placed beneath the metatarsal head, lifting it dorsally to maximize plantar exposure. The fibular sesamoid is mobilized using a Freer elevator. The FHL tendon and the lateral neurovascular bundle are identified and protected. Firm medial traction is applied to the plantar-medial capsule to visualize the intersesamoid ligament, which is then longitudinally incised. The fibular sesamoid is grasped with a Kocher clamp, pulled distally and medially, and excised completely.
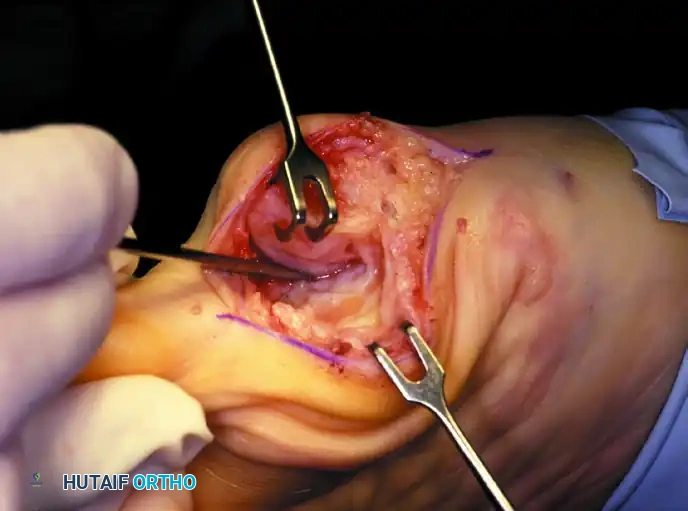
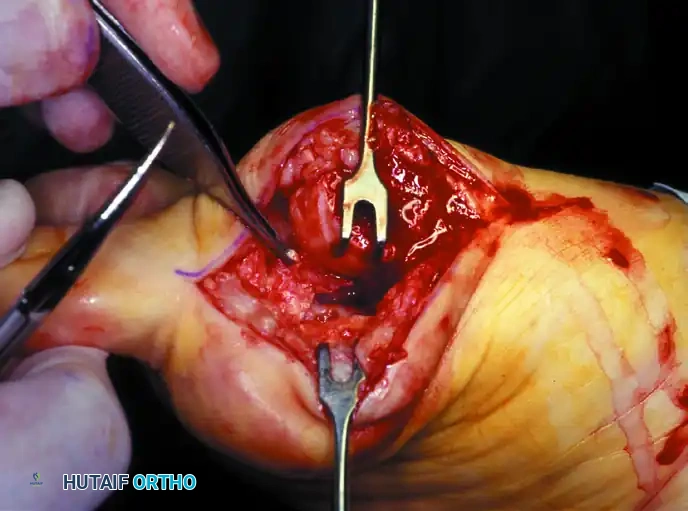
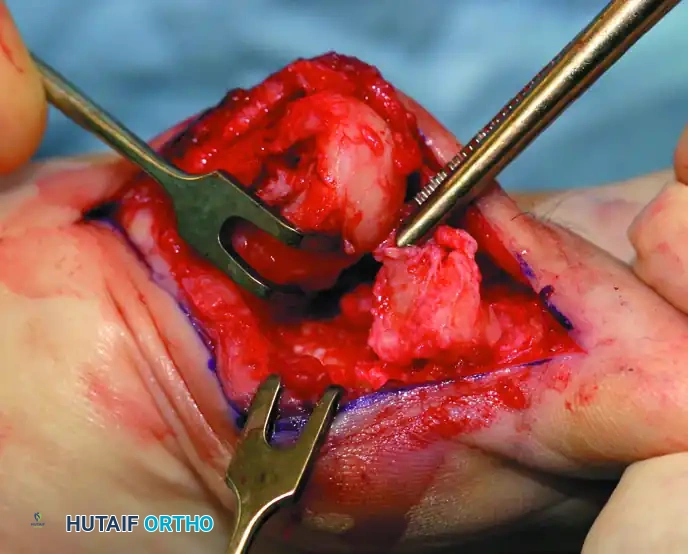
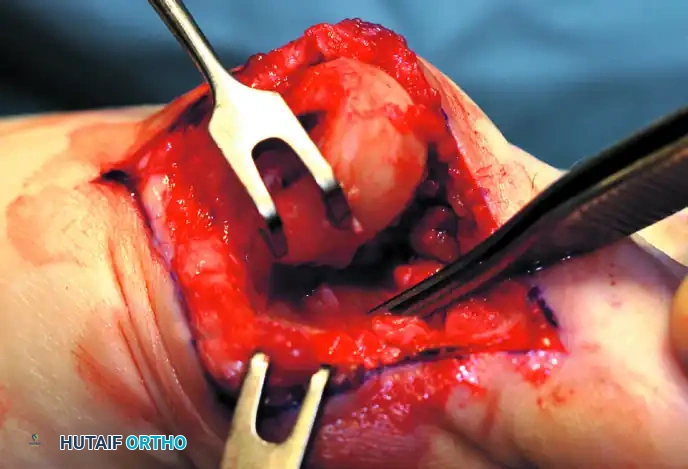
Figure 11: Stepwise diagrammatic representation of fibular sesamoidectomy. Note the relationship between the intersesamoid ligament, the tibial/fibular sesamoids, and the FHL.

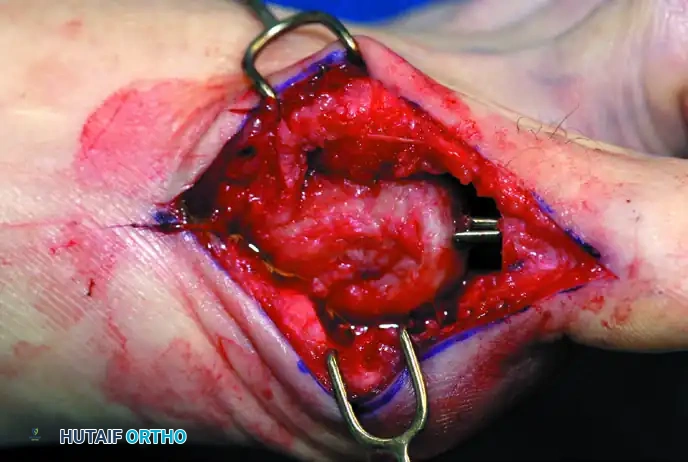
Figure 12: Intraoperative visualization of the sesamoid apparatus and subsequent excision of the fibular sesamoid.
Axial Pinning and Alignment
Stabilization of the pseudoarticulation is paramount to allow the capsule to heal at the correct length and tension, thereby preventing a cock-up deformity. With the ankle held at 90 degrees to ensure physiological tension on the extrinsic tendons, a 0.062-inch (1.6 mm) Kirschner wire is introduced. The wire is driven retrograde through the central axis of the remaining proximal phalanx, traversing the interphalangeal joint, and exiting the tip of the distal phalanx.
The wire driver is then moved to the distal end of the wire. The hallux is carefully positioned in neutral alignment in the transverse plane and approximately 10 to 15 degrees of plantarflexion in the sagittal plane. The K-wire is then driven antegrade into the center of the first metatarsal head and advanced down the medullary canal of the metatarsal shaft for a distance of 3 to 4 centimeters. This rigid axial fixation counteracts the dorsal pull of the EHL. Finally, a meticulous, imbricating capsulorrhaphy is performed using heavy absorbable suture (e.g., 2-0 Vicryl) to reconstruct the medial soft tissue envelope, taking care to close the dead space over the resected medial eminence.
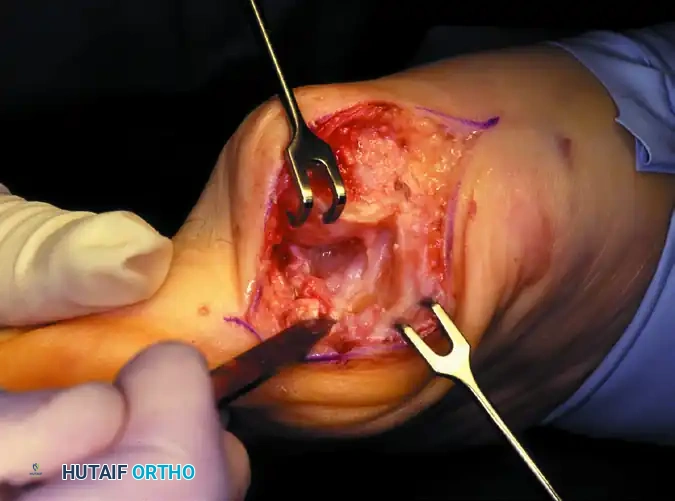
Figure 13: Final axial pinning demonstrating the K-wire traversing the IP and MTP joints, maintaining neutral alignment and slight plantarflexion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following a Keller resection arthroplasty can occur, primarily due to the inherent biomechanical destabilization of the first ray. The most notorious complication is the "cock-up" toe deformity, characterized by fixed dorsal subluxation of the remaining proximal phalanx on the metatarsal head. This occurs due to the unopposed action of the extensor hallucis longus (EHL) following the detachment of the intrinsic plantarflexors. Historically, the incidence of cock-up toe was reported to be as high as 10-15%, but with the modern mandate of temporary axial K-wire fixation and precise metaphyseal-diaphyseal resection, the incidence has dropped to less than 2%.
Transfer metatarsalgia is another significant complication, resulting from the functional shortening of the first ray and the loss of the windlass mechanism. As the load-bearing capacity of the first MTP joint decreases, weight-bearing forces are shifted laterally to the lesser metatarsal heads, particularly the second metatarsal. Patients present with intractable plantar keratoses and pain under the lesser metatarsal heads. The incidence varies widely based on patient selection, but can approach 20% in patients who are overly active or have an unrecognized pre-existing long second metatarsal.
Recurrent hallux valgus or the development of a flail toe (a completely unstable, floppy hallux) are direct consequences of over-resection of the proximal phalanx. If the osteotomy is made too distally into the diaphysis, the remaining bone stock is insufficient to maintain any soft tissue tethering, leading to gross instability. Iatrogenic laceration of the flexor hallucis longus (FHL) tendon is a catastrophic technical error that results in an immediate loss of IP joint active flexion and significantly contributes to dorsal contracture.
Salvage of a failed Keller procedure is notoriously difficult due to the loss of bone stock and severe soft tissue compromise. For a rigid cock-up toe or severe recurrent deformity, the gold standard salvage procedure is a first MTP joint arthrodesis. However, because of the shortened first ray, this often requires the use of an intercalary structural autograft (typically from the iliac crest)
