Masterclass: Surgical Repair of Turf Toe Injuries – An Intraoperative Guide

Key Takeaway
This masterclass guides fellows through the surgical repair of turf toe, focusing on hallux MP joint stabilization. We cover detailed anatomy, meticulous preoperative planning, and real-time intraoperative execution. Learn precise dissection, plantar plate repair, and neurovascular protection. Extensive pearls, pitfalls, and postoperative management strategies ensure optimal patient outcomes for these disabling injuries.
Comprehensive Introduction and Patho-Epidemiology
Good morning, colleagues and fellows. Welcome to the operating theater and to this advanced masterclass. Today, we are undertaking a comprehensive analysis and surgical reconstruction of a notoriously challenging athletic injury: "turf toe." While colloquially dismissed by the lay public as a mere sprain, orthopedic surgeons recognize this entity as a complex, potentially career-ending disruption of the capsular–ligamentous–sesamoid complex of the first metatarsophalangeal (MTP) joint. Our clinical exposure reveals a vast spectrum of these injuries, ranging from stable, self-limiting capsular sprains to complete, profoundly unstable disruptions that mandate meticulous surgical reconstruction. In my clinical experience, limited ankle dorsiflexion serves as a significant, albeit debated, predisposing biomechanical factor. This limitation places undue, magnified stress on the great toe MTP joint during the terminal stance phase of gait, specifically during explosive push-off maneuvers.
Untreated or conservatively mismanaged unstable turf toe injuries inevitably lead to debilitating, long-term sequelae. These include the development of severe hallux limitus or rigidus, intractable chronic pain, and a profound, measurable loss of push-off strength. Such deficits are not merely detrimental to elite athletic performance; they significantly impair routine daily ambulation and occupational functions. The epidemiological rise of these injuries correlates directly with the evolution of athletic environments. The widespread adoption of highly rigid, synthetic artificial playing surfaces, combined with the trend toward lighter, highly flexible, and less supportive athletic shoe wear, has unfortunately magnified the incidence of these injuries. In many cohorts, a severe turf toe injury proves far more disabling and requires a longer convalescence than a severe syndesmotic ankle sprain.
The primary mechanism of injury is a violent hyperextension force applied to the hallux MTP joint. Typically, this catastrophic failure occurs when an axial load is applied to the heel of a foot that is firmly planted and fixed in equinus, thereby forcing the great toe into an extreme, unphysiologic degree of dorsiflexion.

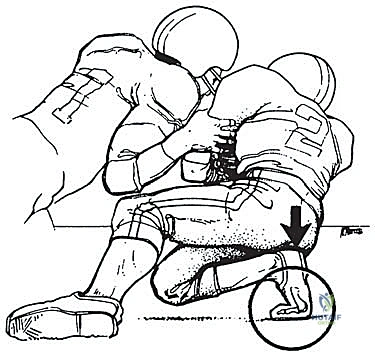
Biomechanical variations of this mechanism include a valgus-directed force vector, which selectively injures the plantar medial complex or the tibial sesamoid. If left untreated, this specific vector leads to the rapid development of a traumatic bunion and progressive hallux valgus deformity due to the unopposed pull of the adductor hallucis. Conversely, a less common varus-directed force can cause a traumatic varus deformity, implicating the lateral sesamoid complex. Early, accurate diagnosis utilizing advanced imaging, coupled with appropriate, anatomically precise surgical intervention, is paramount to restoring native joint kinematics, preserving the articular cartilage, and preventing chronic, irreversible disability.
Detailed Surgical Anatomy and Biomechanics
To execute a successful reconstruction, we must first master the intricate and unforgiving anatomy of the first MTP joint. This joint is a highly specialized ginglymoarthrodial articulation, and its stability relies on a delicate, dynamic interplay of adjacent capsular, ligamentous, tendinous, and osseous structures. A disruption in any single component of this complex constitutes a turf toe injury and alters the biomechanical loading of the entire forefoot.
The Plantar Plate and Sesamoid Complex
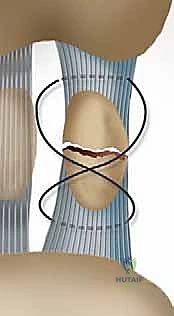
The plantar plate is the primary static stabilizer of the first MTP joint and the focal point of our surgical repair. It is a robust, thick fibrocartilaginous structure that functions essentially as a specialized extension of the joint capsule. Originating from the metatarsal neck just proximal to the articular cartilage, it inserts firmly into the plantar base of the proximal phalanx. The plantar plate is not an isolated structure; it has critical contiguous attachments to the transverse head of the adductor hallucis muscle, the flexor tendon sheaths, and the deep transverse intermetatarsal ligament, which connects the plantar plates of adjacent MTP joints, providing transverse plane stability to the forefoot.
Intimately associated with the plantar plate is the sesamoid complex. The tibial (medial) and fibular (lateral) sesamoids are two small, oval cortico-cancellous bones embedded within the medial and lateral slips of the flexor hallucis brevis (FHB) tendons, respectively. They articulate with the plantar aspect of the first metatarsal head, acting as a crucial mechanical fulcrum. This fulcrum increases the moment arm and enhances the mechanical advantage of the FHB during the push-off phase of gait. Their anatomical relationship to one another is maintained by the intersesamoid ligament, a strong, thick transverse band. Additional robust ligamentous attachments run between the sesamoids and both the metatarsal head (metatarsosesamoid ligaments) and the proximal phalanx (sesamoidophalangeal ligaments). It is imperative to remember that bipartite sesamoids are a common anatomical variant (more frequent in the tibial sesamoid) and must be distinguished from acute transverse fractures during our preoperative radiographic assessment.


Musculotendinous and Neurovascular Architecture
The dynamic stability of the hallux is governed by a complex arrangement of intrinsic musculature. The Flexor Hallucis Brevis (FHB), located in the third plantar layer of the foot, originates from the lateral cuneiform and the cuboid. It bifurcates into two tendinous slips that encase the sesamoids before inserting into the plantar base of the proximal phalanx, innervated by the medial plantar nerve. The Abductor Hallucis, residing in the first plantar layer, originates from the medial process of the calcaneal tuberosity and inserts conjunctly with the medial tendon of the FHB into the medial aspect of the proximal phalanx base. The Adductor Hallucis, also in the third plantar layer, consists of oblique and transverse heads that unite to insert through the fibular sesamoid into the lateral aspect of the hallux proximal phalanx, innervated by the lateral plantar nerve.
Surgically, the neurovascular structures dictate our operative approach and demand meticulous handling. The plantar-medial digital nerve and artery, alongside the plantar-lateral digital nerve and artery, course along the medial and lateral aspects of the great toe. The plantar-medial digital nerve is exceptionally vulnerable during the standard medial surgical approach. It frequently crosses obliquely, immediately deep to the planned incision line. We must identify, neurolyse, and gently retract these structures to avoid devastating iatrogenic traction neuropathies, painful neuroma formation, or localized vascular compromise.

Osteologically, the first metatarsal head is convex, articulating with the shallow concave base of the proximal phalanx. The plantar aspect of the metatarsal head features a prominent central ridge known as the crista, which separates the articular grooves for the tibial and fibular sesamoids. Disruption of the plantar plate or the FHB complex invariably leads to the proximal migration of the sesamoids relative to this crista, a hallmark radiographic sign of a severe turf toe injury.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a turf toe injury hinges on a meticulous clinical examination correlated with advanced imaging. The clinical evaluation must include a thorough history detailing the mechanism, perceived "pop," and any transient dislocation. On physical examination, the Vertical Lachman test is the gold standard for assessing sagittal plane instability. The examiner stabilizes the metatarsal head while applying a dorsal translating force to the proximal phalanx. Any laxity greater than the uninjured contralateral side, or the absence of a firm endpoint, indicates significant plantar plate disruption. We utilize the Anderson classification to grade these injuries: Grade 1 (stretching, minimal swelling), Grade 2 (partial tear, moderate swelling, restricted motion), and Grade 3 (complete tear, severe swelling, gross instability, positive Lachman).
Radiographic evaluation is mandatory and must include weight-bearing AP, lateral, and oblique views of the foot, alongside specific axial sesamoid views. We look for proximal migration of the sesamoids. Studies demonstrate that a distance greater than 10.4 mm from the tip of the tibial sesamoid to the phalanx, or more than 13.3 mm from the fibular sesamoid, indicates a 99.7% probability of complete plantar complex rupture. Forced dorsiflexion lateral views (stress views) are invaluable for diagnosing diastasis of a bipartite sesamoid or a true sesamoid fracture.


Magnetic Resonance Imaging (MRI) is highly recommended for all Grade 2 and Grade 3 injuries. High-resolution MRI, particularly T2-weighted and STIR sequences, accurately delineates the location of the plantar plate tear (distal avulsion vs. midsubstance), assesses the integrity of the intersesamoid ligament, and identifies concomitant articular cartilage damage or subchondral bone bruising on the metatarsal head.




Surgical intervention is definitively indicated for acute Grade 3 injuries in competitive athletes, large intra-articular osteochondral loose bodies, traumatic bunion deformities resulting from asymmetric soft tissue failure, diastasis of a bipartite sesamoid or displaced sesamoid fractures, and chronic injuries that have failed exhaustive nonoperative management (resulting in persistent pain and push-off weakness).
| Surgical Indications | Surgical Contraindications |
|---|---|
| Acute Grade 3 tear in a high-demand athlete | Active local or systemic infection |
| Displaced sesamoid fracture or diastasis > 3mm | Severe peripheral vascular disease |
| Traumatic hallux valgus (bunion) / varus deformity | Medically unfit for anesthesia |
| Retracted proximal migration of the sesamoid complex | Pre-existing severe Hallux Rigidus (Grade III/IV) |
| Failure of > 3-6 months of nonoperative treatment | Non-ambulatory patient status |
| Intra-articular loose bodies or large osteochondral lesions | Poor soft tissue envelope / compromised skin |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of a successful capsuloligamentous reconstruction. The surgical team must meticulously review all advanced imaging, specifically correlating the MRI findings with the anticipated intraoperative pathology. Identifying the exact anatomical location of the tear—whether it is a distal avulsion from the proximal phalanx base, a mid-substance tear, or a proximal avulsion from the metatarsal neck—dictates the choice of implants and the specific repair technique. The surgeon must be prepared with a variety of fixation options, including micro-suture anchors (typically 2.0mm to 3.0mm), heavy non-absorbable braided sutures, and orthobiologics if augmentation is deemed necessary.
Anesthesia typically consists of a regional block (such as an ultrasound-guided popliteal sciatic nerve block combined with a saphenous nerve block) to provide excellent intraoperative anesthesia and prolonged postoperative analgesia. This is usually combined with monitored anesthesia care (MAC) or general anesthesia, depending on patient preference and physiological status. A well-padded calf or ankle tourniquet is applied to ensure a bloodless surgical field, which is absolutely critical for identifying the delicate neurovascular structures and the torn, often retracted, edges of the plantar plate.


The patient is positioned supine on a radiolucent operating table to facilitate unhindered intraoperative fluoroscopy. A small bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the hallux points directly toward the ceiling. The foot is prepped and draped in a standard sterile fashion, allowing access up to the mid-calf. Prior to incision, the surgical landmarks, including the MTP joint line, the medial eminence, and the course of the abductor hallucis, are carefully palpated and marked with a sterile pen.


Step-by-Step Surgical Approach and Fixation Technique
The Surgical Approach and Exposure
The standard approach for a turf toe reconstruction is a medial utility incision, though a plantar approach can be utilized for isolated sesamoid pathology. The medial incision begins at the mid-diaphysis of the first metatarsal and extends distally to the mid-diaphysis of the proximal phalanx, centered directly over the MTP joint line. The incision is placed slightly plantar to the midline of the medial eminence, precisely along the glabrous junction (the transition line between the dorsal and plantar skin).
Upon incising the dermis, meticulous blunt dissection is employed. The immediate priority is the identification, mobilization, and protection of the plantar-medial digital nerve and artery. These structures often lie encased in the superficial fascia immediately deep to the incision. Once identified, they are gently retracted plantarward using vessel loops. The fascia over the abductor hallucis is then incised, and the muscle belly is mobilized and retracted plantarward to expose the underlying capsuloligamentous complex and the medial aspect of the plantar plate.



Joint Inspection and Preparation
A longitudinal arthrotomy is performed through the medial capsule to expose the intra-articular environment. The joint is thoroughly irrigated and inspected. The surgeon must meticulously evaluate the articular cartilage of the metatarsal head, particularly the dorsal aspect, which frequently sustains chondral impaction injuries during the hyperextension mechanism. Any loose chondral fragments are excised, and stable flaps are debrided.
Attention is then directed to the plantar plate. The tear is identified, and the degenerative or frayed edges are aggressively debrided back to healthy, bleeding, robust fibrocartilage. If the tear is a distal avulsion (the most common pattern), the plantar base of the proximal phalanx is decorticated using a high-speed burr or a curette to create a bleeding bony bed, optimizing the biological environment for soft tissue-to-bone healing.


Reconstruction and Fixation
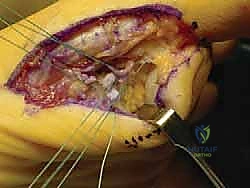
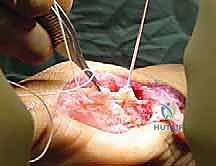
For a distal avulsion, fixation is typically achieved using two micro-suture anchors (e.g., 2.4mm or 3.0mm biocomposite or PEEK anchors) double-loaded with high-strength, non-absorbable tape or suture. These anchors are inserted into the decorticated plantar base of the proximal phalanx. The sutures are then passed through the robust proximal stump of the plantar plate using a horizontal mattress or Mason-Allen configuration to maximize pull-out strength.
Alternatively, a transosseous drill hole technique can be utilized. Crossed K-wires or a specialized drill guide are used to create tunnels from the dorsal aspect of the proximal phalanx exiting at the plantar base. Sutures are passed through the plantar plate, shuttled through the osseous tunnels, and tied dorsally over a bony bridge. Regardless of the technique, the critical step is tying the sutures while the MTP joint is held in approximately 10 to 15 degrees of plantarflexion. This removes all tension from the repair site and ensures the sesamoids are reduced anatomically beneath the metatarsal head.


If a sesamoid fracture is present and deemed unrepairable due to severe comminution, a partial sesamoidectomy (excising the smaller, usually distal pole) is performed, followed by a meticulous repair of the FHB tendon defect to maintain the mechanical linkage. Complete sesamoidectomy is avoided whenever possible due to the high risk of postoperative iatrogenic deformity (hallux valgus or varus) and severe loss of push-off power. Following the primary repair, the medial capsule and abductor hallucis are repaired to restore medial column stability. Intraoperative fluoroscopy is utilized to confirm the anatomic reduction of the sesamoids and the restoration of joint congruity.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following turf toe reconstruction can occur, and the surgeon must be prepared to manage them. The most ubiquitous complication is postoperative stiffness of the first MTP joint, potentially progressing to clinical hallux rigidus. This is an inherent risk, as the surgical goal of restoring stability directly competes with the goal of maximizing range of motion. Incidence rates of clinically significant stiffness range from 15% to 30% in the literature. Management involves aggressive, phased physical therapy; however, recalcitrant cases may require a subsequent manipulation under anesthesia or an arthroscopic/open capsular release.
Iatrogenic nerve injury, specifically to the plantar-medial digital nerve, is a devastating complication resulting in painful neuroma formation or chronic regional pain syndrome (CRPS). The incidence is estimated at 2% to 5%. Meticulous surgical dissection is the primary preventative measure. If a neuroma develops and fails conservative management (gabapentinoids, targeted injections), surgical excision with proximal transposition of the nerve stump into the intrinsic musculature may be required.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| MTP Joint Stiffness / Hallux Rigidus | 15% - 30% | Prevention: Early protected ROM, precise tensioning. ** |
Clinical & Radiographic Imaging Archive