Advanced Arthroscopy and Tendoscopy of the Foot and Ankle: First MTP Joint and Hindfoot Tendons
Key Takeaway
First metatarsophalangeal (MTP) joint arthroscopy and hindfoot tendoscopy are advanced, minimally invasive techniques used to treat osteochondral lesions, synovitis, and tendon pathology. This guide details the precise portal placements, surgical anatomy, and operative steps required for successful first MTP arthroscopy, peroneal tendoscopy, and posterior tibial tendoscopy, providing orthopedic surgeons with evidence-based protocols to optimize patient outcomes and minimize iatrogenic complications.
Comprehensive Introduction and Patho-Epidemiology
The evolution of small joint arthroscopy and tendoscopy has fundamentally revolutionized the management paradigm of foot and ankle pathology. Historically, orthopedic surgeons were relegated to performing extensive open arthrotomies and morbid tenolyses to address intra-articular and peritendinous lesions. These traditional open approaches, while effective in exposing pathology, inherently violated the delicate soft tissue envelope of the distal extremity, frequently resulting in significant postoperative morbidity, severe arthrofibrosis, prolonged rehabilitation trajectories, and heightened risks of wound dehiscence. Today, first metatarsophalangeal (MTP) joint arthroscopy, executed alongside sophisticated peroneal and posterior tibial tendoscopy, offers the modern orthopedic surgeon a highly advanced, minimally invasive armamentarium. These techniques allow for the meticulous diagnosis and treatment of complex conditions with unparalleled visualization, significantly mitigating the iatrogenic trauma associated with classical surgical exposures.
The patho-epidemiology of first MTP joint disorders underscores the necessity for these advanced interventions. Hallux rigidus, the most prevalent osteoarthritic condition of the foot, affects approximately 1 in 45 individuals over the age of 50. The precise etiology is multifactorial, encompassing repetitive microtrauma, altered joint kinematics, and underlying anatomical predispositions such as an elevated first ray (metatarsus primus elevatus). Early-stage hallux rigidus (Coughlin and Shurnas Grades I and II) is characterized by dorsal osteophytosis and focal chondral degradation, primarily on the metatarsal head. Similarly, osteochondral lesions (OCLs) of the first MTP joint, often sequelae of acute hyperextension injuries (turf toe) or insidious osteochondritis dissecans, present a significant clinical challenge. Arthroscopic intervention in these early stages disrupts the pathophysiological cascade of joint degeneration, preserving the articular cartilage and delaying the need for salvage procedures such as arthrodesis or arthroplasty.
In the hindfoot, peritendinous pathology represents a substantial burden of disease, particularly in athletic and aging populations. Peroneal tendon disorders, including tenosynovitis, subluxation, and longitudinal split tears, are frequently encountered in the context of chronic lateral ankle instability or acute inversion trauma. The incidence of peroneal pathology in patients with persistent lateral ankle pain is reported to be as high as 30%. Conversely, posterior tibial tendon dysfunction (PTTD) is the leading cause of adult-acquired flatfoot deformity. The pathogenesis of PTTD involves a progressive, degenerative tendinosis, initially manifesting as florid tenosynovitis (Stage I) before advancing to structural elongation and macroscopic tearing (Stage II). The critical watershed area of the posterior tibial tendon, located posterior and distal to the medial malleolus, renders it highly susceptible to ischemic degeneration under repetitive mechanical load.
The paradigm shift toward tendoscopy for these hindfoot conditions is driven by the profound anatomical and physiological advantages of the technique. By utilizing standard arthroscopic equipment within the tendon sheath, surgeons can perform aggressive tenosynovectomies, debride partial-thickness tears, and assess dynamic tendon stability without disrupting the critical retinacular structures or the delicate vincula that supply the tendon. This minimally invasive approach preserves the physiological gliding mechanism of the tendon, drastically reducing the incidence of postoperative adhesions that historically plagued open tenolysis procedures. As our understanding of foot and ankle pathoanatomy continues to evolve, the application of small joint arthroscopy and tendoscopy will undoubtedly expand, solidifying its role as an indispensable component of contemporary operative orthopedics.
Detailed Surgical Anatomy and Biomechanics
First Metatarsophalangeal Joint Anatomy
The first metatarsophalangeal joint is a highly constrained, complex diarthrodial joint that must withstand immense biomechanical forces, frequently bearing up to 120% of total body weight during the push-off phase of the normal gait cycle. The osseous architecture consists of the convex, asymmetrical head of the first metatarsal articulating with the shallow, concave base of the proximal phalanx. The metatarsal head exhibits a distinct "cam effect," where its radius of curvature increases dorsally, necessitating complex sliding and rolling kinematics to achieve normal hallux dorsiflexion. Plantarly, the metatarsal head is divided by a prominent crista into medial and lateral facets, which articulate with the tibial and fibular sesamoids, respectively. This sesamoid complex acts as a fulcrum, increasing the mechanical advantage of the flexor hallucis brevis (FHB) and absorbing tremendous load during terminal stance.
The stability of the first MTP joint is dictated by an intricate capsuloligamentous network. The collateral ligament complex is composed of the proper collateral ligament (inserting on the proximal phalanx) and the accessory collateral ligament (inserting on the plantar plate and sesamoids). The plantar plate, a thick fibrocartilaginous structure, represents the primary static restraint to dorsal translation of the proximal phalanx. Arthroscopically, the surgeon must possess a profound three-dimensional understanding of these structures to navigate the tight joint space safely. The medial and lateral gutters, the dorsal capsular reflection, and the articular surfaces of the sesamoids must be systematically evaluated without causing iatrogenic scuffing of the articular cartilage.
Neurovascular anatomy surrounding the first MTP joint dictates safe portal placement. The dorsomedial cutaneous nerve, a terminal arborization of the superficial peroneal nerve, courses in perilous proximity to the standard dorsomedial portal. Injury to this nerve results in debilitating neuromas and paresthesias over the medial hallux. Laterally, the deep peroneal nerve and the dorsal metatarsal artery lie adjacent to the extensor hallucis brevis (EHB) tendon. The surgeon must meticulously palpate these landmarks and utilize a "nick and spread" technique, employing blunt dissection down to the joint capsule to displace these critical neurovascular structures safely out of the trajectory of the arthroscopic trocar.
Peroneal Tendon Complex Anatomy
The peroneal tendons traverse a complex anatomical course that predisposes them to mechanical attrition and impingement. Originating from the lateral compartment of the leg, the peroneus brevis and peroneus longus tendons descend toward the lateral malleolus. At the level of the retromalleolar groove, the peroneus brevis is situated anterior and medial (deep) to the peroneus longus, directly abutting the posterior fibula. The retromalleolar groove is deepened by a fibrocartilaginous ridge, which, if incompetent or congenitally shallow, contributes to tendon subluxation. The tendons are constrained within this groove by the superior peroneal retinaculum (SPR), a critical stabilizing structure that originates from the posterolateral fibula and inserts onto the lateral calcaneal wall.
Distal to the fibula, the tendons course toward the peroneal tubercle of the calcaneus, where they are enveloped by the inferior peroneal retinaculum (IPR). The peroneus brevis continues distally to insert on the base of the fifth metatarsal, while the peroneus longus curves acutely plantarly around the cuboid to insert on the base of the first metatarsal and medial cuneiform. The presence of an os peroneum, a sesamoid bone within the peroneus longus tendon at the level of the calcaneocuboid joint, can be a source of localized pathology and must be evaluated during tendoscopic exploration. The vascular supply to the tendons is segmental, delivered via microscopic vincula within the mesotendon. Tendoscopy allows for the preservation of these delicate vascular tethers, which are frequently sacrificed during extensive open exposures.
The primary neurological structure at risk during peroneal tendoscopy is the sural nerve. The sural nerve courses distally along the posterolateral aspect of the leg, crossing the peroneal tendons from posterior to anterior approximately 1 to 2 cm distal to the tip of the lateral malleolus. The proximity of the sural nerve to the standard distal portal makes it highly vulnerable to transection or thermal injury from radiofrequency devices. Surgeons must maintain a heightened awareness of the nerve's trajectory, utilizing transillumination techniques and blunt soft-tissue dissection to ensure the nerve is safely retracted before introducing motorized instrumentation into the tendon sheath.
Posterior Tibial Tendon Anatomy
The posterior tibial tendon (PTT) is the primary dynamic stabilizer of the medial longitudinal arch. Originating from the posterior aspect of the interosseous membrane, the tibia, and the fibula, the muscle belly transitions into a robust tendon in the distal third of the leg. It courses posterior to the medial malleolus within a distinct fibro-osseous tunnel, constrained by the flexor retinaculum. The tendon then takes a sharp anterior turn to insert primarily on the navicular tuberosity, with extensive secondary plantar slips to the cuneiforms, cuboid, and bases of the second through fourth metatarsals. This extensive insertion footprint allows the PTT to effectively invert the hindfoot, lock the transverse tarsal joint, and elevate the medial arch during the stance phase of gait.
The vascularity of the posterior tibial tendon is of paramount clinical significance. Angiographic studies have demonstrated a distinct zone of hypovascularity, or "watershed area," extending from the medial malleolus to the navicular insertion. This region relies heavily on synovial diffusion for nutrition, making it highly susceptible to degenerative tearing when subjected to the repetitive tensile loads of weight-bearing. In the early stages of PTTD, the synovial sheath undergoes florid hypertrophy in an attempt to increase nutrient delivery to the ischemic tendon, resulting in the characteristic tenosynovitis observed clinically and tendoscopically.
Surgical navigation of the PTT sheath requires meticulous attention to the surrounding neurovascular anatomy. The great saphenous vein and the saphenous nerve course anterior to the medial malleolus and are at risk during the establishment of the distal portal near the navicular. More critically, the posterior tibial neurovascular bundle (comprising the posterior tibial artery, accompanying veins, and the tibial nerve) lies immediately posterior and lateral to the PTT within the tarsal tunnel. Aggressive or misdirected use of motorized shavers within the proximal tendon sheath can result in catastrophic vascular injury or nerve transection. The surgeon must maintain strict spatial orientation, keeping the cutting window of the shaver directed anteriorly toward the tendon and away from the posterior neurovascular bundle at all times.
Exhaustive Indications and Contraindications
The success of small joint arthroscopy and tendoscopy is inextricably linked to rigorous patient selection and precise adherence to established indications. While these minimally invasive techniques offer substantial benefits, they are not panaceas for all foot and ankle pathology. The surgeon must synthesize clinical examination findings, advanced imaging data, and an understanding of the patient's physiological demands to determine the appropriateness of endoscopic intervention.
For the first MTP joint, arthroscopy is highly efficacious for intra-articular pathology in the setting of preserved joint space. Osteochondral lesions of the metatarsal head, particularly those that are symptomatic following a trial of conservative management, are prime indications. Arthroscopy allows for precise debridement of unstable cartilage flaps and the execution of marrow stimulation techniques (microfracture) to promote fibrocartilage infill. In the context of hallux rigidus, arthroscopy is indicated for Coughlin and Shurnas Grades I and II, where the primary pathology is dorsal impingement from osteophytes. Arthroscopic cheilectomy effectively resects these impinging lesions, restoring dorsiflexion while minimizing surgical morbidity. However, advanced hallux rigidus (Grades III and IV) with global joint space obliteration is an absolute contraindication to arthroscopic joint preservation, as the procedure cannot address the profound cartilage loss and may paradoxically exacerbate symptoms.
Tendoscopy of the hindfoot is indicated for both diagnostic and therapeutic purposes in the setting of peritendinous pathology. For the peroneal tendons, chronic tenosynovitis that remains refractory to immobilization, physical therapy, and judicious corticosteroid injections is a classic indication. Tendoscopy allows for thorough synovectomy and the identification of subtle, partial-thickness longitudinal split tears of the peroneus brevis, which are frequently missed on preoperative MRI. If a tear involves less than 50% of the tendon's cross-sectional area, it can be effectively debrided and tubularized endoscopically. Similarly, for the posterior tibial tendon, tendoscopy is the gold standard for managing Stage I PTTD. Aggressive tenosynovectomy in this stage can halt the progression of the disease and prevent structural tendon failure. In early Stage II PTTD, tendoscopy is often utilized as an adjunct to joint-sparing bony procedures, such as a medializing calcaneal osteotomy, to address the intra-sheath pathology simultaneously.
Contraindications to these procedures must be strictly respected to avoid devastating complications. Active localized soft tissue infection or generalized sepsis represents an absolute contraindication to any elective arthroscopic or tendoscopic procedure. Severe vascular compromise, advanced peripheral neuropathy (e.g., Charcot neuroarthropathy), and profound anatomical deformity that precludes safe portal placement or instrument navigation are also absolute contraindications. Relative contraindications include previous open surgery in the same anatomical region, which may result in severe adhesions and distorted neurovascular anatomy, significantly increasing the risk of iatrogenic injury during portal establishment.
Indications and Contraindications Mapping
| Pathology / Procedure | Primary Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| First MTP Arthroscopy | - Osteochondral Lesions (OCLs) - Early Hallux Rigidus (Grades I/II) - Loose bodies / Synovial chondromatosis - Inflammatory synovitis (RA, Gout) - Arthrofibrosis release |
- Prior extensive open MTP surgery - Moderate joint space narrowing - Severe hallux valgus deformity (>40 degrees) |
- End-stage Hallux Rigidus (Grades III/IV) - Active joint infection / cellulitis - Charcot neuroarthropathy - Severe peripheral arterial disease |
| Peroneal Tendoscopy | - Refractory tenosynovitis - Partial tears (<50% cross-section) - Recurrent subluxation assessment - Low-lying muscle belly impingement - Os peroneum pathology evaluation |
- Previous open tenolysis/repair - Massive tears requiring graft - Severe lateral ankle instability requiring concurrent open lateral ligament reconstruction |
- Active soft tissue infection - Complete tendon rupture with retraction - Fixed hindfoot varus deformity (requires bony correction) |
| PTT Tendoscopy | - Stage I PTTD (Tenosynovitis) - Early Stage II PTTD (adjunctive) - Post-traumatic adhesions - Partial interstitial tearing |
- Moderate to severe flexible flatfoot - Previous medial ankle surgery - Significant obesity (limits rehab) |
- Stage III/IV PTTD (Rigid deformity) - Complete PTT rupture - Active localized infection - Unmanaged profound diabetes mellitus |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful small joint arthroscopy and tendoscopy. The diagnostic workup must include high-quality, weight-bearing orthogonal radiographs to assess overall alignment, joint space preservation, and the presence of osseous anomalies (e.g., os peroneum, accessory navicular). Advanced imaging is virtually mandatory. High-resolution Magnetic Resonance Imaging (MRI) without contrast is the modality of choice for evaluating the integrity of the capsuloligamentous structures, the extent of osteochondral lesions, and the morphological status of the tendons. Dynamic ultrasound, performed by an experienced musculoskeletal radiologist or the operating surgeon, is an invaluable adjunct, particularly for assessing dynamic peroneal tendon subluxation or the gliding mechanics of the PTT within its sheath.
Anesthesia for these procedures is tailored to patient comorbidities and surgeon preference, but regional anesthesia is highly favored. A comprehensive ankle block, utilizing a long-acting local anesthetic (e.g., bupivacaine or ropivacaine), provides excellent intraoperative anesthesia and profound postoperative analgesia, facilitating early discharge in the ambulatory setting. General anesthesia or conscious sedation may be employed concurrently to ensure patient comfort, particularly during the application of the pneumatic thigh or calf tourniquet, which is essential for maintaining a bloodless surgical field. The tourniquet is typically inflated to 250-300 mmHg following exsanguination of the limb with an Esmarch bandage.
Patient positioning is procedure-specific and critical for optimal surgical ergonomics and anatomical access. For first MTP joint arthroscopy, the patient is positioned supine on the operating table. The operative leg is extended, and a non-invasive distraction device is applied. A sterile Chinese finger trap is secured to the hallux, and a traction cord is connected to a distraction apparatus fixed to the end of the table. Approximately 5 to 10 pounds of longitudinal traction is applied. This traction is imperative to overcome the inherent capsular constraints of the first MTP joint, opening the articular space sufficiently to accommodate the arthroscope and instrumentation without causing iatrogenic scuffing of the delicate chondral surfaces.
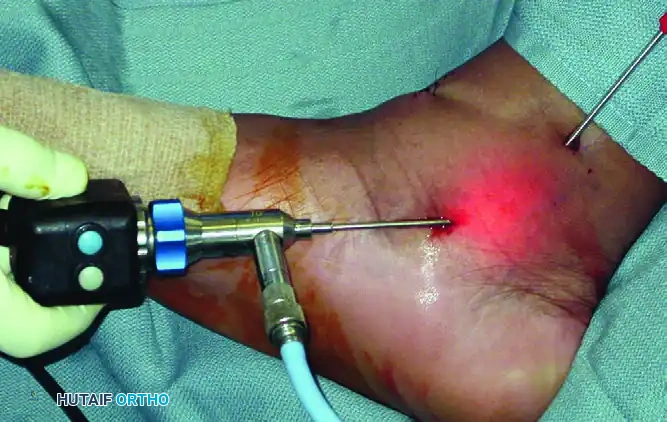
For peroneal tendoscopy, the patient is typically positioned in the lateral decubitus position, which affords unparalleled, direct access to the lateral hindfoot and retromalleolar region. Alternatively, a supine position with a large, firm bump placed under the ipsilateral hip can be utilized to internally rotate the leg maximally.

As demonstrated in the surgical setup above, the lateral aspect of the ankle is exposed. The bony landmarks, including the lateral malleolus, the course of the peroneal tendons, and the anticipated portal sites, are meticulously mapped out with a surgical marker prior to exsanguination. This precise topographical mapping is crucial for maintaining orientation once the limb is draped and the anatomical contours are obscured.
For posterior tibial tendoscopy, the patient is positioned supine. To expose the medial aspect of the ankle optimally, the operative leg is externally rotated and abducted into a "frog-leg" position, with the lateral malleolus resting on the contralateral anterior tibia or a dedicated positioning bump.
As illustrated in the operative image above, this positioning brings the medial malleolus and the course of the posterior tibial tendon directly into the surgeon's operative field. The surgeon typically stands on the side of the operative limb, with the arthroscopic tower positioned directly across the table for an unobstructed line of sight.
Step-by-Step Surgical Approach and Fixation Technique
First MTP Joint Arthroscopy
The procedure commences with the establishment of the dorsomedial and dorsolateral portals. Following the application of longitudinal traction, the joint is insufflated with 2 to 3 mL of sterile normal saline using an 18-gauge needle inserted just medial to the extensor hallucis longus (EHL) tendon at the level of the joint line. This distension creates a safe working space and pushes the capsule away from the articular cartilage. The dorsomedial portal is established first. A #11 scalpel blade is used to incise only the epidermal and dermal layers. A small mosquito hemostat is then introduced and used to bluntly dissect through the subcutaneous tissue down to the joint capsule. This "nick and spread" technique is absolutely critical to sweep the delicate branches of the dorsomedial cutaneous nerve out of the path of the trocar.
A 1.9-mm or 2.7-mm, 30-degree short arthroscope is introduced through the dorsomedial portal. Under direct intra-articular visualization, an 18-gauge spinal needle is utilized to localize the optimal trajectory for the dorsolateral portal, situated just lateral to the EHL tendon. Once the position is confirmed, the dorsolateral portal is established using identical blunt dissection techniques to protect the deep peroneal nerve and dorsal metatarsal artery. A systematic diagnostic round is then performed, evaluating the metatarsal head, the base of the proximal phalanx, the medial and lateral gutters, and the plantar sesamoid articulation.
Therapeutic intervention is dictated by the pathology. For osteochondral lesions, a 2.0-mm or 2.9-mm motorized shaver is introduced to debride fibrillated cartilage to a stable, vertical rim. The necrotic subchondral bone bed is then prepared using a microfracture awl or a 0.045-inch Kirschner wire to penetrate the subchondral plate, releasing marrow elements to stimulate fibrocartilage regeneration. In cases of early hallux rigidus, a small, hooded burr is utilized to resect the dorsal osteophytes on the metatarsal head (arthroscopic cheilectomy). The surgeon must dynamically assess dorsiflexion intraoperatively, continuing the resection until impingement is eliminated and a functional range of motion is restored.
Peroneal Tendoscopy
Peroneal tendoscopy relies on precise portal placement along the course of the tendon sheath. The distal portal is established approximately 1.5 to 2 cm distal to the tip of the lateral malleolus, directly over the palpable peroneal tendons. The proximal portal is placed 2 to 3 cm proximal to the tip of the lateral malleolus. Following blunt dissection to the tendon sheath, a 2.7-mm arthroscope is introduced into the proximal portal.
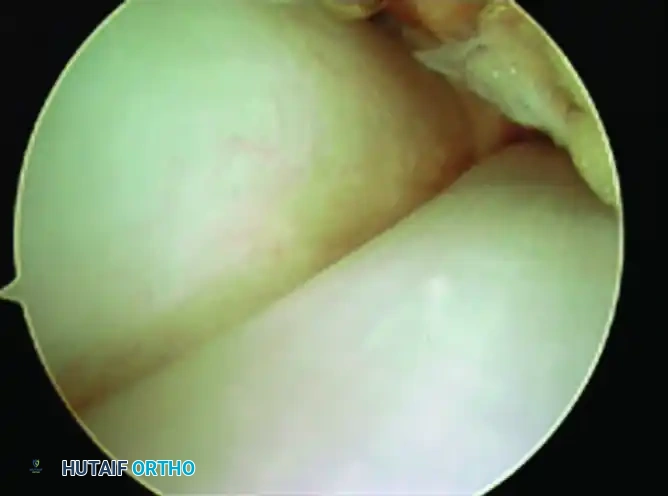
Upon initial entry, the visual field is frequently obscured by hypertrophic, hypervascular synovium. A 2.9-mm shaver is introduced through the distal portal, and a localized synovectomy is performed to establish a clear optical cavity. As seen in the arthroscopic view above, once the sheath is cleared, the anatomical relationship between the tendons becomes strikingly evident. The peroneal brevis tendon (a) is situated medial and deep, directly apposing the fibula, while the peroneus longus tendon (b) lies superficial and lateral.
The surgeon dynamically examines the tendons by passively everting and inverting the ankle, pulling the tendons through the retromalleolar groove. This maneuver exposes interstitial fraying or longitudinal split tears, which most commonly affect the peroneus brevis due to mechanical impingement against the fibular ridge. Frayed edges are meticulously debrided using a motorized shaver or a bipolar radiofrequency wand, taking care not to damage intact collagen bundles. If a significant tear is identified that compromises more than 50% of the tendon substance, the tendoscopic procedure is efficiently converted to a limited open approach for formal tubularization and repair.
Posterior Tibial Tendoscopy
The portals for posterior tibial tendoscopy are established along the anatomical trajectory of the tendon, posterior and distal to the medial malleolus. The proximal portal is placed 2 to 3 cm proximal to the tip of the medial malleolus, while the distal portal is located near the navicular insertion. The "nick and spread" technique is paramount here to avoid injury to the saphenous nerve distally and the posterior tibial neurovascular bundle proximally.
The 2.7-mm arthroscope is typically introduced through the distal portal, directed proximally in a retrograde fashion. In patients with Stage I PTTD, the surgeon will immediately encounter dense, inflammatory tissue characteristic of florid tenosynovitis. A motorized shaver is introduced through the proximal portal, and an aggressive, circumferential tenosynovectomy is performed. The shaver blade must always be directed toward the tendon and away from the posterior neurovascular bundle.
Following synovectomy, the underlying tendon is critically evaluated. The normal PTT should exhibit a taut, glistening, white appearance with distinct longitudinal collagen striations. Degenerative changes manifest as dull, yellowish, fibrillated tissue with loss of normal tension. Small partial tears are debrided. However, if the tendon is found to be profoundly attenuated, structurally elongated, or exhibits massive intrasubstance tearing, tendoscopy alone is insufficient. The procedure must be abandoned in favor of an open reconstruction, typically involving excision of the diseased PTT segment and a flexor digitorum longus (FDL) tendon transfer to the navicular, often augmented with a medializing calcaneal osteotomy to correct the underlying biomechanical deformity.
Complications, Incidence Rates, and Salvage Management
While small joint arthroscopy and tendoscopy are heralded for their minimally invasive nature, they are not devoid of significant risks. The confined anatomical spaces, the proximity of critical neurovascular structures, and the reliance on motorized instrumentation create a unique complication profile that the orthopedic surgeon must proactively manage. A profound understanding of these potential pitfalls is essential for complication avoidance and effective salvage when adverse events occur.
Neurological injury remains the most frequently reported complication across all foot and ankle endoscopic procedures, with an overall incidence ranging from 2% to 10%. These injuries are typically transient neurapraxias resulting from traction, direct trauma from portal placement, or thermal injury from radiofrequency devices. In first MTP arthroscopy, the dorsomedial cutaneous nerve is highly susceptible. In peroneal tendoscopy, the sural nerve is at significant risk near the distal portal. During PTT tendoscopy, the saphenous nerve can be injured distally, and catastrophic injury to the tibial nerve can occur proximally. Meticulous blunt dissection during portal establishment is the primary defense against these injuries.
Iatrogenic tendon damage is a severe complication unique to tendoscopy. The aggressive use of a motorized shaver within the tight confines of a tendon sheath can easily inadvertently resect healthy, load-bearing tendon fibers, precipitating a complete rupture. Surgeons must adhere to strict spatial awareness, utilizing the smooth, non-cutting side of the shaver hood to protect the tendon while selectively resecting the pathological synovium. Furthermore, excessive fluid extravasation is a significant concern. The continuous infusion of pressurized
