Hallux Rigidus: Pathogenesis, Evaluation, and Surgical Management

Key Takeaway
Hallux rigidus is a progressive degenerative arthropathy of the first metatarsophalangeal joint, characterized by restricted dorsiflexion and dorsal osteophyte formation. This comprehensive guide details the underlying biomechanics, clinical evaluation, and evidence-based surgical interventions. From joint-sparing cheilectomy for early-stage disease to first MTP arthrodesis for end-stage arthritis, mastering these techniques ensures optimal restoration of foot biomechanics and durable pain relief for patients.
Comprehensive Introduction and Patho-Epidemiology
Hallux rigidus represents a progressive, highly debilitating osteoarthritis of the first metatarsophalangeal (MTP) joint, clinically characterized by a marked, painful restriction of motion, predominantly in the sagittal plane of dorsiflexion. The nomenclature surrounding this condition has evolved over the past century. The term hallux rigidus was originally introduced to the surgical lexicon by Cotterill in 1888, effectively describing the terminal clinical presentation of a stiff, unyielding great toe. However, the foundational surgical literature traces back to Davies-Colley in 1887, who performed the first documented resection arthroplasty of the proximal phalangeal base. Davies-Colley originally termed the condition hallux flexus, an astute observation of the characteristic plantarflexed posture the proximal phalanx assumes relative to the metatarsal head when the foot is plantigrade, compensating for the severe loss of extension.
Despite over a century of academic inquiry, the precise pathogenesis of hallux rigidus remains a topic of vigorous orthopedic debate. The disease is universally recognized as a cascade of relentless joint degradation, but the initiating event is often debated. The current consensus points toward a multifactorial etiology where localized articular cartilage damage precipitates a profound reactive synovitis. At the molecular level, this inflammatory milieu is driven by the upregulation of pro-inflammatory cytokines, including Interleukin-1 (IL-1) and Tumor Necrosis Factor-alpha (TNF-α), which subsequently activate matrix metalloproteinases (MMPs). These enzymes accelerate the degradation of the extracellular cartilage matrix, leading to progressive chondrocyte apoptosis, robust osteophyte proliferation (particularly along the dorsal articular margin), and eventual subchondral cyst formation and bone collapse.
The McMaster cleavage lesion remains one of the most critical histological and operative observations in understanding the early patho-epidemiology of this disorder. McMaster demonstrated that the earliest microscopic pathology in hallux rigidus is a distinct, localized cleavage lesion within the articular cartilage of the first metatarsal head, occurring entirely independently of subchondral bone detachment. Radiographically, this manifests as a subtle, frequently overlooked depression in the dome of the metatarsal head. Anatomically, this lesion is invariably located between the apex of the metatarsal dome and the dorsal margin of the articular surface.

McMaster postulated a compelling biomechanical etiology for the ensuing clinical cascade. During the terminal stance phase of gait, as the hallux is forced into extension, the proximal phalanx abuts directly against this cartilaginous cleavage lesion. This abutment generates acute nociceptive feedback, prompting an instinctive, protective flexor reflex that actively limits extension. Over time, this functional limitation transitions into a rigid mechanical block as the chronic inflammatory state drives the formation of a prominent dorsal osteophyte. Epidemiologically, hallux rigidus is the most common arthritic condition of the foot, affecting approximately 1 in 45 individuals over the age of 50. It exhibits a strong female predilection and frequently presents bilaterally in adults with primary osteoarthritis, whereas unilateral presentations are overwhelmingly correlated with a prior history of acute trauma or repetitive microtrauma in the adolescent and young adult populations.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the first MTP joint is an absolute prerequisite for any reconstructive orthopedic surgeon. The first MTP joint is a complex, multi-articulating hinge joint that must withstand extraordinary forces during the gait cycle. The primary articulation occurs between the convex head of the first metatarsal and the concave elliptical base of the proximal phalanx. However, the functional joint complex also includes the critical articulation between the plantar aspect of the metatarsal head and the two sesamoid bones, which are embedded within the tendons of the flexor hallucis brevis (FHB). The metatarsal head is characterized by a central crista on its plantar surface, which separates the medial (tibial) and lateral (fibular) sesamoid grooves, ensuring proper tracking of the sesamoid apparatus during sagittal plane motion.
The capsuloligamentous complex of the first MTP joint is robust, designed to provide static stability against the massive deforming forces of push-off. The medial and lateral collateral ligaments originate from the epicondyles of the metatarsal head and fan out to insert onto the base of the proximal phalanx and the margins of the plantar plate. The plantar plate itself is a thick, fibrocartilaginous structure that intimately blends with the joint capsule, the FHB tendons, and the sesamoid-phalangeal ligaments. Dorsally, the joint is reinforced by the extensor hallucis longus (EHL) and extensor hallucis brevis (EHB) tendons, alongside the dorsal joint capsule. The primary blood supply to this region is derived from the first dorsal metatarsal artery and the first plantar metatarsal artery, while innervation is supplied by the dorsomedial cutaneous nerve (a branch of the superficial peroneal nerve) and the deep peroneal nerve laterally.
Biomechanically, the first MTP joint is the linchpin of the foot's propulsive phase. During the normal gait cycle, the joint must transition from a neutral position at heel strike to a highly extended position during terminal stance. Normal ambulation requires approximately 65 to 75 degrees of first MTP joint dorsiflexion. This extreme range of motion is necessary to engage the "windlass mechanism," famously described by Hicks. As the hallux dorsiflexes, the plantar fascia is wound around the metatarsal head, effectively shortening the distance between the calcaneus and the metatarsal heads. This action elevates and stabilizes the medial longitudinal arch, converting the foot from a flexible shock absorber into a rigid lever arm for an efficient, powerful push-off.
In the setting of hallux rigidus, this elegant biomechanical sequence is catastrophically disrupted. The dorsal osteophyte acts as a physical cam-block, preventing the proximal phalanx from gliding dorsally over the metatarsal head. Consequently, the windlass mechanism cannot be fully engaged, leading to a loss of arch stability and a significant reduction in push-off power. To compensate, patients frequently alter their gait mechanics, externally rotating the foot and shifting weight-bearing forces to the lateral column. This compensatory gait pattern frequently results in transfer metatarsalgia beneath the lesser metatarsal heads, lateral column overload, and secondary pathologies in the ipsilateral ankle, knee, and hip joints due to altered kinematic chain mechanics. Furthermore, the instantaneous center of rotation of the first MTP joint is altered, shifting dorsally and proximally, which exponentially increases the compressive sheer forces across the remaining articular cartilage, accelerating the degenerative cycle.
Exhaustive Indications and Contraindications
The management of hallux rigidus is dictated by a meticulous correlation of the patient's subjective symptoms, functional demands, and objective clinical and radiographic findings. The Coughlin and Shurnas classification system remains the gold standard for staging the disease and guiding surgical decision-making. Non-operative management—including rigid Morton's extensions, rocker-bottom shoe modifications, NSAIDs, and targeted intra-articular corticosteroid injections—must be exhausted prior to surgical consideration, particularly in early-stage disease. When conservative measures fail, operative intervention is categorized broadly into joint-sparing procedures (cheilectomy, proximal phalanx osteotomy) and joint-sacrificing procedures (arthrodesis, interpositional arthroplasty, total joint replacement).
Surgical indications are heavily dependent on the integrity of the mid-arc motion. Cheilectomy is indicated for Grade 1 and 2 disease, and highly selected Grade 3 cases where the pain is isolated exclusively to the extremes of dorsiflexion, and the mid-arc of motion remains entirely pain-free. The primary objective of a cheilectomy is to excise the dorsal impingement lesion, thereby increasing the pain-free arc of motion. Conversely, arthrodesis is the definitive, gold-standard procedure for end-stage (Grade 3 and 4) hallux rigidus, where global articular destruction has occurred, and pain is present throughout the entire range of motion, including the mid-arc.
Absolute contraindications for joint-sparing procedures include systemic inflammatory arthropathies (e.g., rheumatoid arthritis), severe global joint space narrowing, and pain during mid-arc motion. Performing a cheilectomy in a patient with mid-arc pain will reliably result in persistent postoperative pain and early failure. Relative contraindications for arthrodesis include severe ipsilateral interphalangeal (IP) joint arthritis, as a fused MTP joint will place exponentially higher mechanical demands on the IP joint, potentially exacerbating distal pain. In such highly specific scenarios, an interpositional arthroplasty or a Keller resection arthroplasty may be considered, though these are generally reserved for older, low-demand patients due to the resultant loss of push-off power and potential for transfer metatarsalgia.
Clinical and Surgical Decision Matrix
| Grade (Coughlin & Shurnas) | Clinical Findings | Radiographic Findings | Surgical Indications & Options |
|---|---|---|---|
| Grade 0 | Stiffness; pain only at extreme dorsiflexion; no mid-arc pain. | Normal radiographs; possible subtle dorsal depression (McMaster lesion). | Non-operative: Shoe modification, orthotics. Operative: Rarely indicated. |
| Grade 1 | Mild pain at extremes of motion; preserved mid-arc motion; palpable dorsal spur. | Mild dorsal osteophyte; joint space well preserved; minimal sclerosis. | First-line: Cheilectomy. Adjunct: Moberg osteotomy if residual soft-tissue tightness exists. |
| Grade 2 | Moderate pain throughout terminal ROM; mid-arc usually pain-free; restricted dorsiflexion. | Moderate dorsal osteophyte; mild-to-moderate joint space narrowing (dorsal > plantar). | First-line: Cheilectomy. Alternative: Cheilectomy + proximal phalanx osteotomy. |
| Grade 3 | Significant stiffness; constant pain at extremes; painful mid-arc motion; no pain at rest. | Severe dorsal/medial/lateral osteophytes; global joint space narrowing; subchondral cysts. | Gold Standard: First MTP Arthrodesis. Alternative: Interpositional arthroplasty (low-demand patients). |
| Grade 4 | Severe global stiffness; constant pain throughout entire ROM and pain at rest. | Same as Grade 3, but clinical presentation is significantly more severe. | Gold Standard: First MTP Arthrodesis. Contraindicated: Cheilectomy. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is paramount to achieving a successful surgical outcome in hallux rigidus. The clinical evaluation must extend beyond the first MTP joint to include a comprehensive biomechanical assessment of the entire lower extremity. The physical examination must quantify the exact arc of active and passive motion. The "Grind Test" is a critical maneuver: the examiner applies axial compression to the proximal phalanx while circumducting it against the metatarsal head. Elicitation of crepitus and sharp pain during this maneuver strongly suggests global, full-thickness cartilage loss, effectively ruling out a joint-sparing cheilectomy.

Furthermore, the examiner must evaluate for concomitant pathologies that could compromise the surgical outcome. The Silfverskiöld test is performed to assess for isolated gastrocnemius contracture versus a combined Achilles tendon contracture, as unrecognized equinus forces will massively overload the first ray postoperatively, leading to early hardware failure or transfer metatarsalgia. The lesser toes must be evaluated for hammertoe deformities, and the midfoot should be assessed for hypermobility or degenerative changes, particularly at the tarsometatarsal (TMT) joints.
Standard weight-bearing radiographs of the foot—consisting of anteroposterior (AP), lateral, and axial sesamoid views—are mandatory. Preoperative templating involves assessing the hallux valgus angle (HVA), the intermetatarsal angle (IMA), and the distal metatarsal articular angle (DMAA). While hallux rigidus is distinct from hallux valgus, mild valgus deformities frequently coexist and must be accounted for during arthrodesis positioning. The lateral view is scrutinized for the extent of the dorsal osteophyte and the presence of metatarsus primus elevatus. Historically, metatarsus primus elevatus was considered a primary etiology of hallux rigidus; however, modern radiographic analyses suggest it is more likely a secondary phenomenon resulting from dorsal osteophyte formation and joint subluxation. Advanced imaging, such as MRI, is rarely indicated for classic adult-onset hallux rigidus but is highly valuable in adolescent patients to evaluate for osteochondritis dissecans (OCD) lesions or early chondral delamination prior to radiographic joint space narrowing.
In the operating room, patient positioning is standardized to optimize exposure and fluoroscopic access. The patient is placed in the supine position on a radiolucent operating table. A bump is frequently placed beneath the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position, which greatly facilitates the dorsal approach to the first MTP joint. A pneumatic tourniquet is applied either at the thigh or the calf, depending on surgeon preference and the anticipated duration of the case. Intravenous prophylactic antibiotics are administered 30 minutes prior to inflation. The foot and ankle are prepped and draped in a standard sterile fashion, ensuring the entire foot is exposed to allow for intraoperative assessment of the cascade of the lesser toes and the overall alignment of the medial column.
Step-by-Step Surgical Approach and Fixation Technique
Surgical execution in hallux rigidus reconstruction demands meticulous soft tissue handling and precise osseous resection. The two workhorse procedures—cheilectomy and arthrodesis—require distinct technical approaches to achieve their biomechanical goals.
1. Cheilectomy (Joint-Sparing Technique)
The objective of a cheilectomy is the complete eradication of the dorsal mechanical block while preserving the maximum viable articular surface.
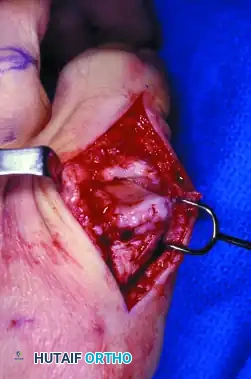
Incision and Exposure: A dorsal longitudinal incision, approximately 4 to 5 cm in length, is centered directly over the first MTP joint. The incision is placed slightly medial to the extensor hallucis longus (EHL) tendon. Blunt dissection is utilized through the subcutaneous tissues to meticulously identify and retract the branches of the dorsomedial cutaneous nerve. Iatrogenic injury to this nerve is a frequent cause of devastating postoperative neuropathic pain.
Capsulotomy: A longitudinal or T-type capsulotomy is performed. The capsule and periosteum are elevated sharply from the dorsal aspect of the metatarsal head and the base of the proximal phalanx, creating full-thickness flaps.
Osteophyte Resection: The prominent dorsal osteophyte is fully exposed. Using an oscillating saw or a sharp, broad osteotome, the dorsal exostosis is resected. The critical rule of cheilectomy is the resection of the dorsal 30% of the metatarsal head. The cut should be made flush with the dorsal cortex of the metatarsal shaft and angled slightly plantarward to ensure no residual dorsal ridge remains.
Debridement and Assessment: Following the primary resection, the joint is distracted and inspected. Any central cleavage lesions are thoroughly debrided to stable margins. Marginal osteophytes on the medial and lateral gutters are excised using a rongeur to decompress the capsule fully. The hallux is then passively dorsiflexed. The surgeon must achieve a minimum of 70 to 80 degrees of passive dorsiflexion intraoperatively without impingement. If osseous impingement is clear, further dorsal resection is required. If dorsiflexion is limited by soft tissue tension despite adequate bone resection, a Moberg (dorsal closing wedge) osteotomy of the proximal phalanx may be performed to functionally dorsiflex the toe without sacrificing further metatarsal articular cartilage. The capsule is closed loosely with absorbable suture to prevent restricting the newly acquired motion.
2. First MTP Joint Arthrodesis (Joint-Sacrificing Technique)
Arthrodesis is the definitive, highly predictable solution for end-stage disease. The success of this procedure hinges entirely on two factors: meticulous joint preparation and absolute precision in spatial positioning.
Joint Preparation: A similar dorsal approach is utilized. Once the joint is exposed, the collateral ligaments are sharply released from the metatarsal head to allow for severe plantarflexion of the proximal phalanx, fully exposing the articular surfaces. All remaining cartilage and subchondral sclerotic bone must be aggressively denuded down to healthy, bleeding cancellous bone. While flat cuts with a saw can be used, cup-and-cone reamers are heavily favored in modern practice. These reamers create congruent, spherical surfaces that maximize cancellous bone contact area while allowing for infinite multi-planar adjustments of the toe position prior to fixation.
Critical Positioning: The spatial orientation of the fused hallux dictates the functional outcome. The universally accepted parameters for fusion are:
* Valgus: 10 to 15 degrees of valgus, ensuring the hallux rests parallel to the second toe without abutting it.
* Dorsiflexion: 10 to 15 degrees of dorsiflexion relative to the floor, or approximately 15 to 20 degrees relative to the longitudinal axis of the first metatarsal. This specific angle allows the toe to clear the ground during the swing phase of gait and accommodates a standard shoe with a moderate heel.
* Rotation: Neutral rotation is imperative. The toenail must face directly dorsal. Any pronation or supination will lead to painful callosities along the borders of the interphalangeal joint.
Rigid Fixation: Once provisional K-wire fixation confirms perfect alignment under fluoroscopy, definitive fixation is applied. The most biomechanically robust construct consists of a low-profile, pre-contoured dorsal titanium plate combined with an independent interfragmentary lag screw crossing the fusion site. Alternatively, crossed compression screws can be utilized, though they offer less resistance to dorsal bending forces. Any remaining osseous voids are packed with local bone graft harvested from the resected dorsal osteophytes. The wound is closed in a standard layered fashion.
Complications, Incidence Rates, and Salvage Management
While surgical interventions for hallux rigidus yield high satisfaction rates, complications are well-documented and can be profoundly disabling if mismanaged. The orthopedic surgeon must be prepared to navigate both the biological failures of healing and the mechanical failures of alignment.
Recurrence of symptoms following a cheilectomy is the most common long-term complication, occurring in up to 10-15% of patients over a 10-year period. This is rarely a failure of the procedure itself, but rather the natural, inexorable progression of the underlying degenerative joint disease. As the remaining cartilage wears away, the patient transitions to a Grade 3 or 4 state, necessitating conversion to a first MTP joint arthrodesis.
In the realm of arthrodesis, symptomatic nonunion is the most feared biological complication, with reported incidence rates ranging from 5% to 10%. Nonunions are frequently hypertrophic, resulting from inadequate rigid fixation, or atrophic, stemming from thermal necrosis during reaming, inadequate debridement of sclerotic subchondral bone, or profound patient non-compliance (particularly active tobacco use).
Malunion represents a catastrophic mechanical failure. Fusing the toe in excessive plantarflexion (hallux flexus) creates a rigid lever that drives the tip of the distal phalanx into the ground during stance, causing severe tip pain, rapid destruction of the interphalangeal joint, and an inability to wear normal footwear. Conversely, fusing the toe in excessive dorsiflexion (hallux extensus) completely unloads the first ray. The massive forces normally borne by the first metatarsal are transferred laterally, resulting in intractable transfer metatarsalgia beneath the second and third metatarsal heads, and frequently leading to stress fractures of the lesser metatarsals.

Complications and Salvage Strategies
| Complication | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Progression of OA (Post-Cheilectomy) | 10 - 15% (at 10 yrs) | Natural history of degenerative joint disease. | Conversion to 1st MTP Arthrodesis. |
| Symptomatic Nonunion | 5 - 10% | Poor fixation, thermal necrosis, smoking, infection. | Revision arthrodesis with structural bone graft (calcaneal or iliac crest) and robust locked plating. |
| Malunion (Excessive Plantarflexion) | 2 - 5% | Intraoperative positioning error; failure to account for metatarsal declination. | Dorsal closing wedge osteotomy through the fusion mass to elevate the hallux. |
| Malunion (Excessive Dorsiflexion) | 2 - 5% | Intraoperative positioning error. | Plantar closing wedge osteotomy through the fusion mass; management of lesser toe metatarsalgia. |
| Hardware Prominence / Irritation | 10 - 20% | Thin dorsal soft tissue envelope overlying the titanium plate. | Hardware removal (only after 6-12 months once solid radiographic union is confirmed). |
| Deep Infection | < 2% | Contamination, compromised soft tissue envelope, diabetes. | Hardware removal, aggressive serial debridement, antibiotic spacer, delayed revision arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be strictly tailored to the specific surgical intervention performed. Joint-sparing procedures demand early, aggressive mobilization to prevent capsular scarring, whereas joint-sacrificing procedures require absolute immobilization and protection until biological osseous union is achieved.
Rehabilitation Following Cheilectomy:
The primary goal in the immediate postoperative phase is the prevention of intra-articular adhesions and capsular contracture, which would negate the surgical resection.
* Phase 1 (0 to 2 Weeks): The patient is placed in a rigid-soled postoperative shoe. Immediate heel-touch or flat-foot weight-bearing is permitted as tolerated. Crucially, active and passive range of motion exercises (specifically focusing on aggressive dorsiflexion) are initiated within 3 to 5 days postoperatively. Patients are instructed to manually stretch the hallux into extension multiple times a day.
* Phase 2 (2 to 6 Weeks): Sutures are removed at 2 weeks. The patient is transitioned into a wide-toed, stiff-soled athletic shoe. Physical therapy is formally initiated, focusing on gait retraining, intrinsic foot muscle strengthening, and maximizing the terminal arc of dorsiflexion.
* Phase 3 (> 6 Weeks): Patients are cleared to return to all activities, including high-impact sports and running, as tolerated by pain and swelling. Maximum medical improvement is typically realized between 3 to 6 months.
Rehabilitation Following Arthrodesis:
The objective here is the protection of the fixation construct to allow for primary bone healing across the fusion interface.
* Phase 1 (0 to 2 Weeks): The patient is placed in a rigid postoperative shoe or a controlled ankle motion (CAM) boot. Weight-bearing is strictly limited to the heel or the lateral border of the foot. The foot must remain elevated to minimize edema, which can compromise the dorsal incision.
* Phase 2 (2 to 6 Weeks): Sutures are removed. The patient remains in the CAM boot. Progressive flat-foot weight-bearing is slowly introduced, provided the patient remains in the rigid boot to completely bypass the propulsive forces of the first ray.
* Phase 3 (6 to 10 Weeks): At the 6-week mark, weight-bearing radiographs are obtained. If there is evidence of consolidating trabecular bone across the arthrodesis site, the patient is transitioned out of the boot and into a stiff-soled shoe with a rocker-bottom modification.
* Phase 4 (> 10 Weeks): Once complete radiographic union is confirmed (typically between 10 to 12 weeks), the patient is released to full, unrestricted activities. High-impact loading is discouraged until the 3-month mark to prevent late stress failures through the maturing fusion mass.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of hallux rigidus is heavily informed by a robust body of landmark orthopedic literature. The foundational text in modern classification remains the seminal 2003 study by Coughlin and Shurnas, published in the Journal of Bone and Joint Surgery. Their prospective analysis validated the 0-to-4 grading system, correlating clinical symptoms with radiographic findings, and definitively established that cheilectomy provides excellent long-term outcomes for Grade 1 and 2 disease, while arthrodesis remains the gold standard for Grade 3 and 4.
The biomechanical implications of first MTP joint arthrodesis were extensively mapped by Brodsky et al., who utilized dynamic gait analysis to demonstrate that a properly positioned first MTP fusion significantly improves overall foot kinematics and propulsive power, dispelling the historical myth that arthrodesis leads to a severely dysfunctional gait. Their work underscored that the restoration of a stable medial column outweighs the loss of sagittal plane motion at the MTP joint.
Furthermore, the precise spatial positioning guidelines for arthrodesis were refined by Stevens et al., who demonstrated through long-term follow-up that slight deviations in valgus and dorsiflexion angles are the primary drivers of postoperative patient dissatisfaction and transfer metatarsalgia. Current consensus guidelines from the American Orthopaedic Foot & Ankle Society (AOFAS) and the American Academy of Orthopaedic Surgeons (AAOS) strongly reaffirm these principles: conservative management should be exhausted first, cheilectomy is highly effective for
