Mastering First MTP Joint Arthrodesis with Bone-Block Distraction: A Comprehensive Intraoperative Guide

Key Takeaway
This masterclass details first MTP joint arthrodesis with bone-block distraction, a salvage procedure for severe great toe deformities and bone loss. Fellows will learn preoperative planning, precise surgical execution, comprehensive anatomical considerations, and critical pearls to restore first ray length and function. We cover patient positioning, meticulous dissection, graft harvesting, and optimal fixation techniques, emphasizing intraoperative decision-making for successful outcomes.
Welcome, colleagues, to this definitive masterclass on one of the most challenging yet profoundly rewarding procedures in foot and ankle reconstruction: the First Metatarsophalangeal (MTP) Joint Arthrodesis with Bone-Block Distraction. This is not your routine primary hallux valgus correction or standard arthrodesis for mild hallux rigidus. We are discussing a complex salvage procedure reserved for patients who have endured multiple prior surgical failures, catastrophic trauma, or severe degenerative conditions resulting in critical bone loss. Our ultimate operative goal is to meticulously restore the anatomic length, precise alignment, and structural integrity of the first ray, thereby alleviating intractable pain and re-establishing physiologic forefoot biomechanics.
Comprehensive Introduction and Patho-Epidemiology
First MTP joint arthrodesis with structural bone-block distraction serves as a robust, definitive alternative to joint-sparing or simple resectional procedures in the salvage of severe great toe deformities. While the modern orthopedic philosophy always strives to preserve motion where possible, in cases of profound joint destruction, avascular necrosis, or iatrogenic bone loss, an isolated in-situ fusion is often insufficient. Fusing a significantly shortened first ray invariably leads to catastrophic biomechanical failure of the forefoot.
We primarily employ the interpositional bone block distraction technique to address substantial osseous defects. The patho-epidemiology of these defects is diverse. A frequent culprit is the failed hallux valgus procedure, particularly those historic or poorly executed osteotomies that resulted in excessive bone resection or compromised the vascular supply to the first metatarsal head. Avascular necrosis (AVN) of the metatarsal head, while relatively rare, is a devastating complication occasionally seen after distal chevron or Mitchell osteotomies. When the necrotic bone collapses, it creates a massive structural void that must be excised and reconstructed.

Another major indication is the failed first MTP joint arthroplasty. The historical use of silicone (silastic) implants, while once popular, has left a legacy of severe complications. The inevitable wear of these implants generates particulate debris, triggering an aggressive foreign-body macrophage response. This leads to massive osteolysis, cyst formation, and profound destruction of both the metatarsal head and the base of the proximal phalanx.

Historically, procedures such as the Keller-Brandes or Mayo resectional arthroplasties were performed to address severe hallux pathology. While they temporarily addressed the immediate pain by decompressing the joint, they inherently led to significant, non-physiologic shortening of the hallux and the entire first ray.


This iatrogenic shortening creates a predictable cascade of biomechanical disasters. The first ray, now mechanically disadvantaged and too short, can no longer bear its physiological share of the load during the terminal stance phase of gait. This shifts excessive, pathological loading to the lesser metatarsal heads—a phenomenon known as transfer metatarsalgia. Patients develop intractable plantar keratoses, severe pain, and frequently progress to lesser MTP joint instability, plantar plate tears, and crossover toe deformities. Therefore, the distraction arthrodesis is not merely about fusing a joint; it is a critical restorative procedure designed to re-establish the weight-bearing capacity of the medial column.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of first ray anatomy and biomechanics is non-negotiable for the reconstructive surgeon attempting this procedure. The first ray, comprising the first metatarsal and the medial cuneiform, is the primary load-bearing structure of the forefoot. During a normal gait cycle, the first metatarsal head bears approximately twice the load of the lesser metatarsals. This load-bearing capacity is entirely dependent on the structural length of the metatarsal and the functional integrity of the plantar aponeurosis via the windlass mechanism.
When the first MTP joint is dorsiflexed during the push-off phase, the plantar fascia tightens around the metatarsal head, elevating the longitudinal arch and converting the foot into a rigid lever for propulsion. If the first ray is iatrogenically shortened, the windlass mechanism is effectively decoupled. The plantar fascia cannot achieve adequate tension, the arch remains supple, and the propulsive forces are abnormally shunted laterally. Restoring the length with a structural bone block re-tensions the plantar fascia and restores this critical biomechanical linkage.
The soft tissue envelope surrounding the first MTP joint is complex and must be managed with extreme care, especially in revision scenarios. Dorsally, the extensor hallucis longus (EHL) and extensor hallucis brevis (EHB) tendons dictate sagittal plane alignment. Plantarly, the flexor hallucis longus (FHL) runs between the medial and lateral sesamoids, which are embedded within the tendons of the flexor hallucis brevis (FHB). In cases of severe shortening or prior surgery, these structures are often encased in dense, unyielding scar tissue.
Furthermore, the neurovascular bundles, specifically the proper plantar digital nerves and the dorsal cutaneous branches of the superficial peroneal nerve, are frequently displaced or tethered by previous surgical scarring. Subperiosteal dissection is mandatory to mobilize the soft tissue envelope as a single, contiguous sleeve. This not only protects the neurovascular structures but also preserves the delicate periosteal blood supply to the remaining host bone, which is absolutely critical for the incorporation of the massive structural graft we are about to interpose.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in bone-block distraction arthrodesis. This procedure is an immense physiological undertaking for the foot, requiring optimal host biology to incorporate a large structural graft. The primary indication remains the symptomatic, significantly shortened first ray with an irreparable MTP joint. We quantify "significant shortening" as anything greater than 5 to 8 millimeters compared to the contralateral normal foot, or shortening that has already precipitated clinical transfer metatarsalgia.
We frequently encounter patients with severe rheumatoid arthritis or other inflammatory arthropathies who present with massive joint destruction and concurrent bone loss. Similarly, post-traumatic conditions resulting in severe intra-articular comminution, cartilage loss, and subsequent bone resorption are excellent candidates. In cases of severe hallux rigidus where aggressive cheilectomies have failed and eroded the dorsal half of the joint, or where the joint space is completely obliterated with cystic degeneration, distraction arthrodesis provides a definitive, durable solution.
However, the contraindications must be respected rigorously. Active or inadequately treated osteomyelitis is an absolute contraindication to structural bone grafting. Any residual infection will rapidly colonize the avascular graft, leading to catastrophic failure. Severe peripheral vascular disease (PVD) or critical limb ischemia also precludes this surgery, as the soft tissue envelope will not tolerate the tension of distraction, and the bone will lack the necessary perfusion for graft incorporation.
| Category | Indications | Contraindications |
|---|---|---|
| Primary Pathologies | Failed hallux valgus surgery with severe shortening | Active or untreated local/systemic infection |
| Degenerative/Necrotic | AVN of the first metatarsal head; Severe cystic hallux rigidus | Critical limb ischemia / Severe PVD |
| Iatrogenic | Failed silastic or metallic MTP arthroplasty | Active Charcot neuroarthropathy of the midfoot/forefoot |
| Traumatic/Structural | Post-traumatic bone loss; Rheumatoid arthritis with severe erosion | Severe, uncorrectable soft tissue contracture precluding closure |
| Clinical Symptoms | Intractable transfer metatarsalgia due to a short first ray | Medical non-compliance or inability to adhere to strict NWB protocols |
Preoperative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the difference between a smooth, predictable reconstruction and an intraoperative disaster. The clinical evaluation must focus heavily on the vascular status of the foot, the quality of the soft tissue envelope, and the presence of any lesser toe deformities that may need concurrent addressing. Assessing the flexibility of the soft tissues is vital; if the toe has been shortened for decades, acute distraction may place excessive tension on the neurovascular bundles, risking digital ischemia.
Radiographic evaluation is exhaustive. We demand high-quality, weight-bearing anteroposterior, lateral, and sesamoid axial views. These radiographs allow us to assess the degree of bone loss, the quality of the remaining bone stock, and the position of the sesamoids. In cases of suspected AVN or occult cysts, an MRI or a fine-cut CT scan is invaluable for mapping the precise margins of viable, bleeding bone.
Templating is a mandatory step. We routinely utilize digital templating software, overlaying the templated footprint of the contralateral, unaffected foot onto the operative foot. This allows us to calculate the exact millimeter length of the structural graft required to restore the parabolic curve of the metatarsal heads. We must also plan for the intrinsic shortening that occurs when we prepare the host bone surfaces down to bleeding, healthy cancellous bone. If we need 10mm of lengthening, and we resect 2mm from both the metatarsal and the phalanx to achieve flat, healthy surfaces, our final graft must be 14mm in length.

The patient is positioned supine on the operating table. A critical maneuver is the placement of a bump beneath the ipsilateral hip. This subtly internally rotates the lower extremity, positioning the foot perfectly straight up for the surgeon. More importantly, if an autologous tricortical iliac crest bone graft is planned, this hip bump elevates the anterior pelvis, providing excellent, unimpeded access to the anterior superior iliac spine (ASIS) and the iliac crest. The C-arm fluoroscopy unit is brought in from the contralateral side, ensuring we can obtain flawless AP and lateral images without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The execution of this procedure demands meticulous soft tissue handling, precise bone preparation, and rigid biomechanical fixation. We begin with the approach to the first MTP joint.
The MTP Joint Approach and Soft Tissue Envelope
We utilize a standard dorsal longitudinal approach. The skin incision begins approximately 4 cm proximal to the MTP joint, centered over the first metatarsal, and extends distally to the interphalangeal (IP) joint. It is imperative to incorporate or cross previous surgical scars at perpendicular angles to avoid creating narrow, ischemic skin bridges.

Deep dissection is carried straight down to the extensor retinaculum. We typically retract the EHL tendon laterally, protecting it throughout the case. The joint capsule and the periosteum over the distal metatarsal and proximal phalanx are incised longitudinally in a single, continuous layer.
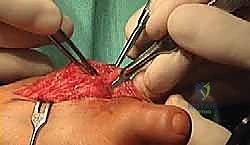
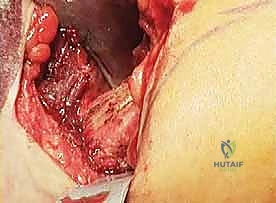
Subperiosteal preparation is absolutely mandatory here. Using a sharp periosteal elevator, we create a full-thickness soft tissue envelope, elevating the capsule, collateral ligaments, and periosteum away from the bone. This extensive release is necessary to mobilize the scarred soft tissues, allowing for the subsequent distraction without tethering.

Host Bone Preparation
Once the joint is exposed, we must aggressively debride all fibrous tissue, necrotic bone, and remnants of previous implants. The goal is to reach punctate, bleeding subchondral bone.

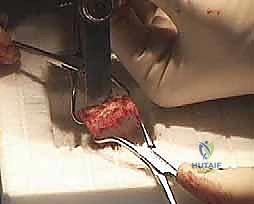
We have two primary methods for bone preparation: flat planar cuts or cup-and-cone reaming. For large structural grafts, flat planar cuts using an oscillating saw are often preferred as they provide excellent surface area contact for a tricortical block. However, if the bone loss is somewhat contained, specialized cannulated reamers can be used to create congruent surfaces.


The metatarsal head and the base of the proximal phalanx are prepared meticulously. We must ensure that the prepared surfaces are perpendicular to the long axis of their respective bones to prevent angular deformity when the graft is interposed.


Autologous Iliac Crest Graft Harvest
If structural autograft is selected, we shift our attention to the ipsilateral iliac crest. The incision is made 2 to 3 cm posterior to the ASIS, strictly avoiding the lateral femoral cutaneous nerve.
We dissect down to the fascia, incise it, and subperiosteally elevate the iliacus and gluteal muscles to expose the inner and outer tables of the ilium. Using an oscillating saw and sharp osteotomes, a tricortical block of the pre-measured dimensions is carefully harvested.

The tricortical nature of this graft is vital; the dense cortical struts provide immediate mechanical stability against the compressive forces of the forefoot, while the rich cancellous interior provides the osteoprogenitor cells and scaffolding necessary for rapid incorporation.


Graft Contouring, Insertion, and Distraction
The harvested autograft (or thawed allograft) must now be sculpted to perfectly match the prepared host bone defects. We use a rongeur or a burr to contour the graft, ensuring maximal surface area contact.


To insert the graft, we apply longitudinal traction to the hallux. In cases of severe contracture, a temporary external fixator or a lamina spreader placed between the metatarsal and phalanx can assist in achieving the necessary distraction. The graft is then press-fit into the defect.

At this juncture, we must critically assess the alignment. The ideal position for a first MTP fusion is approximately 10 to 15 degrees of valgus and 15 to 20 degrees of dorsiflexion relative to the first metatarsal shaft. This allows the hallux to clear the ground during the swing phase while maintaining pulp contact during terminal stance.
Rigid Internal Fixation
Once perfect alignment and length are achieved, rigid internal fixation is applied. While crossed lag screws can be used for simple in-situ fusions, a structural bone-block distraction mandates the use of a robust dorsal or medial locking plate.

The plate acts as a tension band dorsally and neutralizes the massive bending moments placed on the graft. We typically secure the plate with multiple locking screws in both the metatarsal and the proximal phalanx.


If the graft size allows, an independent interfragmentary lag screw can be passed through the plate, traversing the phalanx, the graft, and into the metatarsal to provide massive compression across both fusion interfaces.


Final Evaluation and Closure
Intraoperative fluoroscopy is utilized to confirm hardware placement, graft positioning, and overall axial alignment. We check the cascade of the toes to ensure the first ray is appropriately lengthened without over-distracting the joint, which could lead to digital ischemia.


The wound is meticulously irrigated. The capsuloperiosteal flap is closed over the plate to the best of our ability to prevent tendon tethering. The skin is closed with non-absorbable sutures using a vertical mattress technique to maximize eversion and minimize tension on the compromised skin edges.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, bone-block distraction arthrodesis carries a higher complication profile than primary arthrodesis, largely due to the
