Hallux Rigidus: Pathomechanics, Grading, and Surgical Management
Key Takeaway
Hallux rigidus is a progressive osteoarthritic condition of the first metatarsophalangeal (MTP) joint, characterized by pain and restricted dorsiflexion. Initial management includes stiff-soled shoes and activity modification. Operative interventions range from joint-preserving cheilectomy for early-stage disease to first MTP arthrodesis for advanced degeneration. Successful surgical outcomes depend on accurate radiographic grading, precise osteophyte resection, and restoration of pain-free first ray kinematics.
Comprehensive Introduction and Patho-Epidemiology
Hallux rigidus, a term originally coined by Cotterill in 1888 and further described as hallux flexus by Davies-Colley in 1887, refers to the progressive, symptomatic limitation of motion—specifically dorsiflexion—of the first metatarsophalangeal (MTP) joint due to degenerative osteoarthritis. As the most common arthritic condition of the foot and ankle, hallux rigidus frequently presents with debilitating pain, prominent dorsal osteophyte formation, and severely altered gait mechanics. Epidemiological data suggest that it affects approximately 1 in 40 adults over the age of 50, with a notable female predominance, although it can present in younger athletic populations due to repetitive microtrauma. The condition represents a significant source of morbidity, forcing patients to alter their kinetic chain, which often leads to secondary pathology in the knee, hip, and lumbar spine.
The etiology of hallux rigidus is unequivocally multifactorial, representing a complex interplay of genetic predisposition, biomechanical abnormalities, and environmental factors. It is strongly associated with hallux valgus interphalangeus, bilateral involvement in patients with a familial history, unilateral involvement in patients with a history of acute trauma, and variations in metatarsal morphology. Specific anatomical variants, such as a long first ray, a flattened or chevron-shaped MTP joint, and metatarsus primus elevatus, have been heavily scrutinized as predisposing factors. Furthermore, specific occupational hazards or athletic endeavors that demand repetitive forced dorsiflexion (e.g., turf toe injuries in football players or dancers) can dramatically accelerate joint degeneration through repetitive chondral sheer and impaction.


Understanding the pathomechanics of hallux rigidus is critical for selecting the appropriate surgical intervention. McMaster provided foundational insights into the microscopic and macroscopic progression of the disease. In his seminal evaluation of patients with hallux rigidus, the most common microscopic finding was a distinct cleavage lesion in the articular cartilage of the first metatarsal head, notably without any detached subchondral bone. This lesion is consistently located between the apex of the dome and the dorsal margin of the articular surface. Radiographically, the earliest sign of this pathology is a small, subtle depression in the dome of the metatarsal head. Because this finding is easily overlooked, high clinical suspicion and meticulous evaluation of weight-bearing orthogonal radiographs are required during early evaluation.
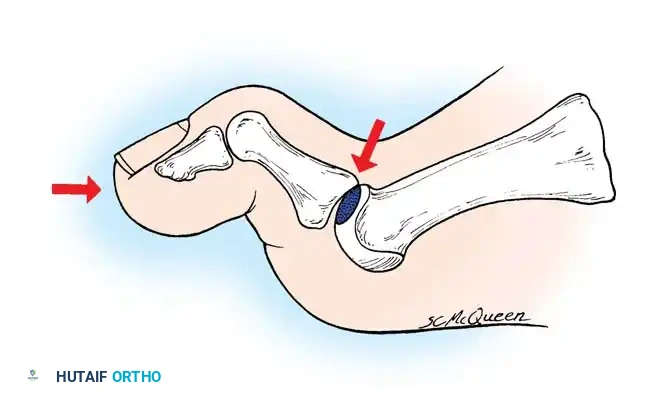
The kinematic cascade of impingement dictates the progressive nature of the disease. When the hallux is extended during the terminal stance phase of gait, the base of the proximal phalanx abuts against the cleavage lesion on the metatarsal head. This abutment produces sharp, focal pain, triggering an instinctive, protective flexion of the joint that actively limits extension. Over time, repetitive impingement leads to the formation of a proliferative dorsal osteophyte at the articular margin of the metatarsal head. This osteophyte creates a hard, mechanical block to extension. Consequently, the first metatarsal is often forced dorsally, decreasing its inclination angle on a weight-bearing lateral radiograph—a condition known as primus elevatus. It is generally accepted in contemporary orthopedic literature that the elevation of the first metatarsal is secondary to the arthritic changes and altered mechanics of the first MTP joint, rather than the primary causal factor of hallux rigidus.
Detailed Surgical Anatomy and Biomechanics
The first metatarsophalangeal joint is a highly complex ginglymoarthrodial articulation designed to withstand immense forces during the propulsive phase of gait. The osseous anatomy consists of the convex, cam-shaped head of the first metatarsal, the shallow concave base of the proximal phalanx, and the two plantar sesamoids (tibial and fibular) that articulate with the plantar aspect of the metatarsal head. The cam-shaped geometry of the metatarsal head is critical; it dictates a dual center of rotation. During the initial degrees of dorsiflexion, the proximal phalanx rolls on the metatarsal head. However, as dorsiflexion progresses beyond 20 to 30 degrees, the joint kinematics transition from rolling to a sliding motion. It is this sliding motion that is abruptly halted by the dorsal osteophyte in hallux rigidus, leading to mechanical impingement and pain.

The capsuloligamentous and musculotendinous structures surrounding the first MTP joint provide dynamic and static stability. The joint capsule is reinforced medially and laterally by the collateral ligaments and the suspensory sesamoid ligaments. Plantarly, the thick fibrocartilaginous plantar plate encapsulates the sesamoids and resists hyperextension. The intrinsic and extrinsic musculature—including the extensor hallucis longus (EHL), extensor hallucis brevis (EHB), flexor hallucis longus (FHL), flexor hallucis brevis (FHB), abductor hallucis, and adductor hallucis—work in concert to stabilize the ray. The sesamoids act as a fulcrum, increasing the mechanical advantage and moment arm of the FHB, which is essential for plantarflexion power during toe-off.
Biomechanically, the first MTP joint is the linchpin of the "windlass mechanism" described by Hicks. As the hallux dorsiflexes during the terminal stance phase of gait, the plantar fascia is wound tightly around the metatarsal head. This winding shortens the distance between the calcaneus and the metatarsal heads, elevating the medial longitudinal arch, locking the midtarsal joints, and converting the foot into a rigid lever for propulsion. Normal gait requires approximately 65 to 75 degrees of first MTP joint dorsiflexion. In hallux rigidus, the inability to achieve this necessary dorsiflexion disrupts the windlass mechanism. Patients compensate by externally rotating the lower extremity, rolling off the lateral border of the foot, or prematurely lifting the heel, which invariably leads to transfer metatarsalgia, lateral column overload, and proximal kinetic chain dysfunction.
Exhaustive Indications and Contraindications
Accurate grading of hallux rigidus dictates the treatment algorithm and is paramount for surgical decision-making. The Coughlin and Shurnas classification system remains the gold standard, comprehensively combining radiographic findings, clinical pain characteristics, and objective MTP joint motion. Conservative management—encompassing shoe modifications (stiff-soled shoes with a wide toe box), carbon fiber orthotic footplates, nonsteroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections—should always be exhausted before surgical intervention is considered, particularly for Grades 0 through 2.
When nonoperative modalities fail, surgical intervention is indicated. The choice of procedure is heavily dependent on the clinical grade, patient age, activity level, and the specific location of articular cartilage degradation. Cheilectomy is indicated for early-stage disease (Grades 1 and 2) where the primary pathology is dorsal impingement and the plantar and central articular cartilage remains viable. First MTP arthrodesis is the definitive procedure for end-stage disease (Grades 3 and 4), providing predictable pain relief and durable functional outcomes. Alternative procedures, such as interpositional arthroplasty or Moberg dorsal closing-wedge osteotomy of the proximal phalanx, may be considered in highly specific patient populations but lack the universal applicability and long-term survivorship of cheilectomy and arthrodesis.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Cheilectomy | Coughlin & Shurnas Grade 1 & 2; Pain isolated to extreme dorsiflexion; >50% viable cartilage on metatarsal head. | Grade 4 disease; Pain during midrange of motion; Active joint infection; Severe inflammatory arthropathy. | Grade 3 disease with diffuse cartilage loss; Severe metatarsus primus elevatus; Osteopenia. |
| First MTP Arthrodesis | Coughlin & Shurnas Grade 3 & 4; Rheumatoid arthritis; Failed previous MTP surgery (salvage); Severe pain throughout ROM. | Active local infection; Critical limb ischemia; Medical comorbidities precluding surgery. | Non-compliant patient; Heavy smoking (high nonunion risk); Severe adjacent IP joint arthritis (requires careful consideration). |
| Interposition Arthroplasty | Grade 3 disease in younger, active patients desiring motion preservation; Failed cheilectomy with adequate bone stock. | Inflammatory arthropathy; Severe bone loss; Grade 4 disease with sesamoid arthritis. | High-demand athletes; Obesity; Significant first ray hypermobility. |
| Moberg Osteotomy | Mild to moderate hallux rigidus with adequate MTP joint cartilage but insufficient dorsiflexion post-cheilectomy. | Severe degenerative joint disease (Grade 3/4); Pre-existing IP joint arthritis. | Short proximal phalanx; Inadequate bone stock for fixation. |

It is crucial to recognize that advanced arthritic changes on radiographs do not always correlate perfectly with clinical symptoms. Thompson and Mann emphasized that arthrodesis should be considered if loss of joint space is evident not only on anteroposterior and lateral views but also on the oblique view. The oblique radiograph frequently reveals remaining viable joint space that is obscured on standard orthogonal views. Furthermore, cheilectomy is strictly contraindicated if the patient experiences pain throughout the midrange of passive motion, as this indicates global joint degeneration rather than isolated dorsal impingement.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with a meticulous clinical examination. The surgeon must assess the active and passive range of motion of the first MTP joint, noting the exact arc of motion where pain is elicited. A positive "grind test"—pain elicited by axial compression and rotation of the proximal phalanx against the metatarsal head—is pathognomonic for advanced, global articular degeneration and strongly points toward arthrodesis rather than joint-preserving surgery. The interphalangeal (IP) joint must also be evaluated; pre-existing IP joint arthritis is a critical consideration before performing a first MTP arthrodesis, as the fused MTP joint will transfer increased biomechanical stress to the IP joint, potentially exacerbating symptoms.
Radiographic evaluation must include standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. The AP view is scrutinized for joint space narrowing, subchondral sclerosis, cystic changes, and the presence of medial or lateral osteophytes. The lateral view is essential for assessing the size of the dorsal osteophyte, the presence of loose bodies, and the degree of metatarsus primus elevatus. The oblique view is critical for evaluating the true extent of joint space preservation. Additionally, a sesamoid axial view should be obtained to rule out concurrent sesamoid arthritis, which, if present and symptomatic, may necessitate sesamoidectomy or strongly favor arthrodesis over cheilectomy.

For patients undergoing first MTP arthrodesis, pre-operative templating is vital to determine the optimal position of fusion. The universally accepted optimal position for fusion is 10 to 15 degrees of valgus, 15 to 20 degrees of dorsiflexion relative to the first metatarsal (or neutral to slight dorsiflexion relative to the floor), and neutral rotation. Templating helps anticipate the necessary bone resection and the appropriate hardware construct.
In the operating room, the patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the foot rests in a neutral, plantigrade position. This is particularly critical during arthrodesis to accurately judge the rotational and sagittal alignment of the hallux. A thigh or calf tourniquet is applied for hemostasis, and the foot is prepped and draped in a standard sterile fashion. Fluoroscopy must be readily available and positioned to allow for effortless AP, lateral, and oblique intraoperative imaging without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Cheilectomy: Joint-Preserving Osteophyte Resection
The primary surgical goal of a cheilectomy is to meticulously resect the proliferative dorsal osteophyte, medial and lateral bony excrescences, and a portion of the dorsal articular cartilage to eliminate the mechanical buttress preventing dorsiflexion, thereby restoring a minimum of 70 degrees of intraoperative impingement-free motion.

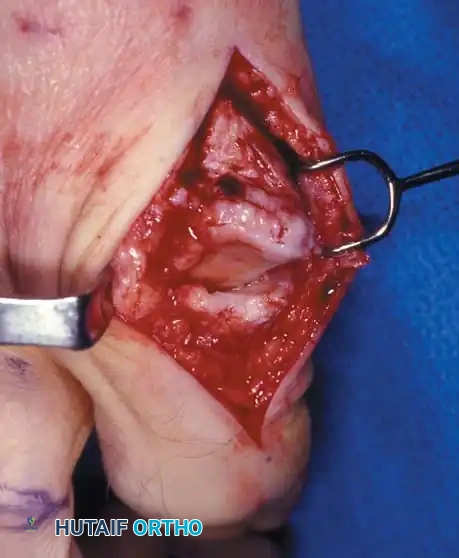
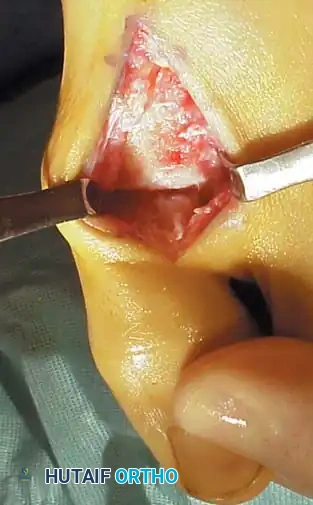
Step 1: Approach and Exposure
A dorsal longitudinal skin incision is made, beginning approximately 1 cm proximal to the interphalangeal joint and extending proximally about 5 cm across the MTP joint. The incision is placed just medial or lateral to the extensor hallucis longus (EHL) tendon. Meticulous blunt dissection through the subcutaneous tissue is essential to identify and carefully retract the dorsomedial cutaneous nerve to prevent painful postoperative neuromas, a complication that can severely compromise patient satisfaction. The EHL tendon is retracted laterally, and a longitudinal capsulotomy is performed to expose the joint.

Step 2: Joint Debridement and Osteophyte Resection
The capsule is elevated via sharp dissection off the metatarsal head and the base of the proximal phalanx, ensuring full exposure of the dorsal, medial, and lateral gutters. A prominent dorsolateral osteophyte is frequently present and must be completely excised. Using an oscillating saw or a sharp, broad osteotome, approximately 20% to 30% of the dorsal aspect of the metatarsal head is resected. The cut should begin dorsally and exit just proximal to the dorsal articular margin, angling slightly plantarward to ensure a smooth transition. The "rule of thirds" is often applied: if the dorsal third of the cartilage is severely eroded, it is resected along with the osteophyte.

Step 3: Dynamic Assessment and Closure
Following resection, the joint is distracted, and a rongeur or curette is used to meticulously remove any loose cartilage, bone debris, or osteochondral fragments from the joint space and the sesamoid articulation. The joint is then aggressively irrigated. The surgeon must passively move the joint through its range of motion, forcefully dorsiflexing the proximal phalanx. It is absolutely critical to achieve 60 to 70 degrees of impingement-free dorsiflexion intraoperatively. If impingement persists, additional dorsal bone must be resected. Bone wax may be applied to the raw cancellous bone surface to reduce postoperative hematoma and stiffness. The capsule is closed with absorbable sutures, followed by standard skin closure.


First MTP Arthrodesis: The Gold Standard for Advanced Disease
For patients with Grade 4 hallux rigidus, or Grade 3 with extensive global cartilage loss, arthrodesis of the first MTP joint provides the most reliable, long-term pain relief and functional restoration. Modern fixation techniques have revolutionized fusion rates, achieving successful arthrodesis in 94% to 98% of cases.
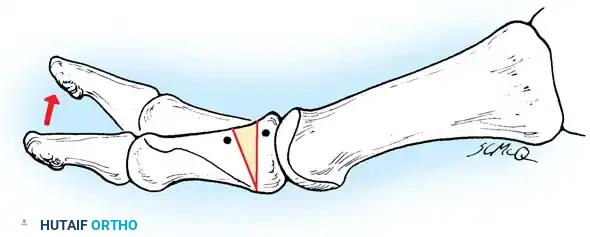
Step 1: Joint Preparation
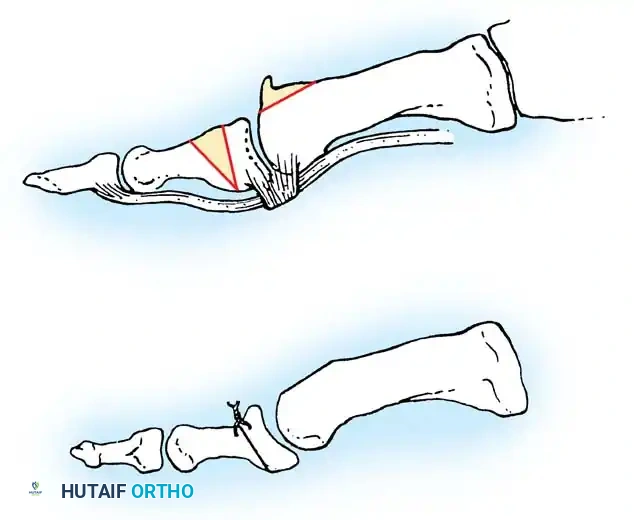
The approach is identical to the cheilectomy. Once the joint is exposed, the remaining articular cartilage and subchondral bone must be completely removed to expose healthy, bleeding cancellous bone. The McKeever technique utilizes specialized conical reamers. The metatarsal head is shaped into a convex cone, and the base of the proximal phalanx is reamed into a matching concave cup. This ball-and-socket preparation is highly advantageous as it allows for multi-planar adjustment of the toe before final fixation and preserves the functional length of the first ray. Alternatively, flat cuts using an oscillating saw can be utilized; while technically simpler, this method shortens the first ray and is less forgiving regarding multi-planar alignment.
Step 2: Alignment and Provisional Fixation
Positioning the fusion is the most critical step of the operation. The hallux must be positioned in 10 to 15 degrees of valgus (to parallel the lesser toes and fit comfortably in footwear), 15 to 20 degrees of dorsiflexion relative to the longitudinal axis of the first metatarsal, and neutral rotation (the toenail should face directly dorsal). Excessive dorsiflexion leads to dorsal toe impingement in shoes, while inadequate dorsiflexion leads to a vaulting gait and rapid degeneration of the IP joint. Once the optimal position is achieved, it is provisionally fixed with Kirschner wires. A sterile flat plate (or the lid of a surgical tray) is often pressed against the plantar aspect of the foot to simulate weight-bearing and confirm the hallux rests appropriately just off the ground.
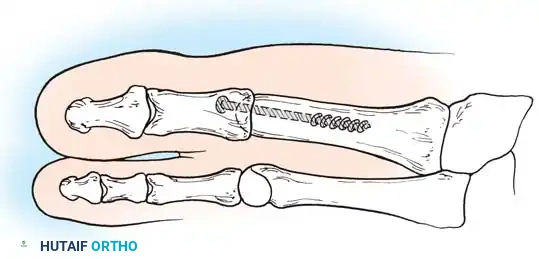
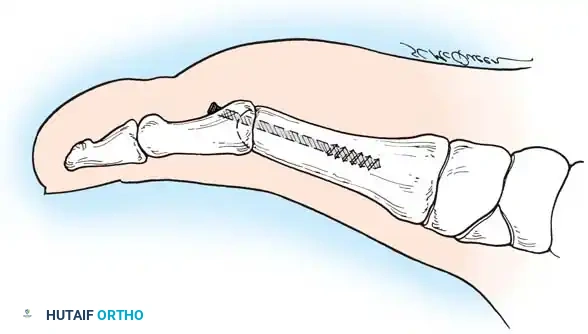
Step 3: Definitive Fixation Construct
Politi et al. conducted a comprehensive biomechanical study demonstrating that the most stable fixation construct is a combination of an interfragmentary oblique lag screw and a dorsal neutralization plate. A 3.5mm or 4.0mm solid or cannulated lag screw is introduced from the medial aspect of the proximal phalanx, directed proximally and laterally into the metatarsal head, compressing the joint surfaces. A low-profile, anatomically contoured dorsal titanium plate is then applied and secured with locking and non-locking screws. This rigid construct resists plantar gapping during the propulsive phase of gait, drastically reducing the risk of nonunion. Intraoperative fluoroscopy is utilized to confirm hardware placement, joint compression, and overall alignment.
Complications, Incidence Rates, and Salvage Management
Despite high success rates, surgical management of hallux rigidus is not without complications. The surgeon must be acutely aware of potential pitfalls, their incidence, and appropriate salvage strategies. Thorough pre-operative patient counseling regarding these risks is mandatory.
| Complication | Incidence Rate | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Nonunion (Arthrodesis) | 5% - 10% | Smoking, non-compliance with NWB, inadequate fixation, poor bone preparation, infection. | Asymptomatic: Observation. Symptomatic: Revision arthrodesis with structural bone grafting (iliac crest) and robust revision hardware. |
| Malunion (Arthrodesis) | 5% - 8% | Intraoperative technical error (excessive dorsiflexion, excessive plantarflexion, malrotation). | Corrective closing or opening wedge osteotomy through the fusion mass; hardware revision. |
| Hardware Prominence | 10% - 15% | Thin dorsal soft tissue envelope; use of bulky dorsal plates. | Hardware removal after radiographic and clinical confirmation of solid bony union (typically >6 months post-op). |
| Progression of Disease (Cheilectomy) | 10% - 20% (Long-term) | Under-resection of osteophyte; pre-existing advanced (Grade 3) disease; natural progression of OA. | Conversion to First MTP Arthrodesis or Interpositional Arthroplasty. |
| Nerve Injury / Neuroma | 2% - 5% | Iatrogenic injury to the dorsomedial cutaneous nerve during exposure or closure. | Conservative: Gabapentin, targeted steroid injections. Surgical: Neuroma excision and proximal nerve burying into muscle or bone. |
| Transfer Metatarsalgia | 3% - 7% | Shortening of the first ray (flat cut arthrodesis); excessive elevation of the first metatarsal. | Custom orthotics with metatarsal pads; rarely, lesser metatarsal shortening osteotomies (Weil osteotomy). |
Malunion remains one of the most frustrating complications following first MTP arthrodesis. If the toe is fused in excessive plantarflexion, the patient will experience severe vaulting during gait, excessive pressure on the distal tip of the toe, and rapid, painful arthritic degeneration of the interphalangeal joint. Conversely, if fused in excessive dorsiflexion, the hallux will rub against the toe box of standard footwear, causing painful hyperkeratotic lesions and dorsal ulcerations. Salvage of a symptomatic malunion requires a technically demanding corrective osteotomy through the fusion mass, realigning the ray, and applying revision fixation.
Progression of disease following a cheilectomy is an expected long-term outcome in a subset of patients, as the procedure does not halt the underlying osteoarthritic process. However, a well-executed cheilectomy does not "burn any bridges." If a patient develops recurrent, debilitating pain years after a cheilectomy due to progressive joint space narrowing, the salvage procedure is a straightforward conversion to a first MTP arthrodesis. The prior removal of the dorsal osteophyte does not significantly compromise the bone stock required for a subsequent fusion.

Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be strictly tailored to the specific surgical procedure performed. The goals of cheilectomy rehabilitation are early, aggressive mobilization to prevent capsular scarring and preserve the surgically gained range of motion. Conversely, the goal of arthrodesis rehabilitation is strict immobilization to facilitate rigid bony union.
**
