First MTP Arthroscopy and Hindfoot Endoscopy: A Master Surgical Guide
Key Takeaway
First metatarsophalangeal (MTP) joint arthroscopy and hindfoot endoscopy are advanced, minimally invasive techniques for treating forefoot and hindfoot pathology. This comprehensive guide details the precise surgical steps, portal placements, and biomechanical considerations for first MTP arthroscopy, peroneal and posterior tibial tendoscopy, and endoscopic calcaneoplasty. Utilizing specialized distraction and small-joint instrumentation allows orthopedic surgeons to achieve excellent clinical outcomes while minimizing soft tissue morbidity.
Comprehensive Introduction and Patho-Epidemiology
The evolution of minimally invasive techniques in foot and ankle surgery has fundamentally transformed the management of both forefoot and hindfoot pathology. Historically, surgical intervention for conditions such as hallux rigidus, peroneal tendon subluxation, and Haglund syndrome required extensive open exposures. These traditional open approaches often necessitated large incisions through tenuous soft tissue envelopes, leading to significant soft tissue morbidity, prolonged rehabilitation, high risks of wound dehiscence, and painful scar neuroma formation. The advent of small joint arthroscopy and endoscopy represents a paradigm shift, prioritizing the preservation of the soft tissue envelope while achieving equivalent or superior intra-articular and extra-articular surgical objectives.
Today, first metatarsophalangeal (MTP) joint arthroscopy, tendoscopy, and endoscopic calcaneoplasty represent the absolute pinnacle of modern operative orthopaedics. Supported by extensive literature—including the foundational and pioneering work by Niek van Dijk, Richard Ferkel, and Tun Hing Lui—these techniques offer brilliant, magnified direct visualization of intra-articular and extra-articular structures. This allows for precise, targeted débridement, synovectomy, and osteophyte resection without the collateral damage associated with arthrotomies. This masterclass provides a rigorous, step-by-step academic guide to these procedures, tailored specifically for the practicing consultant, orthopedic fellow, and advanced resident seeking to refine their minimally invasive armamentarium.
The patho-epidemiology of first MTP joint and hindfoot disorders underscores the necessity for these advanced techniques. Hallux rigidus, the most common osteoarthritic condition of the foot, affects approximately 1 in 45 individuals over the age of 50. It is characterized by progressive degeneration of the articular cartilage, accompanied by dorsal osteophytic proliferation that mechanically blocks terminal dorsiflexion. The pathophysiology is largely driven by repetitive microtrauma and altered biomechanics, particularly in patients with an elevated first ray or hypermobile first tarsometatarsal joint. In the athletic population, acute osteochondral defects (OCDs) of the first metatarsal head are increasingly recognized as primary pain generators, necessitating early arthroscopic intervention to prevent rapid progression to end-stage degenerative joint disease.
Similarly, the patho-epidemiology of the hindfoot is dominated by conditions exacerbated by modern footwear and high-impact athletics. Insertional Achilles tendinopathy, retrocalcaneal bursitis, and Haglund’s deformity constitute a triad of posterior heel pain that plagues both elite runners and sedentary individuals alike. The mechanical impingement of the posterosuperior calcaneal tuberosity against the anterior aspect of the Achilles tendon during ankle dorsiflexion leads to chronic inflammation, bursal hypertrophy, and eventual intrasubstance tendinosis. Endoscopic management addresses the mechanical root cause—the bony exostosis—while simultaneously clearing the hypertrophic bursa, halting the pathological cascade and facilitating rapid functional recovery.
Detailed Surgical Anatomy and Biomechanics
First Metatarsophalangeal Joint Anatomy
The first MTP joint is a highly complex, dual-articulation structure comprising the metatarsophalangeal joint proper and the inferior metatarsosesamoid articulation. The joint capsule is inherently tight, reinforced medially and laterally by robust collateral ligaments, and plantarly by the thick plantar plate and sesamoid complex. The vascular supply is derived primarily from the first dorsal metatarsal artery and the first plantar metatarsal artery, forming a rich anastomotic ring around the metatarsal neck. Neurologically, the joint is innervated by branches of the deep peroneal nerve, the medial dorsal cutaneous nerve, and the medial and lateral plantar nerves. The surgeon must possess an intimate understanding of the dorsal neurovascular anatomy, specifically the arborization of the medial dorsal cutaneous nerve, which courses precariously close to the standard dorsomedial arthroscopy portal.
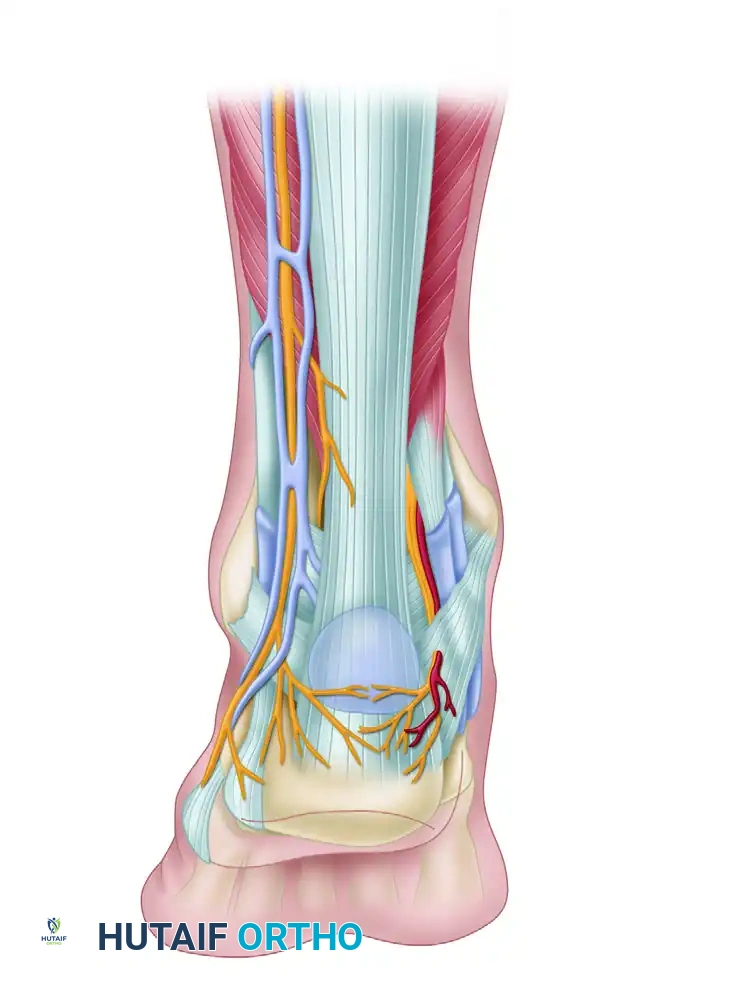
Hindfoot and Retrocalcaneal Anatomy
The posterior ankle and hindfoot present a challenging anatomical landscape for the endoscopic surgeon. The retrocalcaneal space is a distinct anatomical compartment bordered anteriorly by the posterior surface of the calcaneal tuberosity, posteriorly by the anterior epitenon of the Achilles tendon, and superiorly by the deep crural fascia (Kager's fat pad). The retrocalcaneal bursa is a horseshoe-shaped structure draped over the posterosuperior calcaneal prominence. The neurovascular structures in this region are unforgiving. The sural nerve and lesser saphenous vein course along the posterolateral aspect of the ankle, often crossing the lateral border of the Achilles tendon near the insertion. Medially, the tibial nerve and posterior tibial artery reside behind the medial malleolus, giving off the medial calcaneal nerve branches that supply the heel pad.
Biomechanics of the First Ray and Hindfoot
Biomechanically, the first MTP joint is subjected to immense forces during the terminal stance and pre-swing phases of the gait cycle. Through the windlass mechanism, dorsiflexion of the hallux tightens the plantar fascia, elevating the medial longitudinal arch and locking the midtarsal joints to create a rigid lever for propulsion. During this phase, the first MTP joint bears up to 119% of total body weight. Any restriction in dorsiflexion—whether due to dorsal osteophytes (hallux rigidus) or capsular contracture—disrupts this mechanism, leading to compensatory lateral column overload and altered proximal kinematics.
In the hindfoot, the Achilles-calcaneal-plantar fascia continuum acts as a vital energy storage and release mechanism. The insertion of the Achilles tendon is not a simple focal attachment; it is a broad, complex enthesis that dissipates stress across the posterior calcaneus. When a Haglund's deformity is present, the mechanical axis of the Achilles tendon is displaced posteriorly, increasing the lever arm but simultaneously creating a fulcrum of impingement against the anterior tendon fibers during maximum dorsiflexion. Endoscopic calcaneoplasty aims to restore the normal biomechanical glide of the tendon by eliminating this pathological bony fulcrum.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful small joint arthroscopy and endoscopy. The decision to proceed with minimally invasive surgery versus traditional open procedures, or joint-sacrificing operations (such as arthrodesis), hinges upon a meticulous clinical examination, advanced imaging, and a thorough understanding of the patient's functional demands. The primary philosophy underlying these techniques is joint and tissue preservation; therefore, they are most efficacious in the early to moderate stages of disease.
For the first MTP joint, arthroscopy is highly indicated for Coughlin and Shurnas Grade I and Grade II hallux rigidus, where the primary pain generator is dorsal impingement rather than global articular cartilage loss. It is also the gold standard for the evaluation and treatment of osteochondral defects (OCDs) of the metatarsal head, allowing for precise microfracture or retrograde drilling. Furthermore, in cases of chronic, unexplained first MTP joint pain following inconclusive MRI or CT imaging, diagnostic arthroscopy serves as a definitive diagnostic and therapeutic tool. Inflammatory arthropathies, such as rheumatoid arthritis or gouty arthropathy, also benefit significantly from arthroscopic synovectomy and the removal of crystalline deposits or loose bodies.
In the hindfoot, endoscopic calcaneoplasty is indicated for patients with symptomatic Haglund’s syndrome, retrocalcaneal bursitis, and non-insertional Achilles tendinopathy who have failed a rigorous 3-to-6-month course of conservative management (including eccentric stretching, orthotics, and shockwave therapy). Tendoscopy is indicated for chronic tenosynovitis of the peroneal or posterior tibial tendons, low-grade partial longitudinal split tears, and the evaluation of retinacular incompetence.
Absolute contraindications for small joint arthroscopy include active localized or systemic infection, severe peripheral vascular disease precluding safe tourniquet use or wound healing, and advanced Charcot neuroarthropathy with profound architectural collapse. Relative contraindications include end-stage degenerative joint disease (Coughlin and Shurnas Grade III/IV hallux rigidus), where the joint space is obliterated, making safe portal placement and instrument insertion nearly impossible without causing severe iatrogenic chondral damage.
| Procedure Category | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| First MTP Arthroscopy | Grade I/II Hallux Rigidus, OCDs, Synovitis, Loose Bodies, Unexplained Pain | Active Joint Infection, Charcot Arthropathy, Severe Ischemia | Grade III/IV Hallux Rigidus, Prior Arthrodesis, Severe Hallux Valgus |
| Hindfoot Endoscopy | Haglund's Deformity, Retrocalcaneal Bursitis, Posterior Impingement | Local Soft Tissue Infection, Achilles Rupture (Complete) | Extensive Intrasubstance Achilles Calcification, Severe Obesity |
| Tendoscopy | Chronic Tenosynovitis, Partial Split Tears, Retinacular Evaluation | Acute Tendon Rupture, Overlying Cellulitis | Severe Tendon Degeneration requiring reconstruction/transfer |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is critical to the success of minimally invasive foot and ankle surgery. The surgeon must obtain standard weight-bearing radiographs (anteroposterior, lateral, and sesamoid views for the MTP; lateral and axial calcaneal views for the hindfoot). Advanced imaging, particularly MRI without contrast, is highly recommended to assess the integrity of the articular cartilage, the extent of bone marrow edema, and the presence of intrasubstance tendinosis. For Haglund's deformity, a pre-operative lateral radiograph is used to template the Fowler-Philip angle and the parallel pitch lines, quantifying the volume of bone requiring resection.
Patient positioning and operating room setup must be executed with absolute precision. For first MTP joint arthroscopy, the patient is positioned supine on the operating table. A thigh or calf tourniquet is applied and inflated to 250 mmHg to ensure a pristine, bloodless field, which is mandatory given the diminutive size of the joint space. The limb is secured, and a sterile Chinese finger trap is applied to the hallux. The foot is then suspended from a specialized distraction tower (often identical to those utilized in wrist arthroscopy). Approximately 10 to 15 pounds of continuous longitudinal traction is applied. This non-negotiable step opens the tight joint space, preventing iatrogenic scuffing of the articular cartilage during the insertion of the arthroscope and rigid instruments.
For hindfoot endoscopy and calcaneoplasty, the patient is placed in the prone position. The patient is shifted distally so that the foot and ankle hang completely free over the edge of the operating table. This positioning allows the surgeon to perform dynamic intraoperative assessments, freely dorsiflexing and plantarflexing the ankle to evaluate for residual impingement during the bone resection phase. A thigh tourniquet is utilized. The contralateral leg must be heavily padded to prevent pressure neuropathies.
Equipment selection is equally vital. The surgeon should have a 1.9-mm or 2.7-mm, 30-degree short arthroscope available for the first MTP joint, alongside a 2.0-mm or 2.9-mm aggressive shaver and a small arthroscopic burr. For the hindfoot, a standard 4.0-mm, 30-degree arthroscope is preferred, providing a wider field of view and superior illumination. A high-flow fluid management system is utilized, though pump pressures must be carefully monitored (typically kept between 30-40 mmHg) to prevent massive fluid extravasation and potential compartment syndrome of the foot or lower leg.
Step-by-Step Surgical Approach and Fixation Technique
First MTP Arthroscopy Technique
The standard approach utilizes two primary dorsal portals. Prior to portal placement, the joint is insufflated with 2 to 3 mL of normal saline using a 21-gauge needle to distend the capsule. The extensor hallucis longus (EHL) tendon serves as the central anatomical landmark. The dorsomedial portal is established just medial to the EHL tendon at the level of the joint line, while the dorsolateral portal is established just lateral to the EHL. The surgeon must strictly employ a "nick and spread" technique: incising only the epidermis with a #11 blade, followed by blunt dissection with a small mosquito hemostat down to the joint capsule to protect the medial dorsal cutaneous nerve and the terminal branches of the deep peroneal nerve.
Once the portals are established, a diagnostic sweep is performed using a systematic 8-point examination: evaluating the dorsal capsule, medial gutter, lateral gutter, central metatarsal head, proximal phalanx base, and the complex plantar metatarsosesamoid articulations. For hallux rigidus, a cheilectomy is performed by introducing a 2.9-mm arthroscopic burr through the dorsolateral portal. The dorsal osteophyte is systematically resected from medial to lateral until a smooth, anatomical contour is restored. If an osteochondral defect is identified, the lesion is débrided to stable, vertical margins using an arthroscopic curette. Microfracture is then performed using a specialized awl to penetrate the subchondral bone, releasing mesenchymal stem cells to stimulate fibrocartilage formation. In rare cases of massive osteochondral shearing, bioabsorbable pin fixation may be performed percutaneously under arthroscopic guidance.
Hindfoot Endoscopy and Calcaneoplasty
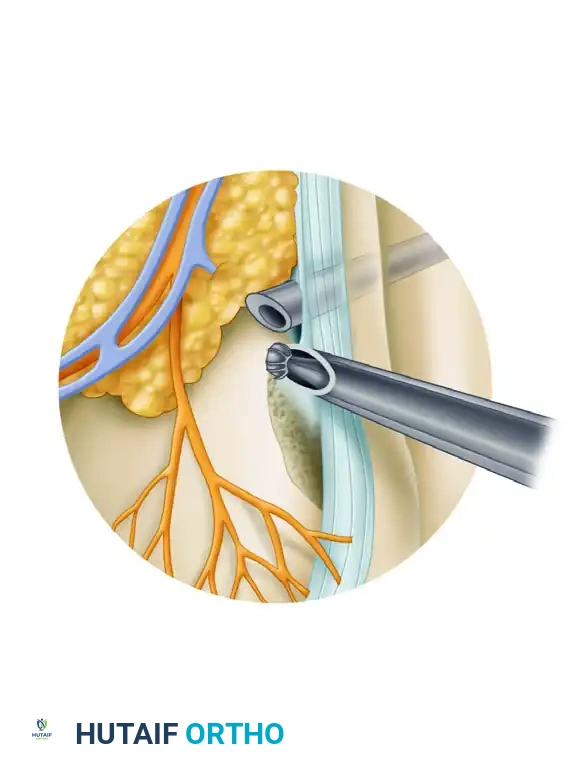
The endoscopic calcaneoplasty utilizes a standard two-portal technique. The lateral portal is placed just lateral to the Achilles tendon at the level of the superior aspect of the calcaneal tuberosity, taking extreme care to avoid the sural nerve. The medial portal is established at the exact same horizontal level, just medial to the Achilles tendon. Placing these portals too anteriorly drastically increases the risk of neurovascular injury.
A 4.0-mm arthroscope is introduced laterally, and a 4.0-mm shaver is introduced medially. The initial view is invariably obscured by dense, hypertrophic bursal tissue. A meticulous bursectomy is performed to clear the retrocalcaneal space, exposing the anterior epitenon of the Achilles tendon and the posterior calcaneal exostosis. Once the bone spur is visualized, the shaver is exchanged for a 4.0-mm or 5.5-mm hooded arthroscopic burr.
The bone resection must be systematic and aggressive. The posterosuperior prominence of the calcaneus is resected, sweeping the burr from medial to lateral. The surgeon must dynamically dorsiflex the ankle fully while viewing the space to ensure no residual impingement exists between the calcaneus and the anterior Achilles tendon. Intraoperative lateral fluoroscopy is mandatory to confirm that the Fowler-Philip angle has been adequately reduced and the Haglund's lesion completely eradicated. If the Achilles tendon is found to be significantly avulsed or damaged during the debridement, endoscopic knotless suture anchor fixation can be utilized to reapproximate the anterior footprint of the tendon to the calcaneus.
Tendoscopy and Retinacular Fixation
For peroneal tendoscopy, portals are established along the course of the tendon sheath, 1-2 cm distal to the fibular tip and 2-3 cm proximal to the lateral malleolus. A thorough tenosynovectomy is performed. In cases of peroneal subluxation, the retromalleolar groove is evaluated. Endoscopic groove deepening is achieved by burring the fibular sulcus while carefully preserving the overlying fibrocartilaginous floor. If the superior peroneal retinaculum is incompetent, it can be plicated using thermal shrinkage or repaired back to the fibula using percutaneous all-suture anchors deployed under direct endoscopic visualization, providing robust fixation without an open incision.
Complications, Incidence Rates, and Salvage Management
While minimally invasive, small joint arthroscopy and endoscopy are technically demanding procedures that carry specific, potentially devastating risks. The orthopedic surgeon must meticulously mitigate these risks through rigorous anatomical knowledge and precise surgical technique. The overall complication rate for foot and ankle arthroscopy ranges from 4% to 9%, which is significantly lower than open equivalents, yet demands profound respect.
Nerve injury is the most common complication. In first MTP arthroscopy, the medial dorsal cutaneous nerve is highly vulnerable at the dorsomedial portal. In hindfoot endoscopy, the sural nerve is at extreme risk during lateral portal placement and lateral burring. Neurological injuries typically present as transient neurapraxias resolving over 3 to 6 months, but complete transections resulting in painful neuromas require subsequent microsurgical excision and nerve capping.
Iatrogenic tendon and articular damage is a catastrophic technical error. Aggressive, uncontrolled use of the motorized shaver or burr in the tight confines of the retrocalcaneal space can result in partial or complete laceration of the Achilles tendon. The shaver blade must always face away from the tendon substance. Similarly, in the first MTP joint, failure to apply adequate traction will result in the arthroscope gouging the fragile articular cartilage.
Inadequate resection is a frequent cause of surgical failure, particularly in endoscopic calcaneoplasty. Failure to resect the medial or lateral borders of the calcaneal spur, or failing to remove enough bone superiorly, leads to persistent mechanical impingement and ongoing pain. This necessitates a revision endoscopic or open procedure. Intraoperative fluoroscopy is the ultimate safeguard against this complication.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Iatrogenic Nerve Injury (Sural / Dorsal Cutaneous) | 2.5% - 5.0% | Strict "nick and spread" technique; avoid anterior portal drift. | Observation for neurapraxia; Gabapentinoids; Open neuroma excision if persistent. |
| Inadequate Bone Resection / Recurrence | 3.0% - 6.0% | Mandatory dynamic intraoperative assessment and lateral fluoroscopy. | Revision endoscopic calcaneoplasty or open Haglund's resection. |
| Iatrogenic Tendon Laceration (Achilles/Peroneal) | < 1.0% | Keep shaver/burr hood facing bone; direct visualization at all times. | Immediate open primary repair; possible augmentation with FHL transfer if severe. |
| Portal Site Infection / Necrosis | 1.0% - 2.0% | Avoid excessive tourniquet time; low pump pressures to prevent fluid extravasation. | Oral/IV antibiotics; local wound care; rarely requires surgical debridement. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management following small joint arthroscopy and endoscopy is generally accelerated compared to traditional open procedures. The preservation of the soft tissue envelope allows for earlier mobilization, which is critical for preventing capsular adhesions and optimizing functional outcomes. However, the rehabilitation protocol must be meticulously tailored to the specific pathology treated and the structural integrity of the tissues post-débridement.
Phase I: Immediate Post-Operative Phase (Weeks 0-2)
For first MTP arthroscopy, the patient is placed in a rigid-soled postoperative shoe immediately following surgery. Heel-weight-bearing is permitted as tolerated to facilitate independent ambulation while protecting the forefoot. Cryotherapy and elevation are highly encouraged to mitigate hemarthrosis. For hindfoot endoscopy, the patient is placed in a controlled ankle motion (CAM) boot equipped with a 1.5 cm to 2.0 cm heel wedge. This wedge is critical as it plantarflexes the ankle, decreasing the mechanical tension on the Achilles tendon insertion, which may have been structurally weakened by the adjacent mechanical débridement of the Haglund's lesion. Weight-bearing as tolerated in the boot is generally permitted.
Phase II: Intermediate Rehabilitation and Mobilization (Weeks 2-6)
Sutures are removed at the 2-week mark. For the first MTP joint, this phase is characterized by aggressive physical therapy. Passive and active range of motion (ROM) exercises of the hallux are initiated immediately. Manual capsular stretching, particularly focusing on terminal dorsiflexion, is vital to prevent the recurrence of stiffness (arthrofibrosis). Patients transition to normal, stiff-soled footwear by week 4.
For the hindfoot, the heel wedge in the CAM boot is gradually reduced by one layer every 5 to 7 days until the foot is plantigrade. Physical therapy is initiated, focusing heavily on isometric strengthening and transitioning to eccentric Achilles stretching protocols. Cross-friction massage of the portal sites is performed to prevent scar tissue tethering to the underlying tendon.
Phase III: Advanced Strengthening and Return to Play (Weeks 6-12+)
By week 6, patients who underwent first MTP arthroscopy are generally cleared to resume linear running and low-impact activities, provided there is no pain with terminal dorsiflexion. Return to high-impact, multidirectional sports (e.g., soccer, basketball) is typically achieved by 8 weeks.
For endoscopic calcaneoplasty patients, the rehabilitation is slightly more protracted due to the load-bearing demands of the Achilles tendon. Running and high-impact activities are strictly restricted until 8 to 10 weeks postoperatively. The final phase of therapy focuses on plyometrics, single-leg heel raises, and sport-specific drills. Full, unrestricted return to elite athletic competition may take up to 4 to 6 months, ensuring the tendon insertion has completely remodeled and recovered its ultimate tensile strength.
Summary of Landmark Literature and Clinical Guidelines
The integration of small joint arthroscopy and endoscopy into mainstream orthopedic practice is heavily supported by a robust body of evidence-based medicine. The seminal literature has consistently demonstrated that these minimally invasive techniques offer equivalent or superior clinical outcomes compared to open surgery, with drastically reduced complication profiles.
Niek van Dijk’s foundational papers in the late 1990s and early 2000s revolutionized the approach to the posterior ankle. His anatomical studies defining the two-portal endoscopic technique for the retrocalcaneal space remain the gold standard. Long-term outcome studies from van Dijk's cohort demonstrated good to excellent results in over 90% of patients undergoing endoscopic calcaneoplasty, with return-to-sport times halved compared to open osteotomy cohorts.
In the realm of forefoot surgery, Tun Hing Lui and Richard Ferkel have published extensively on the indications and outcomes of first MTP joint arthroscopy. Ferkel’s outcome data on arthroscopic cheilectomy for Grade I and II hallux rigidus revealed a 92% patient satisfaction rate at 5-year follow-up, with significant improvements in AOFAS (American Orthopaedic Foot and Ankle Society) forefoot scores and a negligible incidence of wound complications. Lui’s technical monographs on portal safety and the management of osteochondral defects have become mandatory reading for orthopedic trainees.
Current clinical guidelines from the AAOS and AOFAS strongly support the use of diagnostic and therapeutic arthroscopy for early-stage hallux rigidus and symptomatic Haglund's syndrome that has failed conservative management. Looking to the future, the integration of ultra-minimally invasive "needle arthroscopy" (utilizing 1.0-mm optics in the office setting) and the concurrent use of orthobiologics (such as Platelet-Rich Plasma and Bone Marrow Aspirate Concentrate) during arthroscopic microfracture are poised to further expand the frontiers of joint preservation. As instrumentation continues to miniaturize and optical fidelity improves, the indications for these masterful techniques will undoubtedly broaden, cementing their status as the absolute standard of care for complex foot and ankle pathology.
