Comprehensive Management of Hallux Sesamoid Injuries: Diagnosis and Surgical Techniques

Key Takeaway
Hallux sesamoid injuries encompass a spectrum of pathologies, including sesamoiditis, fractures, and osteochondritis dissecans. The tibial sesamoid is most frequently affected due to its central weight-bearing position. Accurate diagnosis relies on localized palpation and specialized axial and oblique radiographs. While conservative management with orthoses and activity modification is the first-line approach, refractory cases may require meticulous surgical excision, carefully preserving the flexor hallucis longus and proper digital nerves to optimize functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The clinical recognition and subsequent management of hallux sesamoid pathology have expanded significantly, evolving from a historically overlooked subset of forefoot pain into a highly specialized domain within sports medicine and advanced foot and ankle surgery. While acute injuries to the sesamoids—such as those sustained during high-impact athletic activities, sudden forced hyperextension, or falls from heights—are typically recognized with alacrity due to their dramatic clinical presentation, more subtle, insidious pathological conditions frequently escape initial diagnosis. These chronic, low-grade presentations often masquerade as non-specific forefoot pain, leading to protracted periods of misdiagnosis and inappropriate therapeutic interventions. The umbrella term "sesamoiditis" has historically been employed as a catch-all diagnosis for chronic inflammatory conditions of a traumatic, infectious, or arthritic origin affecting the hallucal sesamoids. However, contemporary orthopedic understanding recognizes that this term grossly oversimplifies a complex, multifactorial array of underlying structural and biomechanical issues.


Epidemiologically, sesamoid pathology exhibits a strong predilection for specific patient populations, most notably athletes engaged in sports requiring repetitive, high-velocity loading of the first ray. Dancers, sprinters, gymnasts, and turf-sport athletes are disproportionately affected. The tibial (medial) sesamoid is overwhelmingly the most commonly injured of the two, a vulnerability directly attributable to its central location beneath the first metatarsal head, which subjects it to immense, concentrated axial loading during the terminal stance and push-off phases of the gait cycle. In contrast, the fibular (lateral) sesamoid, while less frequently traumatized, is more prone to degenerative changes secondary to altered forefoot mechanics, such as those seen in progressive hallux valgus deformities where the sesamoid apparatus subluxates laterally.
The pathophysiology of sesamoid injuries spans a broad spectrum, from acute osteochondral fractures to insidious stress responses and avascular necrosis (AVN). Repetitive microtrauma, particularly in the presence of a bipartite sesamoid, can lead to a disruption of the syndesmotic or synchondrotic union. This chronic stress through the fibrocartilaginous junction weakens the structural integrity of the complex, ultimately culminating in a displaced "fracture" through the synchondrosis. This specific pathological entity is notoriously resistant to conservative healing modalities due to the constant tensile forces exerted by the flexor hallucis brevis (FHB) tendon and the relatively tenuous vascular supply to the sesamoids. Furthermore, the sesamoids are highly susceptible to a myriad of specific localized conditions, including chondromalacia, flexor hallucis brevis tendinopathy, osteochondritis dissecans (OCD), and intractable plantar keratoses (IPK) secondary to prominent plantar condyles.
Recognizing the exact etiology of sesamoid pathology is paramount for dictating appropriate treatment algorithms. Inflamed bursae, diffuse callus formation beneath the tibial sesamoid, or localized hyperkeratotic lesions often herald severe underlying structural aberrations rather than simple dermatological issues. The orthopedic surgeon must maintain a high index of suspicion, as delayed diagnosis of conditions such as sesamoid AVN or un-united stress fractures can lead to rapid, irreversible degenerative joint disease (DJD) of the first metatarsophalangeal (MTP) joint. A comprehensive understanding of the patho-epidemiology is therefore the foundational prerequisite for any clinician evaluating plantar first MTP joint pain.
Detailed Surgical Anatomy and Biomechanics
The hallucal sesamoids are a pair of specialized ossicles intimately embedded within the tendinous slips of the flexor hallucis brevis muscle, situated precisely beneath the plantar aspect of the first metatarsal head. Embryologically, these structures cartilaginous precursors appear around the eighth week of fetal development, with ossification typically commencing between the ages of 8 and 10 years in females and 10 and 12 years in males. The ossification process is frequently multicentric, which accounts for the relatively high incidence of bipartite or multipartite sesamoids observed in the general population. A bipartite tibial sesamoid is present in approximately 10% to 30% of individuals, and in 25% of these cases, the condition is bilateral. The fibular sesamoid, conversely, is rarely bipartite, a distinction that holds significant clinical relevance when evaluating radiographic anomalies.
Osteologically, the sesamoids articulate with the plantar facets of the first metatarsal head, forming the sesamoidometatarsal joint. A prominent ridge on the plantar aspect of the metatarsal head—the crista—separates the medial and lateral facets, effectively tracking the sesamoids during MTP joint range of motion. The capsuloligamentous complex stabilizing the sesamoids is highly intricate. The sesamoids are tethered to each other by the robust intersesamoid ligament, which forms the roof of the fibro-osseous tunnel through which the flexor hallucis longus (FHL) tendon glides. Proximally, they are anchored by the FHB muscle belly; distally, they attach to the base of the proximal phalanx via the thick plantar plate. Medially and laterally, the sesamoids are stabilized by the collateral and sesamoidophalangeal ligaments, as well as the dynamic expansions of the abductor hallucis and adductor hallucis muscles, respectively.
Biomechanically, the hallucal sesamoids serve several critical, load-bearing, and kinematic functions. Primarily, they act as a vital fulcrum, significantly increasing the moment arm and mechanical advantage of the FHB muscle during plantarflexion of the hallux. This mechanism is essential for achieving rigid stabilization of the first ray during the propulsive push-off phase of gait. Secondly, the sesamoids function as a protective conduit, elevating the metatarsal head to reduce friction and compressive forces on the FHL tendon as it traverses the plantar aspect of the joint. Without the sesamoids, the FHL would be subjected to severe attritional wear against the metatarsal head.
Furthermore, the sesamoids play a paramount role in load distribution and shock absorption. During the terminal stance phase of the gait cycle, the first MTP joint is subjected to immense vertical and shear forces, with the sesamoids absorbing and dissipating up to 300% of total body weight. The tibial sesamoid bears a disproportionately higher percentage of this load compared to the fibular sesamoid, further explaining its higher propensity for traumatic and stress-related injuries. Hyperextension of the first MTP joint combined with axial loading—the classic "turf toe" mechanism—places maximal tensile stress on the plantar plate and compressive stress on the sesamoidometatarsal articulation, frequently resulting in acute fractures, chondral shear injuries, or severe sprains of the stabilizing capsuloligamentous complex.
Exhaustive Indications and Contraindications
The decision-making process regarding the surgical management of hallux sesamoid pathology is nuanced and must be predicated on a rigorous, exhaustive trial of conservative therapies. Surgical intervention, primarily in the form of a partial or total sesamoidectomy, is strictly reserved for patients who have demonstrated recalcitrant symptoms despite a minimum of 6 to 12 months of optimized non-operative management. The initial treatment algorithm must include strict modification of weight-bearing activities, nonsteroidal anti-inflammatory drugs (NSAIDs), custom orthoses with specific sesamoid offloading wells, and prolonged periods of immobilization in a controlled ankle motion (CAM) boot. Only when these modalities fail to provide functional relief should operative excision be entertained.
Specific indications for sesamoidectomy are well-defined within the orthopedic literature. The most frequent indication is a painful non-union of a sesamoid fracture that has failed prolonged immobilization and bone stimulation. Similarly, symptomatic bipartite sesamoids that exhibit chronic diastasis and localized pain unresponsive to offloading are prime candidates for excision. Advanced avascular necrosis (AVN) of the sesamoid, often presenting with fragmentation, sclerosis, and collapse on advanced imaging, represents an absolute indication for surgical removal, as the necrotic bone acts as an abrasive loose body within the joint, accelerating global MTP joint arthrosis. Furthermore, intractable plantar keratoses (IPK) or deep bursitis driven by a prominent, hypertrophic sesamoid exostosis that fails aggressive conservative paring and padding necessitates surgical enucleation of the offending bony prominence.


Contraindications to sesamoidectomy must be meticulously respected to avoid catastrophic postoperative complications. Active localized soft tissue infection or osteomyelitis requires appropriate antimicrobial therapy and potential debridement prior to definitive sesamoid excision. Severe peripheral vascular disease is an absolute contraindication, as the relatively tenuous blood supply to the plantar forefoot can lead to disastrous wound healing complications and potential necrosis following surgical insult. Complex regional pain syndrome (CRPS) affecting the lower extremity is a strong relative contraindication; surgical trauma in these patients frequently exacerbates the neuropathic pain cycle, leading to outcomes far worse than the baseline pathology.
The most critical biomechanical contraindication is the simultaneous excision of both the tibial and fibular sesamoids (total sesamoidectomy). Excision of both sesamoids completely obliterates the intrinsic stabilizing mechanism of the first MTP joint, invariably resulting in a severe, progressive hallux malleus (cock-up) deformity. This occurs due to the unopposed pull of the extensor hallucis longus (EHL) and extensor hallucis brevis (EHB) muscles once the plantar flexor apparatus is rendered incompetent. If bilateral sesamoid pathology is so severe that both must be removed, the surgeon must concomitantly perform a primary arthrodesis of the first MTP joint to provide definitive stability and prevent this debilitating cascade.
| Indication Category | Specific Pathologies Warranting Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Traumatic | Painful non-union of acute fracture; Chronic diastasis of bipartite synchondrosis | Active local or systemic infection | Poorly controlled diabetes mellitus |
| Degenerative/Vascular | Avascular Necrosis (AVN) with fragmentation; Severe localized osteoarthritis | Excision of BOTH sesamoids (without concurrent MTP arthrodesis) | Pre-existing asymptomatic hallux valgus/varus |
| Mechanical/Soft Tissue | Intractable Plantar Keratosis (IPK); Recalcitrant bursitis; Hypertrophic exostosis | Severe peripheral arterial disease (PAD) | Complex Regional Pain Syndrome (CRPS) |
| Infectious | Chronic, localized osteomyelitis failing targeted IV antibiotic therapy | Inadequate soft tissue envelope for closure | Heavy tobacco use (impairs wound healing) |
Pre-Operative Planning, Templating, and Patient Positioning
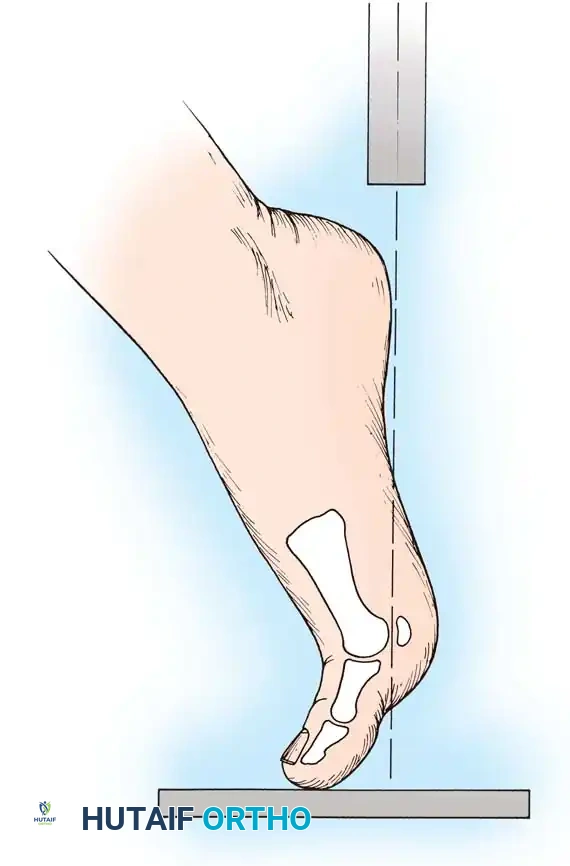
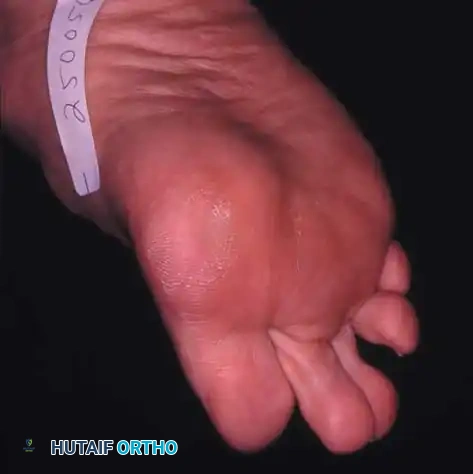
Thorough pre-operative planning begins with a meticulous clinical evaluation to precisely localize the pathology. Patients typically present with diffuse, aching pain around the plantar aspect of the first MTP joint, which can easily mimic gout, hallux rigidus, FHL tendinitis, or a plantar plate rupture. The surgeon must perform targeted, pinpoint palpation of each individual sesamoid. Tenderness highly localized to the medial eminence suggests tibial sesamoid pathology, whereas pain deep in the first web space implicates the fibular sesamoid. The "passive dorsiflexion test" is critical: extending the hallux places the FHB complex under maximum tension, drawing the sesamoids distally into the metatarsal condyles and exacerbating pain in the presence of intra-articular pathology or stress fractures.
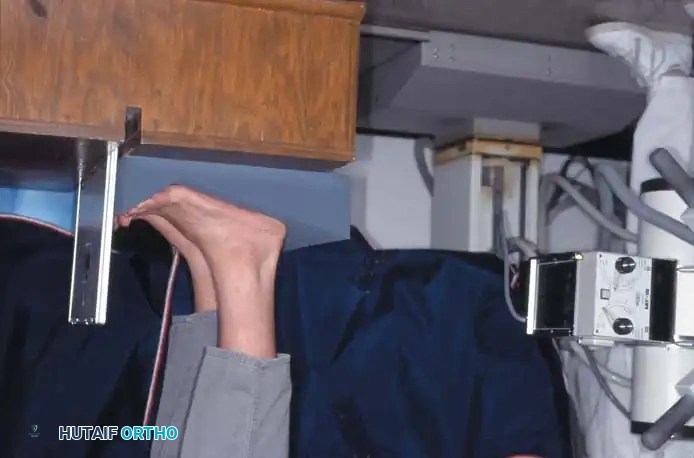
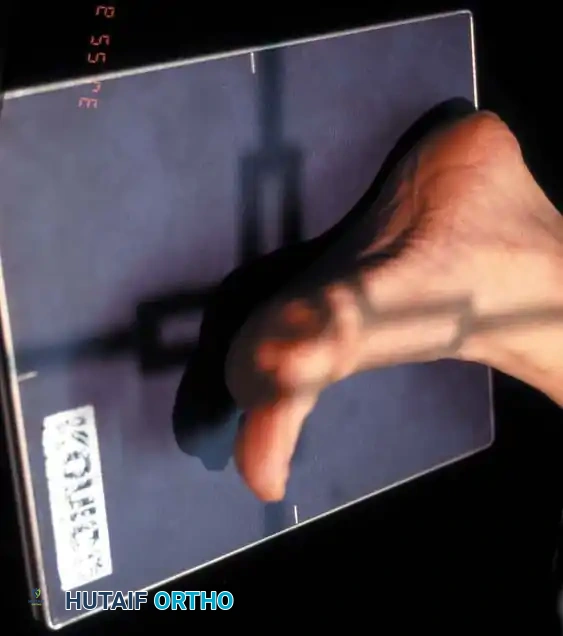
Radiographic evaluation is the cornerstone of pre-operative templating. Standard anteroposterior (AP) and lateral views of the weight-bearing foot are mandatory but often insufficient for definitive diagnosis due to osseous overlap. Specialized views are absolutely critical. The medial oblique view is highly effective for profiling the tibial sesamoid, separating it from the metatarsal head shadow. The axial sesamoid view is the gold standard for assessing the sesamoidometatarsal articulation. This tangential projection allows the surgeon to evaluate joint space narrowing, subluxation, the integrity of the crista, and the presence of coronal plane fractures.



When standard radiographs are equivocal but clinical suspicion remains high, advanced imaging is indicated. Magnetic Resonance Imaging (MRI) is the modality of choice for identifying occult stress fractures, bone marrow edema indicative of early AVN, and concomitant soft tissue pathology such as FHB tears or intersesamoid ligament ruptures. If differentiating between a bipartite sesamoid and a true fracture is challenging, Computed Tomography (CT) provides unparalleled osseous detail; a bipartite sesamoid will exhibit smooth, well-corticated, sclerotic margins, whereas an acute or subacute fracture will display sharp, irregular, non-sclerotic edges without cortication.
In the operating theater, precise patient positioning and setup are vital for ensuring optimal surgical exposure and minimizing iatrogenic trauma. The patient is placed in the supine position on a standard radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, allowing direct overhead access to the medial and dorsal aspects of the foot. A thigh or calf tourniquet is applied over copious padding to provide a bloodless surgical field, which is essential for identifying the delicate neurovascular structures of the plantar forefoot. Regional anesthesia, specifically a popliteal sciatic nerve block supplemented with a saphenous nerve block, provides excellent intraoperative anesthesia and prolonged postoperative analgesia, significantly reducing the need for systemic opioids. Prophylactic intravenous antibiotics are administered 30 minutes prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
Meticulous surgical technique during sesamoidectomy is absolutely paramount to preserve the FHL tendon, protect the digital neurovascular bundles, and prevent devastating postoperative coronal plane deformities of the hallux. The approach varies significantly depending on whether the tibial or fibular sesamoid is being targeted.
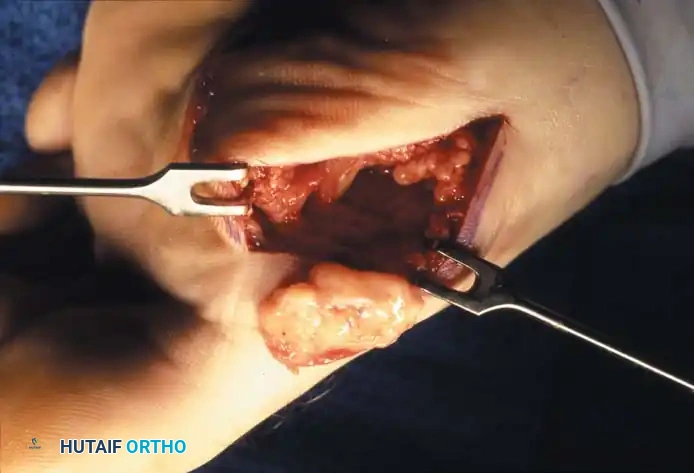
For excision of the tibial sesamoid, a medial approach is universally preferred. A 3-to-4-centimeter longitudinal incision is made along the medial aspect of the first MTP joint, precisely at the junction of the plantar and dorsal skin. This placement is critical to avoid the proper digital branch of the medial plantar nerve, which courses just plantar to the medial eminence and supplies sensation to the medial aspect of the hallux pulp. Dissection is carried down through the subcutaneous tissue, meticulously identifying and retracting any crossing superficial veins. The medial capsule of the MTP joint is identified, and a longitudinal capsulotomy is performed just plantar to the abductor hallucis tendon.
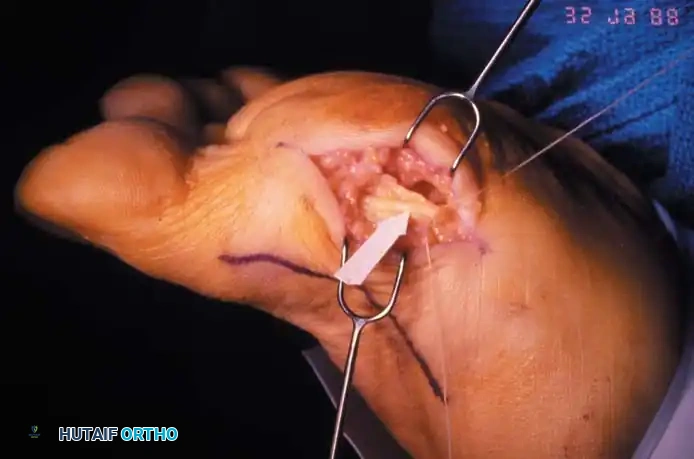

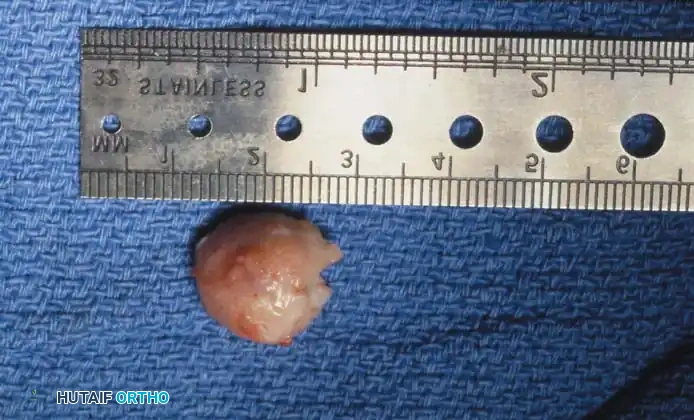
Once the capsule is breached, the tibial sesamoid is located via direct palpation. Using a #15 blade, the surgeon begins to carefully "shell" the sesamoid out of its investment within the medial head of the FHB and the plantar plate. This must be performed with the blade directed strictly toward the bone to avoid inadvertent soft tissue laceration. The most critical step of the procedure is the release of the lateral border of the tibial sesamoid. The FHL tendon lies immediately adjacent in the intersesamoid groove; iatrogenic laceration or partial transection of the FHL is a catastrophic complication. The hallux is kept slightly plantarflexed to relax the FHL, and a Freer elevator is utilized to protect the tendon while the intersesamoid ligament is sharply divided. Once enucleated, the remaining defect in the FHB and plantar plate must be meticulously repaired with heavy, non-absorbable figure-of-eight sutures to restore the medial stabilizing forces and prevent postoperative hallux valgus.
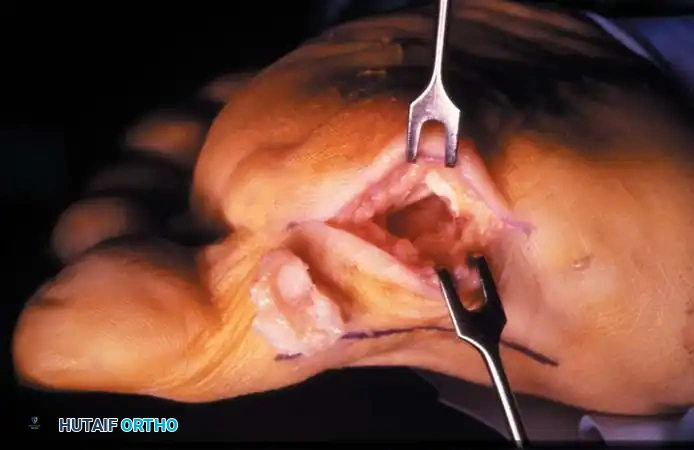
Excision of the fibular sesamoid is technically more demanding and can be approached via a plantar or dorsal incision. The plantar approach involves a longitudinal incision directly over the sesamoid; however, this places the lateral proper digital nerve at extreme risk and can result in a painful plantar scar. Therefore, a dorsal approach through the first web space is frequently advocated. A 3-centimeter dorsal longitudinal incision is made between the first and second metatarsal heads. Deep dissection identifies and retracts the adductor hallucis tendon. The deep transverse metatarsal ligament is identified and carefully preserved if possible, or sectioned and later repaired. The fibular sesamoid is visualized deep in the wound. Similar to the tibial procedure, the sesamoid is shelled out of the lateral FHB slip, with extreme caution taken medially to protect the FHL tendon.
Following excision of either sesamoid, thorough hemostasis is achieved after tourniquet deflation. The joint is copiously irrigated to remove any micro-particulate bone debris. The capsular repair is tested through a full range of motion to ensure no impingement or gaping occurs. The skin is closed with non-absorbable monofilament sutures using a vertical mattress technique to ensure optimal edge eversion and wound healing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical execution, sesamoidectomy carries a significant risk profile, and patients must be extensively counseled regarding potential postoperative complications. The complication rate reported in the literature varies widely but can approach 20% in highly active populations, frequently delaying or precluding a return to pre-injury levels of athletic performance.
The most profound and biomechanically devastating complications are iatrogenic coronal plane deformities of the hallux. Excision of the tibial sesamoid inherently weakens the medial stabilizing structures (medial FHB and abductor hallucis insertion), allowing the unopposed pull of the adductor hallucis and lateral FHB to drive the great toe into a progressive hallux valgus deformity. Conversely, excision of the fibular sesamoid disrupts the lateral stabilizing complex, frequently resulting in a rigid, recalcitrant hallux varus deformity. The incidence of clinically significant hallux valgus following tibial sesamoidectomy is reported to be approximately 10%, while hallux varus following fibular sesamoidectomy occurs in up to 15% of cases. Prevention relies entirely on meticulous, robust repair of the soft tissue defect created during enucleation.

Neurologic complications are also highly prevalent. The proper digital branches of the medial plantar nerve are intimately associated with the plantar-medial and plantar-lateral aspects of the sesamoid apparatus. Inadvertent traction, laceration, or postoperative entrapment within scar tissue can lead to severe, debilitating neuromas or permanent numbness of the hallux pulp. Patients presenting with sharp, shooting pain radiating into the toe postoperatively should be evaluated for neuroma formation, which may require subsequent surgical neurolysis or excision and proximal burial of the nerve stump into intrinsic musculature.
Arthrofibrosis and profound stiffness of the first MTP joint are nearly ubiquitous in the early postoperative period and can become permanent if aggressive rehabilitation is not instituted. Tethering of the FHL tendon within the surgical scar bed can severely limit active hallux plantarflexion.
Salvage management for failed sesamoidectomy or the catastrophic development of hallux malleus following inadvertent total sesamoidectomy is technically challenging. Soft tissue balancing procedures (e.g., EHL lengthening, capsular releases) are rarely sufficient in isolation. The definitive salvage procedure for a painful, deformed, and unstable first MTP joint following failed sesamoid surgery is a primary arthrodesis of the first MTP joint. While this sacrifices motion, it predictably restores a stable, plantigrade, and pain-free first ray, allowing for normal weight-bearing and ambulation.
| Complication | Estimated Incidence | Etiology/Mechanism | Salvage Management / Treatment |
|---|---|---|---|
| Hallux Valgus | 8% - 12% | Failure to repair medial FHB defect post-tibial sesamoidectomy | Soft tissue reconstruction; First MTP Arthrodesis if rigid/arthritic |
| Hallux Varus | 1 |
Clinical & Radiographic Imaging Archive



