Orthopedic Sport Review | Dr Hutaif Sports Medicine Rev -...

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about ORTHOPEDIC MCQS ONLINE 013 SPORT. This orthopedic interactive module offers a sports medicine self-assessment with multiple-choice questions covering various clinical scenarios, such as shoulder dislocation and knee injuries. Each question includes a detailed explanation and a comprehensive discussion for questions, helping users understand appropriate diagnoses and treatment strategies in sports medicine and orthopedics.
Orthopedic Sport Review | Dr Hutaif Sports Medicine Rev -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Anatomic ACL reconstruction relies on identifying the femoral footprint. The lateral intercondylar ridge (Resident's ridge) serves as a key surgical landmark.
Where is the native ACL femoral footprint located relative to this ridge when the knee is viewed at 90 degrees of flexion?
Explanation
Question 2
A 24-year-old athlete undergoes an isolated Posterior Cruciate Ligament (PCL) reconstruction using a double-bundle technique.
To accurately recreate the biomechanics of the native PCL, at what degree of knee flexion should the anterolateral (AL) and posteromedial (PM) bundles be tensioned and fixed, respectively?
Explanation
Question 3
During a Latarjet procedure for recurrent anterior shoulder instability with significant glenoid bone loss, the coracoid process is transferred to the anterior glenoid.
Which nerve is at greatest risk of iatrogenic injury during the medial retraction of the conjoined tendon and subsequent screw fixation?
Explanation
Question 4
A 45-year-old male sustains a posterior root tear of the medial meniscus during a deep squat.
Biomechanically, what is the consequence of this specific injury on the tibiofemoral joint contact pressures if left untreated?

Explanation
Question 5
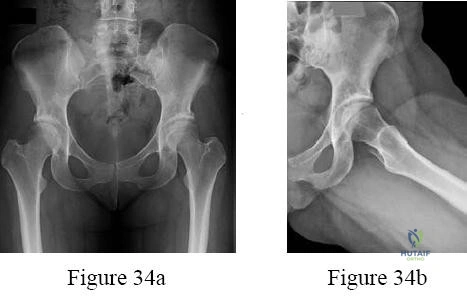
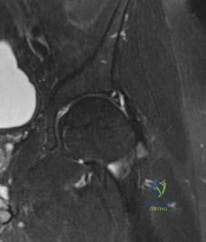
A 22-year-old hockey player presents with anterior groin pain exacerbated by hip flexion and internal rotation. Imaging reveals Cam-type femoroacetabular impingement (FAI).
During hip arthroscopy, which of the following intra-articular pathologic findings is most commonly associated with isolated Cam impingement?

Explanation
Question 6
During a Medial Patellofemoral Ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon inadvertently places the femoral tunnel proximal to the anatomic insertion site.
What is the expected biomechanical consequence during knee range of motion?

Explanation
Question 7
A 30-year-old runner has an isolated, full-thickness 3.5 cm^2 chondral defect on the medial femoral condyle. The surgeon considers Matrix-induced Autologous Chondrocyte Implantation (MACI).
Which of the following represents an absolute or strong relative contraindication to MACI for this patient?

Explanation
Question 8
A 20-year-old collegiate baseball pitcher undergoes an ulnar collateral ligament (UCL) reconstruction utilizing the Docking technique.
Which bundle of the native UCL is the primary restraint to valgus stress at 90 degrees of elbow flexion and is the primary structure surgically reconstructed?
Explanation
Question 9
A 35-year-old overhead athlete presents with posterior shoulder pain and profound weakness in external rotation. An MRI reveals a paralabral cyst in the spinoglenoid notch.
Which physical exam finding and associated intra-articular pathology is most likely present?
Explanation
Question 10
A 28-year-old football player sustains a multiligamentous knee injury. Physical exam reveals a positive posterior drawer test and increased external tibial rotation at 30 degrees of knee flexion compared to the contralateral side. However, at 90 degrees of knee flexion, the external tibial rotation is symmetric bilaterally. What is the most likely injury pattern?
Explanation
Question 11
In the surgical management of a Type V acromioclavicular (AC) joint dislocation, reconstructing the coracoclavicular (CC) ligaments is prioritized.
What is the precise anatomic orientation and insertion of the native conoid and trapezoid ligaments on the clavicle?
Explanation
Question 12
A 35-year-old male sustains an acute, complete rupture of the Achilles tendon.
He opts for non-operative management utilizing a functional rehabilitation protocol. Compared to surgical repair, which of the following is true regarding his clinical outcomes according to recent level-1 evidence?

Explanation
Question 13
A 14-year-old female gymnast complains of lateral elbow pain, clicking, and a loss of 15 degrees of extension. Radiographs and MRI demonstrate a 12mm osteochondral defect of the capitellum with subchondral fluid and a loose cartilaginous flap.
What is the most appropriate surgical intervention?

Explanation
Question 14
A 22-year-old female with an isolated ACL deficiency and genu varum is scheduled for an ACL reconstruction and an opening-wedge high tibial osteotomy (HTO). What is the potential biomechanical consequence of a standard medial opening-wedge HTO on the sagittal plane of the knee, and how does it affect the ACL graft?
Explanation
Question 15
In overhead throwing athletes, a Type II SLAP tear is often attributed to the 'peel-back' mechanism.
During which phase of the throwing motion does the maximal peel-back force occur on the superior labrum?

Explanation
Question 16
During the surgical evaluation of an acute ankle injury, the 'Cotton test' is performed to assess the integrity of the syndesmosis. Which specific anatomic structure is considered the primary restraint to anterior subluxation of the distal fibula and is typically the first to tear in an external rotation syndesmotic injury?
Explanation
Question 17
A 9-year-old Tanner stage 1 male sustains a complete, mid-substance ACL tear.
A physeal-sparing extra-articular reconstruction is planned. Which structure is traditionally utilized and routed over the 'over-the-top' position to reconstruct the ACL without violating the open physes?
Explanation
Question 18
A 65-year-old manual laborer presents with a massive, irreparable posterosuperior rotator cuff tear (supraspinatus and infraspinatus) with an intact subscapularis and functional deltoid. He lacks active external rotation (positive hornblower's sign). Which tendon transfer is most biomechanically appropriate to restore external rotation in this patient?
Explanation
Question 19
In the Schenck classification of knee dislocations (KD), a KD III-L injury indicates disruption of the ACL, PCL, and the Posterolateral Corner (PLC).
This specific injury pattern carries the highest risk of injury to which of the following neurovascular structures?

Explanation
Question 20
A 28-year-old competitive weightlifter feels a 'pop' in his anterior axilla while performing a heavy bench press. MRI confirms a complete rupture of the pectoralis major tendon.
At the humeral insertion site, what is the spatial relationship of the sternocostal head relative to the clavicular head?

Explanation
Question 21
A 23-year-old professional soccer player presents with anterior knee pain and swelling. MRI reveals a 4.5 cm² full-thickness osteochondral defect with a 6 mm deep subchondral bone cyst on the weight-bearing surface of the medial femoral condyle. He has previously undergone a failed microfracture procedure. What is the most appropriate definitive surgical treatment?
Explanation
Question 22
A 45-year-old construction worker complains of deep shoulder pain that worsens with overhead lifting. Physical examination reveals a positive O'Brien's test and pain with resisted forearm supination. MRI demonstrates a Type II Superior Labrum Anterior to Posterior (SLAP) tear. Given his age and occupation, what is the most appropriate surgical management if conservative therapy fails?
Explanation
Question 23
During the evaluation of a patient with a multiligamentous knee injury, the examiner performs the Dial test. The test demonstrates 15 degrees of increased external rotation of the tibia relative to the femur at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is symmetric bilaterally. This clinical finding most likely indicates an isolated injury to which of the following?
Explanation
Question 24
A 28-year-old professional hockey player presents with chronic groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a prominent bony bump at the anterosuperior femoral head-neck junction with an alpha angle of 65 degrees. He is diagnosed with Femoroacetabular Impingement (FAI). Which of the following conditions is a known risk factor for the development of this specific type of lesion?
Explanation
Question 25
A 19-year-old collegiate baseball pitcher complains of medial elbow pain during the late cocking and early acceleration phases of throwing. The 'moving valgus stress test' is strongly positive. If surgical reconstruction is indicated, which bundle of the ulnar collateral ligament (UCL) must be primarily reconstructed, and at what degree of flexion is it the primary restraint to valgus stress?
Explanation
Question 26
A 16-year-old female presents with recurrent patellar dislocations. Imaging reveals a ruptured Medial Patellofemoral Ligament (MPFL). If the surgeon plans a reconstruction, the anatomic femoral attachment of the MPFL (Schöttle point) should be located in relation to which osseous landmarks on a true lateral radiograph?
Explanation
Question 27
A 32-year-old weightlifter feels a sudden pop in his anterior chest wall while performing a heavy bench press. He presents with a loss of the anterior axillary fold and ecchymosis extending down his arm. An MRI confirms a complete rupture of the pectoralis major tendon. Which of the following best describes the pathoanatomy and usual location of this specific injury?
Explanation
Question 28
A 55-year-old patient undergoes an arthroscopic partial meniscectomy for an isolated posterior horn tear of the medial meniscus. Intraoperatively, the tear is identified as a complete radial tear located 2 mm from the posterior bony attachment. Which of the following correctly describes the biomechanical consequence of leaving this root tear un-repaired?
Explanation
Question 29
A 24-year-old professional football player suffers an acute ankle injury after his foot is planted and externally rotated while a defender falls on his leg. Physical examination reveals a positive squeeze test and tenderness extending 6 cm proximal to the ankle joint over the anterior tibiofibular ligament. What is the most reliable intraoperative dynamic test to confirm syndesmotic instability?
Explanation
Question 30
A 13-year-old gymnast complains of chronic, insidious onset lateral elbow pain, stiffness, and clicking. Examination reveals a 15-degree flexion contracture. Radiographs show a radiolucent lesion on the anterolateral aspect of the capitellum. MRI confirms Osteochondritis Dissecans (OCD) with an intact articular surface. What differentiates capitellar OCD from Panner's disease?
Explanation
Question 31
A 60-year-old female presents with lateral hip pain that radiates down her lateral thigh. She reports pain when rising from a seated position and lying on the affected side. On exam, she has a positive Trendelenburg sign and weakness in hip abduction. Trochanteric bursitis treatments have failed. MRI reveals a full-thickness tear of the gluteus medius tendon. At which anatomic footprint does this tendon most commonly tear?
Explanation
Question 32
A 22-year-old professional baseball pitcher presents with posterior shoulder pain. On exam, he has a 25-degree deficit in glenohumeral internal rotation (GIRD) compared to his non-throwing arm, but total arc of motion is equal bilaterally. When his shoulder is placed in 90 degrees of abduction and maximal external rotation, he complains of deep posterior pain. What is the classic pathoanatomic finding on arthroscopy for 'Internal Impingement' in this population?
Explanation
Question 33
A 26-year-old male is involved in a high-speed motorcycle accident. In the ER, his knee is grossly unstable in multiple planes, and he has a documented Knee Dislocation (Schenck KD-III). His Ankle-Brachial Index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 34
A 34-year-old recreational weightlifter presents with severe shoulder pain and inability to actively internally rotate the shoulder after a forceful extension injury. On exam, he has increased passive external rotation compared to the normal side and a positive 'lift-off' test. An MRI confirms an isolated subscapularis tendon rupture. Which accompanying pathology is most frequently associated with a complete rupture of the upper subscapularis?
Explanation
Question 35
A 29-year-old professional volleyball player complains of isolated, painless weakness of the throwing arm. On physical examination, she demonstrates marked weakness in active external rotation with the arm at the side, but normal internal rotation, normal abduction, and no sensory deficits. An MRI is performed. What is the most likely pathological finding?
Explanation
Question 36
A 19-year-old dancer presents with a painful snapping sensation in her anterior hip when extending her hip from a flexed, abducted, and externally rotated position. An ultrasound demonstrates the iliopsoas tendon snapping over a bony prominence. What is the most common anatomic structure over which the iliopsoas snaps in 'Internal Snapping Hip' (Coxa Saltans Interna)?
Explanation
Question 37
A 35-year-old recreational basketball player sustains an acute Achilles tendon rupture. He is discussing operative vs. non-operative management. According to recent high-level evidence, if an early functional rehabilitation protocol is utilized, how do the outcomes of non-operative management compare to operative repair?
Explanation
Question 38
A 14-year-old male presents with non-specific knee pain. Imaging reveals Osteochondritis Dissecans (OCD) of the knee. What is the most common anatomical location for an OCD lesion in the knee?
Explanation
Question 39
A 25-year-old rugby player sustains an acute anterior shoulder dislocation. During the reduction in the emergency department, the physician notes weakness in shoulder abduction and decreased sensation over the lateral deltoid. Which of the following describes the most likely associated nerve injury and its typical prognosis?
Explanation
Question 40
A 40-year-old male falls directly onto his shoulder point. Radiographs show an acromioclavicular (AC) joint separation with 150% superior displacement of the clavicle relative to the acromion. There is no disruption of the deltotrapezial fascia. Based on the Rockwood classification, what type of injury is this, and what is the generally recommended treatment for this specific grade?
Explanation
Question 41
A 25-year-old male sustains a dashboard injury during a motor vehicle collision. Physical examination reveals a grade III posterior sag sign. A Posterior Cruciate Ligament (PCL) reconstruction is planned. What distinct biomechanical advantage does the tibial inlay technique offer over the traditional transtibial technique for PCL reconstruction?
Explanation
Question 42
A 22-year-old collegiate soccer player is evaluated for a knee injury. The dial test demonstrates 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the uninjured contralateral side, but symmetric external rotation at 90 degrees of knee flexion. Which of the following is the most likely isolated injured structure?
Explanation
Question 43
A 16-year-old female presents with recurrent lateral patellar dislocations. Surgical stabilization with Medial Patellofemoral Ligament (MPFL) reconstruction is indicated. Based on the classic anatomical layers of the medial knee described by Warren and Marshall, the native MPFL is located in which layer?
Explanation
Question 44
A 20-year-old collegiate baseball pitcher undergoes an ulnar collateral ligament (UCL) reconstruction using the docking technique. What is the primary anatomical landmark for the accurate placement of the ulnar bone tunnel?
Explanation
Question 45
A 13-year-old male gymnast presents with a 4-month history of lateral elbow pain, locking, and catching. MRI demonstrates an osteochondritis dissecans (OCD) lesion of the capitellum with T2 fluid signal interposing between the osteochondral fragment and the underlying bone. What is the most appropriate next step in management?
Explanation
Question 46
A 22-year-old professional baseball pitcher presents with posterior shoulder pain. Physical examination demonstrates Glenohumeral Internal Rotation Deficit (GIRD) with internal rotation decreased by 25 degrees and the total arc of motion decreased by 15 degrees compared to the non-throwing shoulder. What is the primary pathophysiological driver of this true pathologic GIRD?
Explanation
Question 47
During surgical repair of an acute, complete pectoralis major rupture in a weightlifter, the surgeon must accurately identify and reattach the tendinous footprint. Which of the following statements correctly describes the anatomical relationship of the pectoralis major insertion on the humerus?
Explanation
Question 48
A 25-year-old hockey player presents with chronic groin pain exacerbated by hip flexion, adduction, and internal rotation. Radiographs reveal an alpha angle of 65 degrees. He is diagnosed with Femoroacetabular Impingement (FAI) and undergoes hip arthroscopy for cam lesion resection. A cam lesion most commonly occurs at which location on the proximal femur?
Explanation
Question 49
A 28-year-old professional soccer player presents with chronic lower abdominal and proximal medial thigh pain unresponsive to 6 months of nonoperative management. MRI reveals a core muscle injury (athletic pubalgia). The primary pathology typically involves a disruption or imbalance at the confluence of which two structures?
Explanation
Question 50
A 21-year-old cross-country runner presents with bilateral exercise-induced anterolateral leg pain that resolves 30 minutes after stopping activity. Chronic exertional compartment syndrome (CECS) is suspected. According to the Pedowitz criteria, which of the following intramuscular compartment pressure measurements is diagnostic of CECS?
Explanation
Question 51
A 45-year-old recreational overhead athlete is diagnosed with an isolated Type II Superior Labrum Anterior and Posterior (SLAP) tear. According to recent literature, what is the expected clinical advantage of primary biceps tenodesis over SLAP repair in this specific patient demographic?
Explanation
Question 52
A 50-year-old female marathon runner complains of recalcitrant lateral hip pain. Physical examination demonstrates a positive Trendelenburg sign. MRI confirms a full-thickness tear of the gluteus medius tendon. During an open repair, the surgeon isolates the primary footprint of the gluteus medius. This tendon inserts onto which specific facet(s) of the greater trochanter?
Explanation
Question 53
A 19-year-old ballet dancer complains of a painful popping sensation deep in her anterior hip when she extends her hip from a flexed, abducted, and externally rotated position. Dynamic ultrasound confirms internal coxa saltans. Which anatomical structures are mechanically interacting to cause this snapping?
Explanation
Question 54
A 40-year-old male sustains a severe hyperflexion injury to his knee and is diagnosed with a posterior medial meniscal root tear. Which of the following statements best describes the in vivo biomechanical consequence of this specific injury?
Explanation
Question 55
A 25-year-old professional basketball player presents with persistent medial knee pain. MRI reveals an isolated, unipolar, full-thickness (Outerbridge Grade IV) chondral defect on the weight-bearing surface of the medial femoral condyle, measuring 4.5 cm². The subchondral bone is completely intact without cysts or edema. He has failed nonoperative treatment. Which cartilage restoration procedure is most appropriate?
Explanation
Question 56
During an anatomic reconstruction of the coracoclavicular (CC) ligaments for a high-grade acromioclavicular (AC) joint separation, the surgeon must drill clavicular and coracoid tunnels to recreate the conoid and trapezoid ligaments. Which of the following statements accurately describes their native anatomical relationship?
Explanation
Question 57
A 35-year-old water skier suffers a forceful hip flexion injury with the knee extended, resulting in a 3 cm retracted avulsion of the proximal hamstring complex. During open surgical repair, the surgeon identifies the ischial tuberosity footprint. Which of the following accurately describes the anatomical footprint of the proximal hamstring complex?
Explanation
Question 58
A 12-year-old baseball pitcher presents with progressive medial elbow pain and decreased pitch velocity. Radiographs reveal widening and irregularity of the medial epicondyle apophysis. He is diagnosed with 'Little Leaguer's Elbow' (medial epicondyle apophysitis). What is the primary biomechanical force responsible for this condition?
Explanation
Question 59
A 21-year-old collegiate basketball player sustains an acute Zone II fifth metatarsal base fracture (Jones fracture). To minimize the risk of nonunion and expedite return to play, intramedullary screw fixation is planned. Which of the following vascular structures is most uniquely at risk of disruption by this specific fracture pattern, predisposing to nonunion?
Explanation
Question 60
A 19-year-old football player sustains a severe blunt trauma to his anterior thigh from a helmet collision. Three weeks later, he presents with significantly restricted knee flexion and a firm, painful mass in his quadriceps. Radiographs demonstrate peripheral calcification within the muscle belly. What is the most appropriate initial management for this condition?
Explanation
Question 61
A 24-year-old hockey player presents with anterior groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a prominent alpha angle.
Which of the following is the most likely location of the associated labral or chondral pathology in this condition?
Explanation
Question 62
A 25-year-old football player sustains a high-energy knee dislocation (KD-III).
Following closed reduction in the emergency department, his Ankle-Brachial Index (ABI) is measured at 0.85. He has palpable distal pulses. What is the most appropriate next step in management?
Explanation
Question 63
A 22-year-old collegiate baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. He exhibits increased external rotation and decreased internal rotation (GIRD) compared to the contralateral side. What is the primary pathophysiologic mechanism of this condition?
Explanation
Question 64
During an ulnar collateral ligament (UCL) reconstruction using the docking technique, the surgeon decides to transpose the ulnar nerve subcutaneously. Which of the following is the primary risk factor for postoperative ulnar neuropathy in this specific scenario?
Explanation
Question 65
A 26-year-old professional soccer player suffers an external rotation injury to his ankle. Radiographs show no fracture.
An MRI demonstrates a complete tear of the anterior inferior tibiofibular ligament (AITFL) and interosseous membrane extending 4 cm proximal to the joint line, with an intact deltoid ligament. Dynamic stress views show no widening of the medial clear space. What is the most appropriate management?
Explanation
Question 66
A 21-year-old athlete undergoes an anatomic posterolateral corner (PLC) reconstruction. The fibular collateral ligament (FCL) graft is being secured on the femur. What are the correct anatomic landmarks for the femoral footprint of the FCL?
Explanation
Question 67
A 45-year-old female marathon runner complains of recalcitrant lateral hip pain. Examination shows a positive Trendelenburg sign and pain with resisted hip abduction. MRI reveals a full-thickness tear of the gluteus medius at its insertion. To which facet(s) of the greater trochanter does the main tendon of the gluteus medius primarily attach?
Explanation
Question 68
A 35-year-old weightlifter feels a "pop" in his anterior shoulder during a heavy bench press. He now has increased passive external rotation and profound weakness in internal rotation.
He tests positive on the bear hug test. Which of the following associated injuries is most likely present given this pathology?
Explanation
Question 69
A 19-year-old soccer player has a symptomatic 2.5 cm^2 full-thickness chondral defect on the weight-bearing surface of the medial femoral condyle. He has failed conservative management. What is the most appropriate surgical treatment that provides hyaline-like cartilage repair for a defect of this size?
Explanation
Question 70
A 22-year-old college basketball player sustains a fracture at the metaphyseal-diaphyseal junction of the fifth metatarsal.
He is in mid-season and wishes to return to play as soon as possible. What is the recommended treatment?
Explanation
Question 71
A 28-year-old professional volleyball player presents with vague posterior shoulder pain and weakness in external rotation. Examination reveals isolated atrophy of the infraspinatus muscle.
Where is the most likely site of neural compression?
Explanation
Question 72
A 14-year-old male presents with knee pain and catching. Radiographs demonstrate a classical osteochondritis dissecans (OCD) lesion.
What is the most common anatomical location for this lesion in the knee?
Explanation
Question 73
A 42-year-old competitive weightlifter undergoes an anterior single-incision repair for an acute complete distal biceps tendon rupture.
Postoperatively, he complains of significant numbness over the lateral aspect of his forearm. Which nerve is most likely injured?
Explanation
Question 74
During an arthroscopic posterior cruciate ligament (PCL) reconstruction using a single-bundle technique, the tibial tunnel is prepared.
Which of the following describes the correct anatomic trajectory of the PCL tibial guide pin to optimize footprint coverage while avoiding neurovascular injury?
Explanation
Question 75
A 60-year-old male undergoes arthroscopic rotator cuff repair.
To optimize tendon-to-bone healing, the surgeon decorticates the greater trochanter footprint. What is the primary histological mechanism of healing at the tendon-bone interface following this repair?
Explanation
Question 76
A 24-year-old rugby player falls with his foot plantar flexed and another player lands on his heel.
Radiographs suggest a subtle widening between the first and second rays. MRI confirms a complete tear of the Lisfranc ligament. He undergoes open reduction and internal fixation. Which specific articulation does the primary Lisfranc ligament span?
Explanation
Question 77
A 16-year-old female dancer experiences her first episode of acute lateral patellar dislocation. Radiographs show no osteochondral loose bodies. MRI confirms an isolated full-thickness tear of the medial patellofemoral ligament (MPFL).
What is the most common site of MPFL injury in an acute lateral patellar dislocation?
Explanation
Question 78
A 45-year-old construction worker with chronic anterior shoulder pain undergoes an open subpectoral biceps tenodesis.
During the surgical approach, retractors are placed deep to the short head of the biceps and coracobrachialis (conjoined tendon). Which nerve is at greatest risk of injury with overly aggressive medial retraction in this specific area?
Explanation
Question 79
A 20-year-old female ballet dancer presents with a palpable and audible "snap" over her deep anterior groin when she extends her hip from a flexed, abducted, and externally rotated position.
Dynamic ultrasound evaluation demonstrates a tendon snapping over a bony prominence. What is the most likely diagnosis?
Explanation
Question 80
A 30-year-old runner complains of lateral knee pain that is particularly worse when running downhill.
Examination reveals tenderness exquisitely localized over the lateral femoral epicondyle. Which clinical test is most specific for confirming the diagnosis of Iliotibial Band Friction Syndrome?
Explanation
Question 81
A 45-year-old male feels a pop in his posterior knee while squatting. MRI shows a medial meniscus posterior root tear. What is the primary biomechanical consequence of leaving this specific lesion untreated?
Explanation
Question 82
During an arthroscopic anterior cruciate ligament (ACL) reconstruction, the femoral tunnel is inadvertently placed too anteriorly within the intercondylar notch. What is the most likely clinical consequence during postoperative rehabilitation?
Explanation
Question 83
A 25-year-old football player presents with an acute knee injury. The Dial test demonstrates 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side, but symmetric external rotation at 90 degrees of flexion. What is the most likely injury pattern?
Explanation
Question 84
A 22-year-old rugby player suffers recurrent anterior shoulder instability. 3D CT reconstruction demonstrates 12% anterior glenoid bone loss and a deep, engaging Hill-Sachs lesion. Which of the following is the most appropriate surgical management?
Explanation
Question 85
When performing a medial patellofemoral ligament (MPFL) reconstruction, accurate placement of the femoral attachment is critical to prevent graft anisometry. Based on Schöttle's anatomic landmarks, where is the correct femoral footprint of the MPFL located?
Explanation
Question 86
A 19-year-old collegiate baseball pitcher undergoes a modified Jobe ulnar collateral ligament (UCL) reconstruction using a palmaris longus autograft. Which of the following represents the most common postoperative complication associated with this specific surgical technique?
Explanation
None
