Orthopedic Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
349 min read
89 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
The patient is treated by another physician and undergoes the procedure shown in Figures 40a and 40b. She currently cannot stand upright. Spinopelvic measurements reveal her pelvic incidence to be 85 degrees and pelvic tilt to be 40 degrees. Her lordosis from T12-S1 is 35 degrees. Which additional surgical procedure should be considered?
40A
B
40A
B

Explanation
- Single-level pedicle subtraction osteotomy
Question 2High Yield
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure.
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 3High Yield
-Premature arrest following growth plate injury is attributed to what mechanism?
Explanation
No detailed explanation provided for this question.
Question 4High Yield
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an

Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Question 5High Yield
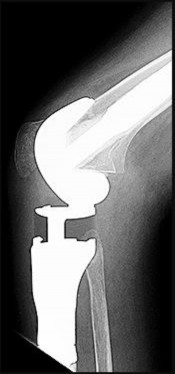
Figures 92a and 92b are the reconstruction radiographs of a 16-year-old boy with a high-grade conventional osteosarcoma of his right proximal tibia. He has completed neoadjuvant
chemotherapy. Wide resection, endoprosthetic proximal tibia replacement, a medial gastrocnemius flap, and a split-thickness skin graft were performed. The preferred postsurgical knee rehabilitation regimen is
chemotherapy. Wide resection, endoprosthetic proximal tibia replacement, a medial gastrocnemius flap, and a split-thickness skin graft were performed. The preferred postsurgical knee rehabilitation regimen is

Explanation
This patient underwent resection of the patellar tendon insertion onto the proximal tibia. The residual tendon is sutured to the prosthesis with augmentation of the repair by the medial gastrocnemius flap. Immobilization for 6 weeks in full extension is preferred to permit healing of the tendon repair and prevent patella alta with associated extensor lag. Cast, splint, or brace are all acceptable options for the initial immobilization. Risk for knee stiffness with such immobilization is low because all of the distal knee ligamentous and capsular attachments are transected with resection. Two weeks of immobilization may be adequate for flap and skin graft healing, but this amount of time is inadequate for patellar tendon healing. Continuous passive motion vs therapist-
directed range of motion has not been rigorously compared for proximal tibia replacement. Responses 1 and 2 include early motion.
RECOMMENDED READINGS
89. [Eckardt JJ, Matthews JG 2nd, Eilber FR. Endoprosthetic reconstruction after bone tumor resections of the proximal tibia. Orthop Clin North Am. 1991 Jan;22(1):149-60. PubMed PMID: 1992431. ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[View](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[ ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1992431)
90. [Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensor function after medial gastrocnemius flap reconstruction of the proximal tibia. Clin Orthop Relat Res. 2013 Jul;471(7):2333-9. doi: 10.1007/s11999-013-2851-8. Epub 2013 Feb 20. PubMed PMID: 23423620. ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23423620)
91. [Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013 Mar;107(4):335-42. doi: 10.1002/jso.23216. Epub 2012 Jul 17. PubMed PMID: 22806768. ](http://www.ncbi.nlm.nih.gov/pubmed/22806768)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22806768)
directed range of motion has not been rigorously compared for proximal tibia replacement. Responses 1 and 2 include early motion.
RECOMMENDED READINGS
89. [Eckardt JJ, Matthews JG 2nd, Eilber FR. Endoprosthetic reconstruction after bone tumor resections of the proximal tibia. Orthop Clin North Am. 1991 Jan;22(1):149-60. PubMed PMID: 1992431. ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[View](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[ ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1992431)
90. [Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensor function after medial gastrocnemius flap reconstruction of the proximal tibia. Clin Orthop Relat Res. 2013 Jul;471(7):2333-9. doi: 10.1007/s11999-013-2851-8. Epub 2013 Feb 20. PubMed PMID: 23423620. ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23423620)
91. [Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013 Mar;107(4):335-42. doi: 10.1002/jso.23216. Epub 2012 Jul 17. PubMed PMID: 22806768. ](http://www.ncbi.nlm.nih.gov/pubmed/22806768)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22806768)
Question 6High Yield
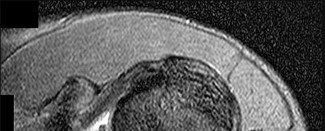
Figure 59 is the MR image of a 17-year-old high school wrestler who has had multiple subluxation episodes of his right shoulder. Physical therapy has not controlled his symptoms, and he was unable to finish the wrestling season because of pain and instability. CT scanning is suggested. What is the advantage of a CT scan?

Explanation
Most studies suggest that bone loss is most accurately imaged with a CT scan. Soft-tissue damage is more difficult to assess. Although the Goutallier classification for fatty infiltration is based on CT and not MR imaging findings, this is not relevant here. Multidirectional instability is a clinical, not imaging, diagnosis. CT’s substantial radiation dose can be especially harmful to young people
who presumably could live long enough to develop radiation-induced malignancies. Cost differences are minimal, and faster acquisition times are not clinically relevant. Breast and thyroid tissue exposure poses increased risk for radiation exposure for shoulder CT.
RECOMMENDED READINGS
4. [Jahnke AH Jr, Petersen SA, Neumann C, Steinbach L, Morgan F. A prospective comparison of computerized arthrotomography and magnetic resonance imaging of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):695-700; discussion 700-1. ](http://www.ncbi.nlm.nih.gov/pubmed/1456363)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1456363)
5. [Orchard JJ, Orchard JW, Grenfell T, Mitchell A. Ionising radiation: three game-changing studies for imaging in sports medicine. Br J Sports Med. 2014 Apr;48(8):677-8. doi: 10.1136/bjsports-2013-092499. Epub 2013 Jun 1. PubMed PMID: 23729176. ](http://www.ncbi.nlm.nih.gov/pubmed/23729176)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23729176)
6. [What are the Radiation Risks from CT? ](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)[http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)Rays/ucm115329.htm (Accessed August 25, 2016).
RESPONSES FOR QUESTIONS 60 THROUGH 66
1. Initial period of sling immobilization followed by physical therapy
2. Open reduction and internal fixation with or without bone grafting
3. Reverse total shoulder arthroplasty (rTSA)
4. Hemiarthroplasty
5. Unconstrained (TSA)
6. Closed reduction and Kirschner wire (K-wire) stabilization
Match the treatment listed above with the clinical scenario described below.
who presumably could live long enough to develop radiation-induced malignancies. Cost differences are minimal, and faster acquisition times are not clinically relevant. Breast and thyroid tissue exposure poses increased risk for radiation exposure for shoulder CT.
RECOMMENDED READINGS
4. [Jahnke AH Jr, Petersen SA, Neumann C, Steinbach L, Morgan F. A prospective comparison of computerized arthrotomography and magnetic resonance imaging of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):695-700; discussion 700-1. ](http://www.ncbi.nlm.nih.gov/pubmed/1456363)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1456363)
5. [Orchard JJ, Orchard JW, Grenfell T, Mitchell A. Ionising radiation: three game-changing studies for imaging in sports medicine. Br J Sports Med. 2014 Apr;48(8):677-8. doi: 10.1136/bjsports-2013-092499. Epub 2013 Jun 1. PubMed PMID: 23729176. ](http://www.ncbi.nlm.nih.gov/pubmed/23729176)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23729176)
6. [What are the Radiation Risks from CT? ](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)[http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)Rays/ucm115329.htm (Accessed August 25, 2016).
RESPONSES FOR QUESTIONS 60 THROUGH 66
1. Initial period of sling immobilization followed by physical therapy
2. Open reduction and internal fixation with or without bone grafting
3. Reverse total shoulder arthroplasty (rTSA)
4. Hemiarthroplasty
5. Unconstrained (TSA)
6. Closed reduction and Kirschner wire (K-wire) stabilization
Match the treatment listed above with the clinical scenario described below.
Question 7High Yield
Figure 58 is the CT scan of a 50-year-old man who has fallen from a height of 12 feet. He has a reported incomplete spinal cord injury. He is intubated and sedated prior to an examination. What are the likely neurological examination findings?

Explanation
This patient has sustained a fracture dislocation of his spine at T5. At this level of injury, the incident is unlikely to affect motor strength in the upper extremities, but it can affect motor function below T5. Sensation to the nipple line is typically at T4 and the umbilicus at T10. The absence of the bulbocavernosus reflex indicates spinal shock. Bulbocavernosus reflex refers to anal sphincter contraction in response to squeezing the glans penis or pulling on the Foley. Spinal shock usually resolves within 48 hours, and the return of the reflex signals termination of spinal shock. With this degree of fracture dislocation, it is unlikely that motor function is spared without sensation changes.
RECOMMENDED READINGS
5. [Ko HY, Ditunno JF Jr, Graziani V, Little JW. The pattern of reflex recovery during spinal shock. Spinal Cord. 1999 Jun;37(6):402-9. PubMed PMID: 10432259.](http://www.ncbi.nlm.nih.gov/pubmed/10432259)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432259)
6. [Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. doi: 10.1179/204577211X13207446293695. PubMed PMID: 22330108. ](http://www.ncbi.nlm.nih.gov/pubmed/22330108)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22330108)
7. American Spinal Injury Association Standards for neurological classification of spinal injured patients. Chicago, IL: ASIA; 1982.
RECOMMENDED READINGS
5. [Ko HY, Ditunno JF Jr, Graziani V, Little JW. The pattern of reflex recovery during spinal shock. Spinal Cord. 1999 Jun;37(6):402-9. PubMed PMID: 10432259.](http://www.ncbi.nlm.nih.gov/pubmed/10432259)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432259)
6. [Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. doi: 10.1179/204577211X13207446293695. PubMed PMID: 22330108. ](http://www.ncbi.nlm.nih.gov/pubmed/22330108)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22330108)
7. American Spinal Injury Association Standards for neurological classification of spinal injured patients. Chicago, IL: ASIA; 1982.
Question 8High Yield
Which of the following soft tissue tumors may cause tumor-induced osteomalacia:
Explanation
Tumor-induced osteomalacia can be caused by a small tumor of bone or soft tissue (phosphaturic tumor). Small tumors may not be detected.
I. General Features
A. Presentation
1/. C hronic, vague symptoms - principally, bone pain
2/. Muscle weakness
3/. Fractures may occur
B. Metabolic profile
1/. Hypophosphatemia
2/. Low reabsorption of phosphate from the kidney
3/. 1,25 dihydroxy vitamin D - low or normal
4/. 25 hydroxy vitamin D, 24,25 dihydroxy vitamin D - normal
C . Tumor types
1/. Soft tissue
a. Hemangiopericytoma b. Sclerosing angioma
c. Benign angiofibroma d. Neurofibromatosis
D. Pathophysiology
1/. A molecule that wastes phosphorus - phosphatonin
E. Radiographic features
1/. Osteopenia
2/. Pseudofractures
3/. C oarsened trabeculae
4/. Soft tissue - a small, well-circumscribed soft tissue mass may be noted
F. Treatment
1/. Oral phosphate
2/. 1,25 dihydroxy vitamin D Correct Answer: Hemangiopericytoma
I. General Features
A. Presentation
1/. C hronic, vague symptoms - principally, bone pain
2/. Muscle weakness
3/. Fractures may occur
B. Metabolic profile
1/. Hypophosphatemia
2/. Low reabsorption of phosphate from the kidney
3/. 1,25 dihydroxy vitamin D - low or normal
4/. 25 hydroxy vitamin D, 24,25 dihydroxy vitamin D - normal
C . Tumor types
1/. Soft tissue
a. Hemangiopericytoma b. Sclerosing angioma
c. Benign angiofibroma d. Neurofibromatosis
D. Pathophysiology
1/. A molecule that wastes phosphorus - phosphatonin
E. Radiographic features
1/. Osteopenia
2/. Pseudofractures
3/. C oarsened trabeculae
4/. Soft tissue - a small, well-circumscribed soft tissue mass may be noted
F. Treatment
1/. Oral phosphate
2/. 1,25 dihydroxy vitamin D Correct Answer: Hemangiopericytoma
Question 9High Yield
**ONLINE ORTHOPEDIC MCQS FOOT0 9**
**1**. Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?
**1**. Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?




Explanation
The patient has a failed Silastic implant. Nonsurgical management will not work at this point. A Keller resection will only exacerbate her metatarsalgia. Implant removal with structural bone grafting and MTP fusion is the most appropriate choice because restoration of length is needed to alleviate the forefoot pain and bone grafting is required to fuse the MTP joint because there is an abundance of osteolysis. Total toe implants do not offer good long-term outcomes and are very difficult to fit into the large exploded-out cavity of the proximal phalanx.**
**
**
Scientific References
- : Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.**
**Myerson MS, Schon LC, McGuigan FX, et al: Results of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.**
**2****. A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?
1- Transfer lesion to the fourth metatarsal head
2- Fifth toe fixed claw toe deformity
3- Ulceration at the level of the resected head
4- Peroneal atrophy
5- Charcot arthropathy with midfoot collapse and forefoot abduction
PREFERRED RESPONSE: 1**
**DISCUSSION: CMT is characterized by a cavovarus foot position that increases weight-bearing stresses along the lateral border. Removal of the fifth metatarsal head carries the risk of creating a transfer lesion at the fourth metatarsal head, particularly with a cavovarus foot. Claw toes are common in CMT, but the fifth toe would be flail in this situation. Ulceration is unlikely given the lack of underlying bone. Peroneal atrophy is associated with CMT but would not be a complication of this procedure. Charcot arthropathy is a neuropathic process frequently seen in individuals with diabetes mellitus.**
**REFERENCES: Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.**
**Coughlin MJ, Mann RA, Saltzman CL: Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 1312-1315.**
**3****. A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
1- Irrigation and debridement with immediate intramedullary fixation, vascular repair, and primary closure
2- Irrigation and debridement with external fixation, vascular repair, and delayed closure
3- Irrigation and debridement with external fixation, vascular repair, exploration of the tibial nerve, and delayed closure
4- Guillotine amputation at the fracture site with delayed closure
5- Immediate below-knee amputation
PREFERRED RESPONSE: 2**
**DISCUSSION: In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise.**
**REFERENCES: Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608.**
**Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208.**
**Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.**
**Baumgaertner MR, Tornetta P III (eds): Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 65-74.**
**4****. The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
1- Intrinsics overpowering a relatively weak extensor digitorum longus
2- Plantar plate overpowering a relatively weak extensor digitorum brevis
3- Lumbricals overpowering relatively weak intrinsics
4- Extensor digitorum longus overpowering relatively weak intrinsics
5- Extensor digitorum longus overpowering a relatively weak extensor digitorum brevis
PREFERRED RESPONSE: 4**
**DISCUSSION: The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe.**
**REFERENCES: Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints.
J Am Acad Orthop Surg 1995;3:166-173.**
**Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed. 7. St Louis, MO, Mosby, 1999,
pp 325-328.**
**5****. A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?
1- It may be difficult to obtain informed consent, even with an interpreter.
2- The husband may be unwilling to allow his wife to have the appropriate surgery.
3- Associated comorbidities in the patient increase the risk of surgical intervention.
4- There is the potential of not being able to obtain a satisfactory CT scan because
of claustrophobia.
5- Postsurgical care may be jeopardized by the patient’s role as caretaker for her children, thus compromising her ability to comply with weight-bearing restrictions.
PREFERRED RESPONSE: 5**
**DISCUSSION: With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.**
**REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**6****. A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?
1- No further treatment is advised unless a second ulcer develops
2- Oxford shoes with a rubber sole
3- Depth-inlay shoes with a custom accommodative foot orthosis
4- Dorsiflexion third metatarsal osteotomy
5- Achilles tendon lengthening
PREFERRED RESPONSE: 3**
**DISCUSSION: This is the first occurrence of diabetic foot-specific morbidity. The patient has a foot deformity, a history of a diabetic foot ulcer, and is insensate to the monofilament. He is at moderate risk for the development of a recurrent ulcer. This is best avoided with therapeutic footwear. Commercially available depth-inlay shoes should be combined with a custom accommodative foot orthosis to accommodative the deformity.**
**REFERENCES: Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.**
**Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.**
**7****. A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?
1- Ankle arthroscopy and lateral ligament reconstruction
2- Tendon transfer, lateral column lengthening, and heel cord lengthening
3- Ankle arthrodesis with retrograde intramedullary nail fixation
4- Calcaneal osteotomy and transverse tarsal osteotomy
5- Total ankle arthroplasty and deltoid ligament reefing
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal.**
**REFERENCES: Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.**
**Mäenpää H, Lehto MU, Belt EA: What went wrong in triple arthrodesis? An analysis of failures in 21 patients. Clin Orthop Relat Res 2001;391:218-223.**
**8****. If heel varus corrects with a Coleman block test, then the hindfoot deformity is flexible. This test proves that the varus is due to a
1- dorsiflexed first ray.
2- varus position of the forefoot.
3- plantar flexed first ray.
4- valgus hindfoot.
5- rigid flatfoot.
PREFERRED RESPONSE: 3**
**DISCUSSION: The Coleman block test is used to evaluate the effect of the forefoot on the rearfoot varus. If the deformity corrects with the block, then the hindfoot deformity is flexible and the varus position is secondary to the plantar flexed first ray or valgus position of the forefoot. A rearfoot orthotic will not correct the forefoot cause of the deformity. The patient still may need a lateralizing calcaneal osteotomy to realign the hindfoot.**
**REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.**
**Alexander IJ, Johnson KA: Assessment and management of pes cavus in Charcot-Marie-Tooth disease. Clin Orthop Relat Res 1989;246:273-281.**
**9****. A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?
1- Anterior tibialis tendon transfer to the dorsolateral midfoot
2- Posterior tibialis tendon transfer to the dorsolateral midfoot
3- Peroneus longus tendon transfer to the dorsolateral midfoot
4- Peroneus brevis tendon transfer to the dorsolateral midfoot
5- Flexor hallucis longus tendon transfer to the peroneus brevis
PREFERRED RESPONSE: 3**
**DISCUSSION: Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus. Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque.**
**REFERENCES: Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.**
**Vienne P, Schoniger R, Helmy N, et al: Hindfoot instability in cavovarus deformity: Static and dynamic balancing. Foot Ankle Int 2007;28:96-102.**
**10****. Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?
1- Posterior talofibular ligament
2- Distal tibiofibular syndesmosis
3- Anterior talofibular ligament
4- Deltoid ligament
5- Calcaneofibular ligament
PREFERRED RESPONSE: 4**
**DISCUSSION: In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used.**
**REFERENCES: Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398.**
**McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.**
**Schock HJ, Pinzur M, Manion L, et al: The use of the gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br 2007;89:1055-1059.**
**11****. A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
1- Nonunion
2- Deep infection
3- Delayed wound healing
4- Peroneal tendinitis
5- Posttraumatic arthritis
PREFERRED RESPONSE: 3**
**DISCUSSION: Delayed wound healing and wound dehiscence is the most common complication of surgical management of calcaneal fractures through an extensile lateral approach, occurring in up to 25% of patients. Most wounds ultimately heal with local treatment; the deep infection rate is approximately 1% to 4% in closed fractures. Posttraumatic arthritis may develop despite open reduction and internal fixation, but the percentages remain low. Peroneal tendinitis may occur from adhesions within the tendon sheath or from prominent hardware but is relatively uncommon. Nonunion of a calcaneal fracture is rare.**
**REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.**
**Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD,
Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.**
**12****. Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
1- MRI of the ankle
2- CT of the ankle
3- Technetium bone scan
4- Radiographs of the tibia and fibula
5- Repeat radiographs of the ankle in 5 to 7 days
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle.**
**REFERENCES: Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2,
pp 1973-2016.**
**Marsh JL, Saltzman CL: Ankle fractures, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2147-2247.**
**13****. A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
1- Fifth metatarsal head lateral ostectomy
2- Fifth metatarsal head excision
3- Metatarsal osteotomy and fifth metatarsal head ostectomy
4- Fifth metatarsal plantar condylectomy
5- Fifth metatarsophalangeal Silastic implant arthroplasty
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection.**
**REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.**
**Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.**
**14****. A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
1- Continued AFO bracing and therapy
2- Ankle fusion
3- Exploration and release of the common peroneal nerve
4- Transfer of the PTT through the interosseous membrane with attachment to the tibialis anterior and peroneus tertius above the level of the ankle, debridement of the anterior compartment, and Achilles tendon lengthening
5- Transfer of the peroneus longus to the dorsum of the foot and Achilles tendon lengthening
PREFERRED RESPONSE: 4**
**DISCUSSION: This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough. Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis.**
**REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192.**
**Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.**
**Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.**
**Williams PF: Restoration of muscle balance of the foot by transfer of the tibialis posterior. J Bone Joint Surg Br 1976;58:217-219.**
**15****. When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
1- Deltoid branch of the artery of the tarsal canal
2- Dorsalis pedis artery
3- Tarsal sinus artery
4- Perforating peroneal artery
5- Navicular artery
PREFERRED RESPONSE: 1**
**DISCUSSION: A Hawkins III fracture-dislocation generally presents with posteromedial displacement with the deltoid ligament intact. Therefore, the only remaining blood supply is the deltoid branch of the artery of the tarsal canal originating from the posterior tibial artery. Often, the medial malleolus is fractured, assisting in reduction and visualization of fracture reduction. If the medial malleolus is intact, a medial malleolus osteotomy allows visualization of the reduction without compromising the last remaining blood supply to the talus.**
**REFERENCES: Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.**
**Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.**
**16****. A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
1- Bone scan
2- Curettage and bone grafting of the cyst
3- Cast immobilization
4- Observation with reduced activity
5- Skeletal survey
PREFERRED RESPONSE: 4**
**DISCUSSION: The most likely diagnosis is Sever’s disease, which is considered either an apophysitis or a para-apophyseal stress fracture. It is common in athletic children and is associated with a tight Achilles tendon. Cast immobilization may be necessary if activity reduction fails. Calcaneal cysts are quite common and do not require any further diagnostic testing or treatment unless they occupy the full width of the calcaneus or one third of the length of the calcaneus.**
**REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.**
**Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.**
**17****. A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel’s sign is noted plantar medially and no Mulder’s click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?
1- Residual foreign body
2- Lateral plantar nerve laceration
3- Impingement of Baxter’s nerve
4- Interdigital neuroma
5- Digital nerve laceration
PREFERRED RESPONSE: 2**
**DISCUSSION: The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter’s nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel’s sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder’s click. A digital nerve laceration would exhibit isolated numbness more distally.**
**REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.**
**Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. Philadelphia, PA, JB Lippincott, 1983.**
**18****. A 69-year-old man reports pain over his bunion while wearing shoes and pain in the joint with push-off when barefoot. Nonsurgical management has failed to provide relief. Radiographs are shown in Figures 8a and 8b. What is the surgical procedure of choice?
1- First metatarsophalangeal arthrodesis
2- Distal chevron osteotomy and bunionectomy with closing wedge osteotomy and soft-tissue release
3- Bunionectomy with proximal metatarsal osteotomy
4- Bunionectomy with first metatarsal cuneiform fusion
5- Bunionectomy with proximal phalanx osteotomy and distal chevron osteotomy
PREFERRED RESPONSE: 1**
**DISCUSSION: Arthrodesis is indicated for severe bunion and hallux valgus deformities, but particularly with extensive degenerative disease of the first metatarsophalangeal joint. The other bunionectomy procedures have different indications, none of which include symptomatic first metatarsophalangeal degenerative disease.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 3-15.**
**Tourne Y, Saragaglia D, Zattara A, et al: Hallux valgus in the elderly: Metatarsophalangeal arthrodesis of the first ray. Foot Ankle Int 1997;18:195-198.**
**19****. A 65-year-old man has chronic Achilles insertional tendinitis that is refractory to nonsurgical management. A radiograph is shown in Figure 9. Preoperative counseling should include a discussion of the realistic duration of postoperative recovery. You should inform the patient that his expected recovery will last
1- 6 weeks.
2- 12 weeks.
3- 3 to 6 months.
4- 9 months.
5- 12 months.
PREFERRED RESPONSE: 5**
**DISCUSSION: An older patient with calcaneal enthesopathy may take a year or more to recover after tendon debridement and calcaneal ostectomy. Young patients, and those with purely tendon pathology, may recover more quickly.**
**REFERENCES: McGarvey WC, Palumbo RC, Baxter DE, et al: Insertional Achilles tendinitis: Surgical treatment through a central tendon splitting approach. Foot Ankle Int 2002;23:19-25.**
**Watson AD, Anderson RB, Davis WH: Comparison of results of retrocalcaneal decompression for retrocalcaneal bursitis and insertional Achilles tendinosis with calcific spur. Foot Ankle Int 2000;21:638-642.**
**20****. Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion.
If excisional biopsy is performed, what is the most likely complication?
1- Metastatic spread
2- Recurrence of the lesion
3- High likelihood of wound breakdown
4- Injury to the medial plantar nerve
5- Loss of the local windlass effect of the plantar fascia
PREFERRED RESPONSE: 2**
**DISCUSSION: The MRI scan shows plantar fibromatosis. The treatment is usually nonsurgical.
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.**
**REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.**
**Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.**
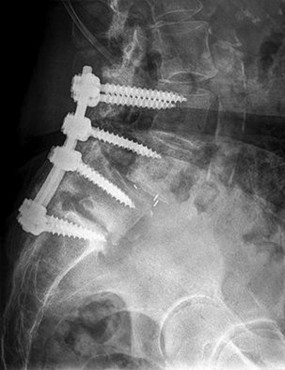
**21****. A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?
1- Late rotatory deformity
2- Limb-length discrepancy
3- Talar osteonecrosis
4- Tibial stress fracture
5- Hardware failure
PREFERRED RESPONSE: 4**
**DISCUSSION: The interlocking screws at the proximal end of the rod can act as a stress riser and lead to fracture. Postoperative pain at this level should prompt inclusion of this diagnosis in the differential. Removing the screws following bone union can decrease the chances of this occurring. A short rod that avoids the diaphyseal area may also be beneficial. Rotatory deformity is controlled by the perpendicularly oriented distal transfixion screws. Talar osteonecrosis would be unusual since the dissection can be minimized with an intramedullary rod. Any type of hardware can fail if the construct does not lead to a solid arthrodesis.**
**REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237.**
**Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.**
**Hammett R, Hepple S, Forster B, et al: Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail: The results of 52 procedures. Foot Ankle Int 2005;26:810-815.**
**22****. A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
1- Short leg cast for 6 weeks
2- Splinting with early range of motion at 3 weeks
3- Immediate open reduction and internal fixation through a medial approach
4- Delayed open reduction and internal fixation
5- Fusion
PREFERRED RESPONSE: 4**
**DISCUSSION: Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended.**
**REFERENCES: Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264.**
**Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.**
**Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
23/. A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?
1- Gadolinium-enhanced MRI of the great toe
2- Serum uric acid level, C-reactive protein, and erythrocyte sedimentation rate
3- Serum rheumatoid factor
4- Aspiration of the first metatarsophalangeal joint
5- Fasting serum glucose level
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has gouty arthropathy of the first metatarsophalangeal joint. This definitive diagnosis is achieved with aspiration of the joint and polarized light microscopy that shows needle-shaped negatively birefringent monosodium urate crystals. Differential diagnoses of infectious arthritis and pseudogout are also definitively made through joint aspiration. Although rheumatoid arthritis is a possibility, a serum rheumatoid factor is not always diagnostic and a patient with rheumatoid arthritis may have concomitant gouty arthritis. The radiographic findings are not typical of diabetes mellitus or of a patient with Charcot arthropathy.**
**REFERENCES: Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.**
**Harris MD, Siegel LB, Alloway JA: Gout and hyperuricemia. Am Fam Physician 1999;59:925-934.**
**24****. Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the
best treatment?
1- Moist dressings and continued observation
2- Debridement of the necrotic tissue
3- Amputation at the metatarsophalangeal level with open wound management
4- Closed forefoot amputation
5- Guillotine transtibial amputation
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement.**
**REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.**
**Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.**
**25****. The peroneus tertius is a commonly used landmark for arthroscopic portal placement.
What is the function of this tendon?
1- Dorsiflexion
2- Eversion
3- Dorsiflexion and eversion
4- Fifth toe extension
5- Lesser toe extension
PREFERRED RESPONSE: 3**
**DISCUSSION: The peroneus tertius, although absent in 10% of the population, originates on the distal third of the extensor surface of the fibula and inserts onto the base of the fifth metatarsal, possibly extending to the fascia over the fourth interosseous space. The muscle is located in the anterior compartment of the leg and is innervated by the deep peroneal nerve. The tendon produces dorsiflexion and eversion when walking and can be used as an insertion point during tendon transfers to assist dorsiflexion. This tendon is peculiar to humans and is a proximally migrated deep extensor of the fifth toe.**
**REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.**
**Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.**
**Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.**
**26****. A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?
1- Triple antibiotic coverage
2- Transfer to the ICU and a consult with infectious disease
3- Urgent irrigation and debridement with gentle skin closure
4- Urgent hyperbaric oxygen treatments and immunoglobulin
5- Urgent aggressive debridement of skin, subcutaneous fat, and fascia
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used
after surgery.**
**REFERENCES: Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.**
**Ozalay M, Ozkoc G, Akpinar S, et al: Necrotizing soft-tissue infection of a limb: Clinical presentation and factors related to mortality. Foot Ankle Int 2006;27:598-605.**
**27****. A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?
1- Dorsiflexion osteotomy of the first metatarsal
2- Dorsiflexion osteotomy of the first metatarsal combined with anterior transfer of the tibialis posterior
3- Triplanar osteotomy at the apex of the deformity
4- Triplanar osteotomy at the apex of the deformity combined with valgus calcaneal osteotomy
5- Triplanar osteotomy at the apex of the deformity combined with anterior transfer of the tibialis posterior
PREFERRED RESPONSE: 1**
**DISCUSSION: This deformity is early in the disease process. The foot is still flexible, as evidenced by correction with the Coleman block test. A simple dorsiflexion osteotomy of the first metatarsal should provide a plantigrade foot. More complex osteotomies are required later in the disease process when the foot is not flexible and the deformity does not correct with the Coleman block test. The patient may also require a tibialis anterior transfer later in the disease process but not at the present time.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.**
**Dehne R: Congenital and acquired neurologic disorders, in Coughlan MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 525-557.
28/. A 58-year-old man with type 1 diabetes mellitus is seen in the emergency department and he reports a 3-day history of a red swollen foot but no history of trauma. Examination reveals that the skin is intact, and the patient has discomfort with passive range of motion at the ankle, hindfoot, and midfoot joints. He denies any fever. Laboratory studies show a WBC count of 7,800/mm3, an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 23, and a serum glucose of 100. A radiograph and MRI scans are shown in Figures 16a through 16c. What is the next most appropriate step in management?
1- Technetium Tc 99m triple phase bone scan
2- Admit for elevation, observation, and IV antibiotics
3- Total contact casting, no weight bearing, and weekly cast changes until erythema and swelling is decreased
4- Immediate stabilization of the talus and midfoot with internal fixation and postoperative splinting, no weight bearing, and total contact casting
5- Total contact casting, weight bearing as tolerated, with weekly cast changes
PREFERRED RESPONSE: 3**
**DISCUSSION: Whereas it is difficult to distinguish between cellulitis, septic joint, osteomyelitis, and early Eichenholtz stage 1 Charcot, the presence of a fracture in the absence of ulcerations with a normal WBC count and serum glucose strongly indicates that the described symptoms are due to an early Charcot process alone. A technetium Tc 99m scan alone would not be helpful; however, the addition of a sulfur colloid marrow scan or indium In 111 scan may be more specific to rule out infection, though it is not warranted here. Total contact casting with non-weight-bearing or limited weight bearing during Eichenholtz stage 1 when the foot is warm, erythematous, and swollen is advised to help prevent deformity. Alternatively, stabilization with pneumatic bracing may also be considered. While some authors have proposed early fixation or arthrodesis for Eichenholtz stage 1, the gold standard is still total contact casting with no to limited weight bearing until the swelling resolves and evidence of consolidation is seen on radiographs.**
**REFERENCES: Trepman E, Nihal A, Pinzur MS: Current topics review: Charcot neuropathy of the foot and ankle. Foot Ankle Int 2005;26:46-63.**
**Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 123-134.**
**Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.**
**29****. Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?
1- Fluoroquinolone antibiotics
2- Diabetes mellitus
3- Obesity
4- Steroid exposure
5- Estrogen deficiency
PREFERRED RESPONSE: 5**
**DISCUSSION: Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy.**
**REFERENCES: Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.**
**Holmes GB, Mann RA, Well L: Epidemiological factors associated with rupture of the Achilles tendon. Contemp Orthop 1991;23:327-331.**
**30****. Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and
1- removal of the extruded talus and placement of an external fixator.
2- immediate tibiocalcaneal fusion.
3- reimplantation of the talus, external fixation, and/or open reduction and internal fixation of the talar neck fracture.
4- reimplantation followed by primary tibiotalar arthrodesis.
5- Syme amputation.
PREFERRED RESPONSE: 3**
**DISCUSSION: The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation,
7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure.**
**REFERENCES: Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.**
**Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.**
**Marsh JL, Saltzman CL, Iverson M, et al: Major open injuries of the talus. J Orthop Trauma 1995;9:371-376.**
**31****. Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate
the symptoms?
1- Neutral posted rigid custom foot orthosis
2- Custom rigid UCBL foot orthosis
3- Ankle-foot orthosis with the ankle locked at 90 degrees
4- Shoe modification with a cushioned heel and rocker sole
5- Metal hinged/leather short ankle “Arizona” orthosis
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a malunion of an attempted open reduction of a Lisfranc dislocation. The pain occurs during the terminal stance phase of gait as load is being transferred from the hindfoot to the forefoot. The bending moment can be best neutralized with shoe modification with a cushioned heel and rocker sole, which best unloads the tarsal-metatarsal junction.**
**REFERENCES: Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.**
**Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.**
**32****. An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
1- Gradual return to play
2- Physical therapy program
3- Custom orthosis
4- Non-weight-bearing cast
5- Weight-bearing AP radiograph
PREFERRED RESPONSE: 5**
**DISCUSSION: Differentiating between a midfoot sprain and Lisfranc diastasis is critical in the management of the athlete with an acute injury to the midfoot. Greater than 2 mm of displacement between the first and second metatarsals on a weight-bearing radiograph is an indication for anatomic reduction with internal fixation of the tarsometatarsal joints. If no subluxation is noted, treatment should consist of a non-weight-bearing cast for 6 weeks, followed by a gradual return
to activity.**
**REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.**
**Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.**
**33****. A 36-year-old woman is wearing an ankle-foot orthosis for a foot drop secondary to spastic hemiplegia following a postpartum stroke 2 years ago. Knee and hip motion and strength are within normal ranges. She has undergone multiple rounds of physical therapy but has seen no improvement over the past several months. No improvement has been recorded by electromyography (EMG) studies over the past year. Examination reveals a 5-degree plantar flexion contracture with clonus, heel varus, and compensatory knee hyperextension when standing. She has 4/5 power in the tibialis anterior and gastrocnemius soleus complex with resistance testing. Everters are 2/5 to resistance testing. EMG gait studies show that the tibialis anterior demonstrates activity during both swing and stance phase that is increased during swing phase. Premature firing of the triceps surae is noted when positioning the foot in equinus prior to floor contact. What is the most appropriate management?
1- Percutaneous Achilles tendon lengthening
2- Percutaneous Achilles tendon lengthening and split tibialis anterior transfer to the lateral cuneiform
3- Percutaneous Achilles tendon lengthening and interosseous posterior tibialis tendon transfer to the peroneus tertius
4- Percutaneous Achilles tendon lengthening and tenotomy of the long toe flexor tendons
5- Percutaneous Achilles tendon lengthening, tenotomy of the long toe flexors, and Bridle procedure
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has a dynamic varus deformity secondary to spasticity of the tibialis anterior during stance phase with inverter/everter imbalance. The patient still has active motion of the tibialis anterior; therefore, an out-of-phase posterior tibial tendon transfer should not be performed. The same is true of the Bridle procedure. Transfer of the posterior tibialis in this patient may also result in subsequent planovalgus deformity. Lengthening of the Achilles tendon through a percutaneous tenotomy will restore dorsiflexion and decrease clonus from the stretch response. If adequate dorsiflexion is not obtained intraoperatively, then posterior tibialis tendon lengthening may be considered. A split tibialis anterior tendon transfer to the lateral cuneiform, or, transfer of the entire tendon to the cuneiform should correct the varus component and compensate for the weakened peroneals.**
**REFERENCES: Yamamoto H, Okumura S, Morita S, et al: Surgical correction of foot deformities after stroke. Clin Orthop Relat Res 1992;282:213-218.**
**Piazza SJ, Adamson RL, Moran MF, et al: Effects on tensioning errors in split transfers of tibialis anterior and posterior tendons. J Bone Joint Surg Am 2003;85:858-865.**
**Morita S, Muneta T, Yamamoto H, et al: Tendon transfers for equinovarus deformed foot caused by cerebrovascular disease. Clin Orthop Relat Res 1998;350:166-173.**
**34****. A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?
1- CT scan
2- Repeat period of immobilization
3- Referral to pain management for sympathetic blocks
4- Continued observation and physical therapy
5- Acupuncture
PREFERRED RESPONSE: 1**
**DISCUSSION: Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit.**
**REFERENCES: Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.**
**Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 182-183.**
**35****. What is the most frequent complication of percutaneous repair of an acute Achilles tendon rupture?
1- Sural nerve entrapment
2- Re-rupture
3- Infection
4- Suture granuloma
5- Wound healing complications
PREFERRED RESPONSE: 1**
**DISCUSSION: Sural nerve entrapment is the major risk of percutaneous repair. A small mini-open technique with a suture guide can obviate that issue. Re-rupture rates after surgical repair are approximately 3%. Infection and wound problems are rarely encountered with percutaneous repair; they are issues with open repair.**
**REFERENCES: Aracil J, Pina A, Lozano JA, et al: Percutaneous suture of Achilles tendon ruptures. Foot Ankle 1992;13:350-351.**
**Sutherland A, Maffulli N: A modified technique of percutaneous repair of the ruptured Achilles tendon. Oper Orthop Traumatol 1998;10:50-58.**
**Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am
2002;84:161-170.**
**36****. A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?
1- Observation as the deformity should resolve in time
2- Wearing of straight last shoes
3- Serial stretching and casting for the next 6 to 12 weeks
4- Heyman, Herndon, and Strong capsular release at the tarsometatarsal and intermetatarsal joints
5- Berman and Gartland dome-shaped osteotomies of the metatarsal bases
PREFERRED RESPONSE: 3**
**DISCUSSION: Weinstein reported on 31 patients (45 feet) with congenital metatarsus adductus followed for an average of 33 years. Twenty-nine feet had moderate to severe deformities treated with manipulation and casting with a 90% success rate. In a young child, surgery is not indicated until nonsurgical management has failed. In patients 2 to 4 years of age, tarsometatarsal capsulotomies are indicated, whereas multiple metatarsal osteotomies are reserved for recalcitrant deformities in children older than 4 years of age. Mild or moderate metatarsus adductus that is passively correctable will resolve without treatment.**
**REFERENCES: Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988.**
**Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus.
J Pediatr Orthop 1999;19:49-50.**
**Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes
of treatment. J Bone Joint Surg Am 2000;82:980-990.**
**37****. A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?
1- Ankle arthrodesis
2- Subtalar arthrodesis
3- Pantalar arthrodesis
4- Posterior tibialis tendon transfer to the lateral midfoot with Achilles tendon lengthening
5- Split anterior tibialis tendon transfer to the lateral midfoot with Achilles tendon lengthening
PREFERRED RESPONSE: 4**
**DISCUSSION: Arthrodesis of any of the ankle or hindfoot joints should be reserved for fixed deformities or end-stage degenerative arthritis. Achilles tendon lengthening is necessary to correct the equinus and to improve dorsiflexion-plantar flexion balance. Similarly, transfer of the posterior tibialis tendon reduces both plantar flexion and inversion torque.**
**REFERENCES: Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.**
**Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.**
**38****. Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?
1- Decreased risk of posttraumatic arthritis
2- Avoid growth arrest
3- Minimize risk of osteonecrosis
4- Prevent clinical internal rotation deformity
5- Prevent development of a late tarsal tunnel syndrome
PREFERRED RESPONSE: 1**
**DISCUSSION: Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis.**
**REFERENCES: Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.**
**Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.**
**Spiegel PG, Mast JW, Cooperman DR, et al: Triplane fractures of the distal tibial epiphysis.
Clin Orthop Relat Res 1984;188:74-89.**
**39****. A 75-year-old woman reports foot pain and states that her foot has become progressively “flatter” in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?
1- Posterior tibial tendon debridement and synovectomy
2- Tendon transfer, spring ligament repair, and heel cord lengthening
3- Tendon transfer, lateral column lengthening, and heel cord lengthening
4- Realignment triple arthrodesis and heel cord lengthening
5- Medial column arthrodesis and heel cord lengthening
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has end-stage midfoot arthritis, with a secondary flatfoot deformity through the midfoot. The ability to perform a single limb heel rise indicates that the posterior tibial tendon is functioning, and the weight-bearing radiographs show normal calcaneal pitch and talar head coverage, thus confirming that the flatfoot deformity is isolated to the midfoot. Therefore, the most appropriate treatment is medial column arthrodesis and heel cord lengthening. The other listed procedures are not indicated because they are used in the management of adult flatfoot from posterior tibial tendon insufficiency.**
**REFERENCES: Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.**
**Horton GA, Olney BW: Deformity correction and arthrodesis of the midfoot with a medial plate. Foot Ankle 1993;14:493-499.**
**40****. A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?
1- First metatarsophalangeal arthrodesis
2- Soft-tissue interposition arthroplasty
3- First metatarsophalangeal total joint arthroplasty
4- First metatarsophalangeal resurfacing hemiarthroplasty
5- Proximal phalanx dorsiflexion osteotomy (Moberg)
PREFERRED RESPONSE: 1**
**DISCUSSION: All but the Moberg osteotomy are capable of providing pain relief; however, arthrodesis offers the best long-term results and restores weight bearing and propulsion function to the first ray.**
**REFERENCES: Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.**
**Myerson MS, Schon LC, McGuigan FX, et al: Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.**
**41****. During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
1- Posterior heel
2- Plantar-lateral foot
3- Plantar-medial foot
4- Dorso-lateral foot
5- Dorso-medial foot
PREFERRED RESPONSE: 4**
**DISCUSSION: The sural nerve runs with the small saphenous vein on the posterior leg just lateral to the Achilles tendon. It is formed by contributions from both the tibial and common peroneal nerves and provides sensation on the dorso-lateral aspect of the foot.**
**REFERENCES: Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.**
**Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.**
**42****. A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
1- Talectomy
2- Revision open reduction and internal fixation (ORIF) with bone grafting
3- Ankle arthrodesis
4- Tibiotalocalcaneal arthrodesis
5- Triple arthrodesis
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case.**
**REFERENCES: Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction.
Foot Ankle Clin 2007;12:137-151.**
**Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.**
**43****. What type of physical therapy is most effective for chronic noninsertional Achilles tendinopathy?
1- Stair climbing
2- Eccentric strengthening
3- Concentric strengthening
4- Isometric strengthening
5- Rope jumping
PREFERRED RESPONSE: 2**
**DISCUSSION: Eccentric gastrocsoleus strengthening (especially with heavy loads) consistently has been shown to be superior in the management of Achilles tendinopathy. Decreases in pain and increases in strength have been demonstrated despite the frequently refractory nature of this condition.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 91-102.**
**Vora AM, Myerson MS, Oliva F, et al: Tendinopathy of the main body of the Achilles tendon.
Foot Ankle Clin 2005;10:293-308.**
**44****. A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
1- Physical therapy and bracing
2- Reassurance that the deformity will resolve with time
3- Achilles tendon lengthening, and release or retromalleolar lengthening of the flexor digitorum longus (FDL) and flexor hallucis longus (FHL)
4- FDL and FHL tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot
5- FDL and FHL tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion
PREFERRED RESPONSE: 3**
**DISCUSSION: This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated.**
**REFERENCES: Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.**
**Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.**
**45****. A 24-year-old man reports the development of a foot drop following a knee dislocation
1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
1- Repeat neurolysis of the common peroneal nerve at the knee level
2- Repeat neurolysis of the common peroneal nerve with cable grafting
3- Extensor hallucis longus transfer to the distal first metatarsal
4- Anterior transfer of the tibialis posterior tendon through the interosseous membrane
5- Ankle fusion
PREFERRED RESPONSE: 4**
**DISCUSSION: The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients. Successful ankle fusion is likely to fail with time due to the development of forefoot equinus.**
**REFERENCES: Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.**
**Lipscomb P, Sanchez J: Anterior transplantation of the posterior tibial tendon for persistant palsy of the common peroneal nerve. J Bone Joint Surg Am 1961;43:60-66.**
**46****. A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
1- Quicker return to activities
2- Quicker return to work
3- Increased subtalar joint range of motion
4- Decreased risk of nonunion
5- Decreased risk of posttraumatic arthritis
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method.**
**REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.**
**Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.**
**47****. A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
1- Subtalar fusion
2- Posterior tibial tendon transfer to the cuboid
3- Split posterior tibial tendon transfer to the lateral cuneiform
4- Flexor digitorum longus transfer to the fifth metatarsal
5- Excision of both the peroneus longus and brevis
PREFERRED RESPONSE: 4**
**DISCUSSION: A flexor digitorum longus transfer, while not as strong as the peroneals, improves the tendon balance and maintains hindfoot mobility. Subtalar fusion is a salvage procedure. Posterior tibial tendon transfer compromises inversion strength and arch height. Functional absence of the peroneals results in an imbalance that could lead to forefoot varus.**
**REFERENCES: Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.**
**Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.**
**48****. Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?
1- Radiograph
2- CT
3- MRI
4- Ultrasound
5- Bone scan
PREFERRED RESPONSE: 4**
**DISCUSSION: Ultrasound is best at imaging abrupt changes in the density of adjacent tissue and therefore is best at imaging wood in the soft tissues of the foot.**
**REFERENCES: Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.**
**Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.**
**49****. A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
1- surface irrigation, sterile dressing, and a short leg cast.
2- surface irrigation, sterile dressing, a short leg cast, and oral antibiotics.
3- surface irrigation, sterile dressing, a short leg cast, and IV antibiotics.
4- surgical debridement, a short leg cast, and IV antibiotics.
5- surgical debridement, external or internal fixation, and IV antibiotics.
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean.**
**REFERENCES: Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res
2003;408:86-91.**
**Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.**
**50****. What is the most frequent location of entrapment of the deep peroneal nerve?
1- Tendon of the extensor hallucis brevis
2- Inferior extensor retinaculum
3- Osteophytes of the talonavicular joint
4- Os intermetatarseum
5- Base of the fifth metatarsal
PREFERRED RESPONSE: 2**
**DISCUSSION: The most frequently described entrapment of the deep peroneal nerve is the anterior tarsal tunnel syndrome. This syndrome refers to entrapment of the deep peroneal nerve under the inferior extensor retinaculum. Entrapment can also occur as the nerve passes under the tendon of the extensor hallucis brevis. Compression by underlying dorsal osteophytes of the talonavicular joint and an os intermetatarseum (between the bases of the first and second metatarsals) have previously been described in runners.**
**REFERENCES: Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.**
**Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.**
**51****. What is the most common malignant tumor of the foot?
1- Chondrosarcoma
2- Synovial sarcoma
3- Osteosarcoma
4- Clear cell sarcoma
5- Melanoma
PREFERRED RESPONSE: 5**
**DISCUSSION: Whereas chondrosarcoma is the most frequently occurring malignant bone tumor of the foot and synovial sarcoma is the most common soft-tissue foot malignancy, the most common malignant tumor overall is melanoma. It constitutes approximately 25% of lesions found on the lower extremity. Furthermore, 31% of all melanomas arise in the foot.**
**REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.**
**Bos GD, Ester RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.**
**52****. A 40-year-old man underwent an ankle arthroscopy 6 months ago for a talus osteochondral defect. He continues to have pain and burning on the lateral portal but states that the pain is now more superficial than his original pain. Examination reveals that he has shooting pain to his medial foot and ankle when his lateral portal is tapped. A previous injection around the lateral portal gave him relief for about 2 weeks. What treatment will best eliminate his pain?
1- Neuroplasty of the sural nerve
2- Neuroplasty or excision and burial of the deep peroneal nerve
3- Neuroplasty or excision and burial of the medial branch of the superficial peroneal nerve
4- Repeat arthroscopy for worsening of the talus osteochondral defect
5- Anaesthetic skin patches
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient clearly has entrapment of the superficial peroneal nerve in the lateral portal. It is most likely only the medial branch by examination. If the nerve is in good condition, it can simply be released. If the nerve is cut or severely thinned, it is better excised and buried. The sural nerve most likely would be caught in a posterior-lateral portal.**
**REFERENCES: Jobe MT, Wright PE: Peripheral nerve injuries, in Canale ST (ed): Campbell’s Operative Orthopaedics. St Louis, MO, Mosby, 1998, pp 3839-3844.**
**Saito A, Kikuchi S: Anatomic relations between ankle arthroscopic portal sites and the superficial peroneal and saphenous nerves. Foot Ankle Int 1998;19:748-752.**
**53****. When performing a Weil osteotomy of a lesser metatarsal, the desired angle of the saw cut should be approximately
1- perpendicular to the shaft of the metatarsal.
2- parallel with the inclination of the metatarsal.
3- parallel with the plantar surface of the foot.
4- 45 degrees to the shaft of the metatarsal.
5- 10 degrees to the shaft of the metatarsal.
PREFERRED RESPONSE: 3**
**DISCUSSION: Appropriate orientation of the saw cut when performing a Weil osteotomy is approximately parallel with the plantar surface of the foot. This is done in an effort to minimize plantar displacement of the capital fragment. The removal of additional bone from the osteotomy site either by removing a separate wafer of bone or using a thicker saw blade has also been described to minimize plantar displacement of the distal fragment.**
**REFERENCES: Trnka H, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.**
**Grimes J, Coughlin M: Geometric analysis of the Weil osteotomy. Foot Ankle Int 2006;27:985-992.**
**54****. A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other
foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
1- Snug fitting shoe to block side-to-side motion that is common after this procedure
2- Leather sole shoe to prevent catching the shoe on carpet which is common with crepe-soled shoes
3- Lateral wedge on the shoe to offset the external rotation during the toe-off phase of gait commonly seen after this procedure
4- Steel shank to extend the foot lever and prevent deformity at the toe break
5- Custom-made shoe to provide the best possible fit and function
PREFERRED RESPONSE: 4**
**DISCUSSION: The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but “snug” fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem.**
**REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.**
**Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.**
**55****. A 32-year-old laborer reports left ankle pain and deformity. History reveals that he
sustained a left ankle fracture 2 years ago and was treated with closed reduction and
casting. Radiographs are shown in Figures 25a through 25c. What is the most
appropriate management?
1- Bracing and physical therapy
2- Intra-articular injection of steroids into the ankle joint, bracing, and physical therapy
3- Intra-articular injection of hyaluronic acid product into the ankle joint, bracing, and physical therapy
4- Ankle fusion
5- Corrective osteotomy of the fibula and medial malleolus with reconstruction of the syndesmosis if unstable
PREFERRED RESPONSE: 5**
**DISCUSSION: Corrective osteotomy of fibular malunions, with appropriate lengthening, even in the presence of early arthritis, has been shown to decrease ankle pain and increase stability. Reduction and bone grafting of the medial malleolar nonunion is also needed. There is no evidence supporting the use of intra-articular steroids or hyaluronic acid in the ankle joint. Lateral talar displacement of even 1 mm has been reproducibly shown to decrease tibiotalar contact by 40% to 42%, causing a predisposition to arthritis.**
**REFERENCES: Weber D, Friederich NF, Muller W: Lengthening osteotomy of the fibula for post-traumatic malunion: Indication, technique and results. Int Orthop 1998;22:149-152.**
**Lloyd J, Elsayed S, Hariharan K, et al: Revisiting the concept of talar shift in ankle fractures. Foot Ankle Int 2006;27:793-796.**
**Offierski CM, Graham JD, Hall JH, et al: Later revision of fibular malunion in ankle fractures. Clin Orthop Relat Res 1982;171:145-149.**
**Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.**
**56****. Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
1- Flexor hallucis longus tendon
2- Flexor hallucis brevis tendon
3- Abductor hallucis tendon
4- Adductor hallucis tendon
5- Extensor hallucis brevis tendon
PREFERRED RESPONSE: 2**
**DISCUSSION: Complications of medial sesamoidectomy include stiffness, claw toe, and hallux valgus. Each sesamoid sits within its respective head of the flexor hallucis brevis tendon. Excision of one sesamoid can result in slack in its flexor hallucis brevis tendon; therefore, it is imperative to preserve or repair the flexor hallucis brevis tendon when removing the medial sesamoid.**
**REFERENCES: Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.**
**Lee S, James WC, Cohen BE, et al: Evaluation of hallux alignment and functional outcome after isolated tibial sesamoidectomy. Foot Ankle Int 2005;26:803-809.**
**57****. In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
1- Relatively young, active patient
2- Patient with an inflammatory systemic disorder
3- Elderly patient with a sedentary lifestyle
4- Patient with severe arthritis of the ipsilateral hip or knee
5- Patient with Parkinson’s disease
PREFERRED RESPONSE: 3**
**DISCUSSION: Most authors recommend an initial trial of nonsurgical management in the treatment of adult-acquired flatfoot deformity such as posterior tibial tendon dysfunction. Chao and associates found that there is high patient satisfaction with ankle-foot orthoses and UCBL-type inserts in elderly patients with a relatively sedentary lifestyle. Alternatively, there was a higher dissatisfaction rate in young active patients, those with balance and ambulation difficulties (Parkinson’s, severe arthritis of the hip or knee), and patients with inflammatory systemic disorders.**
**REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.**
**Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.**
**58****. Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?
1- Avoid wearing the prosthesis until the ulcer is healed and perform local wound care.
2- Obtain a new prosthesis with an energy-storing foot to dampen impact.
3- Perform local wound care in conjunction with modification of the prosthetic socket and cushioned liner.
4- Excise the wound and advance the soft-tissue envelope.
5- Perform a distal tibiofibular bone bridge and advance the soft-tissue envelope.
PREFERRED RESPONSE: 3**
**DISCUSSION: The first step in the treatment of an amputation residual limb (stump) ulcer is local wound care and adjustment of the residual limb-prosthetic interface, as well as adjusting prosthetic alignment. Surgical revision should be undertaken only when prosthetic modification is unsuccessful.**
**REFERENCES: Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.**
**Smith DG, Ferguson JR: Transtibial amputations. Clin Orthop Relat Res 1999;361:108-115.**
**59****. The spring ligament of the foot connects what two bones?
1- Tibia and talus
2- Talus and navicular
3- Talus and calcaneus
4- Calcaneus and cuboid
5- Calcaneus and navicular
PREFERRED RESPONSE: 5**
**DISCUSSION: The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot.**
**REFERENCES: Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.**
**Davis WH, Sobel M, DiCarlo EF, et al: Gross, histological and microvascular anatomy and biomechanical testing of the spring ligament complex. Foot Ankle Int 1996;17:95-102.**
**60****. An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a
3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?
1- Exostectomy
2- Lateral column lengthening
3- Medial slide calcaneal osteotomy
4- Talonavicular arthrodesis
5- Triple arthrodesis
PREFERRED RESPONSE: 5**
**DISCUSSION: The deformity is long-standing, the hindfoot is immobile, and the radiographs reveal severe degenerative arthritis involving the entire hindfoot, severe deformity, and talonavicular dislocation. The “exostosis” responsible for the callus is the talar head; resection would severely destabilize the foot. Degenerative arthritis and fixed deformity preclude lateral column lengthening, medial slide calcaneal osteotomy, and talonavicular arthrodesis. Triple arthrodesis is the only viable option.**
**REFERENCES: Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.**
**Pinney SJ, Lin SS: Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.**
**61****. A 20-year-old collegiate football player sustains an injury to his left foot 3 weeks before the start of the fall season. Examination reveals localized tenderness over the lateral midfoot and normal foot alignment. Radiographs are shown in Figures 28a through 28c. What is the treatment of choice?
1- Intramedullary screw fixation
2- Onlay bone graft
3- Application of a walking boot with weight bearing as tolerated
4- Application of a short leg cast with weight bearing as tolerated
5- Application of a short leg cast and non-weight-bearing
PREFERRED RESPONSE: 1**
**DISCUSSION: Due to the relatively high incidence of delayed union and nonunion associated with this mildly displaced Jones-type fracture, and the temporal proximity to his playing season, intramedullary screw fixation is the treatment of choice in this collegiate athlete to best ensure healing and expedite his return to football. If nonsurgical management were elected, application of a non-weight-bearing short leg cast would be appropriate since a higher likelihood of healing is expected with it versus a short leg walking cast. The risk of recurrent fracture of fractures that heal with nonsurgical management has reportedly been high (approximately 30%).**
**REFERENCES: Quill GE: Fractures of the proximal fifth metatarsal. Orthop Clin North Am 1995;26:353-361.**
**Torg JS, Balduini FC, Zelko RR, et al: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.**
**Dameron TB Jr: Fractures of the proximal fifth metatarsal: Selecting the best treatment option.
J Am Acad Orthop Surg 1995;3:110-114.**
**62****. When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
1- increased abduction.
2- pronation.
3- flexion.
4- flexion and pronation.
5- extension.
PREFERRED RESPONSE: 4**
**DISCUSSION: The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal.**
**REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.**
**Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.**
**63****. When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral
base of the proximal phalanx of the great toe. This conjoined tendon is made up of what
two muscles?
1- Flexor hallucis longus and flexor hallucis brevis
2- Flexor hallucis longus and adductor hallucis
3- Flexor hallucis brevis and adductor hallucis
4- Flexor hallucis longus and abductor hallucis
5- Flexor hallucis brevis and abductor hallucis
PREFERRED RESPONSE: 3**
**DISCUSSION: Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis.**
**REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.**
**Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.**
**64****. Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
1- There is no significant difference between the infection rate for this fracture and a similar closed fracture.
2- Due to the risk of infection, open reduction and internal fixation is not recommended for this fracture.
3- The infection rate is three to five times more likely with this fracture.
4- Due to the risk of infection from a lateral approach, treatment is confined to limited internal fixation or an external fixator.
5- The patient will need to undergo 3 weeks of IV antibiotics at home.
PREFERRED RESPONSE: 1**
**DISCUSSION: Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds.**
**REFERENCES: Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.**
**Buckley RE, Tough S: Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg 2004;12:172-178.**
**65****. When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
1- Wound infection
2- Sural nerve injury
3- Achilles tendon re-rupture
4- Weakness
5- Deep venous thrombosis
PREFERRED RESPONSE: 1**
**DISCUSSION: Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique.**
**REFERENCES: Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures:
A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170.**
**Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.**
**Cretnik A, Kosanovic M, Smrkolj V: Percutaneus versus open repair of the ruptured Achilles tendon: A comparative study. Am J Sports Med 2005;33:1369-1379.**
**66****. A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
1- physical therapy and bracing.
2- reassurance that these problems will resolve with time.
3- posterior capsule release, Achilles tendon lengthening, and excision of the scarred muscle and tendon in the leg and foot.
4- Achilles tendon lengthening, and flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with transfer of the posterior tibial tendon to the dorsum of the foot.
5- flexor digitorum longus and flexor hallucis longus tenotomies at the individual digits with midfoot capsular release and hallux interphalangeal fusion.
PREFERRED RESPONSE: 3**
**DISCUSSION: This is an example of a missed deep posterior compartment syndrome that typically presents 6 months after the injury with progressive clawing due to necrosis, scarring, and contracture of the posterior tibial tendon, flexor digitorum longus, and flexor hallucis longus. Treatment consists of debridement of necrotic muscle and scar tissue with corresponding tendon excision. After debridement and posterior capsule release, if the equinus is relieved with knee flexion, a gastrocnemius slide may be performed. Otherwise, the lengthening should be at the level of the Achilles tendon. Bracing will not address the claw toes.**
**REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213.**
**Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.**
**Early JS, Ricketts DS, Hansen ST: Treatment of compartmental liquefaction as a late sequelae of a lower limb compartment syndrome. J Orthop Trauma 1994;8:445-448.
67/. A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
1- Deep infection
2- Failure of repair
3- Peroneus longus tear
4- Peroneus brevis tear
5- Tibiotalar arthritis
PREFERRED RESPONSE: 4**
**DISCUSSION: Chronic lateral instability is commonly associated with a longitudinal split tear of the peroneus brevis tendon. The interrelationship of lateral ankle instability with superior retinacular laxity and resultant peroneus brevis split can account for persistent lateral ankle pain in this patient. Surgical treatment must identify and correct the underlying tendon pathology and should attempt to repair or debride the peroneus brevis tendon, reconstruct the superior peroneal retinaculum, flatten the posterior edge of the fibula by removing the sharp bony prominence, or deepening the fibular groove, along with addressing lateral ankle ligamentous instability. The laboratory values are not consistent with infection. A negative anterior drawer test confirms stability of the repair. Ankle arthritis is not seen on radiographs and usually takes longer than 3 months to develop.**
**REFERENCES: Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.**
**Sobel M, Geppert MJ, Warren RF: Chronic ankle instability as a cause of peroneal tendon injury. Clin Orthop Relat Res 1993;296:187-191.**
**68****. A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
1- Tendon transfer, lateral column lengthening, and heel cord lengthening
2- Triple arthrodesis and heel cord lengthening
3- Tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening
4- Tendon transfer, spring ligament repair, and heel cord lengthening
5- Tendon repair, medial displacement calcaneal osteotomy, and heel cord lengthening
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has an atypical adult flatfoot deformity. The radiographs reveal forefoot abduction, mild loss of calcaneal pitch, and marked plantar flexion sag through the naviculocuneiform joint. The inability to perform a single limb heel rise indicates that the posterior tibial tendon is nonfunctional; however, the deformity remains flexible. In this patient, surgical treatment should include a tendon transfer, lateral column lengthening, medial column arthrodesis, and heel cord lengthening. Because a substantial portion of the deformity stems from the naviculocuneiform joint in this instance, tendon transfer and lateral column lengthening alone provide insufficient deformity correction. Triple arthrodesis and heel cord lengthening is best reserved for fixed flatfoot deformities. Soft-tissue procedures alone are associated with a high failure rate, as are attempted tendon repairs.**
**REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.**
**Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.**
**69****. Optimal management of the injury shown in Figure 31 should include which of
the following?
1- Cast immobilization in equinus
2- Open reduction and internal fixation once the acute soft-tissue swelling has resolved
3- Urgent reduction and fixation
4- Arthroscopic-assisted percutaneous fixation
5- Open reduction and internal fixation with primary subtalar arthrodesis
PREFERRED RESPONSE: 3**
**DISCUSSION: The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular.**
**REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.**
**Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.**
**70****. A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
1- Surgical stabilization within 6 to 8 hours of injury
2- Extent of initial fracture displacement
3- Nicotine use
4- Posterior-to-anterior screw fixation
5- Anatomic fracture reduction
PREFERRED RESPONSE: 2**
**DISCUSSION: The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction.**
**REFERENCES: Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.**
**Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.**
**71****. A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
1- Peroneal longus tendon
2- Peroneal brevis tendon
3- Superior peroneal retinaculum
4- Anterior talofibular ligament
5- Calcaneofibular ligament
PREFERRED RESPONSE: 3**
**DISCUSSION: The symptoms and MRI scan indicate dislocated peroneal tendons. In this patient, the structure that needs to be repaired is the superior peroneal retinaculum. If the popping was coming from a torn peroneal tendon, repair would involve the peroneal longus or brevis tendon, but this is not shown in the MRI scan. The anterior talofibular ligament or the calcaneofibular ligament would need to be repaired if the patient had ankle instability due to an ankle sprain.**
**REFERENCES: Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.**
**Timins ME: MR imaging of the foot and ankle. Foot Ankle Clin 2000;5:83-101.**
**72****. A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
1- Plastizote orthotics with a metatarsal pad and a cutout under the fifth metatarsal head
2- Hyperbaric oxygen and prolonged non-weight-bearing
3- A healing shoe that completely alleviates any weight bearing on the forefoot
4- A gastrocnemius release and supportive wound care
5- A transmetatarsal amputation
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification.**
**REFERENCES: Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.**
**Aronow MS, Diaz-Doran V, Sullivan RJ, et al: The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int 2006;27:43-52.**
**73****. The hallucal sesamoids are held together by which of the following structures?
1- Intersesamoid ligament
2- Intermetatarsal ligament
3- Spring ligament
4- Plantar fascia
5- Flexor hallucis longus tendon
PREFERRED RESPONSE: 1**
**DISCUSSION: The two sesamoids of the metatarsophalangeal joint are embedded in the tendons of the short flexor of the great toe. They are held together by the intersesamoid ligament and the plantar plate, which inserts on the base of the proximal phalanx of the hallux. The flexor hallucis longus tendon inserts onto the distal phalanx of the great toe. The plantar calcaneonavicular (spring) ligament, by supporting the head of the talus, principally maintains the arch of the foot. The plantar fascia inserts distally onto the skin and to the flexor tendons and transverse metatarsal ligaments at each metatarsophalangeal joint. The intermetatarsal ligament attaches to the base of the second through fifth metatarsals.**
**REFERENCES: Lewis WH (ed): Gray’s Anatomy of the Human Body, ed 20. Philadelphia, PA, Lea & Febiger, 2000. **
**Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.**
**74****. Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?
1- Therapeutic footwear/depth-inlay shoes and a custom accommodative foot orthosis
2- Charcot restraint orthotic walker (CROW)
3- Percutaneous Achilles tendon lengthening, a total contact cast, and a CROW walker
4- Surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear
5- Ankle disarticulation (Syme) amputation
PREFERRED RESPONSE: 4**
**DISCUSSION: This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear.**
**REFERENCES: Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573.**
**Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.**
**Pinzur M: Surgical versus accommodative treatment for Charcot arthropathy of the midfoot.
Foot Ankle Int 2004;25:545-549.**
**75****. Which of the following conditions precludes performing a tendon transfer?
1- The target joint has a full passive range of motion.
2- The range of motion of the target joint only occurs in the direction of correction.
3- The target joint cannot be passively corrected to its neutral position.
4- The muscle to be transferred is out-of-phase.
5- There is no pulley to assist the transferred muscle’s fulcrum.
PREFERRED RESPONSE: 3**
**DISCUSSION: Several conditions must be met before a tendon transfer has the potential to correct a dynamic deformity. If the target joint cannot be passively corrected to neutral, it indicates that a static joint contracture or bony deformity exists that cannot be corrected with a dynamic tendon transfer. While in-phase muscles are best, out-of-phase muscles are often the only muscles available for transfer. Tendon transfer should pull in a straight line to avoid tethering and late failure.**
**REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.**
**Coughlin MJ, Mann RA: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 786-861.**
**76****. A 26-year-old rugby player injured his foot when tackled from behind. Radiographs are seen in Figures 35a through 35c. What is the most appropriate treatment?
1- Closed reduction and percutaneous pin fixation
2- Application of a short leg non-weight-bearing cast
3- Application of a walking boot with weight bearing as tolerated
4- Open reduction and internal fixation
5- Elastic bandage wrap and activity as tolerated
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a ligamentous Lisfranc injury. Diastasis seen between the bases of the second metatarsal and medial cuneiform is pathognomonic for a rupture of the Lisfranc’s ligament. This injury is best treated surgically with either open reduction and internal fixation or possibly closed manipulation and percutaneous screw fixation if anatomic alignment can be achieved closed. Pin fixation has been shown to be inferior to screw fixation due to the length of time that fixation is required for adequate ligament healing.**
**REFERENCES: Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries of the tarsometatarsal joint. Orthop Clin North Am 2001;32:11-20.**
**Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.**
**77****. A 32-year-old woman sustained a closed calcaneus fracture 2 years ago and was treated nonsurgically. She now reports a 6-month history of progressively worsening pain over the anterior ankle and lateral hindfoot. Climbing stairs and ascending slopes is particularly difficult for her. Bracing and intra-articular corticosteroid injections have not provided sufficient relief. Figure 36 shows a weight-bearing lateral radiograph. What is the most appropriate surgical option?
1- Subtalar arthrodesis in situ with plantar flexion osteotomy of the talar neck
2- Distraction subtalar arthrodesis with a corticocancellous bone block autograft
3- Subtalar arthrodesis in situ
4- Triple arthrodesis
5- Subtalar arthrodesis in situ with anterior ankle exostectomy
PREFERRED RESPONSE: 2**
**DISCUSSION: Intra-articular fractures of the calcaneus often include depression of the posterior facet of the subtalar joint. This can lead to dorsiflexion of the talus because of diminished height posteriorly. In a weight-bearing position, the dorsal surface of the talar neck can impinge against the distal tibia, causing anterior ankle pain. In addition, posttraumatic arthritis of the subtalar joint typically occurs after a calcaneus fracture. The patient’s symptoms are consistent with both anterior ankle impingement and subtalar degenerative arthritis. The Bohler angle, approximately 15 degrees, confirms depression of the posterior facet. Distraction subtalar arthrodesis with a corticocancellous bone block autograft will improve talar declination, decrease anterior impingement, and address the subtalar degenerative arthritis simultaneously.**
**REFERENCES: Rammelt S, Grass R, Zawadski T, et al: Foot function after subtalar distraction bone-block arthrodesis: A prospective study. J Bone Joint Surg Br 2004;86:659-668.**
**Trnka HJ, Easley ME, Lam PW, et al: Subtalar distraction bone block arthrodesis. J Bone Joint Surg Br 2001;83:849-854.**
**78****. A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
1- The role her husband will play in the decision to proceed with surgery
2- Her role as primary caregiver in the household
3- Dietary concerns during her hospitalization
4- Daily cleansing rituals that may affect wound care
5- The importance of maintaining modesty precautions during examination, surgery, and postoperative appointments
PREFERRED RESPONSE: 5**
**DISCUSSION: In considering faith-based issues regarding treatment of this patient, the presence of her husband for the office visit would imply an agreement with her decision to have surgery. It also may facilitate her examination. Her role as caregiver, dietary concerns, and cleansing rituals are less important considerations with an outpatient-based procedure. Privacy concerns remain paramount to Muslim women, which include limited exposure during examination, during surgery, and in subsequent follow-up visits.**
**REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**79****. A 35-year-old female runner reports progressive vague aching pain involving her midfoot. Her pain is most notable when running. She denies specific injury. Examination reveals minimal swelling and localized tenderness over the dorsal medial midfoot and navicular. Radiographs and an MRI scan are shown in Figures 37a through 37c. What is the most appropriate management?
1- Non-weight-bearing immobilization and CT
2- Walking boot and weight bearing as tolerated
3- Activity restrictions (avoidance of running) and repeat radiographs in 2 to 4 weeks
4- Activity restrictions and a bone scan
5- Surgical fixation
PREFERRED RESPONSE: 1**
**DISCUSSION: A high index of suspicion is required to identify a possible navicular stress fracture, especially in runners. High pain tolerance in the competitive athlete and often minimal swelling contribute to frequent delays in diagnosis. Localized tenderness over the dorsal navicular (so-called “N spot”) in a running athlete should alert the treating physician. In this patient, the radiographs are negative and the MRI scan shows marrow edema within the navicular. This could represent a stress reaction, stress fracture, or osteonecrosis. Appropriate management should include non-weight-bearing immobilization and obtaining a CT scan to determine if a fracture is present. Early surgical treatment may be considered but only if a fracture is identified.**
**REFERENCES: Lee A, Anderson R: Stress fractures of the tarsal navicular. Foot Ankle Clin 2004;9:85-104.**
**Coughlin M: Tarsal navicular stress fractures. Tech Foot Ankle Surg 2002;1:112-122.**
**80****. A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
1- Metatarsophalangeal joint arthrodesis
2- Medial capsular release with lengthening of the abductor hallucis
3- Medial capsular release with lateral sesamoid excision
4- Proximal phalangeal lateral closing wedge osteotomy
5- Medial capsular lengthening and split extensor hallucis longus tendon transfer
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has a flexible hallux varus that is a complication of the bunion surgery. With joints that are not arthritic and still flexible, a medial release is necessary to realign the joint. The extensor hallucis longus split transfer helps maintain position and still preserve motion at the interphalangeal joint level. Arthrodesis is a salvage procedure. Soft-tissue releases alone are most likely inadequate. Excision of the lateral sesamoid is contraindicated because that further compromises the forces resisting hallux varus. Phalangeal osteotomy would not address the medial subluxation at the metatarsophalangeal joint.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.**
**Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.**
**81****. A 43-year-old man reports a 3-year history of progressively worsening pain in the first metatarsophalangeal joint that is aggravated by activity. Larger shoes, intra-articular corticosteroid injections, and a Morton’s extension pedorthic have failed to provide relief. Motion is limited to 10 degrees of dorsiflexion, and the “grind test” is positive. An AP radiograph is shown in Figure 39. What is the most appropriate surgical treatment?
1- Cheilectomy
2- Moberg osteotomy
3- Keller resection arthroplasty
4- Resurfacing implant hemiarthroplasty
5- First metatarsophalangeal arthrodesis
PREFERRED RESPONSE: 5**
**DISCUSSION: Stage III hallux rigidus comprises end-stage degenerative arthritis with loss of cartilage from the phalanx and metatarsal. Therefore, cheilectomy, osteotomy, and resection arthroplasty are inadequate. Resection arthroplasty results in diminished propulsion and transfer metatarsalgia. Resurfacing implant hemiarthroplasty remains unproven for earlier stages of hallux rigidus, but is not appropriate when there is cartilage loss from the base of the proximal phalanx. First metatarsophalangeal arthrodesis has proven to be a very reliable and functional treatment of end-stage hallux rigidus.**
**REFERENCES: Gibson JN, Thomson CE: Arthrodesis or total replacement arthroplasty for hallux rigidus: A randomized controlled trial. Foot Ankle Int 2005;26:680-690.**
**Brage ME, Ball ST: Surgical options for salvage of end-stage hallux rigidus. Foot Ankle Clin 2002;7:49-73.**
**82****. A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
1- Correction of the flatfoot deformity
2- Achilles tendon lengthening followed by orthotic support
3- Excision of the tarsal coalition
4- Sinus tarsi debridement
5- Triple arthrodesis
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has a calcaneonavicular tarsal coalition. Symptoms of calcaneonavicular coalitions typically are seen between the ages of 10 and 14 years. The cause of pain has not been clearly established. It has been postulated that the coalition stiffens with maturity and microfractures can result, producing pain. Resection of a calcaneonavicular coalition generally has been associated with a satisfactory result. Soft-tissue interposition, most commonly using the extensor digitorum brevis muscle, appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.**
**REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.**
**Lemley F, Berlet G, Hill K, et al: Current concepts review: Tarsal coalition. Foot Ankle Int 2006;27:1163-1169.**
**83****. A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in
the radiographs?
1- Reduces shrinkage of the residual limb
2- Creates a more stable platform for load transfer
3- Reduces wound healing complications by avoiding the soft-tissue dissection necessary to transect the fibula at a level proximal to the tibia
4- Connecting bone strut provides an attachment point for more effective myodesis
5- Allows a more proximal resection level to decrease tension on the wound
PREFERRED RESPONSE: 2**
**DISCUSSION: The Ertl modification of a below-knee amputation has been proposed to create a more stable “platform” to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient’s perceived functional outcome.**
**REFERENCES: Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula.
Foot Ankle Int 2006;27:907-912.**
**Pinzur MS, Pinto MA, Schon LC, et al: Controversies in amputation surgery. Instr Course Lect 2003;52:445-451.
84/. Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm3, a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm3. What treatment has the best potential to optimize his survival and independence?
1- Local wound care, parenteral antibiotic therapy, metabolic support, and reevaluation in 1 week
2- Vascular consultation for a bypass operation
3- Syme ankle disarticulation
4- Guillotine transtibial amputation
5- Closed transtibial amputation
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient was admitted to the hospital with sepsis. The sepsis has resolved, leaving the patient with a negative nitrogen balance. Now that the patient is stable, metabolic support should be used to optimize his nutrition. If the serum albumin can be increased to 2.5 g/dL, he has an excellent potential to heal an amputation at the Syme ankle disarticulation level; a level that will optimize his functional independence.**
**REFERENCES: Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.**
**Pinzur MS, Smith D, Osterman H: Syme ankle disarticulation in peripheral vascular disease and diabetic foot infection: The one-stage versus two-stage procedure. Foot Ankle Int 1995;16:124-127.**
**85****. A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
1- Resolution by age 3 or 4 years without active treatment in most patients
2- Resolution by age 8 or 9 years without active treatment in most patients
3- Resolution with casting as the most effective treatment
4- Resolution with bracing and shoe modification as the most effective treatment
5- Resolution with surgery as the most effective treatment
PREFERRED RESPONSE: 1**
**DISCUSSION: Excessive internal tibial torsion is a common cause of intoeing in toddlers. In most children, this resolves spontaneously by 3 to 4 years of age. Intoeing in elementary age children is usually the result of excessive femoral anteversion. Studies have shown that active intervention (casting, splinting, and shoe modifications) has no demonstrable effect on the natural history or resolution of tibial torsion. Surgery is rarely indicated in adolescents with severe internal tibial torsion that has not resolved and is resulting in cosmetic and functional problems.**
**REFERENCES: Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.**
**Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.**
**86****. Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
1- Talonavicular
2- Naviculocuneiform
3- Subtalar
4- Cuboid-fifth metatarsal
5- Calcaneocuboid
PREFERRED RESPONSE: 1**
**DISCUSSION: Arthrodesis of the talonavicular joint eliminates almost all hindfoot motion. Arthrodesis of the subtalar joint eliminates 74% of talonavicular motion and 44% of calcaneocuboid motion. Arthrodesis of the calcaneocuboid joint eliminates 33% of talonavicular motion and 8% of subtalar motion. Arthrodesis of the naviculocuneiform or cuboid-fifth metatarsal joint has limited effect on hindfoot motion.**
**REFERENCES: Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.**
**Savory KM, Wülker N, Stukenborg C, et al: Biomechanics of the hindfoot joints in response to degenerative hindfoot arthrodeses. Clin Biomech 1998;13:62-70.**
**87****. A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
1- Irrigation and debridement of the cystic lesion and 6 weeks of IV antibiotics
2- Curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics
3- Complete resection of the infected portion of bone, placement of an external fixator to stabilize the tibia, and 6 weeks of IV antibiotics
4- Amputation
5- Local debridement of bone and the overlying skin and soft tissues, 6 weeks of IV antibiotics, and free-flap wound coverage
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful.**
**REFERENCES: Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.**
**Beals RK, Bryant RE: The treatment of chronic open osteomyelitis of the tibia in adults.
Clin Orthop Relat Res 2005;433:212-217.**
**88****. Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
1- Artery medial, then lateral
2- Artery lateral, then medial
3- Artery always medial
4- Artery always lateral
5- Artery always deep
PREFERRED RESPONSE: 1**
**DISCUSSION: At the ankle level, the anterior tibial artery lies medial to the EHL tendon. The artery becomes the dorsalis pedis after crossing onto the dorsum of the foot. At this point, the artery lies lateral to the tendon.**
**REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.**
**Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.**
**89****. A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?
1- Steroid injection
2- Debridement and side-to-side repair
3- Debridement and flexor hallucis longus tendon transfer
4- Brisement
5- Continued nonsurgical management with use of a short leg walking cast
PREFERRED RESPONSE: 3**
**DISCUSSION: The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.**
**Den Hartog BD: Flexor hallucis longus transfer for chronic Achilles tendinosis. Foot Ankle Int 2003;24:233-237.**
**90****. A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled “A” in Figure 45?
1- Longitudinal split tear in the peroneus longus
2- Longitudinal split tear in the peroneus brevis
3- Plantaris
4- Peroneus accessorius
5- Peroneus quartus
PREFERRED RESPONSE: 5**
**DISCUSSION: The structure labeled “A” is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath.**
**REFERENCES: Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.**
**Sobel M, Levy ME, Bohne WH: Congenital variations of the peroneus quartus muscle: An anatomic study. Foot Ankle 1990;11:81-89.**
**91****. You are asked to evaluate the patient whose current clinical photographs are shown in Figures 46a and 46b following aortic valve replacement 9 days ago. He is currently taking anticoagulation medication. He has no systemic signs of sepsis. What is the best management?
1- Warming in a water or saline bath at 104 degrees F (40 degrees C) with no dressings
2- Observation with possible late debridement
3- Urgent arteriogram
4- Reversal of anticoagulation, parenteral antibiotics, and debridement
5- Reversal of anticoagulation, parenteral antibiotics, and open forefoot amputation
PREFERRED RESPONSE: 2**
**DISCUSSION: These lesions are emboli related to the cardiac surgery, and the patient is already on anticoagulation medication. The foot reveals no signs consistent with gangrene or infection. Unless the patient shows local or systemic signs of sepsis, the best management is observation. It is unlikely that formal debridement will be necessary.**
**REFERENCES: Bowker JH, Pfeiffer MA (eds): The Diabetic Foot. St Louis, MO, Mosby, 2001,
pp 219-260.**
**Coughlin MJ, Mann RA: Soft tissue disorders of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1373-1397.**
**92****. A 48-year-old woman with a history of a spinal cord injury as a teenager, has unilateral weakness in the left lower extremity. She has used an ankle-foot orthosis for many years without difficulty but recently has had a recurrent painful callus beneath the great toe that has been recalcitrant to nonsurgical management. Examination reveals intact sensation with an intractable plantar keratosis (IPK) beneath the first metatarsal head. Motor examination reveals no active ankle or great toe dorsiflexion, and 4/5 plantar flexion strength at the ankle and great toe. Passive ankle dorsiflexion is 10 degrees, whereas passive plantar flexion is
40 degrees. Passive great toe dorsiflexion is 30 degrees and plantar flexion is 10 degrees. Foot alignment on standing is normal. Radiographs are shown in Figures 47a and 47b with a marker beneath the IPK. Based on her request for surgical treatment, what is the most appropriate procedure?
1- Gastrocnemius recession
2- Keller bunionectomy
3- Flexor hallucis longus tendon transfer
4- Planing/excising the superficial half of the medial sesamoid
5- Dorsiflexion osteotomy of the first metatarsal
PREFERRED RESPONSE: 4**
**DISCUSSION: Passive dorsiflexion is adequate to accommodate standing erect without excessive pressure, and a gastrocnemius recession may lead to more instability. Complete excision of the medial sesamoid could lead to an iatrogenic hallux valgus deformity. She does not have a cock-up toe deformity; therefore, a flexor hallucis longus tendon transfer is not warranted. There is no significant foot deformity; therefore, a dorsiflexion osteotomy is not warranted. The appropriate procedure is planing of the plantar half of the medial sesamoid, thereby preserving its function while diminishing the excessive pressure.**
**REFERENCES: Grace DL: Sesamoid problems. Foot Ankle Clin 2000;5:609-627.**
**Mizel MS, Miller RA, Scioli MW (ed): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 135-150.**
**Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.**
**93****. The cavovarus deformity associated with Charcot-Marie-Tooth (CMT) disease is caused by which of the following?
1- Streptococcal disease during infancy
2- Viral infection of the motor nerves
3- Sex-linked selective motor imbalance
4- Autosomal-dominant myelin sheath disease
5- Germ cell defect leading to asymmetrical growth disturbance
PREFERRED RESPONSE: 4**
**DISCUSSION: The most common inherited neuromuscular disease seen by orthopaedic surgeons is CMT, which is an inherited autosomal-dominant disease. It is more commonly seen in men due to the nature of the inheritance. Identification of cavus deformity in the foot of a child should arouse suspicion.**
**REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-143.**
**Charcot-Marie-Tooth Disease (CMT) Penn State Hershey Medical Center.**
**www.hmc.psu.edu/healthinfo/c/cmt.htm**
**94****. When performing a gastrocnemius recession, what structure should be protected?
1- Tibial nerve
2- Sural artery
3- Plantaris
4- Posterior tibial artery
5- Sural nerve
PREFERRED RESPONSE: 5**
**DISCUSSION: When performing a gastrocnemius slide at the tendinous portion of the gastrocnemius insertion, the sural nerve and saphenous vein, which tend to run midline posterior at this level, must be protected and retracted laterally. An anatomic study of the sural nerve at this level localized the nerve superficial to the deep fascia overlying the gastrocnemius in 42.5% of the cases; deep to the superficial fascia in 57.5% of the cases, and directly applied to the gastrocnemius tendon in 12.5% of cases.**
**REFERENCES: Pinney SJ, Sangeorzan BJ, Hanen ST Jr: Surgical anatomy of the gastrocnemius resection (Strayer procedure). Foot Ankle Int 2004;25:247-250.**
**Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 415-417.**
**95****. A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle
6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
1- Physical therapy
2- Hardware removal
3- Repeat placement of a syndesmotic screw
4- Deltoid ligament reconstruction
5- Revision ORIF with exploration of the syndesmosis and medial ankle
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction.**
**REFERENCES: Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.**
**Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.**
**96****. A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
1- Cephalosporin
2- Cephalosporin and aminoglycoside
3- Cephalosporin and penicillin
4- Cephalosporin and vancomyacin
5- Cephalosporin, aminoglycoside, and penicillin
PREFERRED RESPONSE: 5**
**DISCUSSION: A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries.**
**REFERENCES: Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.**
**Holtom PD: Antibiotic prophylaxis: Current recommendations. J Am Acad Orthop Surg 2006:14:S98-S100.**
**97****. A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient’s ability to heal the wound postoperatively?
1- Absolute toe pressures of 55 mm Hg
2- Transcutaneous oxygen level of 20 mm Hg
3- Arterial brachial indices (ABI) of 1.2 at the level of surgery
4- ABI 0.3 at the level of surgery
5- Albumin level of 2.5
PREFERRED RESPONSE: 1**
**DISCUSSION: Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status.
A transcutaneous oxygen level should be greater than 40 mm Hg for healing.**
**REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.**
**Pinzur MS, Stuck R, Sage R: Benchmark analysis on diabetics at high risk for lower extremity amputation. Foot Ankle Int 1996;17:695-700.**
**98****. Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
1- Methotrexate
2- Gold
3- Hydroxychloroquine
4- TNF-a inhibitors
5- Smoking
PREFERRED RESPONSE: 5**
**DISCUSSION: Clinical studies have shown that smoking cessation for 4 weeks reduces the risk of infection to the level of nonsmokers. Adverse effects on wound healing caused by chemotherapy used to treat rheumatoid arthritis has not been borne out in the literature.**
**REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.**
**Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.**
**Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.**
**99****. Intrinsic muscles of the foot act on the toes by
1- abducting the metatarsophalangeal joints and flexing the interphalangeal joints.
2- extending the metatarsophalangeal and interphalangeal joints.
3- extending the metatarsophalangeal joints and flexing the interphalangeal joints.
4- flexing the metatarsophalangeal and interphalangeal joints.
5- flexing the metatarsophalangeal joints and extending the interphalangeal joints.
PREFERRED RESPONSE: 5**
**DISCUSSION: Intrinsic muscles of the foot function to flex the metatarsophalangeal joints and extend the interphalangeal joints.**
**REFERENCES: Myerson MS, Shereff MJ: The pathologic anatomy of claw and hammertoes.
J Bone Joint Surg Am 1989;71:45-49.**
**Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 71-80.**
**100****. A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
1- Continued bracing, physical therapy, and Botox injections in the triceps surae
2- Peroneus longus to brevis transfer, medializing calcaneal osteotomy, and transfer of the extensor digitorum longus to the peroneus tertius
3- Peroneus longus to brevis transfer, and transfer of the posterior tibial tendon to the tibialis anterior tendon
4- Peroneus longus to brevis transfer, first metatarsal cuneiform dorsal closing wedge osteotomy, and lateralizing calcaneal osteotomy with proximal translation
5- Triple arthrodesis
PREFERRED RESPONSE: 4**
**DISCUSSION: The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended.**
**REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.**
**Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.**
**Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL,
American Academy of Orthopaedic Surgeons, 2003, pp 135-143.**
Question 10High Yield
Figure 6a through 6c
Explanation
Figure 2 depicts a typical unicameral bone cyst with a pathologic fracture. The decision to treat this lesion should be based on the amount of cortical thinning. If these lesions involve a pathologic fracture, many surgeons will treat them nonsurgically to see if the fracture stimulates healing of the cyst. If the cyst wall remains thin or the patient is symptomatic, then treatment is directed at decreasing cyst volume, increasing cortical thickness, and eliminating symptoms. This can be accomplished by curettage and grafting, injection with autogenous bone marrow, or grafting with 1 of the many available bone void fillers. In some cases, internal fixation may be required. This typically is accomplished with flexible intramedullary nails.
Figure 3 shows a typical nonossifying fibroma. These benign lesions are usually incidental findings on a radiograph and often resolve in adulthood. Treatment usually is not required, and these lesions typically do not produce symptoms.
Figure 4 shows an osteoid osteoma of the femoral neck. This is characterized by a central radiolucent nidus surrounded by reactive bone with increased radiodensity. These lesions are painful because of the large amount of prostaglandin they secrete. They temporarily respond to oral anti-inflammatory drugs. Treatment is directed at eliminating the nidus and can be done through curettage, but radiofrequency ablation, which allows for a minimally invasive approach, is often used today.
Figure 5 shows diskitis with vertebral osteomyelitis. The disease is characterized by fever and back pain. Movement is extremely uncomfortable for these children, and they may adopt unusual postures to alleviate pain. The MRI shows involvement of 1 vertebrae and an adjacent disk. Left untreated, this condition often spreads to involve multiple vertebrae and also can cause an epidural abscess. Treatment during the early stages is IV antibiotics. Many orthopaedic surgeons also use bracing to prevent late vertebral collapse.
Figures 6a through 6c show septic arthritis of the ankle with metaphyseal osteomyelitis. The recommended treatment is incision and drainage followed by IV antibiotics. MRI may be considered before surgery to assess for an associated osteomyelitis or abscess that may also necessitate surgical debridement. Increasingly, these scenarios are managed with a rapid transition to oral antibiotics.
Figure 3 shows a typical nonossifying fibroma. These benign lesions are usually incidental findings on a radiograph and often resolve in adulthood. Treatment usually is not required, and these lesions typically do not produce symptoms.
Figure 4 shows an osteoid osteoma of the femoral neck. This is characterized by a central radiolucent nidus surrounded by reactive bone with increased radiodensity. These lesions are painful because of the large amount of prostaglandin they secrete. They temporarily respond to oral anti-inflammatory drugs. Treatment is directed at eliminating the nidus and can be done through curettage, but radiofrequency ablation, which allows for a minimally invasive approach, is often used today.
Figure 5 shows diskitis with vertebral osteomyelitis. The disease is characterized by fever and back pain. Movement is extremely uncomfortable for these children, and they may adopt unusual postures to alleviate pain. The MRI shows involvement of 1 vertebrae and an adjacent disk. Left untreated, this condition often spreads to involve multiple vertebrae and also can cause an epidural abscess. Treatment during the early stages is IV antibiotics. Many orthopaedic surgeons also use bracing to prevent late vertebral collapse.
Figures 6a through 6c show septic arthritis of the ankle with metaphyseal osteomyelitis. The recommended treatment is incision and drainage followed by IV antibiotics. MRI may be considered before surgery to assess for an associated osteomyelitis or abscess that may also necessitate surgical debridement. Increasingly, these scenarios are managed with a rapid transition to oral antibiotics.
Question 11High Yield
A 68-year-old man presents with chronic progressive right shoulder pain and loss of motion. He has active shoulder elevation of 120° and 5-/5 shoulder forward flexion strength limited by pain. He has exhausted nonsurgical management over the past year and is now interested in surgical intervention. Figure 1 is the preoperative axial CT scan of his shoulder. During surgical reconstruction, the surgeon should anticipate the location of maximal glenoid erosion to be
58
58
Explanation
In patients with primary osteo- arthritis of the shoulder, eccent- ric wear on the face of the glenoid is frequently combined with static subluxation of the humeral head. Current studies have clarified that patients with Walch B2 glenoid develop wear along the posterior inferior face of the glenoid and not directly posterior. At the time of shoulder arthroplasty, the eccentric center of rotation must be corrected by soft-tissue, bony, and/or implant
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
Question 12High Yield
Nerve conduction velocity is slowed by
Explanation
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no association between hand dominance and nerve conduction velocity.
RECOMMENDED READINGS
57. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
58. Freedman M, Helber G, Pothast J, Shahwan TG, Simon J, Sher L. Electrodiagnostic evaluation of compressive nerve injuries of the upper extremities. Orthop Clin North Am. 2012 Oct;43(4):409-16. doi:10.1016/j.ocl.2012.07.010. Epub 2012 Sep 10. Review. PubMed PMID: 23026456.
59. Lundborg G. A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am. 2000 May;25(3):391-414. Review. PubMed PMID: 10811744.
RECOMMENDED READINGS
57. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
58. Freedman M, Helber G, Pothast J, Shahwan TG, Simon J, Sher L. Electrodiagnostic evaluation of compressive nerve injuries of the upper extremities. Orthop Clin North Am. 2012 Oct;43(4):409-16. doi:10.1016/j.ocl.2012.07.010. Epub 2012 Sep 10. Review. PubMed PMID: 23026456.
59. Lundborg G. A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am. 2000 May;25(3):391-414. Review. PubMed PMID: 10811744.
Question 13High Yield
The mangled extremity severity score (MESS) utilizes all of the following variables EXCEPT:
Explanation
The MESS is a tool utilized to help predict limb salvage success versus primary amputation at the time of presentation. As a screening tool for amputation, this scoring system has a high specificity but low sensitivity, as scores lower than 7 may also ultimately need amputation. All of the variables except choice #5 are part of the scoring system.
The scoring system is as follows: 1. Skeletal / soft-tissue injury: Low energy = 1; Medium energy = 2; High energy = 3; very high energy = 4; 2. Limb ischemia: Pulse reduced or absent but perfusion normal = 1; Pulseless = 2; Cool, paralyzed, insensate = 3; 3. Shock: normotensive = 0; transient hypotension = 1; persistent hypotension = 2; 4. Age: < 30 = 0; 30-50 = 1;
>50 = 2. Limb category scores are doubled for ischemia > 6 hours. The system's original designers reported a cutoff of 7 as predicting amputation.
The referenced study by Ly et al found that the scoring system did not predict functional outcomes at 6 or 24 months. They also found that the Limb Salvage Index; the Predictive Salvage Index; the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score; and the Hannover Fracture Scale-98 all did not predict outcomes at 6 or 24 months.
The scoring system is as follows: 1. Skeletal / soft-tissue injury: Low energy = 1; Medium energy = 2; High energy = 3; very high energy = 4; 2. Limb ischemia: Pulse reduced or absent but perfusion normal = 1; Pulseless = 2; Cool, paralyzed, insensate = 3; 3. Shock: normotensive = 0; transient hypotension = 1; persistent hypotension = 2; 4. Age: < 30 = 0; 30-50 = 1;
>50 = 2. Limb category scores are doubled for ischemia > 6 hours. The system's original designers reported a cutoff of 7 as predicting amputation.
The referenced study by Ly et al found that the scoring system did not predict functional outcomes at 6 or 24 months. They also found that the Limb Salvage Index; the Predictive Salvage Index; the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score; and the Hannover Fracture Scale-98 all did not predict outcomes at 6 or 24 months.
Question 14High Yield
Figures 77a and 77b are the recent knee radiographs of a 53-year-old man whose history includes tobacco use and secondary polycythemia. He is now experiencing bilateral knee pain, knee swelling, and increasing discomfort with ambulation. All efforts at nonsurgical treatment have failed. What is the most reasonable next treatment option?


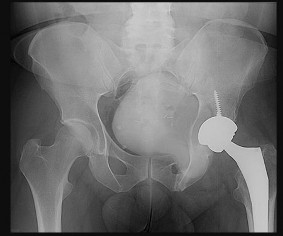

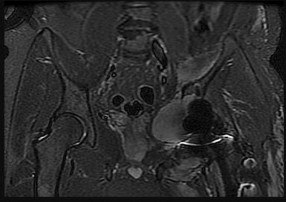
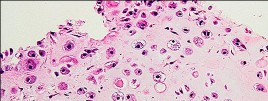
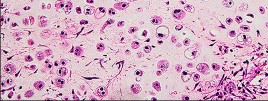
Explanation
The radiographs reveal bilateral bone infarcts with subchondral collapse. The images are diagnostic for bone infarct. Other hematological conditions are associated with multiple bone infarcts, including sickle-cell disease, hemophilia, aplastic anemia, thalassemia, and acute lymphoblastic leukemia. Postsurgical radiation therapy is considered for Paget disease, but the radiographic appearance is not consistent with that diagnosis.
RECOMMENDED READINGS
57. [Lotke PA, Ecker ML. Osteonecrosis of the knee. J Bone Joint Surg Am. 1988 Mar;70(3):470-3. Review. PubMed PMID: 3279040.](http://www.ncbi.nlm.nih.gov/pubmed/3279040)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3279040)
58. [Sorich MM, Cherian JJ, McElroy MJ, Banerjee S, Jones LC, Minniti CP, Mont MA. Osteonecrosis of the Hip in Hematologic Disease: A Review of Conditions and Treatment Options. J Long Term Eff Med Implants. 2015;25(4):253-68. PubMed PMID: 26852634.](http://www.ncbi.nlm.nih.gov/pubmed/26852634)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26852634)
59. Karim AR, Cherian JJ, Jauregui JJ, Pierce T, Mont MA. Osteonecrosis of the knee: review. Ann Transl Med. 2015 Jan;3(1):6. doi: 10.3978/j.issn.2305-5839.2014.11.13. Review. PubMed PMID: 25705638.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25705638)
CLINICAL SITUATION FOR QUESTIONS 78 AND 79
Figures 78a through 78d are the radiograph, CT scans, and biopsy specimen of a 45-year-old man with a history of treatment for localized low-grade pelvic chondrosarcoma with limb salvage. He now has recurrent pain about his hip.
RECOMMENDED READINGS
57. [Lotke PA, Ecker ML. Osteonecrosis of the knee. J Bone Joint Surg Am. 1988 Mar;70(3):470-3. Review. PubMed PMID: 3279040.](http://www.ncbi.nlm.nih.gov/pubmed/3279040)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3279040)
58. [Sorich MM, Cherian JJ, McElroy MJ, Banerjee S, Jones LC, Minniti CP, Mont MA. Osteonecrosis of the Hip in Hematologic Disease: A Review of Conditions and Treatment Options. J Long Term Eff Med Implants. 2015;25(4):253-68. PubMed PMID: 26852634.](http://www.ncbi.nlm.nih.gov/pubmed/26852634)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26852634)
59. Karim AR, Cherian JJ, Jauregui JJ, Pierce T, Mont MA. Osteonecrosis of the knee: review. Ann Transl Med. 2015 Jan;3(1):6. doi: 10.3978/j.issn.2305-5839.2014.11.13. Review. PubMed PMID: 25705638.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25705638)
CLINICAL SITUATION FOR QUESTIONS 78 AND 79
Figures 78a through 78d are the radiograph, CT scans, and biopsy specimen of a 45-year-old man with a history of treatment for localized low-grade pelvic chondrosarcoma with limb salvage. He now has recurrent pain about his hip.
Question 15High Yield
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
**
**
DISCUSSION: The condition described in this case is known as a stinger or burner. It is caused by stretching the upper trunk of the brachial plexus in the C5 and C6 nerve roots. The symptoms are temporary and last 15 to 20 minutes. There are no residual deficits, unless the patient has had multiple repetitive injuries. Once motor and sensory examination findings and reflexes have normalized, the athlete can return to play. Acute spinal cord injury may cause temporary complete paralysis in the upper and lower extremities with resolution of symptoms within 24 hours. Central cord syndrome affects the upper more than lower extermities and affects mostly elderly patients. Nerve root avulsions lead to permanent deficits and have a poor prognosis for return of function. Guillain-BarDe syndrome is an autoimmune disease that presents as an ascending paralysis with weakness in the legs that spreads to the upper limbs and the face along with complete loss of deep tendon reflexes.
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
**
DISCUSSION: The condition described in this case is known as a stinger or burner. It is caused by stretching the upper trunk of the brachial plexus in the C5 and C6 nerve roots. The symptoms are temporary and last 15 to 20 minutes. There are no residual deficits, unless the patient has had multiple repetitive injuries. Once motor and sensory examination findings and reflexes have normalized, the athlete can return to play. Acute spinal cord injury may cause temporary complete paralysis in the upper and lower extremities with resolution of symptoms within 24 hours. Central cord syndrome affects the upper more than lower extermities and affects mostly elderly patients. Nerve root avulsions lead to permanent deficits and have a poor prognosis for return of function. Guillain-BarDe syndrome is an autoimmune disease that presents as an ascending paralysis with weakness in the legs that spreads to the upper limbs and the face along with complete loss of deep tendon reflexes.
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 16High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 17High Yield
A 40-year-old male laborer with an acute left shoulder injury (Figures 94a and 94b).


Explanation
- Open reduction and internal fixation (ORIF)_
Question 18High Yield
Which of the following statements is true concerning atlanto-occipital dislocations in children:
Explanation
Pediatric atlanto-occipital dislocation is increasing in frequency due to improved emergency care. Although the injuries are sometimes fatal and are often accompanied by severe spinal cord injury, this is not always the case. Although the dens-basion distance should be less than 10 mm and the power ratio should be less than 1 in normals, these are not always abnormal in children with such injuries. C linical and radiographic correlation, with computer tomography or magnetic resonance imaging if needed, are called for to maximize diagnosis.
Question 19High Yield
..What is the best next step?
Explanation
- Posterior shoulder dislocation PREFERRED RESPONSE: 2- CT scan
Question 20High Yield
Which muscles cause the fracture displacement of the proximal fragment shown in figure A?

Explanation
The gluteus medius attaches to the greater trochanter, leading to abduction, while the iliopsoas attaches to the lesser trochanter, leading to flexion. French et al evaluated forty-five Russell-Taylor Type 1B subtrochanteric femoral fractures which were stabilized using an interlocked cephalomedullary nail. The intraoperative complication rate was 13.5%; and the most frequent complication was a varus malreduction. The primary reason for this was failure to counteract the muscle forces acting on the proximal fragment combined with the adducted position of the distal femur during portal creation. This problem can be avoided if the position of the proximal fragment is evaluated carefully and reduced before guidewire insertion.
Question 21High Yield
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
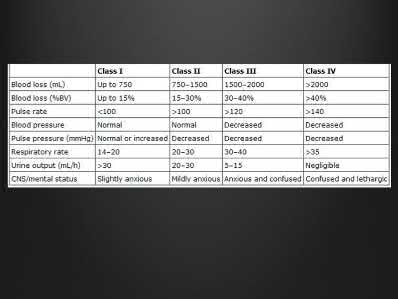
Explanation
Normal lactate levels or base excess indicate adequate tissue perfusion.
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 22High Yield
Figures 66a and 66b are the radiographs of a healthy 54-year-old right-hand-dominant man 3 months after he fell onto his outstretched left hand. He was initially treated with 8 weeks of closed reduction and casting. He reports ongoing ulnar-sided wrist pain, stiffness, and diminished function. An examination reveals a clinical sag deformity with a loss of radial length but no substantial swelling. The distal radius is nontender, and rotation is nearly full. Wrist motion is limited, with 55 degrees of flexion, 25 degrees of extension, and full digital motion. The most appropriate treatment is


Explanation
This patient has a substantial nascent malunion of his distal radius. Although a distal ulna excision would likely improve his ulnar-sided wrist pain, the Darrach procedure is more appropriate for older, somewhat less active individuals. In addition, the distal radius malunion is substantial, and it would be preferable to address the malunion given the major loss of radial length, inclination, and increased palmar tilt. The joint surface of the distal radius is uninvolved, and there is no evidence of arthrosis. It is preferable to osteotomize the distal radius sooner rather than later. Delayed osteotomy is often more difficult with more severe soft-tissue contractures, and improved results have been demonstrated following surgical treatment of nascent rather than mature distal radius malunions. Advantages include easier correction, no need for structural bone grafts, less overall total disability, and earlier return to work.
RECOMMENDED READINGS
30. Bilgin SS, Armangil M. Correction of nascent malunion of distal radius fractures. Acta Orthop Traumatol Turc. 2012;46(1):30-4. PubMed PMID: 22441449.
31. Jupiter JB, Ring D. A comparison of early and late reconstruction of malunited fractures of the distal end of the radius. J Bone Joint Surg Am. 1996 May;78(5):739-48. PubMed PMID: 8642031.
RECOMMENDED READINGS
30. Bilgin SS, Armangil M. Correction of nascent malunion of distal radius fractures. Acta Orthop Traumatol Turc. 2012;46(1):30-4. PubMed PMID: 22441449.
31. Jupiter JB, Ring D. A comparison of early and late reconstruction of malunited fractures of the distal end of the radius. J Bone Joint Surg Am. 1996 May;78(5):739-48. PubMed PMID: 8642031.
Question 23High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 24High Yield
Figures 15a and 15b are the radiographs of an active 65-year-old woman who has a 3-year history of increasing foot pain and flattening of the left foot. Inversion strength is 5+ and does not reproduce her symptoms. Bracing and nonsteroidal anti-inflammatory drugs have failed to provide adequate relief. She has a supple hindfoot and normal heel cord flexibility. What is the most appropriate treatment?
---
---


Explanation
The patient has a calcaneal fracture malunion, with symptomatic subtalar arthritis and anterior ankle and lateral subfibular impingement. Distraction subtalar arthrodesis addresses subtalar arthritis and anterior impingement and lateral wall ostectomy relieves symptoms of lateral impingement.The other procedures do not address all facets of the patient’s symptoms.
Question 25High Yield
-Figure 81 is the radiograph of a healthy 72-year-old man who has a 3-month history of medial knee pain.He denies any specific trauma. Until 3 months ago when the pain began, he had been an avid runner for many years. Initial treatment should be oral anti-inflammatory medication
Explanation
No detailed explanation provided for this question.
Question 26High Yield
Tourniquet use has been associated with increased pain post-operatively.
A 24-year-old male sustains the isolated injuries shown in Figures A and B during a high-speed motor vehicle accident. On physical examination, the overlying skin is intact and there is no evidence of a Morel-Lavallée lesion. Which of the following surgical techniques is considered to have the highest rate of fracture malreduction with this combined injury?
A 24-year-old male sustains the isolated injuries shown in Figures A and B during a high-speed motor vehicle accident. On physical examination, the overlying skin is intact and there is no evidence of a Morel-Lavallée lesion. Which of the following surgical techniques is considered to have the highest rate of fracture malreduction with this combined injury?









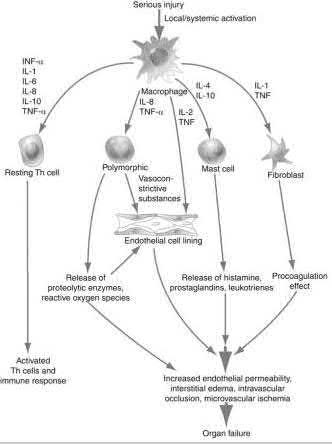



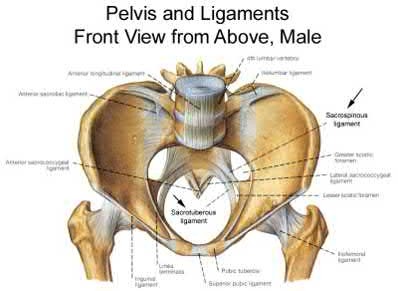

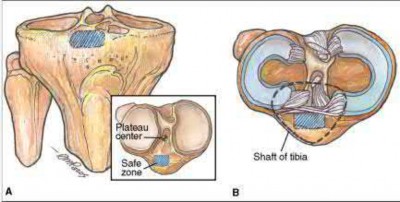
Explanation
Based on the radiographs shown, the patient has a comminuted trans-olecranon fracture dislocation of the elbow. Stability will be optimized with internal fixation in the form of a plating construct.
Trans-olecranon fracture dislocations often occur in the young secondary to high energy mechanisms. Direct blows often lead to high levels of comminution; the distal humerus is driven into the proximal ulna and olecranon, thereby leading to a concomitant dislocation. In this setting, the optimal treatment is use of a plate and screw fixation construct to provide mechanical stability.
Veillette et al. review the epidemiology, pathophysiology and treatment options for olecranon fractures. They highlight that because olecranon injuries involve the articular surface, fixation constructs should allow anatomic restoration of the joint surface. Additionally, fixation constructs should allow for early mobilization in order to prevent stiffness of the elbow.
Mortazavi et al. retrospectively reviewed eight patients who sustained anterior trans-olecranon fracture dislocations of the elbow. Based on their experience, they recommend use of plate fixation to optimize stability of the elbow.
Additionally, they indicate that satisfactory results can be obtained if the greater sigmoid notch is appropriately reduced.
Figures A and B show the AP and lateral radiographs of a trans-olecranon fracture dislocation of the elbow. Severe comminution of the olecranon can be seen on the lateral radiograph in Figure B.
Incorrect Answers:
Answers 1, 2, 4: K-wires alone would not provide optimal stability and allow for early motion. A tension-band construct or IM screw fixation is contraindicated with this degree of comminution.
: Use of cast immobilization would lead to high levels of stiffness and is not indicated for this patient.
A 25-year-old male sustained an isolated injury to his right foot after a fall from height. On examination, he has moderate swelling and pain over the dorsum of the foot. The overlying skin is intact. Radiographs of the foot are seen in Figures A and B. A CT scan image is seen Figures C. When consenting the patient for open reduction and internal fixation of this injury, what would you document as the most common complication?
1) Symptomatic implants
2) Subtalar arthritis
3) Tibiotalar arthritis
4) Malunion
5) Wound dehiscence
This patient has sustained a displaced talar neck fracture. The most common complication associated with this injury is post-traumatic arthritis of the subtalar and tibiotalar joint.
Talar neck fractures are the most common fracture of the talus. They occur most frequently during forced dorsiflexion of the foot with axial load. Displaced fractures are best treated with anatomic reduction and stable internal fixation.
Complications of surgery include nonunion or malunion, post-traumatic arthritis, infection, osteonecrosis, and secondary surgery. The prevalence of post-traumatic subtalar arthritis has been shown to be approximately 50-100% with these injuries.
Lindvall et al. examined a retrospective cohort of twenty-six displaced talar neck fractures that had been treated with open reduction and stable internal fixation. They reported that 26/26 fractures developed post-traumatic arthritis and pain within 48 months of follow-up after fixation. They concluded that post-traumatic arthritis is a more common complication than osteonecrosis following operative treatment.
Vallier et al retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p
A 23-year-old man presents with the injury seen in Figure A after a motor vehicle collision. He undergoes the treatment seen in Figure B. Which of the following statements is most accurate when comparing his treatment with open reduction and internal fixation?
1) Higher rates of radial nerve injury
2) Higher total complication rate
3) Lower rates of nonunion
4) Lower rates of shoulder impingement
5) Lower rates of malunion
Antegrade intramedullary (IM) nailing of humeral shaft fractures has been found to be associated with increased complication rates when compared with open reduction and internal fixation (ORIF).
Operative treatment of humeral shaft fractures remains controversial, with prospective randomized studies demonstrating small differences between IM nailing and ORIF.
Heineman et al. (2010) conducted a meta-analysis of prospective randomized studies comparing IM nailing with ORIF for humeral shaft fractures. The authors found no significant difference between the two treatment modalities for either their primary outcome (complications) or any of the secondary outcomes (nonunion, infection, nerve palsy, re-operation)
Heineman et al. (2012) have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of these newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF.
Figure A demonstrates a displaced, transverse humeral shaft fracture. Figure B demonstrates antegrade IM nailing of a humeral shaft fracture
Incorrect Answers:
Answer 1: Radial nerve injury has not been shown to be different between IM nailing and ORIF
Answer 3: No difference in union rates between the two modalities in prospective studies
Answer 4: Higher rates of shoulder impingement have been seen with IM nailing in some studies
Answer 5: No difference in rates of malunion between IM nailing and ORIF
Elevated interleukin 6 (IL-6) is most closely associated to which of the following clinical outcomes in orthopedic trauma patients?
1) Decreased mortality rates
2) Increased mortality rates
3) Decreased osteomyelitis infection rates
4) Increased rhabdomyolysis rates
5) Increased compartmental syndrome rates
Elevated levels of Interleukin 6 (IL-6) is most closely associated with higher injury severity scores and increased mortality rates in polytrauma orthopaedic patients.
Hyperstimulation of the inflammatory system by major trauma is considered to be the key element in the pathogenesis of severe inflammatory response syndrome and multi-organ dysfunction syndrome. IL-6 is a complex acute-reactant cytokinase that is expressed by cells in response to tissue injury. IL-6 levels are associated with injury severity, complications, and mortality.
Patients with the most severe injuries have the highest IL-6 serum levels.
Sears et al. reviewed the markers of inflammation in major trauma. They suggest that interleukin-6 and human leukocyte antigen-DR class II molecules appear to have the greatest potential for use in predicting the clinical course and outcome in trauma patients. Early identification of traumatic patients, based on inflammatory markers and genomic predisposition, could help to guide intervention and treatment.
Pape et al measured the perioperative concentrations of interleukin-6 in sixty-eight blunt trauma patients with non-life threatening pelvic fractures. Release of proinflammatory cytokines were higher in patients undergoing surgical procedures that cause increased blood loss. The release of markers seems to be related to the type and magnitude of surgery, rather than to the duration of the procedure.
Illustration A shows a diagram of the acute inflammatory response after major trauma
Incorrect Answers:
Answer 1: Mortality rates have shown to be increased with elevated levels of IL-6 in early trauma.
Answer 3: Osteomyelitis is a complication of open fracture trauma. Elevated levels of IL-6 and CRP are seen with this infection.
Answer 4: IL-6 is not commonly measured in rhabdomyolysis. Creatine kinase is commonly elevated with musculoskeletal injury.
Answer 5: Elevated IL-6 levels are not closely correlated with incidence incidence of compartmental syndrome.
A 26-year-old female sustained a closed femoral shaft fracture which was treated as shown in Figure A. She subsequently developed a painful oligotrophic nonunion and an exchange nailing was performed 6 months later. However, she has had persistent pain in the thigh since time of revision surgery seven months ago, but denies any fevers, chills, or night sweats. Current examination reveals a mildly tender right thigh with no obvious deformity. Laboratory studies for infectious markers are normal, but her radiograph in Figure B continues to show an oligotrophic nonunion. Which of the following factors has most likely contributed to her current presentation?
1) One pack of cigarettes per day for last 8 years
2) Positive intraoperative cultures for coagulase-negative Staphylococcus at the time of nail exchange
3) Iliac crest bone grafting at the time of nail exchange
4) Exchange nail was dynamically interlocked
5) A larger diameter nail was used in the exchange
The clinical presentation and radiographs are consisted with persistent oligotrophic non-union of the femur, after reamed nail exchange. Of the following factors, cigarette smoking has been shown to have the biggest effect on non-union in this population.
Reamed intramedullary nail exchange has become widely accepted as the treatment of choice for most diaphyseal femoral nonunions. The use of reamed exchange nailing are thought to allow for more biomechanical stability via larger diameter nails and improved biologics with bone reaming. These will help to generate bone healing and bridge fracture gaps. Smoking has been shown clinically and experimentally to affect union rate and fracture callus strength. Patients with femoral shaft non-unions should be forewarned of the its effect on fracture healing in nail exchange.
Hak et al retrospectively reviewed a cohort of 23 patients treated with reamed nail exchange for symptomatic femoral shaft non-unions. 15 of the patients were smokers and only 10 (66.7 percent) went on to heal after reamed nail exchange. This was in comparison to all 8 non-smoking patients who healed without complication after exchange reamed nailing. They suggest that smokers should be referred to an appropriate smoking cessation program before revision nail exchange is considered.
Figure A shows a proximal third femoral shaft fracture that was treated with intramedullary nailing. The oblique fracture line remains evident with a small callus response at the fracture site at 8 months post-operative. Figure B shows an radiograph of the exchange femoral nail 7 months after revision sugary.
There is increased fracture callus at fracture site, however the fracture line remains evident.
Incorrect Answers:
Answer 2: Intraoperative coagulase-negative staph. cultures are likely contaminant. The patient denies infectious symptoms and inflammatory markers for infection are negative. In addition, the radiographs do not suggest infection as there is no cortex irregularity, bone lysis, or implant loosening.
Answer 3: Bone grafting at the time of nail exchange has shown to increase bone union.
Answer 4: Dynamic interlocked screws were shown to increase bone union greater than static interlocked screws at the time nail exchange.
Answer 5: Bone grafting at the time of nail exchange has shown to increase bone union.
The sacrospinous and sacrotuberous ligaments are disrupted in which of the following injury patterns?
1) Ischial tuberosity avulsion fracture
2) Type I anterior-posterior compression pelvic ring injury
3) Type II lateral compression pelvic ring injury
4) Type II anterior-posterior compression pelvic ring injury
5) Both column acetabular fracture
Type II anterior-posterior compression (APC) pelvic ring injuries have disruption of the symphysis pubis, as well as disruption of the anterior SI ligaments, sacrotuberous ligament, and sacrospinous ligament. The alternative pattern of disruption of the pelvic floor ligaments is sometimes seen as an avulsion injury from the bony attachments of these structures (sacrum or ischium).
The progression of this pattern to involve the posterior SI joint ligaments creates a type III pattern, which is vertically and rotationally unstable.
Tile published a comprehensive review of pelvic ring injuries, focusing on the
anatomy and pathology of these injuries. He noted that the posterior SI complex is the most important to pelvic ring stability, which is the reason why these are generally classified by the grade of posterior injury. He also reminds the reader that these classification systems are not a substitute for individualized treatment decision making.
Illustration A shows an APC III pelvic ring injury, with significant symphyseal diastasis and SI joint widening. Illustration B shows the ligamentous anatomy of the pelvic ring.
Incorrect Answers:
Answer 1: These injuries are generally seen in sports-related trauma, with avulsion of the hamstring(s) from the ischium.
Answer 2: This injury pattern does not have any involvement of these two ligaments by definition.
Answer 3: This injury pattern involves inward rotation of the hemipelvis, thus protecting these structures. A type III LC injury may have a contralateral rupture of these ligaments, however.
Answer 5: This injury pattern typically does not involve rupture of these ligaments unless an ipsilateral pelvic ring injury is seen.
A 34-year-old man is involved in a motorcycle accident and sustains a closed tibia fracture and multiple rib fractures. A radiograph is provided in Figure A. During surgical treatment of this fracture, which of the following techniques will help facilitate a successful reduction and intramedullary fixation?
1) Hyperflexion to help prevent apex anterior angulation
2) A medial parapatellar incision to help prevent valgus angulation
3) Starting point just lateral to the medial tibial eminence to help prevent valgus angulation
4) A medially placed blocking screw to help prevent valgus angulation
5) Suprapatellar nailing technique to help prevent apex anterior angulation
The clinical scenario and radiograph demonstrate a proximal tibia fracture amenable to intramedullary nail fixation. The suprapatellar nailing technique helps prevent apex anterior or procurvatum deformity typical of these injuries.
Proximal third tibial shaft fractures are often difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. Many different techniques have been devised to overcome the deforming forces. These include (1) Poller blocking screws posterior and lateral to the intramedullary nail (IMN), (2) utilizing a semi-extended knee position during IMN of proximal tibia fractures, (3) use of a suprapatellar approach for IMN,
Trans-olecranon fracture dislocations often occur in the young secondary to high energy mechanisms. Direct blows often lead to high levels of comminution; the distal humerus is driven into the proximal ulna and olecranon, thereby leading to a concomitant dislocation. In this setting, the optimal treatment is use of a plate and screw fixation construct to provide mechanical stability.
Veillette et al. review the epidemiology, pathophysiology and treatment options for olecranon fractures. They highlight that because olecranon injuries involve the articular surface, fixation constructs should allow anatomic restoration of the joint surface. Additionally, fixation constructs should allow for early mobilization in order to prevent stiffness of the elbow.
Mortazavi et al. retrospectively reviewed eight patients who sustained anterior trans-olecranon fracture dislocations of the elbow. Based on their experience, they recommend use of plate fixation to optimize stability of the elbow.
Additionally, they indicate that satisfactory results can be obtained if the greater sigmoid notch is appropriately reduced.
Figures A and B show the AP and lateral radiographs of a trans-olecranon fracture dislocation of the elbow. Severe comminution of the olecranon can be seen on the lateral radiograph in Figure B.
Incorrect Answers:
Answers 1, 2, 4: K-wires alone would not provide optimal stability and allow for early motion. A tension-band construct or IM screw fixation is contraindicated with this degree of comminution.
: Use of cast immobilization would lead to high levels of stiffness and is not indicated for this patient.
A 25-year-old male sustained an isolated injury to his right foot after a fall from height. On examination, he has moderate swelling and pain over the dorsum of the foot. The overlying skin is intact. Radiographs of the foot are seen in Figures A and B. A CT scan image is seen Figures C. When consenting the patient for open reduction and internal fixation of this injury, what would you document as the most common complication?
1) Symptomatic implants
2) Subtalar arthritis
3) Tibiotalar arthritis
4) Malunion
5) Wound dehiscence
This patient has sustained a displaced talar neck fracture. The most common complication associated with this injury is post-traumatic arthritis of the subtalar and tibiotalar joint.
Talar neck fractures are the most common fracture of the talus. They occur most frequently during forced dorsiflexion of the foot with axial load. Displaced fractures are best treated with anatomic reduction and stable internal fixation.
Complications of surgery include nonunion or malunion, post-traumatic arthritis, infection, osteonecrosis, and secondary surgery. The prevalence of post-traumatic subtalar arthritis has been shown to be approximately 50-100% with these injuries.
Lindvall et al. examined a retrospective cohort of twenty-six displaced talar neck fractures that had been treated with open reduction and stable internal fixation. They reported that 26/26 fractures developed post-traumatic arthritis and pain within 48 months of follow-up after fixation. They concluded that post-traumatic arthritis is a more common complication than osteonecrosis following operative treatment.
Vallier et al retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p
A 23-year-old man presents with the injury seen in Figure A after a motor vehicle collision. He undergoes the treatment seen in Figure B. Which of the following statements is most accurate when comparing his treatment with open reduction and internal fixation?
1) Higher rates of radial nerve injury
2) Higher total complication rate
3) Lower rates of nonunion
4) Lower rates of shoulder impingement
5) Lower rates of malunion
Antegrade intramedullary (IM) nailing of humeral shaft fractures has been found to be associated with increased complication rates when compared with open reduction and internal fixation (ORIF).
Operative treatment of humeral shaft fractures remains controversial, with prospective randomized studies demonstrating small differences between IM nailing and ORIF.
Heineman et al. (2010) conducted a meta-analysis of prospective randomized studies comparing IM nailing with ORIF for humeral shaft fractures. The authors found no significant difference between the two treatment modalities for either their primary outcome (complications) or any of the secondary outcomes (nonunion, infection, nerve palsy, re-operation)
Heineman et al. (2012) have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of these newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF.
Figure A demonstrates a displaced, transverse humeral shaft fracture. Figure B demonstrates antegrade IM nailing of a humeral shaft fracture
Incorrect Answers:
Answer 1: Radial nerve injury has not been shown to be different between IM nailing and ORIF
Answer 3: No difference in union rates between the two modalities in prospective studies
Answer 4: Higher rates of shoulder impingement have been seen with IM nailing in some studies
Answer 5: No difference in rates of malunion between IM nailing and ORIF
Elevated interleukin 6 (IL-6) is most closely associated to which of the following clinical outcomes in orthopedic trauma patients?
1) Decreased mortality rates
2) Increased mortality rates
3) Decreased osteomyelitis infection rates
4) Increased rhabdomyolysis rates
5) Increased compartmental syndrome rates
Elevated levels of Interleukin 6 (IL-6) is most closely associated with higher injury severity scores and increased mortality rates in polytrauma orthopaedic patients.
Hyperstimulation of the inflammatory system by major trauma is considered to be the key element in the pathogenesis of severe inflammatory response syndrome and multi-organ dysfunction syndrome. IL-6 is a complex acute-reactant cytokinase that is expressed by cells in response to tissue injury. IL-6 levels are associated with injury severity, complications, and mortality.
Patients with the most severe injuries have the highest IL-6 serum levels.
Sears et al. reviewed the markers of inflammation in major trauma. They suggest that interleukin-6 and human leukocyte antigen-DR class II molecules appear to have the greatest potential for use in predicting the clinical course and outcome in trauma patients. Early identification of traumatic patients, based on inflammatory markers and genomic predisposition, could help to guide intervention and treatment.
Pape et al measured the perioperative concentrations of interleukin-6 in sixty-eight blunt trauma patients with non-life threatening pelvic fractures. Release of proinflammatory cytokines were higher in patients undergoing surgical procedures that cause increased blood loss. The release of markers seems to be related to the type and magnitude of surgery, rather than to the duration of the procedure.
Illustration A shows a diagram of the acute inflammatory response after major trauma
Incorrect Answers:
Answer 1: Mortality rates have shown to be increased with elevated levels of IL-6 in early trauma.
Answer 3: Osteomyelitis is a complication of open fracture trauma. Elevated levels of IL-6 and CRP are seen with this infection.
Answer 4: IL-6 is not commonly measured in rhabdomyolysis. Creatine kinase is commonly elevated with musculoskeletal injury.
Answer 5: Elevated IL-6 levels are not closely correlated with incidence incidence of compartmental syndrome.
A 26-year-old female sustained a closed femoral shaft fracture which was treated as shown in Figure A. She subsequently developed a painful oligotrophic nonunion and an exchange nailing was performed 6 months later. However, she has had persistent pain in the thigh since time of revision surgery seven months ago, but denies any fevers, chills, or night sweats. Current examination reveals a mildly tender right thigh with no obvious deformity. Laboratory studies for infectious markers are normal, but her radiograph in Figure B continues to show an oligotrophic nonunion. Which of the following factors has most likely contributed to her current presentation?
1) One pack of cigarettes per day for last 8 years
2) Positive intraoperative cultures for coagulase-negative Staphylococcus at the time of nail exchange
3) Iliac crest bone grafting at the time of nail exchange
4) Exchange nail was dynamically interlocked
5) A larger diameter nail was used in the exchange
The clinical presentation and radiographs are consisted with persistent oligotrophic non-union of the femur, after reamed nail exchange. Of the following factors, cigarette smoking has been shown to have the biggest effect on non-union in this population.
Reamed intramedullary nail exchange has become widely accepted as the treatment of choice for most diaphyseal femoral nonunions. The use of reamed exchange nailing are thought to allow for more biomechanical stability via larger diameter nails and improved biologics with bone reaming. These will help to generate bone healing and bridge fracture gaps. Smoking has been shown clinically and experimentally to affect union rate and fracture callus strength. Patients with femoral shaft non-unions should be forewarned of the its effect on fracture healing in nail exchange.
Hak et al retrospectively reviewed a cohort of 23 patients treated with reamed nail exchange for symptomatic femoral shaft non-unions. 15 of the patients were smokers and only 10 (66.7 percent) went on to heal after reamed nail exchange. This was in comparison to all 8 non-smoking patients who healed without complication after exchange reamed nailing. They suggest that smokers should be referred to an appropriate smoking cessation program before revision nail exchange is considered.
Figure A shows a proximal third femoral shaft fracture that was treated with intramedullary nailing. The oblique fracture line remains evident with a small callus response at the fracture site at 8 months post-operative. Figure B shows an radiograph of the exchange femoral nail 7 months after revision sugary.
There is increased fracture callus at fracture site, however the fracture line remains evident.
Incorrect Answers:
Answer 2: Intraoperative coagulase-negative staph. cultures are likely contaminant. The patient denies infectious symptoms and inflammatory markers for infection are negative. In addition, the radiographs do not suggest infection as there is no cortex irregularity, bone lysis, or implant loosening.
Answer 3: Bone grafting at the time of nail exchange has shown to increase bone union.
Answer 4: Dynamic interlocked screws were shown to increase bone union greater than static interlocked screws at the time nail exchange.
Answer 5: Bone grafting at the time of nail exchange has shown to increase bone union.
The sacrospinous and sacrotuberous ligaments are disrupted in which of the following injury patterns?
1) Ischial tuberosity avulsion fracture
2) Type I anterior-posterior compression pelvic ring injury
3) Type II lateral compression pelvic ring injury
4) Type II anterior-posterior compression pelvic ring injury
5) Both column acetabular fracture
Type II anterior-posterior compression (APC) pelvic ring injuries have disruption of the symphysis pubis, as well as disruption of the anterior SI ligaments, sacrotuberous ligament, and sacrospinous ligament. The alternative pattern of disruption of the pelvic floor ligaments is sometimes seen as an avulsion injury from the bony attachments of these structures (sacrum or ischium).
The progression of this pattern to involve the posterior SI joint ligaments creates a type III pattern, which is vertically and rotationally unstable.
Tile published a comprehensive review of pelvic ring injuries, focusing on the
anatomy and pathology of these injuries. He noted that the posterior SI complex is the most important to pelvic ring stability, which is the reason why these are generally classified by the grade of posterior injury. He also reminds the reader that these classification systems are not a substitute for individualized treatment decision making.
Illustration A shows an APC III pelvic ring injury, with significant symphyseal diastasis and SI joint widening. Illustration B shows the ligamentous anatomy of the pelvic ring.
Incorrect Answers:
Answer 1: These injuries are generally seen in sports-related trauma, with avulsion of the hamstring(s) from the ischium.
Answer 2: This injury pattern does not have any involvement of these two ligaments by definition.
Answer 3: This injury pattern involves inward rotation of the hemipelvis, thus protecting these structures. A type III LC injury may have a contralateral rupture of these ligaments, however.
Answer 5: This injury pattern typically does not involve rupture of these ligaments unless an ipsilateral pelvic ring injury is seen.
A 34-year-old man is involved in a motorcycle accident and sustains a closed tibia fracture and multiple rib fractures. A radiograph is provided in Figure A. During surgical treatment of this fracture, which of the following techniques will help facilitate a successful reduction and intramedullary fixation?
1) Hyperflexion to help prevent apex anterior angulation
2) A medial parapatellar incision to help prevent valgus angulation
3) Starting point just lateral to the medial tibial eminence to help prevent valgus angulation
4) A medially placed blocking screw to help prevent valgus angulation
5) Suprapatellar nailing technique to help prevent apex anterior angulation
The clinical scenario and radiograph demonstrate a proximal tibia fracture amenable to intramedullary nail fixation. The suprapatellar nailing technique helps prevent apex anterior or procurvatum deformity typical of these injuries.
Proximal third tibial shaft fractures are often difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. Many different techniques have been devised to overcome the deforming forces. These include (1) Poller blocking screws posterior and lateral to the intramedullary nail (IMN), (2) utilizing a semi-extended knee position during IMN of proximal tibia fractures, (3) use of a suprapatellar approach for IMN,
Question 27High Yield
Lyme disease is caused by which of the following organisms or mechanisms:
Explanation
Lyme disease was initially thought to be an idiopathic autoimmune disorder; however, in the 1970s, researchers at Yale University identified Borrelia burgdorferi as the cause of the disease. The disease is transmitted by a deer tick known as Ixodes ricinusi.
Group A streptococcal pharyngitis may be followed by rheumatic fever, but not Lyme disease.
Vibrio vulnificus is the organism responsible for severe soft tissue infections in patients who are exposed to fresh-water shellfish. Group B Streptococcus is a common etiologic agent for necrotizing fasciitis.
Group A streptococcal pharyngitis may be followed by rheumatic fever, but not Lyme disease.
Vibrio vulnificus is the organism responsible for severe soft tissue infections in patients who are exposed to fresh-water shellfish. Group B Streptococcus is a common etiologic agent for necrotizing fasciitis.
Question 28High Yield
In obstetric brachial plexus injury, return of which of the following muscle by 3 months is considered an indicator of plexus recovery:
Explanation
Biceps recovery at 3 months is considered the single most important indicator of recovery in obstetric plexus palsy.
Question 29High Yield
Disruption of which anatomic structure is necessary for the second-toe pathology to occur?
Explanation
- Plantar plate
Question 30High Yield
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of
Explanation
Arthroscopic capsular release is an effective means of treating stiffness that is the result of capsular contractures, such as in the case of a tight Bankart repair. Open release allows lengthening of a surgically shortened subscapularis, such as after a tight Putti-Platt repair. Additional physical therapy is unlikely to be effective because 8 months of treatment has failed to result in improvement. Accepting this degree of asymptomatic limited motion is not advisable because of the functional limitations for the patient and the increased risk of postoperative degenerative arthritis.
REFERENCES: Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
REFERENCES: Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 31High Yield
A 45-year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral
compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 32High Yield
Which of the following drugs is a selective estrogen receptor modulator:
Explanation
A new class of selective estrogen receptor modulator acts as an antagonist in breast tissue and an agonist in bone. Raloxifene selectively stimulates estrogen receptors in bone and is an antagonist in breast tissue.
Progestin used in conjunction with estrogen opposes the action of estrogen and lowers the risk of endometrial cancer that might occur with estrogen therapy alone.
Aredia, Fosamax, and alendronate are biphosphonates that inhibit osteoclasts, thereby decreasing bone resorption.Correct
Answer: Evista (raloxifene, Eli Lilly and Company)
Progestin used in conjunction with estrogen opposes the action of estrogen and lowers the risk of endometrial cancer that might occur with estrogen therapy alone.
Aredia, Fosamax, and alendronate are biphosphonates that inhibit osteoclasts, thereby decreasing bone resorption.Correct
Answer: Evista (raloxifene, Eli Lilly and Company)
Question 33High Yield
In an obese patient undergoing unicondylar knee arthroplasty (UKA):
Explanation
The knee should have less than 15° of deformity in varus or valgus and less than 10° flexion contracture. Inflammatory or crystalline-induced arthritis, knee subluxation, gross ligamentous laxity, and obesity are relative contraindications to the procedure. Scott and colleagues found that increased body weight contributed to failure in UKA and suggested that the best candidates are less than 180 lb
Question 34High Yield
The patient fails nonsurgical treatment for this condition. What is the best next step?
Explanation
Osgood-Schlatter disease is an apophysitis of the tibial tubercle. This condition is present in males more than females and occurs prior to fusion of the tubercle to the epiphysis of the tibia. The apophysis is cartilaginous before 11 years of age and begins to ossify between 11 and 14 years of age. The apophysis fuses to the epiphysis between 14 and 18 years of age (females before males). Symptoms are pain and swelling, and pain is worse with jumping and running. Initial treatment should consist of activity limitation, ice, quadriceps and hamstring stretching, and possible bracing. NSAIDs may be used to control symptoms. When symptoms resolve, the athlete may return to activities. In fewer than 10% of cases, symptoms persist after skeletal maturity. For these patients, excision of the ossicle will usually resolve symptoms. The ossicle is usually not part of the tendon attachment and can be resected without detaching any of the patellar tendon.
RECOMMENDED READINGS
1. [Vergara-Amador E, Davalos Herrera D, Moreno LÁ. Radiographic features of the development of the anterior tibial tuberosity. Radiologia. 2016 Feb 22. pii: S0033-8338(16)00019-9. doi: 10.1016/j.rx.2016.01.005. [Epub ahead of print] English, Spanish. PubMed PMID: 26917430. ](http://www.ncbi.nlm.nih.gov/pubmed/26917430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26917430)
2. [Frank JB, Jarit GJ, Bravman JT, Rosen JE. Lower extremity injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2007 Jun;15(6):356-66. Review. PubMed PMID: 17548885. ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548885)
RECOMMENDED READINGS
1. [Vergara-Amador E, Davalos Herrera D, Moreno LÁ. Radiographic features of the development of the anterior tibial tuberosity. Radiologia. 2016 Feb 22. pii: S0033-8338(16)00019-9. doi: 10.1016/j.rx.2016.01.005. [Epub ahead of print] English, Spanish. PubMed PMID: 26917430. ](http://www.ncbi.nlm.nih.gov/pubmed/26917430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26917430)
2. [Frank JB, Jarit GJ, Bravman JT, Rosen JE. Lower extremity injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2007 Jun;15(6):356-66. Review. PubMed PMID: 17548885. ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548885)
Question 35High Yield
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?
Explanation
The radiograph shows a bony avulsion of the ACL attachment site on the tibial spine in this skeletally immature patient. In this age group, injury often results in failure of the bony attachment site rather than the substance of the ligament. Avulsion of the patellar tendon insertion site can occur, but this structure is located at the apophysis of the tibial tubercle. The attachment site of the PCL is much more posterior. In adults, bony avulsion is more commonly associated with PCL injuries than with ACL injuries. When a small bony avulsion of the lateral capsule from the lateral tibial plateau is seen on the AP view, this finding is considered pathognomonic of an ACL injury (Segond sign) in adults. The area of the pes anserinus is anterior and distal; avulsion would be unusual.
REFERENCES: Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 406-432.
REFERENCES: Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 406-432.
Question 36High Yield
The second-toe deformity is most accurately described as
Explanation
- crossover toe.
Question 37High Yield
Figures 1 and 2 are the AP and lateral radiographs of a 5-year-old African-American boy who has a 1-month history of pain and swelling in his upper arm. His mother reports a medical history that includes sickle cell disease. Laboratory studies demonstrate elevated erythrocyte sedimentation rate and C-reactive protein level, and a white blood cell count of 17,000. What organism is most likely associated with this process in the patient?

Explanation
■
Although patients with sickle cell disease are at far higher risk of developing salmonella osteomyelitis than the general population, Staphylococcus aureus remains the most common organism causing osteomyelits in children of this age group.
■
Although patients with sickle cell disease are at far higher risk of developing salmonella osteomyelitis than the general population, Staphylococcus aureus remains the most common organism causing osteomyelits in children of this age group.
Question 38High Yield
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
DISCUSSION: The loss of hair or alopecia, is the only nonreversible effect of anabolic steroid use.
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 39High Yield
Which of the following genes has been shown to stimulate proteoglycan synthesis for prevention of disk degeneration:
Explanation
Intervertebral disk degeneration has been associated with a progressive decrease in proteoglycan content of nucleus pulposus. The potential application of gene therapy for prevention of disk degeneration is to increase or maintain the proteoglycan content of nucleus pulposus. Thompson and colleagues reported that addition of TGF-Ã1 to canine disk tissue in culture stimulated in vitro proteoglycan synthesis
Question 40High Yield
Figures 38a and 38b


Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23959223)
2. [Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. ](http://www.ncbi.nlm.nih.gov/pubmed/22465516)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22465516)
3. [Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22956165)
4. [Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. ](http://www.ncbi.nlm.nih.gov/pubmed/16330511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16330511)
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23959223)
2. [Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. ](http://www.ncbi.nlm.nih.gov/pubmed/22465516)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22465516)
3. [Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22956165)
4. [Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. ](http://www.ncbi.nlm.nih.gov/pubmed/16330511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16330511)
Question 41High Yield
Which of the following statements best characterizes a Dega osteotomy as a distinct osteotomy from a Salter osteotomy:
Explanation
The Dega osteotomy, originally described in Poland in 1964, is an incomplete transiliac osteotomy. The medial pelvic cortex is largely preserved, and the osteotomy hinges upon this point. Both osteotomies are best performed in young children, before triradiate cartilage closure. The Salter osteotomy is stabilized by pins, so the Dega needs no internal fixation. The Salter osteotomy lengthens the limb because it is a complete osteotomy.
Question 42High Yield
A 5-year-old boy has had a limp for the past 4 weeks with intermittent pain at the foot. He remains normally active and has no history of trauma. He has no fevers, rashes, or swelling. Examination reveals tenderness at the mid-dorsum of the foot medially. Radiographs are seen in Figures la and lb. Treatment should include which of the following?

Explanation
DISCUSSION: Osteochondrosis of the tarsal navicular is most commonly identified between the ages of 2 and 9 years. The condition is benign and self limited in nature. In patients with severe pain, a period of casting may be warranted, but otherwise management usually consists of observation or a supportive orthotic.
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
Question 43High Yield
A 24-year-old white man presents to the emergency department. He was bitten on his fist while fighting with another man. You notice teeth marks on the dorsum of the metacarpophalangeal (MC P) joint of the right middle finger. The bite does not appear to be deep because the joint is not exposed, and you can see the extensor tendon, which seems intact. The patient has active extension at the MC P joint. The wound is red and swollen, but there is no tenderness or redness on the volar aspect of the MC P joint. The patient has some limitation in range of motion. He is afebrile. Radiographs reveal air in the joint but no joint
dislocation or fracture, and there is no neurovascular deficit. All of the following are appropriate steps in the management of this patient except:
dislocation or fracture, and there is no neurovascular deficit. All of the following are appropriate steps in the management of this patient except:
Explanation
Human bite wounds on the hand are typically found over the MP joint. The mechanism of injury is a clenched-fist blow to the mouth. Oral flora enters the wound, which often communicates with the joint. Eikenella corrodens is frequently cultured from human bite wounds, but the most common pathogen is staphylococcus aureus. Appropriate treatment includes the administration of tetanus toxoid, exploration if there is air in the joint or frank infection, observation, intravenous antibiotics, arm elevation, and splinting. All bites over joints should be assumed to penetrate and require formal incision and drainage.
Question 44High Yield
Second-impact syndrome following a concussion






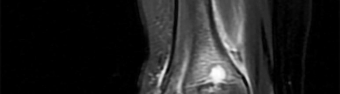
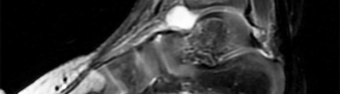
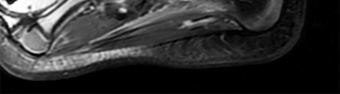
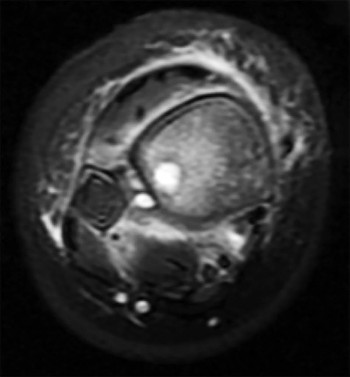
Explanation
According to several consensus statements, no child or adolescent athlete with a concussion should be allowed to return to play on the same day, regardless of severity. Second-impact syndrome refers to a second traumatic head injury that occurs while an athlete is still experiencing symptoms from the first injury. Young athletes are particularly vulnerable to second-impact syndrome. The mechanism by which this syndrome occurs likely is disruption of cerebral autoregulation, which may result in cerebral vascular congestion, diffuse brain swelling, and death.
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6a
Figure 6b
Figure 6c
RESPONSES FOR QUESTIONS 2 THROUGH 6
1. Curettage and/or grafting
2. Radiofrequency ablation
3. Intravenous (IV) antibiotics
4. Incision, drainage, and IV antibiotics
5. Neoadjuvant chemotherapy followed by surgical reconstruction
6. Observation alone
For each clinical vignette seen in the figures, select the best initial treatment from the list above.
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6a
Figure 6b
Figure 6c
RESPONSES FOR QUESTIONS 2 THROUGH 6
1. Curettage and/or grafting
2. Radiofrequency ablation
3. Intravenous (IV) antibiotics
4. Incision, drainage, and IV antibiotics
5. Neoadjuvant chemotherapy followed by surgical reconstruction
6. Observation alone
For each clinical vignette seen in the figures, select the best initial treatment from the list above.
Question 45High Yield
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
The axial MRI scan reveals a subluxated biceps tendon. In the study by Koh and associates, 85% of patients with a biceps subluxation on MRI were found to have a subscapularis tear at the time of arthroscopy. These are not always obvious on the MRI, and close inspection of the leading edge/upper border of the subscapularis tendon at the time of arthroscopy is necessary. Although supraspinatus tears, SLAP tears, and Bankart tears can all occur in conjunction with a biceps subluxation, none have been shown to be strongly correlated with this pathology, nor as specific to this pathology.
57
57
Question 46High Yield
A 15-year-old right-handed pitcher reports shoulder pain after throwing. His symptoms have been present for 3 months and have been getting progressively worse. Clinical examination shows no atrophy of the shoulder muscles, but he has pain with resisted motion of the shoulder, especially internal rotation. Radiographs are shown in Figures 73a and 73b. What is the next step in the evaluation and treatment of his shoulder pain?
Explanation
DISCUSSION: The patient has proximal humeral epiphyseolysis, otherwise known as “Little League shoulder.” This is an overuse injury of the shoulder in the skeletally immature overhead throwing athlete. Most frequently seen in pitchers, it usually develops after an increase in the amount or intensity of throwing activity. Initial treatment involves cessation of throwing activities so the proximal humeral growth plate injury can heal, followed by a gradual return to throwing.
REFERENCES: Chen FS, Diaz VA, Loebenberg M, et al: Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg 2005;13:172-185.
Keeley DW, Hackett T, Keims M, et al: A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop 2008;28:452-459.
Sabick MB, Kim YK, Torry MR, et al: Biomechanics of the shoulder in youth baseball pitchers:
Implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med 2005;33:1716-1722.
REFERENCES: Chen FS, Diaz VA, Loebenberg M, et al: Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg 2005;13:172-185.
Keeley DW, Hackett T, Keims M, et al: A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop 2008;28:452-459.
Sabick MB, Kim YK, Torry MR, et al: Biomechanics of the shoulder in youth baseball pitchers:
Implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med 2005;33:1716-1722.
Question 47High Yield
Figure 1 is the radiograph of a 49-year-old man who sustained a closed injury to his
left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---
left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---



Explanation
The fixation construct most likely failed due to a lack of inferomedial calcar support. Biomechanical and clinical studies have emphasized the importance of medial calcar support in preventing varus collapse. This can be accomplished in a number of ways, including anatomic reduction of the medial calcar, long locking screws that engage the inferomedial humeral head, or medial cortical reconstruction with a fibular strut.
The working length of the construct is not excessively long, and the plate length is sufficient. Though there remains a gap at the fracture site, the overall reduction is satisfactory and not the primary cause for fixation failure.
The working length of the construct is not excessively long, and the plate length is sufficient. Though there remains a gap at the fracture site, the overall reduction is satisfactory and not the primary cause for fixation failure.
Question 48High Yield
Which of the following statements is true regarding scoliosis in cerebral palsy (C P):
Explanation
C urves greater than 50° usually progress.
Scoliosis is most common in totally involved C P patients. Scoliosis is rare in patients with hemiplegia. Braces rarely halt curves in C P.
Surgery has no proven effect on prolonging life expectancy. The complication rate is higher in C P.
Scoliosis is most common in totally involved C P patients. Scoliosis is rare in patients with hemiplegia. Braces rarely halt curves in C P.
Surgery has no proven effect on prolonging life expectancy. The complication rate is higher in C P.
Question 49High Yield
What is the theoretical advantage of an open subpectoral technique of tenodesis of the long head of the biceps tendon compared to arthroscopic soft-tissue tenodesis techniques?

Explanation
DISCUSSION: A subpectoral biceps tenodesis requires an additional incision at the insertion of the pectoralis major tendon on the humerus. This can be difficult to do in the lateral decubitus position and certainly this technique does not decrease surgical time when compared to arthroscopic soft-tissue techniques. There have been no level I studies comparing the two techniques; however, the theoretical advantage of the open biceps subpectoral tenodesis is that the biceps tendon is removed from the bicipital groove, which may eliminate a source of pain in the biceps tendon.
REFERENCES: Mazzocca AD, Rios CG, Romeo AA, et al: Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy 2005;21:896.
Osbahr DC, Diamond AB, Speer KP: The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy 2002;18:483-487.
Figure 94
REFERENCES: Mazzocca AD, Rios CG, Romeo AA, et al: Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy 2005;21:896.
Osbahr DC, Diamond AB, Speer KP: The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy 2002;18:483-487.
Figure 94
Question 50High Yield
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
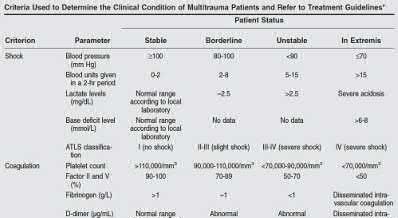
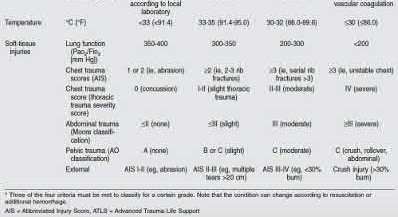
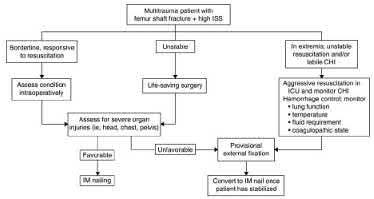











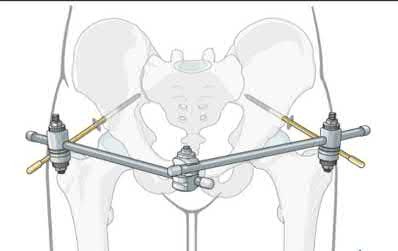









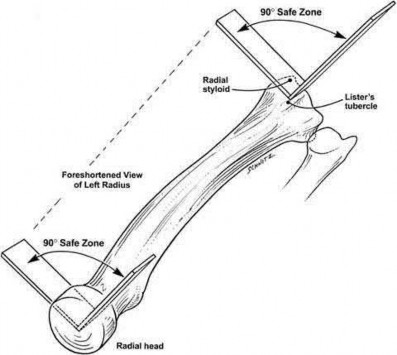


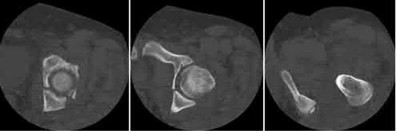

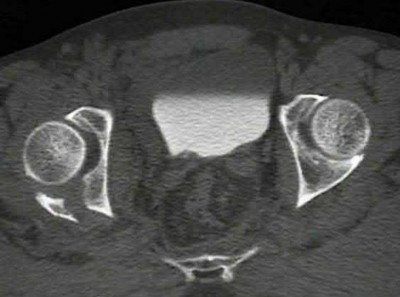













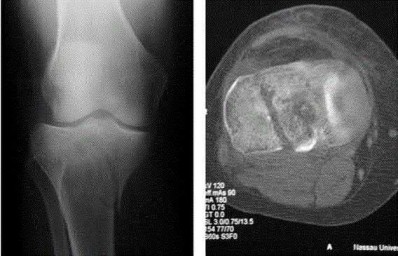
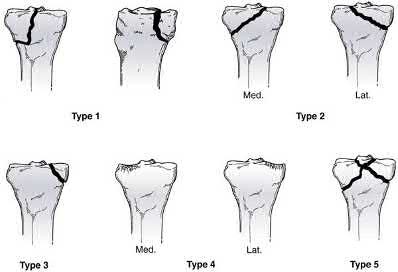
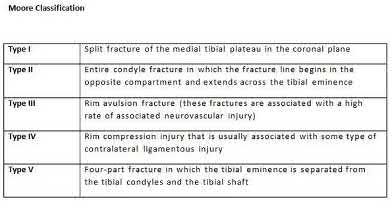















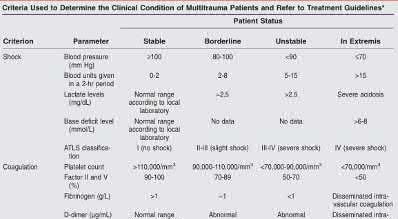
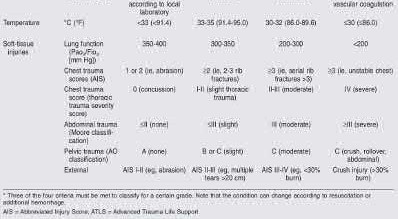


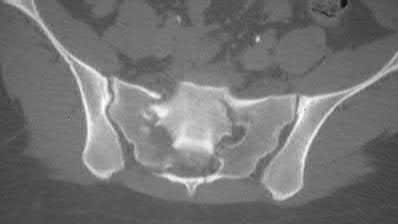
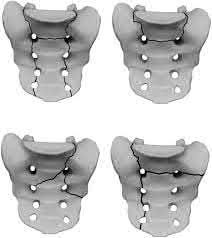






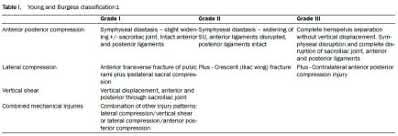




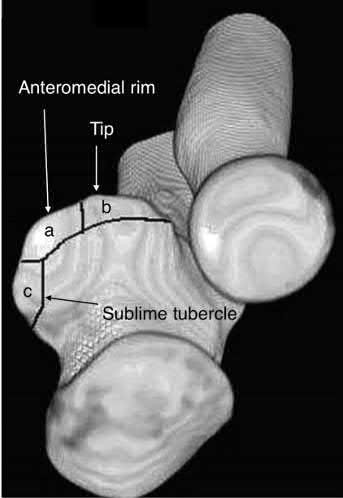


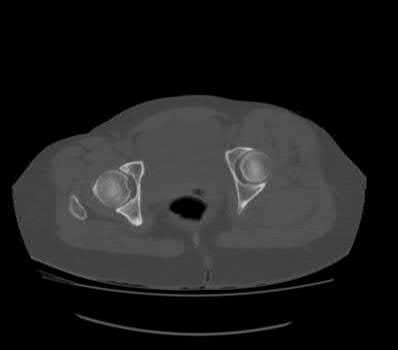



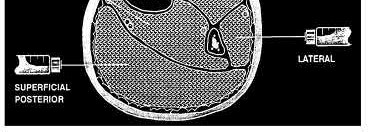


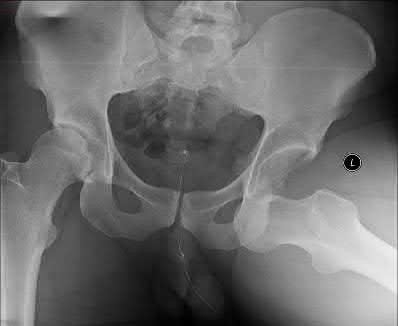


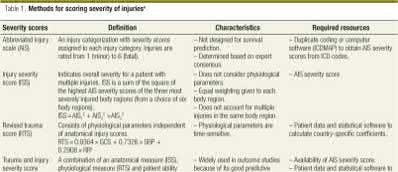








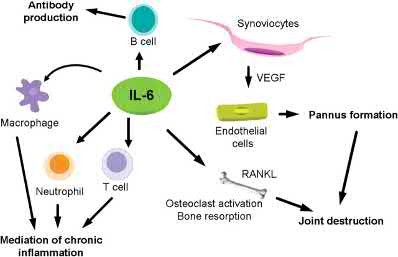
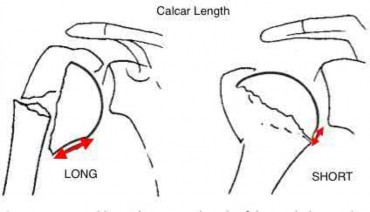
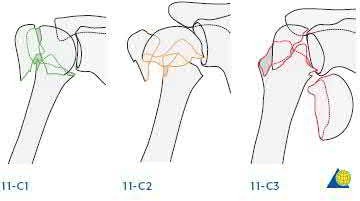
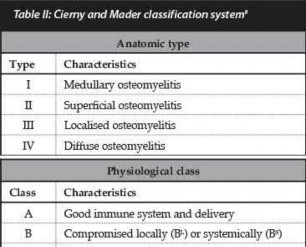
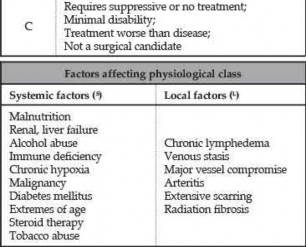
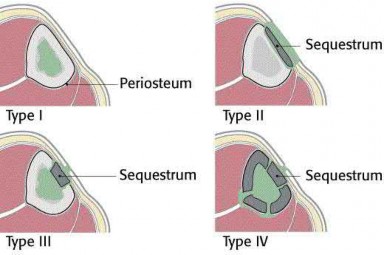










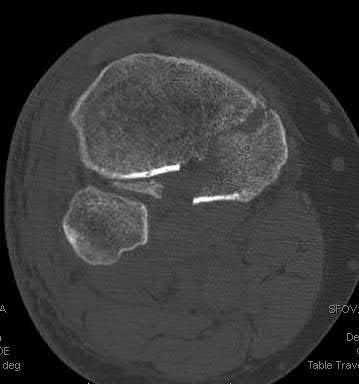


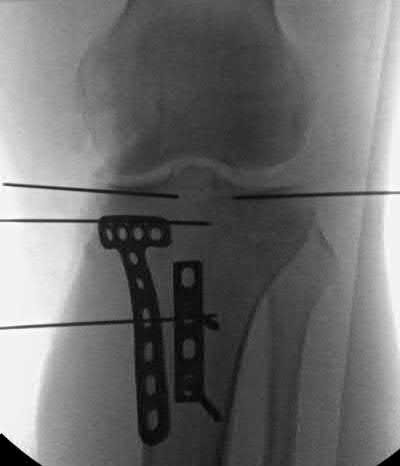



















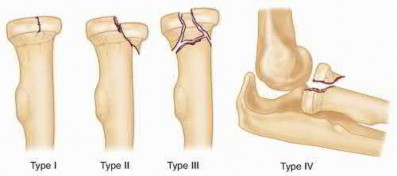
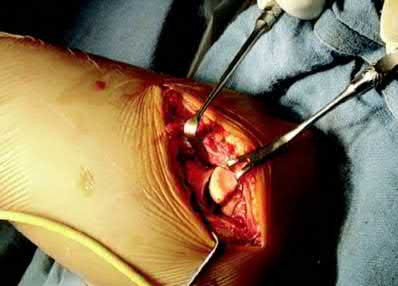

















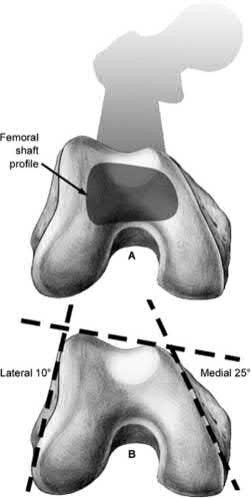





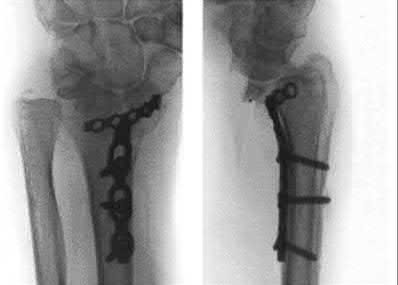







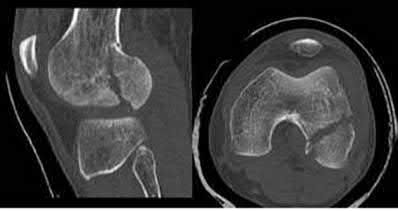


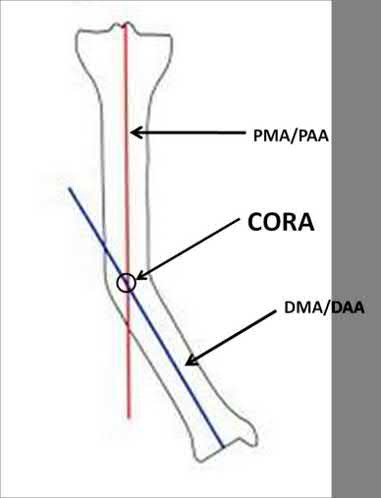



















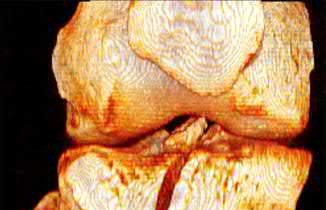












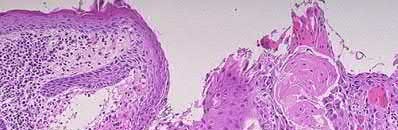
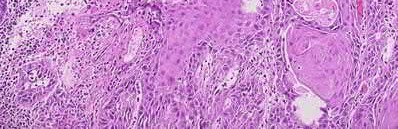
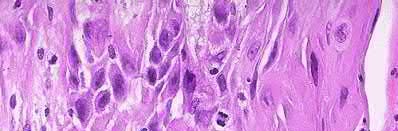









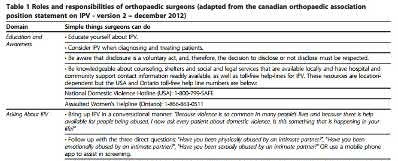
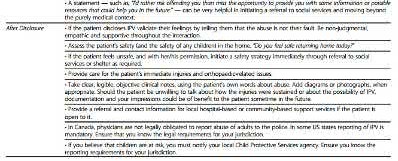










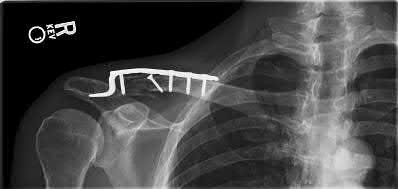

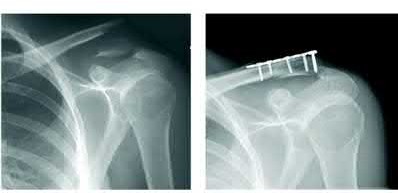
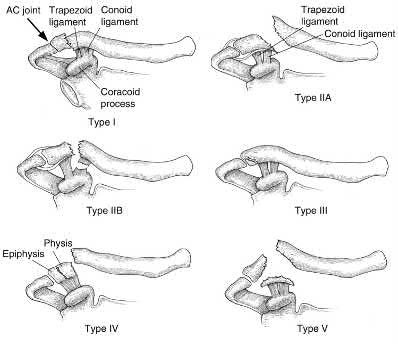
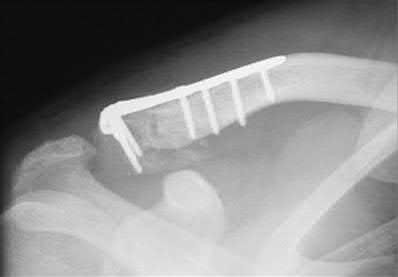


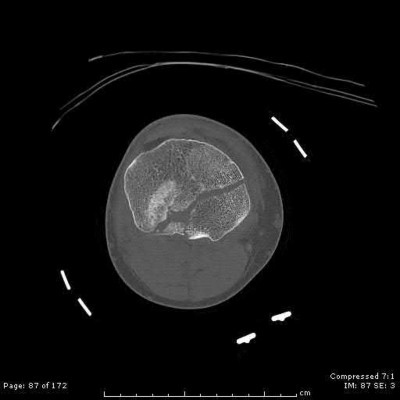
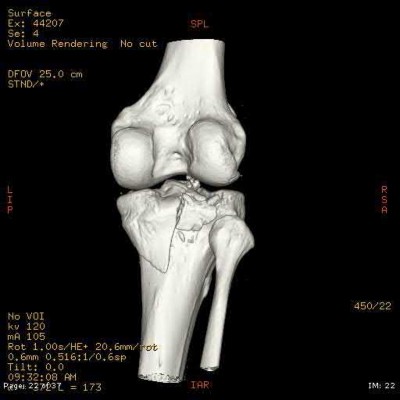




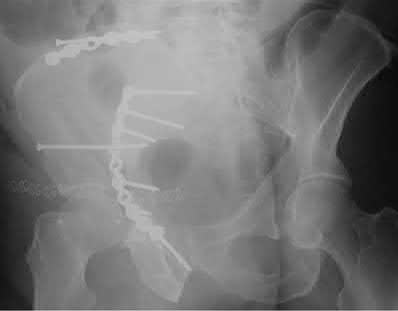
Explanation
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
. All displaced olecranon fractures should be considered for internal fixation. Displacement alone does not direct choice of implant.
Answer 2. Intra-articular extension is an indication for surgery to re-establish articular congruity but does not dictate implant selection.
Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown
Answer 4. This fracture is comminuted, without a distinct fracture line.
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?
1) Bilateral open reduction and internal fixation
2) Open reduction internal fixation on the right, reamed intramedullary nailing on the left
3) Temporizing external fixation on the right, open reduction and internal fixation on the left
4) Bilateral reamed intramedullary nailing
5) Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Answer 1-3: Open reduction internal fixation would not be indicated in damage control orthopaedics.
Answer 4: Bilateral reamed intramedullary nailing would be indicated in early total care of these injuries. As this patient is hemodynamically unstable, with a high injury severity score and bilateral lung contusions, damage control orthopaedics would be indicated.
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
1) Removal of locking screws
2) Removal of small fragment plates
3) Removal of metaphyseal implants
4) Removal of implants less than 1 year after insertion
5) Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:
Answer 1: Removal of locking screws does not increase the risk of refracture. Answer 2: Removal of large fragment plates (4.5mm) are at increased risk of refracture as compared to small fragment plates (3.5mm).
Answer 3: Metaphyseal implant removal has a decreased risk of refracture compared to diaphyseal implant removal.
Answer 5: Protective splinting for 6 weeks is all that is generally recommended for these patients.
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?
1) Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
2) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
3) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
4) Irrigation, debridement and placement external fixator right ankle, femur and tibia
5) Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
Answer 1: A pelvic binder would not be helpful in this scenario and actually may worsen the deformity.
Answer 2: Definitive plate fixation of the anterior pelvis will be needed, but only when the patient is adequately resuscitated.
Answer 3: An anterior external fixator may actually do more harm than good as it may require more time than placing skeletal traction, and also have difficulty controlling the posterior pelvis from the front.
Answer 5: Percutaneous SI screws may be placed later, once the patient is resuscitated and stable.
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?
1) Foot drop
2) Injury to the anterior tibial artery
3) Septic arthritis
4) Flexion contracture of the knee
5) Patellar tendon rupture
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
Answer 1: Foot drop would occur secondary to common peroneal nerve injury, which is not at risk with very proximal pin placement.
Answer 2: The anterior tibial artery is not at risk with very proximal pin placement.
Answer 4: The knee is free to move and therefore should not develop a flexion contracture secondary to the external fixator.
Answer 5: Patellar tendon rupture is not complication of external fixator pin placement in the tibia.
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
1) Radial nerve palsy
2) Intra-articular extension
3) 2mm fracture distraction, 5 degrees of rotational malignment
4) Ipsilateral proximal both bone forearm fracture
5) Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
Answer 1,2,3,5: These associated injuries are NOT an absolute indication for surgery. An area of controversy is the occurrence of new-onset radial nerve injuries after closed manipulation. However, the current algorithm does not support early open nerve exploration and fixation.
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
1) Posterior-stabilized total knee implant
2) Cruciate retaining total knee implant
3) Spiral fracture pattern
4) Distal femoral replacement
5) Knee flexion contracture of 15 degrees
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?
1) Full pronation
2) 25 degrees pronation
3) Neutral
4) 25 degrees supination
5) Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
1) Bilateral femur fractures
2) Rib fractures
3) Lactate of 5.2
4) Urine output of 20 cc/hr
5) Heart rate and blood pressure
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
Answer 1: Bilateral femur fractures are an indication to practice damage control orthopaedics and delay definitive fixation
Answers 3,4,5: All of these answers suggest that the patient is underresuscitated. Definitive fixation should be delayed
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
Answers 1,2,3, and 5: Posterior sided injuries, especially for these injuries, would probably be best approached via the Kocher-Langenback approach. Surgical dislocation with a trochanteric slide may help visualization in answer 1.
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?
1) Hand dominance
2) Angulation of fracture
3) Smoking
4) Early physical therapy
5) Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Answers 1,2,4: These factors do not have a significant influence on bone healing.
Answer 5: Diet has shown to improve bone healing but this does not have the greatest impact.
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?
1) Abduction brace for three weeks, followed by therapy
2) Right shoulder MR arthrogram
3) Open reduction and internal fixation
4) Hemiarthroplasty
5) Early range of motion
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
Answer 1: The GT fragment is displaced more than 5-10mm which would warrant surgical reduction and stabilization of the fracture.
Answer 2: MR arthrogram may be indicated to rule out an intra-capsular soft-tissue injury. However, this would not be warranted prior to fixation of the fracture.
Answer 4: Hemiarthroplasty would be indicated in some 4-part proximal humerus fractures or elderly patients. Considering this patient's age and valgus impaction of the fracture, ORIF would be most appropriate.
Answer 5: Early range of motion would be warranted AFTER fixation of the fracture.
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
1) Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
2) Left ASIS to mid-symphysis, right lateral window incision
3) Subumbilical incision
4) ASIS to ASIS bilaterally
5) Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
Answers 1,2: While these approaches may give access to the pelvic brim, each only give access to one side; one needs to circumferentially access and pack the pelvis.
Answer 4: An ASIS to ASIS skin incision is an unnecessary dissection with too many important structures that lie very close to the skin, including the femoral vessels.
Answer 5: A pararectus incision is an alternative approach to access the quadrilateral plate for acetabular fractures and does not play a role in pelvic packing.
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
1/.
1) 30-40%
2) 40-50%
3) >50%
This patient has likely lost 30-40% of his blood volume and is likely in stage III hemorrhagic shock on the basis of his heart rate, blood pressure, and urine output.
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal 100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
Answer 1: Schatzker II tibial plateau fractures can be treated with a single lateral plate.
Answer 2: Proximal third tibial shaft fractures can be treated with an intramedullary nail or percutaneous plating
Answer 3: Schatzker IV tibial plateau fractures can be treated with a single medial or posteromedial plate.
Answer 5: Tibial tubercle fractures in children can be treated with anterior to posterior screws.
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?
1) Immediate surgical intervention
2) Postoperative epidural analgesia
3) Postoperative antibiotics
4) Pre-operative medical optimization
5) Choosing total hip arthroplasty instead of hemiarthroplasty
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Answer 1: Most studies have shown an association between operative delay of
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
Answer 2: Post-operative epidural anaesthesia has shown to decrease postoperative delirium but does not affect 30-day mortality.
Answer 3: Postoperative antibiotics have not shown to reduce the 30-day mortality.
Answer 5: Total hip arthroplasty has shown to improved functional outcomes at 1 year compared with hemiarthroplasty. However, there has been no change in mortality.
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?
1) Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
2) Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
3) Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
4) Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
5) Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
Answer 1: A patient cannot do touch-down weight bearing on one side and non-weightbearing on the other side simultaneously.
Answer 3: The LC-I injury pattern is stable and can undergo immediate weightbearing as tolerated.
Answer 4: The LC-I pattern is stable and would allow immediate weightbearing, and the right pilon fracture would require non-weightbearing. Answer 5: The right pilon fracture would require non-weightbearing at this time.
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
1) Moore I
2) Moore II
3) Schatzker III
4) Schatzker V
5) OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:
Answer 1: Moore Type I is a coronal split fracture of the medial tibia plateau which displaces distally. It does not cross over to the contralateral side of the eminence.
Answer 3: Schatzker Type III is a pure lateral plateau depression.
Answer 4: Schatzker Type V is a bicondylar fracture where the metaphysis and diaphysis remain intact.
Answer 5: OTA type 41B3 is a partial articular fracture with a split-depression of the unilateral plateau.
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:
Answer 2: Vertical medial malleolar fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Juvenile Tillaux fractures occur typically in patients with open physes. They do not occur in patients with closed physes, and are not associated with tibial shaft fractures.
Answer 4: Spiral/oblique tibial shaft fractures are not associated with talus fractures.
Answer 5: Knee dislocations are considered high energy injuries, and are not associated with tibial shaft fractures.
What would be the most appropriate treatment for this patient at this time?
1) Observation only
2) Referral to physiotherapy
3) MRI spine and hip
4) Total hip arthroplasty
5) Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Answer 1: Symptomatic lateral femoral cortical stress fractures, known as "dreaded black lines", should be treated with early stabilization to prevent subtrochanteric fracture.
Answer 2: Referral to physiotherapy would not be indicated.
Answer 3: Symptoms are related to a subtrochanteric stress fracture, which has been identified on radiograph. MRI would not be indicated.
Answer 4: This patient has mild arthritis. Treatment with a long bridging femoral stem may stabilize the fracture, However, the gold standard treatment would be intramedullary nailing.
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?
1) Age greater than 70 years.
2) Fracture pattern in Figure A
3) Significant medical comorbidities.
4) Fracture pattern in Figure B
5) Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Answers 1, 2, 3, and 5 are all factors that would favor non-operative management for a proximal humerus fracture.
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?
1) HR >110
2) Bilateral pulmonary contusions seen on chest radiograph
3) SBP = 90mmHg
4) Unilateral femur fracture
5) Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Answer 1: Heart rate alone (even elevated severely) is not an indicator to
implement DCO.
Answer 3: A systolic BP of 90 mmHg is not an indicator to implement DCO. A SBP of 70mmHg or lower may indicate a patient in extremis (along with other parameters) indicating the benefits of DCO.
Answer 4: A unilateral femur fracture alone in a stable patient is not an indicator of DCO; a patient with bilateral femur fractures, however, may benefit from DCO.
Answer 5:A lactate of 2.5 mMol/L, while slightly elevated, does not warrant DCO. A lactate value of greater than 6 alone would indicate the need for DCO.
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?
1) Young-Burgess APC Type II
2) Young-Burgess LC Type I
3) "U" Type Spinopelvic Dissociation
4) Denis Zone-I
5) Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
Answer 1: APC Type II fractures do not classify fracture extensions into the sacral canal. The posterior SI ligaments are considered intact. There is usually disruption of sacrospinous and sacrotuberous ligaments.
Answer 2: LC Type I is an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture.
Answer 4,5: Figures A-C demonstrate a "U" type fracture of the sacrum.
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?
1) Ulnar neuropathy
2) Posterior interosseous nerve injury
3) Early loss of fixation
4) Elbow flexion contracture
5) Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:
Answers 1,2,3,5: All of these may be complications with this surgery. These complications are not as common as elbow contracture or stiffness.
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?
1) Chronic suppressive, culture-directed, antibiotic therapy
2) Above knee amputation
3) Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
4) Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
5) Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Answer 1: Chronic suppressive therapy would be considered in a patient that is unable to undergo surgical intervention
Answer 2: Amputation is a primary option for patients unable to undergo lengthy or multiple surgical interventions.
Answer 3: After removing the hardware, the fracture non-union will need to be stabilized.
Answer 5: This patients has a chronic infection that requires radical bone debridement and local infection control. The use of acute bone grafting in a single stage procedure in the distal 1/3 tibia (poor blood supply) is less ideal, especially in the setting of infection.
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?
1) Fracture classification
2) Number of blood transfusions in the first 24 hours
3) Gender
4) Time to operative fixation
5) Use of pelvic binders
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
Answers 1,3-5: Gender, fracture pattern, time to operative fixation or use of pelvic blinders do not correlate directly with mortality.
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?
1) Early range of motion
2) Hinged elbow brace for 4 weeks
3) Repair lateral collateral ligament
4) Remove and upsize implant
5) Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Answer 1: Early range of motion is supported after radial head arthroplasty. However, the next most appropriate step in this scenario would be the intraoperative assessment for radiohumeral joint overstuffing.
Answer 2: Hinged braces may be used in the post operative period. However, overstuffing the radiohumeral joint is of first priority.
Answer 3: There is no indication in this question for lateral collateral ligament repair
Answer 4: Removing the implant and upsizing the radial head would be the opposite of what is needed in this scenario.
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?
1) Medial only
2) Lateral only
3) Anterior and medial
4) Posterior and medial
5) Posterior and lateral
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
Answer 1: would prevent varus malalignment Answer 2: would prevent valgus malalignment alone
Answer 3: would prevent varus and recurvatum malalignment Answer 4: would prevent varus and procurvatum malalignment
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
1) A fracture of the radial head requiring ORIF
2) A highly comminuted radial head fracture requiring radial head arthroplasty or resection
3) An MCL injury requiring repair
4) A type I avulsion fracture of the coronoid
5) An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
Answers 1, 2, 3: Radial head fractures, and MCL injuries are not seen in varus/posteromedial mechanisms. They are seen in terrible triad elbow injuries which are due to valgus and posterolateral rotatory forces.
Answer 4: The coronoid fracture seen in these injuries is an anteromedial facet fracture, and not an avulsion fracture of the tip of the coronoid.
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?
1) Femoral skeletal traction
2) CT scan
3) Hip spica cast application
4) Observation only
5) Serial neurovascular examinations
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:
Answer 1: Femoral skeletal traction would be considered if there was an associated acetabular fracture or loose body.
Answer 3: Hip spica casts are not used with these injuries.
Answer 4: Observation would be considered after the CT scan is performed. Answer 5: There was no mention of neurovascular injury. This patient has a normal neurovascular examination. There is no fracture or risk of hematoma formation. This would not be necessary.
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?
1) MRI angiography of leg
2) Four-compartment fasciotomy
3) Follow-up examination the following day
4) Continued monitoring and serial examinations
5) EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) 30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
1) Repeat closed reduction under conscious sedation
2) Selective compartment fasciotomies
3) External fixation and compartment monitoring
4) 4-compartment fasciotomies with fracture fixation done emergently
5) Modify the cast to reposition the ankle into slight plantarflexion
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
Answers 1, 3: The stem does not suggest that the reduction was lost, so neither repeating a closed reduction or placement of an external fixator is indicated at this time.
Answers 2, 4: While suspicion should remain elevated for the development of compartment syndrome, simple conservative measures such as cast modification are ideal first steps to avoid onset of compartment syndrome. The clinical vignette given does not portray clinical compartment syndrome requiring emergent fasciotomy. It would be reasonable to maintain a high level of suspicion given the injury, but non-invasive cast modification is a simple, safe and quick first step.
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
Answers 2,3,4,5: Any pelvic or lower limb fracture can cause a disruption in a patients activities of daily living. This may include sexual dysfunction, for both men and women. The injury pattern that has the greatest potential for sexual dysfunction are APC type pelvic injuries.
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
1/. 18
1) 25
2) 33
3) 41
4) 48
This patients Injury Severity Score (ISS) is 41. In this patient, the highest AIS scores were from the head (AIS=4), abdomen (AIS=4) and pelvis (AIS=3).
Therefore, the calculation for the ISS score was 4^2 + 4^2 + 3^2 = 41.
The ISS score is calculated as the sum of the square values from the highest Abbreviated Injury Score [AIS] scores in the three most severely injured ISS body regions. ISS scores range from 1 to 75. A single score of 6 on any AIS region results in automatic score of 75. ISS scores > 15 are associated with mortality of 10%.
Poole et al. found that the AIS and ISS appropriately reflect the impact of extraskeletal injuries in patients with femur fractures, but they do not adequately reflect the increased morbidity associated with multiple lower extremity fractures.
Balogh et al. aimed to compare the scoring efficacy of the injury severity score (ISS) and the new injury severity score (NISS) in predicting post-injury outcomes. They found that multiple orthopaedic injuries, as used in the NISS system, had a significantly greater impact on reported poor post-injury outcomes. They suggest that NISS should replace the traditional ISS when grading trauma related outcomes.
Illustration A shows a table of the various ways to score injury severity in trauma patients.
Incorrect Answers:
Answers 1,2,3,5: ISS = A^2 + B^2 + C^2, where A, B, C are the AIS scores of the three most severely injured ISS body regions. The only correct answer is ISS=41.
A 60-year-old otherwise healthy female sustains the fracture in Figure A. Immediate surgical treatment would most likely prevent which of the following complications?
1) Malunion.
2) Regional osteopenia.
3) Skin necrosis.
4) Posttraumatic arthritis.
5) Refracture.
The patient has a calcaneal tuberosity fracture. The Achilles tendon is attached to the displaced fragment, which can cause soft tissue compromise and skin necrosis if not treated promptly.
Displaced calcaneal tuberosity and tongue-type calcaneus fractures have a high incidence of wound complications if not treated urgently. Recommended management includes surgical fixation often performed percutaneously. Lag screws are typically directed from the posterior superior tuberosity inferiorly and distal. In cases of skin sloughing and skin necrosis, flaps may be needed.
Gardner et al. reviewed 139 tongue-type calcaneus fractures, and found that 21% had some degree of posterior skin compromise. Additionally, there was a statistically significant increase in posterior skin compromise with delayed presentations.
Hess et al. reviewed 3 cases of calcaneal tuberosity avulsion fractures that let to skin necrosis because of a delay in treatment.
Tornetta reviewed the indications for percutenaous treatment of calcaneus fractures, and found it was successful and most useful in tongue-type calcaneus fractures.
Figure A shows a lateral radiograph of a R ankle showing a calcaneal tuberosity fracture. Illustration A shows an AP radiograph of a R ankle following percutaneous reduction and internal fixation of the calcaneus fracture with two cannulated screws. Illustration B shows a lateral radiograph of a R ankle showing interval reduction and fixation of the calcaneus fracture. Illustration C shows a clinical photograph of posterior skin compromise associated with a calcaneal tuberosity fracture.
Incorrect Answers:
Malunion, regional osteopenia, posttraumatic arthritis, and refracture risk would not be significantly altered with immediate surgical intervention as opposed to operative management within a reasonable time frame.
When elevating the joint surface in the injury pattern seen in Figure A, what material has the highest compressive strength when filling the metaphyseal void?
1) Calcium phosphate
2) Tricalcium phosphate
3) Cancellous autograft
4) Cancellous allograft
5) rhBMP-7
Figure A illustrates a depressed lateral tibial plateau. One of the key components of fixing a depressed articular segment is maintaining the reduction.
Trenholm et al reviewed an experimental study where a split depression (Schatzker II) fracture was created in a cadaveric model. The stiffness of the elevated fragment in cadavers using calcium phosphate cement versus cancellous bone graft as support showed no difference, but calcium phosphate cement was found to have greater compressive strength than cancellous bone alone.
The review article by Hak reviews the composition, advantages, and disadvantages of commerically available bone graft substitutes.
Incorrect answers:
2: Tricalcium phosphate is a bone graft substitute that is osteoconductive, but has less compressive strength.
3-4: Cancellous bone has less compressive strength than calcium phosphate. 5: rhBMP-7 is not used as a bone filling agent in this instance, as it is typically provided on a easily compressible collagen sponge.
A 42-year-old male sustains multiple abdominal injuries along with the fractures shown in Figures A and B. Which of the following factors is most useful to determine the patient's resuscitation and ability to undergo early definitive fixation of these two fractures?
1) Pulse pressure
2) Respiratory rate
3) Urine output
4) Platelet count
5) Base deficit
The base deficit, or lactate level, has been shown to best reflect the resuscitation status and survival after trauma.
Normalization of hemodynamic parameters does not accurately reflect the resuscitation status and a patient can be in compensated shock (occult tissue hypoperfusion) despite normalization of the heart rate and blood pressure. The use of temporizing measures with delayed definitive fracture treatment has been shown to decrease systemic complications in these patients with occult hypoperfusion.
Crowl et al. performed a retrospective study of 127 patients with femoral shaft fractures undergoing intramedullary nailing, assessing for occult hypoperfusion. Patients with occult hypoperfusion preoperatively had a twofold increase in postoperative complications and significant increase in postoperative infections.
Tisherman et al. present a review of hemodynamic parameters and their use in assessment of resuscitation. They report that hyperlactatemia is common among critically ill patients, and lactate levels and their trend may be reliable markers of illness severity and mortality. Therefore, measurement of blood lactate is recommended to stratify patients based on the need for fluid resuscitation and the risks of multiple organ dysfunction syndrome and death. They conclude that lactate is a reliable indicator of sepsis severity and a marker of resuscitation; however, it is an unreliable quantitative marker of tissue hypoxia/hypoperfusion.
Pallister et al. present a review of the effect of early stabilization of long bone fractures. They note that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure, both of which are caused by activation of the systemic inflammatory response. This activation results in tissue recruitment of and injury by circulating polymorphonuclear leukocytes.
Figure A is a radiograph showing a femoral shaft fracture, while Figure B shows an open tibial shaft fracture.
Incorrect Answers:
Answers 1-4: Normalization of these factors does not always predict adequate resuscitation.
Interleukin-6 levels have been shown to be a reliable measure of which of the following?
1) Osteoporosis
2) Severity of injury
3) Sarcomatous tumor burden
4) Bone turnover
5) Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production.
Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
A 31-year-old male sustained a displaced proximal humerus fracture after a motor vehicle accident. Which of the following factors has the lowest association with humeral head ischemia in these injuries?
1) Four-part fracture
2) Head-splitting fracture
3) Neck fracture with a long calcar segment
4) Disrupted medial periosteal hinge
5) AO type C3 fracture
A long calcar fracture segment, also known as the posteromedial metaphyseal head extension, is a good prognostic sign against the development of osteonecrosis in displaced proximal humerus fractures.
The humeral head is directly supplied by the anterior and posterior humeral circumflex arteries. Disruption of these vessels can result in humeral head osteonecrosis. Fracture patterns with long medial metaphyseal segments (greater than 8 mm) have not shown to critically disrupt the vascular supply to the humeral head causing osteonecrosis. Other factors shown to be protective against osteonecrosis after trauma include an intact medial hinge and simple fracture patterns.
Hertel et al. examined the factors predictive of osteonecrosis of the humeral
head after fracture. These include four-part fragments, angular displacement
>45 degrees of the head, displacement of the tuberosities greater than 10 mm, glenohumeral fracture-dislocation, and head-splitting fractures.
In Hertel's second paper and follow up study they noted that the initial post-fracture humeral head ischemia does not predict development of necrosis.
Illustration A shows an example of a long and short calcar fracture segment. Illustration B shows the AO classification of proximal humerus fractures.
Incorrect Answers:
Answers 1,2,4,5: All these factors are predictive of osteonecrosis.
A 50-year-old female has been diagnosed with osteomyelitis of her left tibia. The infection is isolated to the meduallary canal of the bone, and her past medical history is significant for heavy smoking and chronic venous stasis. Based on the clinical staging of osteomyelitis, what would be her Cierney-Mader classification?
1) Stage 2A
2) Stage 1B
3) Stage 1C
4) Stage 3B
5) Stage 4C
The Cierny-Mader classification is a clinical classification based on clinical and anatomic features. This patient's Cierny-Mader classification is Stage 1B.
The Cierney-Mader classification system characterizes osteomyelitis in one of four anatomic stages. Stage 1 is confined to the medullary cavity of the bone. Stage 2 involves only cortical bone. Stage 3 is a localized infection to cortical and medullary bone. However, the bone remains stable. Stage 4 involves the entire thickness of the bone, with loss of bone stability. The Cierny-Mader system also sub-characterizes patients as A, B, or C. The [A} patients have no systemic or local immune compromising factors. The [B] patients have one or more systemic or local compromising factors. The [C] patients are severely immunocompromised and treatment will lead to greater morbidity than the infection.
Mader et al. described the treatment algorithm of osteomyelitis using the Cierny-Mader classification. Treatment involves both antibiotic and surgical debridement. For type 1 infection, thorough intramedullary reaming and unroofing is usually performed.
Illustration A shows a table for the Cierny-Mader classification. Illustration B shows a schematic illustration of the anatomical involvement of osteomyelitis using the Cierny-Mader classification.
Incorrect Answers:
Answer 1: This would be a cortical infection only in a healthy patient. Answer 3: This would be a medullary cavity infection only in a severely compromised patient.
Answer 4: This would be a localized infection to cortical and medullary bone in a patient with one or more systemic or local compromising factors.
Answer 5: This would be a diffuse infection involving the entire bone in a severely compromised patient.
A 68-year-old female sustains a fall to her dominant arm and sustains the fracture seen in Figure A. She undergoes uneventful open reduction internal fixation with a locked plate and screw construct. Which of the following radiographs (Figures B, C, D, E, or F) show the most common complication associated with this treatment modality?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Figure B shows screw penetration of the articular surface, which is the most common complication following locked plate and screw fixation.
Inadequate fixation, typically in the humeral head, subsequently fails leading to varus deformity and screw penetration. This most commonly occurs in fixation for 3 and 4 part fractures, but can also occur following fixation for 2 part fractures.
Egol et al. retrospectively reviewed 51 patients following locked plating of 3-and 4-part proximal humerus fractures, they found 16% had screw penetration. The authors recommended ensuring appropriate number and length of the screws placed to prevent cut-out.
Brunner et al. reviewed 158 proximal humerus fractures. They found at 1 year follow-up noted 14% screw penetration rate. They recommended close followup to monitor for cut-out.
Figure A shows a 3-part proximal humerus fracture. Figure B exhibits varus cut-out and screw penetration. Figure C exhibits non-union and fixation failure. Figure D exhibits avascular necrosis and complete head collapse. Figure E (arrow) exhibits changes consistent with heterotopic ossification.
Figure F exhibits non-union and fixation failure at the level of the shaft.
Incorrect answers:
Answer choice 2/5 (figure C/F): Non-union and fixation failure can also occur, but at a relatively low rate.
Answer choice 3 (Figure D): Avascular necrosis also occurs, but at a lower rate than screw penetration.
Answer choice 4 (Figure E): Heterotopic ossification (arrow) can occur but is rare.
Figure A shows an acute, isolated and closed, left knee injury in a 40-year-old male struck by a motor vehicle. What would be the most
appropriate surgical fixation for this injury?
1) Definitive external fixation
2) Temporary external fixation then lateral percutaneous screws
3) Lateral nonlocking plate +/- bone graft substitutes
4) Medial and lateral locking plate +/- bone graft substitutes
5) Lateral percutaneous screws with assisted arthroscopy
This patient has sustained a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. The most appropriate treatment of this fracture would be fixation with a lateral nonlocking plate +/- bone graft substitute.
Displaced, widened and depressed tibia plateau fractures are an indication for operative intervention. The aim of surgery is to restore anatomic articular congruity, length, alignment and rotation of the proximal tibia. This is best achieved by (1) direct reduction of the articular surface, and (2) fixation of the interfragmentary piece with a plate and screw construct, which provides subarticular support, interfragmentary compression, and prevents shearing of the fracture. In patients with good bone quality, this is best achieved with an undercontoured lateral nonlocking plate in buttress mode.
Karunakar et al. showed that there was no significant difference between split depression tibial plateau fractures (Shatzker II) fixed with either (1) buttress plate with rafting screws versus (2) periarticular plate with built in rafting screw hole options.
Gardner et al. examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Figure A provided a sequence of coronal CT scan images of a left knee. There is a lateral split depression tibial plateau fracture with significant joint
depression, articular impaction and condylar widening.
Incorrect Answers:
Answer 1: Definitive external fixation of tibial plateau fractures may be considered in patients who are unable to tolerate definitive surgery, severe open fractures, infections, or significant bone loss.
Answer 2: Temporary external fixation would be considered in patients with significant soft tissue injury.
Answer 4: Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure. Medial plating would support a bicondylar fracture.
Answer 5: Screws alone are unlikely to be adequately stable in this patient. Although not commonly employed, knee arthroscopy is considered by some surgeons to be a valuable method to assist in obtaining the best articular surface reduction during surgery.
An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two non-locking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?
1) Absolute stability with direct healing by callus formation
2) Relative stability with indirect healing by callus formation
3) Absolute stability with direct healing by internal remodeling
4) Relative stability with indirect healing by internal remodeling
5) Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Restoration of the radial bow, length, and alignment in conjunction with primary bone healing would optimize the restoration of pronation/supination in the forearm. Compression plating and anatomic reduction of articular fractures are examples of absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting.
Moed et al. reviewed 56 patients with open diaphyseal forearm fractures treated with immediate internal fixation. The complications included deep infection in 2 patients and non-union in 6. This study indicated immediate stable plate fixation was a beneficial method of treatment for open diaphyseal forearm fractures.
Jones et al. discussed current literature on treating adult diaphyseal forearm fractures with open reduction internal fixation versus intramedullary nailing, and concluded a randomized prospective study is needed. They stated current literature is inconclusive.
Figure A shows a both bone forearm fracture fixed with absolute stability. The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Incorrect Answers:
Answers 1-2, 4-5: Absolute stability is a biological process of osteonal bone remodelling. This is predominantly intramembranous ossification. Enchondral bone formation occurs in non-rigid fracture healing (secondary bone healing).
A 27-year-old man sustains a tibial plateau fracture as pictured in Figure A-D. Which combination of fixation constructs and stability
would optimize his outcome?
1) Intramedullary nailing for a relative stability construct
2) Posteromedial buttress plating for an absolute stability construct
3) Locked lateral plating an absolute stability construct
4) Medial antiglide plating for a relative stability construct
5) Spanning external fixation for an absolute stability construct
Intraarticular tibial plateau fractures require absolute stability constructs to maintain anatomic joint reductions without callus formation. This condylar split fracture is ideally treated with buttress fixation at the apex of the fracture to avoid the high likelihood of shear failure with a laterally placed fixed-angle construct.
Tibial plateau fractures in young adults are high energy injuries, and the condylar split components of the fractures occur due to shear failure. The mechanism of failure - axial loading combined with a varus or valgus moment with the knee extended or flexed - dictates the orientation of the condylar split fracture line(s). There are multiple fracture classification schemes that assist with surgical decision making, particularly with placement of buttress plate fixation to resist shear failure. Articular impaction and joint depression must also be addressed.
Bai et al. performed a biomechanical study on fresh cadavers to simulate residual articular step-offs after fixation. With a >5 mm step-off, contact pressures increased over 200%.
AO guidelines of tibial plateau fracture management are discussed in depth in AO Principles of Fracture Management, and up-to-date principles can be found on the AO surgery reference. Anatomic reduction and absolute stability are important elements of all intraarticular proximal tibia fractures.
Figures A and B are injury films of a tibial plateau fracture with a large posterior split of the medial condyle. Figure C shows an axial CT cut displaying the same fracture. Illustrations A-C show how the injury was treated. Through a posterior incision, an under-contoured anti-glide plate was used to reduce the fracture at the apex. Subsequently, a pre-contoured posteromedial buttress plate was placed to maintain the reduction. The articular reduction was finalized with rafting screws outside of the plating construct to optimize the angle of subchondral support.
Incorrect Answers:
Answers 1, 4: Relative stability is inappropriate for intraarticular fractures that require anatomic reductions
Answer 3: Laterally-based locked plating for a medial condyle fracture creates large moments about the screw-plate interface, and the construct is apt to fail in shear
Answer 5: Spanning external fixation is most commonly used for temporizing tibial plateau fractures when significant soft tissue is present - in the absence of additional fixation for a hybrid construct, it would provide relative stability
Surgical fixation with absolute stability would be most appropriate for which of the following fracture patterns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Anatomic reduction and fixation with absolute stability is appropriate for articular fractures, such as posterior malleolar ankle fractures with significant joint involvement.
Compression plating and anatomic reduction of periarticular fractures yield absolute stability. Fractures treated with absolute stability achieve primary bone healing. Posterior malleolar ankle fractures comprising greater than 25% of the joint and non-comminuted lateral malleolar ankle fractures are typically treated with internal fixation to achieve absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting. In fractures with significant comminution and in lower extremity diaphyseal long bone fractures, relative stability is employed.
Gardner et al. surveyed members of the Orthopaedic Trauma Association (OTA) and American Orthopaedic Foot and Ankle Society (AOFAS) regarding treatment of posterior malleolus ankle fractures. They found that size influenced decision making, with 97% electing to treat those posterior malleolus fractures that comprised 50% of the joint. The most common used
approach was the posterolateral approach, which utilizes the interval between the flexor hallucis longus and peroneals.
Forsberger et al. reviewed 45 consecutive patients treated with surgical fixation of the posterior malleolus through the posterolateral approach. This approach allowed excellent exposure with few soft tissue complications.
De Vries et al. reviewed 45 patients with ankle fractures that had a posterior malleolar component. Those patients that had the posterior malleolar fragment fixed did not have statistically better functional scores than those who did not have the fragment fixed. They concluded that those patients with fragment sizes less than 25% did not require fixation and had good functional outcomes at 13 year follow-up.
Figure A shows an AP and lateral radiograph of a right comminuted distal third radial shaft fracture. Figure B shows an AP and lateral radiograph of a lateral and posterior malleolar ankle fracture in addition to a deltoid rupture. Figure C shows an AP and lateral radiograph of a comminuted middle third tibial shaft fracture. Figure D shows an AP radiograph of a minimally displaced greater trochanter fracture. Figure E shows an AP and lateral radiograph of a pediatric distal radial metaphyseal fracture. Illustration A shows an AP, mortise, and lateral radiograph of a posterior and lateral malleolus ankle fracture treated with open reduction and internal fixation.
Incorrect answers:
Answer 1: Significant comminuted radial shaft fractures are treated with bridge plating, which would achieve relative stability.
Answer 3: Diaphyseal tibial fractures are treated with intramedullary nailing, which achieves relative stability.
Answer 4: Minimally displaced greater trochanter fractures are treated nonoperatively.
Answer 5: Pediatric distal radius fractures are typically treated with closed reduction and casting, which achieves relative stability.
Figures A and B are radiographs of a 72-year-old male who presented to hospital 3 days after an unwitnessed fall. He presents with pain and the inability to mobilize since the fall. The patient lives independently and has no significant past medical history. Physical examination reveals an alert and oriented patient. This is an isolated injury with no other focal or systemic deficits. What would be the most important investigation to be obtained before taking this patient to the operating room?
1) Pelvic inlet and outlet views
2) CT head
3) Duplex ultrasound of both lower extremities
4) CT hip and pelvis
5) MRI hip and pelvis
The most appropriate investigation to order in this patient would be a duplex ultrasound of both lower extremities.
Immobilized elderly patients with a delay of more than two days from the fracture to presentation at the hospital are at a higher risk of deep-vein thrombosis (DVT). The risk can be higher in patients with factors that predispose to clot formation, such as malignancy. Patients with a delayed presentation to hospital should be investigated for DVT. The most common screening modality is duplex ultrasound of both lower extremities.
Hefley et al. looked at the effect of delayed admission to the hospital on the preoperative prevalence of DVT associated with hip fractures. They found that 6 out of 11 patients with a delay of more than two days between the fracture and admission to the hospital had evidence of thrombosis. They conclude all patients with delayed admission, after a hip fracture, should be evaluated for DVT preoperatively.
Figure A and B are AP and lateral radiographs that show a displaced left subcapital hip fracture.
Incorrect Answers:
Answer 1: There is no indication of pelvic inlet and out views. Generally speaking, pelvic inlet and outlet views assess the pelvic ring and pelvic bone stock, which are normal in this patient.
Answer 2: CT head would be indicated after an unwitnessed fall if the patient admitted to head injury, had neurological symptoms or acute focal/systemic deficits on exam. None of these are present in this patient.
Answer 4 and 5: A CT or MRI of the hip and pelvis are not indicated in a displaced fracture, but may be useful in diagnosing nondisplaced fractures.
A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?
1) Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
2) Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
3) Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
4) A delay in surgery greater than 48 hours is acceptable if the patient has multiple medical comorbiditiesm which are not fully optimized
5) Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months.
Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of early surgery on incidence of AVN. However, delay of internal fixation of more than 24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Answer 1: Patients treated with hemiarthroplasty or total hip arthroplasty
demonstrated no statistically significant difference in mortality.
Answer 2: Arthroplasty consistently has better outcomes compared to internal fixation for the treatment of unstable/displaced (Garden III and IV) femoral neck fractures in elderly patients.
Answer 3: Outcomes of unipolar and bipolar hemiarthroplasty for unstable femoral neck fractures are similar.
Answer 5: Dislocation rates are higher with total hip arthroplasty compared to hemiarthroplasty.
An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?
1) Intramedullary nail
2) Hemiarthroplasty
3) Closed reduction percutaneous pinning
4) Total hip arthroplasty
5) Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture
Incorrect answers:
Answers 1, 3, 5 are not the treatment standards for displaced femoral neck fractures in the elderly.
Answer 4 is incorrect because the patient is minimally ambulatory at baseline with little independence.
A 20-year-old female arrives to the trauma bay following a motor vehicle accident. She was a restrained driver and has bilateral chest tubes placed in the trauma slot. Initial laboratory values are significant for a hematocrit of 45.5 g/dL and a lactate of 7 mmol/L. Both lower extremities exhibit grossly open wounds. Radiographs are shown in Figure A and B. What is the best initial management of her orthopaedic injuries?
1) Irrigation and debridement of left femur and right tibia with bilateral external fixator placement
2) Irrigation and debridement of left femur and right tibia with left external fixator placement and right tibial intramedullary nail placement
3) Irrigation and debridement of left femur and right tibia with left femoral and right tibial intramedullary nail placement
4) Irrigation and debridement of left femur and right tibia with left femur open reduction and internal fixation and right tibial intramedullary nail placement
5) Irrigation and debridement of left femur and right tibia with bilateral long leg splint placement
Presenting as an unstable patient, damage control orthopaedics (DCO) should be performed by placing bilateral external fixators following irrigation and debridement.
Signs of clinical instability include an elevated lactate level as well as injuries to both lungs, necessitating bilateral chest tubes. Furthermore, while the patient is young and her hematocrit reflects a 'normal' number, more likely is a hypovolemic state due to bilateral open long bone injuries. Resuscitation is required and early total care (ETC) should be avoided.
Pape et al. review the early data regarding DCO and ETC. Identification of patients in extremis, borderline, unstable or stable patients is critical to determining appropriate management. Adequate resuscitation, by tracking lactate, as well as full evaluation of the multiply injured patient is crucial in determining application of DCO versus ETC. DCO is necessary as a temporizing stage to improve mortality in critically injured patients.
Renaldo and Egol revisit the evolution of trauma care where early, acute treatment evolved to ETC, and again to the development and implementation of DCO and staged fixation. Reviewing the initial post-traumatic inflammatory response, the authors review literature that supports the implementation of DCO in the unstable patient, especially the role of the 'second hit' phenomenon and the spike in inflammatory cascade that occurs between days 2-5 following injury.
Figure A is a lateral x-ray of a comminuted, displaced, open distal femur fracture. Figure B is an anteroposterior radiograph of a spiral, oblique, open tibia fracture.
Incorrect Answers:
Answers 2-4: Due to the elevated lactate levels and unstable nature of the patient, DCO should be applied via placement of external fixators. Definitive fixation at this time could worsen the patient's acute condition and subsequent
morbidity and mortality.
Answer 5: This patient, while unstable, is not in extremis, therefore temporary skeletal stabilization should be placed with external fixators.
Figure A is a radiograph of a 31-year-old male cyclist who was struck by a vehicle. Physical examination revealed a 2 cm opening in the skin over the anteromedial leg. He was treated operatively with an unreamed intramedullary nail. What outcome can be expected using this operative modality when compared with reamed intramedullary nailing?
1) Higher rates of nonunion
2) Higher rates of malunion
3) Higher rates of infection
4) Lower rates of infection
5) No difference
The best definitive surgical fixation option for an open fracture of the tibia would be either a reamed or unreamed intrameduallary nail.
Treatment of open tibia fractures require immediate antibiotics and early
irrigation and debridement. Surgical fixation options are vast, but largely based on the severity of injuries both locally or systemically. External fixation devices are mainly used for provisional fixation in polytrauma patients or definitively in proximal or distal metaphyseal fractures. Plating may be used in a staged fashion after a period of external fixation. The most common fixation method is intramedullary nailing. The use of a reamed or unreamed nail technique does not affect union rates, infection rates, or need for additional surgeries in open tibia fractures.
Bhandari et al conducted a multicenter, blinded randomized trial of 1319 adults in whom a tibial shaft fracture was treated with either reamed or unreamed intramedullary nailing. When comparing outcomes in open and closed injuries at twelve months, they found a benefit for reamed intramedullary nailing in patients with closed fractures, but found no difference between approaches in patients with open fractures.
Finkenmeier et al conducted a randomized controlled study of reamed vs. unreamed nails in open and closed tibia fractures (excluding Grades IIIB and IIIC). They found that the use of reamed insertion of IM nails for the treatment of closed tibia fractures lead to an earlier time to union without increased complications. The authors reported no differences in infection rate, compartment syndrome rate, or percent needing additional surgeries to obtain union. More secondary procedures were needed with unreamed nails in closed fractures only.
Figure A shows a mid-shaft tibia fracture. Incorrect Answers:
Answers 1, 2, 3, 4: All prospective studies show no difference in the rates of
non-union, malunion, or infection when using a reamed or unreamed nails to treat open tibia fractures.
A 27-year-old male presented to the trauma bay following a motor vehicle crash and was diagnosed with a comminuted open tibia fracture. He was subsequently treated with an irrigation and debridement, and un-reamed intramedullary nail. At 4 months followup, despite some signs of healing, the fracture is not fully united. Which of the following is true?
1) Patient should be scheduled for exchange nailing.
2) Use of an un-reamed nail increased this patients risk of infection.
3) Use of an un-reamed nail increased this patient's risk of non-union.
4) Patient should continue to be observed without intervention.
5) Use of an un-reamed nail decreased this patient's risk of infection.
Tibia fractures, open or closed, when treated with an intramedullary nail can take 6 months or longer to achieve clinical and radiographic healing, and should be observed for at least 6 months before secondary intervention is considered.
Open tibia fractures should be managed with debridement and irrigation initially. The choice of definitive fixation between reamed and unreamed nailing remains controversial. Recent randomized controlled studies have examined the outcomes of reamed and unreamed nailing for both closed and open tibia shaft fractures.
Bhandari et al. present a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. Surgeons participating in the study were mandated to delay intervention for delayed union/nonunion until 6 months after the initial procedure. The authors found that many tibia fractures in both the reamed and unreamed nailing groups progressed to union without secondary intervention with this 6 month delay.
Finkemeier et al. present a prospective randomized trial of tibia fractures treated with reamed or un-reamed intramedullary nails. For closed fractures they found a higher rate of union at 4 months in the reamed group, but no difference at 6 or 12 months. There was no difference in union rates for open fractures at any time point. They found no differences in other variables such as infection or compartment syndrome.
Incorrect answers:
Answer 1: This fracture has signs of healing at 4 months, and should continue to be observed until at least 6 months before a secondary operation is considered.
Answers 2 and 5: There is no difference in infection risk between reamed and un-reamed nails for open tibia fractures
Answer 3: There is no difference in rate of eventual union between reamed and un-reamed nails for open tibia fractures.
A 27-year-old male sustains a type I open both bone forearm fracture as seen in Figure A. During irrigation and debridement a 1 cm of cortex is removed leaving a segmental gap. Which of the following adjuvants is recommended to supplement your internal fixation?
1) Bone grafting
2) Tricalcium phosphate
3) Calcium phosphate
4) Calcium sulphate
5) BMP-3
Bone grafting in the primary fixation of fractures is typically limited to those with segmental defects. While the increased surface area of a comminuted fracture may aid in the healing potential, the segmental defect is a limiting factor to fracture healing. Calcium sulphate, tricalcium phosphate, BMP-3, and calcium phosphate are not indicated in this clinical picture. BMP-2,4,6, and 7 all have osteoinductive activity but BMP-3 does not demonstrate osteoinductive activity.
In their retrospective review of 198 fracture, Wright et. al found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental bone defect.
Wei et. al also performed a retrospective review of 64 fractures in 49 patients and found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental defect.
Finally, Schemitsch and Richards determined that optimal outcome post forearm fracture depends on restoration of the radial bow.
A 30-year-old female falls onto her outstretched arm and sustains the injury shown in Figures A and B. After intra-articular lidocaine injection, her elbow range of motion is 30°-95° extension/flexion, 45° supination, 65° pronation. There is no wrist tenderness and the radius pull test is symmetric to the contralateral forearm. What is the most appropriate treatment?
1) Fragment excision via the extensor carpi ulnaris / anconeus approach
2) Internal fixation with headless compression screws via the brachialis / pronator teres approach
3) Internal fixation with a periarticular plate via the extensor carpi ulnaris /
anconeus approach
4) Radial head arthroplasty via the brachialis / pronator teres approach
5) Sling and early elbow range of motion
This patient has a Mason type III radial head fracture composed of two articular fragments with a mechanical block to motion and should be treated with open reduction internal fixation (ORIF) using a lateral approach to the radial head.
Treatment of radial head fractures depends on fracture anatomy, elbow/forearm motion and ipsilateral forearm injury. Minimally displaced fractures with no mechanical block to motion (Type I; see Illustration C) are most common and are treated with a sling and early motion. Displaced fractures with one fragment (Type II) and block to motion are often managed with ORIF. Fragments less than ~30% of the articular surface may be excised, provided there is no concern for ipsilateral forearm instability. Displaced multi-fragmentary fractures (Type III) are usually managed with radial head arthroplasty, but may be treated with ORIF in young patients with less than three fragments.
Ring et al. performed a retrospective study of 56 patients who underwent radial head ORIF. Patients with more than three articular fragments had significantly poorer patient outcome scores, loss of forearm rotation and required more secondary procedures to ultimately resect the radial head. The authors concluded that ORIF is effective for fractures with less than three articular fragments and that fractures with three or more fragments are better managed with prosthetic replacement.
Ruchelsman et al. reviewed radial head and neck fractures. Choice of treatment is impacted by fragment number, size (percentage of articular disc), comminution and stability, as well as radiocapitellar alignment and block to motion. When feasible, ORIF allows restoration of anatomic congruity and initiation of early motion. Radial head arthroplasty is preferred for radial head fractures with multiple fragments or if stable fixation cannot be ensured.
Figures A and B are the AP and lateral radiographs of the left elbow showing a displaced complete articular radial head fracture with two articular fragments [Ruchelsman et al.]. Illustrations A and B are fluoroscopic images showing subsequent fixation of the fracture with a periarticular plate [Ruchelsman et al.]. Illustration C is the Mason classification of radial head fractures.
Illustration D is an intraoperative photograph showing exposure of the radial head fracture via the Kocher approach (extensor carpi ulnaris / anconeus
interval).
Incorrect Answers:
Answer 1: While the patient has no evidence of ipsilateral distal radioulnar joint or interosseous membrane injury (no wrist tenderness, normal radius pull test), fragment excision is reserved for partial articular fractures involving less than 30% of the articular surface. Complete radial head resection can lead to long-term elbow dysfunction and should be reserved for elderly, low-demand patients.
Answer 2: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. ORIF can be performed with either headless compression screws or periarticular plates. Use of headless compression screws has been associated with improved postoperative ROM compared to plates.
Answer 4: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. Radial head arthroplasty should be reserved for older patients and fractures with three or more articular fragments.
Answer 5: Nonoperative treatment is not appropriate for this patient with a displaced fracture and mechanical block to motion.
What nerve is most at risk when applying the external fixator shown in Figure A using a minimally invasive fluoroscopic technique of pin insertion?
1) Ilioinguinal nerve
2) Obturator nerve
3) First branch of the femoral nerve
4) Lateral femoral cutaneous nerve
5) Superior gluteal nerve
Pelvic external fixation with supraacetabular pins through the AIIS can be utilized to stabilize a pelvic fracture. While using this technique, care must be taken not to injure the lateral femoral cutaneous nerve (LFCN). Gardner et al describe the technique for placement of supraacetabular external fixation pins and state that pins in this location are more stable biomechanically compared to other locations in the iliac crest. Grothaus et al performed a cadaveric study to determine the anatomic detail and variation of the LFCN and the distances it traveled from various landmarks.The found the nerve to potentially be at risk as far as 7.3 cm medial to the anterior superior iliac spine along the inguinal ligament and as much as 11.3 cm distal on the sartorius muscle from the anterior superior iliac spine. Riina et al performed a cadaveric study to define the neurovascular structures at risk with the placement of anterior-posterior locking screws in the proximal femur. They found that risks to the neurovascular structures during anterior-posterior locking in the proximal femur are diminished if locking is performed above the level of the lesser trochanter.
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?
1) Sural nerve injury
2) Tethering of the flexor hallucis longus by fracture fragments
3) Medial plantar nerve neuropathy
4) Weakness of the tibialis posterior
5) Unrecognized foot compartment syndrome
Contracture of the intrinsic flexor muscles of the foot can be the result of unrecognized foot compartment syndrome. Foot compartment syndrome is a known complication of calcaneus fractures.
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal.
The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
A 25-year-old male sustains a closed elbow dislocation after falling during a soccer game. Two months later, the patient continues to complain of pain and instability. Radiographs and physical exam are concerning for posteromedial instability. Which of the following fracture patterns is most consistent with this diagnosis?
1) Coronoid tip
2) Coronoid anteromedial facet
3) Radial head
4) Olecranon
5) Capitellar impaction injury
of coronoid fractures, they indicate that identification of anteromedial facet injuries is often difficult and that treatment should be instituted promptly to limit persistent instability and subsequent arthritis.
Illustration A shows an AP radiograph of the affected elbow. An event of posteromedial instability is evidenced by the fracture through the anteromedial facet of the coronoid. Illustrations B and C show the AP and lateral radiographs of a patient who developed significant arthrosis after inadequate treatment of varus posteromedial rotatory instability.
Incorrect answers
Answers 1, 3, 5: These injuries may be seen as the sequlae of posterolateral rotatory instability.
Answer 4: Large coronoid fractures are seen in olecranon fracture-dislocations around the elbow.
A 7-year old boy presents to the emergency room following a ATV accident with complaints of left pelvic pain. In the emergency room he is alert and oriented and is hemodynamically stable. On physical exam he is unable to bear weight on his left lower extremity. There is no tenderness to palpation at the posterior pelvis. A radiograph is performed and shown in Figure A and CT examination shows the posterior ring is stable and age-appropriate. What is the most appropriate treatment for this injury pattern?
1) Nonoperative management with weight bearing as tolerated
2) Percutaneous sacroiliac screw
3) Pelvic external fixation
4) Anterior pelvic ring plating
5) Anterior and posterior pelvic ring plating
The clinical presentation is consistent for a mildly displaced parasymphyseal fracture in a pediatric patient with an open triradiate cartilage. Weight bearing as tolerated is the most appropriate treatment.
In skeletally immature pelvic ring fractures, the majority of cases can be treated nonoperatively. Open reduction and internal fixation is required for acetabular fractures with >2 mm of fracture displacement and for any intraarticular or triradiate cartilage fracture displacement >2 mm. External fixation is necessary for pelvic ring displacement of >2 cm to prevent limb-length discrepancies.
Holden et al. emphasize that children with open triradiate cartilage have
different fracture patterns than do children whose triradiate cartilage has closed. They report because of the immaturity of the pelvis, the iliac wing is weaker than the elastic pelvic ligaments, resulting in bone failure before pelvic ring disruption has a chance to occur. For this reason fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment.
Spiguel et al. reviewed 2850 pediatric trauma admissions at their institution and reviewed cases with a pelvic ring fracture. They found that although pelvic fractures are an uncommon injury in pediatric trauma patients, the morbidity associated with these injuries is significant. They report while the majority of pelvic fractures in children are treated nonoperatively, more than one-half of these patients have concomitant injuries requiring operative management.
Figure A shows an inferior rami fracture in a pediatric patient with an open triradiate cartilage.
Incorrect Answers:
Answers 1,3,4,5: These treatment options are not appropriate in a stable pelvic ring fracture in a child with open triradiate cartilage.
A 75-year-old-male presents after being struck by a vehicle while crossing the street. He complains of right leg pain, and physical exam reveals no evidence of an open fracture. Initial radiographs are shown in Figures A and B, and intramedullary nailing of the fracture is planned. What is the proper blocking screw technique to prevent apex anterior and valgus deformity of the fracture?
1) Insertion of blocking screws lateral and posterior to the nail
2) Insertion of blocking screws medial and posterior to the nail
3) Insertion of blocking screws lateral and anterior to the nail
4) Insertion of blocking screws medial and anterior to the nail
5) Insertion of blocking screws medial, lateral, and posterior to the nail
Apex anterior and valgus deformity of the proximal tibia fracture can be prevented by inserting blocking screws lateral and posterior to the nail in the proximal segment.
Blocking screws may be used to prevent deformity when performing intramedullary fixation of proximal tibia fractures. Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to prevent valgus deformity. Stability screws can be placed prior to insertion of the nail to prevent deformity during nail passage, or after nail insertion to prevent postoperative deformity from developing.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibial shaft. Post-operatively, all patients in their series had less than 5 degrees
of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Figures A and B demonstrate a segmental tibial shaft fracture. Illustration A shows an intraoperative fluoroscopic image demonstrating insertion of the blocking screws intraoperatively. Illustrations B and C show post-operative radiographs demonstrating placement of the blocking screws and adequate alignment of the proximal segment.
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. As an alternative to lactate and base deficit measurements, which of the following would best indicate adequate resuscitation has been achieved?
1) Systolic blood pressure > 120
2) Heart rate between 60-100
3) Urine output equals 0.4 cc/kg/hr
4) Gastric intramucosal pH of 7.4
5) Potassium between 3.5-4.5
Of the following variables, only a normal gastric mucosal pH (>7.3) is associated with restoration of tissue oxygenation.
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism
with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Answers 1-3: A patient may have normalized blood pressure, heart rate, and urine output but may still be in a state of compensated shock requiring further resuscitation.
Answer 5: Potassium levels do not assess adequate resuscitation
A 32-year-old man sustains the knee injury seen in Figure A after falling from a ladder. Which of the following options is the most biomechanically stable and appropriate definitive surgical treatment?
1) Spanning knee external fixation
2) Lateral plateau locking plate
3) Posteromedial locking plate
4) Lateral plateau percutaneous lag screws and posteromedial plate
5) Lateral plateau and posteromedial plating
The above clinical scenario is consistent with a bicondylar tibial plateau fracture. Bicondylar tibial plateau fractures are best definitively treated with dual incision technique using separate lateral plateau and posteromedial plates.
Yoo et al perfored a biomechanical study comparing locking and nonlocking single and dual plating constructs in maintaining posteromedial fragment reduction in a bicondylar tibial plateau fractures. They found that the posteromedial fracture fragment tolerated higher loads with a posteromedial conventional plate construct. The superiority of this dual plating construct may be caused by unreliable penetration of the posteromedial fragment by the lateral locking screws alone.
Zeng et al also performed a biomechanical study comparing the biomechanical strength of four different fixation methods for the posteromedial tibial plateau split fracture. The four following constructs: anteroposterior lag-screws, an anteromedial limited contact dynamic compression plate (LC-DCP), a lateral locking plate, or a posterior T-shaped buttress plate were studied. They found that the posterior-based buttress plating technique was the most biomechanically stable fixation method allowing the least amount of fracture subsidence for posteromedial split tibial plateau fractures.
Figure A shows an AP radiograph of a bicondylar tibial plateau. Illustration A shows a post-operative radiograph following the dual-plating technique for bicondylar tibial plateau fractures.
Incorrect answers:
Answer 1: External fixation is not the most appropriate definitive care for bicondylar tibial plateau fractures.
Answers 2-4: Not as biomechanically stable as dual plating technique for bicondylar tibial plateau fractures.
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?
1) Intraoperative anterior compartment measurement of 29, with preoperative diastolic pressure 58
2) Preoperative anterior compartment measurement of 25, with preoperative diastolic pressure of 60
3) Intraoperative anterior compartment measurement of 25, with intraoperative diastolic pressure of 54
4) Intraoperative anterior compartment measurement of 28, with intraoperative diastolic pressure of 72
5) Preoperative anterior compartment measurement of 22, with mean arterial pressure of 70
A delta P (diastolic blood pressure minus compartment pressure measurement)of
A 44-year-old male is involved in a motorcycle collision and presents with the radiographs shown in Figure A. A CT scan is obtained which shows intra-articular extension of the fracture, and lateral locked plating with intercondylar lag screw fixation is planned. Which of the following is important intra-operatively to ensure that the
intercondylar screws are contained within the bone and are of appropriate length?
1) AP fluoroscopic imaging with the leg in 30 degrees of internal rotation
2) AP fluoroscopic imaging with the leg in 30 degrees of external rotation
3) AP fluoroscopic imaging with the knee in full extension
4) Lateral fluoroscopic imaging with the knee in 30 degrees of internal rotation
5) Lateral fluoroscopic imaging with the knee in 15 degrees of flexion
Figure A illustrates a comminuted distal femur fracture. AP fluoroscopic imaging with the leg in 30 degrees of internal rotation is important to prevent intercondylar screw prominence.
Hardware irritation is a common post-operative complication of distal femoral plate fixation. Two common sites of pain are laterally where the iliotibial band is in contact with the plate, and medially where intercondylar screws may penetrate the cortex if they are of inappropriate length. Iliotibial irritation most commonly presents with activities requiring knee flexion and extension. It is important to remember that the lateral metaphysis of the distal femur is angulated 10 degrees from the sagittal plane, and the medial metaphysis is angulated 25 degrees from the sagittal plane. Therefore, if a straight AP view is obtained, a distal screw can appear to be inside the bone even if it is too long. In order to assess the exact length of the screw, one must obtain an AP view with 30° internal rotation of the lower extremity.
Gwathmey et al discuss distal femoral fractures in their review article. They state that the goal of surgical management is to promote early knee motion while restoring the articular surface, maintaining limb length and alignment,
and preserving the soft-tissue envelope with a durable fixation that allows functional recovery during bone healing. They describe a variety of surgical exposures, techniques, and implants developed to treat these injuries, including intramedullary nailing, screw fixation, and periarticular locked plating, possibly augmented with bone fillers.
Illustration A demonstrates the sagittal plane angulation of the medial and lateral cortex of the distal femur. Illustration B shows a knee in external rotation, with the intercondylar screw appearing to be of appropriate length. Illustration C shows the knee in internal rotation, which indicates that the screw is penetrating the medial cortex.
A 68-year-old male falls onto his outstretched hand and suffers the injury shown in Figures A and B. He undergoes operative treatment of his fracture, and immediate post-op radiographs are shown in Figure C. Two weeks later he presents with significantly increased pain and deformity. He denies any new trauma, and has followed all postoperative activity restrictions. Current radiographs are shown in Figure D and a clinical photograph of the affected wrist is shown in Figure E. Which of the following is the most likely cause for failure of fixation in this patient?
1) Failure to support the lunate facet with fragment specific fixation
2) Use of a non-locking plate
3) Lack of volar tilt restoration
4) Lack of radial styloid column plating
5) Use of only three bicortical screws in the intact radial shaft proximally
The failure of this patient's fixation post-operatively is caused by failure to support the lunate-facet fragment noted on the injury radiographs.
The stability of comminuted fractures of the distal part of the radius with volar fragmentation is determined not only by the reduction of the major fragments but also by the reduction of the small volar lunate fragment. The distal volar lunate fragment is the site of origin of the strong volar radiolunate ligaments which insert onto the lunate, and so displacement of this small piece volarly will allow the lunate and the rest of the carpus to subluxate volarly. The unique anatomy of this fragment may prevent standard fixation devices for distal radial fractures from supporting the entire volar surface effectively, as a standard volar plate cannot capture this small distal piece without risking injury to the flexor tendons. Fragment specific fixation of the volar lunate facet fragment with commercially available small plates, or with a tension-band construct or augmentation with K-wires may be required to reduce and stabilize this fragment.
Harness et al. reported on a cohort of 7 patients with a volar shearing fracture of the distal radius who lost fixation of a volar lunate facet fragment with subsequent carpal displacement after open reduction and internal fixation. Five patients underwent revision surgery with adequate results. The authors concluded that with regards to lunate facet fracture fragments, it is preferable to recognize the complexity of the injury prior to the initial surgical intervention and to plan accordingly to prevent early post-operative failure.
Taylor et al. compared the biomechanical stability of a fixed-angle volar plate versus a fragment specific fixation system in the treatment of an intraarticular, dorsally comminuted distal radius fracture model. They found that both fixed-angle volar plate and fragment-specific fixation systems performed comparably in a simulated early postoperative motion protocol. Fragment-specific fixation had improved stiffness characteristics only with respect to the smaller ulnar-sided fragment.
Figures A and B show a shearing radiocarpal-fracture subluxation with small lunate-facet fracture. Figure C shows an immediate post-operative radiograph. Figure D shows subluxation of the radiocarpal joint caused by failure to support lunate-facet fragment. Figure E shows the clinical appearance of a volarly subluxated wrist.
Incorrect Answers:
Answer 2: The use of a non-locking plate in this situation did not directly lead to the failure of fixation, and applying a similar construct with locking fixation
would not have prevented volar subluxation of the lunate facet fragment. Answer 3: Volar tilt was grossly restored post-operatively.
Answer 4: Radial styloid plating would not have prevented volar subluxation of the lunate facet fragment.
Answer 5: Three bicortical screws in the intact radial shaft proximally is adequate fixation.
Which of the following is most commonly associated with both simple and complex elbow dislocations?
1) radial head fracture
2) radial neck fracture
3) loss of terminal extension
4) repeat dislocation
5) coronoid base fracture
Elbow dislocations are classified as either simple (no associated fracture) or complex (associated fracture). The goal of treatment is a stable joint that tolerates early motion. The initial range of motion is the stable arc found on postreduction examination. Studies have demonstrated a better outcome when simple elbow dislocations are treated non-surgically rather than with surgical repair. Simple elbow dislocations usually have an excellent outcome (return of functional range of motion with normal strength). A loss of terminal extension is the most common sequelae.
Ross et al. reported on 20 patients with simple closed posterior elbow dislocations who were treated with immediate active ROM under close supervision. They found a final arc of motion of -4 to 139 degrees, with final motion reached a mean of 19 days after dislocation. Only 1 patient had recurrent instability.
A 36-year-old female sustains a knee injury after falling from a ladder onto her flexed knee; she cannot do a straight leg raise after a lidocaine injection into her knee. A radiograph is shown in Figure A. Which of the following treatment options has been shown to have the best outcomes with this injury?
1) Long leg cast
2) Hinged knee brace use with functional rehabilitation protocol
3) Open treatment with internal fixation or excision with patellar tendon advancement
4) Distal patellar resection and allograft reconstruction
5) Placement of a cerclage wire from patella to proximal tibia
The clinical presentation is consistent with and inferior pole patella fracture. Open reduction and internal fixation or excision with patellar tendon advancement is the most appropriate treatment of this injury pattern.
Whenever possible, salvage of the inferior pole through open reduction internal fixation is favored over simple excision and patellar tendon advancement, as this has been shown to be associated with improved outcomes. This is not always possible, however, and pole resection can be performed if the inferior comminution precludes fixation. Inferior outcomes of the partial distal patellectomy and patellar tendon advancement are (aside from the possible resulting patella baja) probably not directly related to the patellofemoral articulation. On the undersurface, the proximal 75% of the patella is covered with articular cartilage; however, the distal 25% is not, and does not articulate with the femoral trochlea.
Kastelec et al. performed a retrospective review of ORIF v. pole resection followed over 4.6 years postoperatively. There was a significant increase (better) in patellofemoral score with ORIF; significant differences in knee pain,
tolerated activity levels, and ROM were also noted. Patella baja was frequently noted with pole resection and correlated with worse functional outcomes.
Matejcic et al. performed a retrospective review of ORIF v. pole resection followed over 5.3 years postoperatively. Results were excellent/good in 90.1% of the ORIF and only 73.1% of the pole resection patients. In addition, significant differences between the groups were noted with regard to knee pain, swelling, level activity, compression pain, range of motion, muscular atrophy, muscular strength, and final patellofemoral score (all better with ORIF).
Figure A is a lateral knee radiograph showing an inferior pole patella fracture.
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?
1) Sling immobilization
2) Displacement and comminution
3) Age less than 40 years old
4) Immediate motion exercises
5) Male
Robinson et al have shown that lack of cortical apposition, comminution, female gender, and advancing age are the 4 factors that contribute to nonunion.
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p
A 34-year-old male presents after falling off a roof at his job. He has an obvious deformity of his left lower extremity, and injury radiographs are shown in Figures A and B. He has no other injuries. Which of the following definitive treatment algorithms will most likely lead to the best outcomes in this patient?
1) Closed reduction and percutaneous screw fixation of the femoral neck, followed by reamed antegrade nailing of the femur fracture
2) Reamed antegrade nailing of the femoral shaft fracture, followed by open reduction and percutaneous screw fixation of the femoral neck fracture
3) Reamed retrograde nailing of the femoral shaft fracture, followed by closed
reduction and percutaneous screw fixation of the femoral neck
4) Open reduction and screw fixation of the femoral neck, followed by reamed retrograde nailing of the femoral shaft fracture
5) Open reduction and screw fixation of the femoral neck, followed by plating of the femoral shaft fracture
The clinical presentation is consistent with a femoral shaft fracture with an ipsilateral femoral neck fracture. Of the options presented, the most appropriate treatment is open reduction and lag screw fixation of the femoral neck fracture followed by reamed retrograde nailing of the femoral shaft fracture.
Ipsilateral femoral neck/shaft fractures are an uncommon injury estimated to occur in 2-6% of all femoral shaft fractures. It is generally agreed upon that due to the potentially devastating complications of the femoral neck fracture in young patients, the neck fracture should be treated first and the shaft fracture second. Anatomic reduction of the femoral neck fracture is paramount in obtaining successful healing, and therefore open reduction is recommended in the setting of fracture displacement. Provisional reduction of the femoral neck fracture, followed by antegrade nailing with subsequent addition of definitive fixation of the femoral neck is also acceptable.
Peljovich et al. present a review article on ipsilateral femoral neck and shaft fractures. The treatment algorithm they propose consists of first treating the femoral neck fracture, and then addressing the femoral shaft fracture with retrograde nailing. They also highlight the risk and benefits of each treatment approach.
Watson et al. reviewed 13 patients who had healing complications after undergoing surgical fixation of their ipsilateral femoral neck and shaft fractures. They found that lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications. Therefore, this approach was recommended as the treatment of choice.
Figures A and B demonstrate an ipsilateral comminuted femoral shaft fracture, and a displaced femoral neck fracture. Illustrations A-C show an example of a femoral shaft fracture with an ipsilateral femoral neck fracture treated with lag screws of the femoral neck fx and retrograde nailing.
Incorrect Answers:
Answer 1: Open reduction of the femoral neck fracture with anatomic
alignment is preferred to closed reduction in this case.
Answer 2,3: The femoral neck fracture should be addressed first.
Answer 5: Nailing of the femoral shaft fracture would be preferred initially in this case to prevent disruption of the biology and fracture healing around the comminuted segments.
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?
1) Medial to lateral screw placement across lateral femoral condyle
2) Anterior to posterior screw placement across medial femoral condyle
3) Medial to lateral screw placement across medial femoral condle
4) Anterior to posterior screw placement across lateral femoral condyle
5) Anterior to posterior screw placement across intercondylar notch
The most common variation of a Hoffa fracture is a coronal fracture of the lateral femoral condyle. The most appropriate screw placement of the above answer choices in the treatment of the most common Hoffa fracture variant would be anterior to posterior screws across the lateral condyle for fixation.
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Illustration A shows sagittal and axial CT scan cuts showing a Hoffa fracture of the lateral femoral condyle. Illustration B shows multiple anterior to posterior, and posterior to anterior oriented screws for ORIF of the Hoffa fracture.
A 26-year-old right hand dominant male is involved in a motor vehicle collision and sustains the left humerus injury demonstrated in Figure A. The brachial artery is disrupted and requires urgent attention in the operating room. The patient's preoperative nerve evaluation demonstrates that the patient is unable to initiate extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis brevis, extensor digitorum, extensor indicis proprius, and extensor pollicis longus motor activity. What is the most likely etiology for this observed neurologic examination?
1) Neurapraxia of the median nerve
2) Axonotmesis of the radial nerve
3) Neurotmesis of the ulnar nerve
4) Neurotmesis of the radial nerve
5) Axonotmesis of the ulnar nerve
The most likely cause of the radial nerve palsy in a high energy open humerus fracture is laceration or complete disruption of the radial nerve (Neurotmesis).
Neurotmesis is complete disruption of nerve and is associated witn no spontaneous recovery without intervention. Axonotmesis constitutes axon disruption, but the surrounding neural connective tissue is intact and nerve regeneration can occur(Wallerian or antegrade degeneration). Neurapraxias occur often by compression and the axon maintains continuity but local demyelination and ischemia occur.
Ring et al. present a Level 4 study of 24 patients that had radial nerve palsy associated with a humerus fracture. All 6 patients with a transected radial nerve had an open humerus fracture also. The results of primary nerve repair in this circumstance found that there was no recovery in any of the patients.
Foster et al. authored a Level 4 review of 14 patients had a radial nerve palsy and an associated open humerus fracture. 64% of the 14 patients had a radial nerve that was either lacerated or interposed between the fracture fragments. They recommend exploration of the radial nerve in the setting of a radial nerve palsy and concomitant open humerus fracture in contrast to observation of a radial nerve palsy in closed humerus fractures.
Figure A demonstrates an open left humerus fracture.
Incorrect Answers:
Answer 1,3,5: The radial nerve provides distal motor activity to the ECRL, ECRB, EPB, EIP, and EPL.
Answer 2: Axonotmesis of the radial nerve is not the most common form of injury associated with closed or open humerus fractures.
Which of the following is true regarding the center of rotation of angulation (CORA) as it refers to tibial diaphyseal angular deformity?
1) It is the point at which the proximal mechanical axis and distal mechanical axis meet
2) It is the point at which the proximal anatomical axis and proximal mechanical axis meet
3) It is always the point on the cortex at the most concave portion of the deformity
4) It is the point at which the distal anatomical axis and distal mechanical axis meet
5) It is always the point on the cortex at the most convex portion of the deformity
The center of rotation of angulation(CORA) in diaphyseal tibial deformity is defined as the intersection of the proximal mechanical(PMA) or anatomical axis(PAA), and the distal mechanical(DMA) or anatomical axis(DAA).
Angular deformity of the femur or tibia involves angulation not only of the bone but also of its axes. When a bone is divided and angulated, the mechanical and anatomic axis of the bone are also divided into proximal and distal segments.
The pairs of proximal and distal axis lines intersect to form an angle. The point at which the proximal and distal axis lines intersect is called the CORA.
The axis line of the proximal bone segment is called the PMA or PAA, and axis line of the distal segment is called the DMA or DAA. In the tibia, because the mechanical and anatomical axes are almost the same, the PMA and PAA lines overlap, as do the DMA and DAA lines.
Illustration A shows the CORA as it relates to the axes of an angulated tibia.
Incorrect Answers:
2-5:These do not describe the CORA or any other specific anatomical points as they related to long bone deformity.
At long term follow-up, a male who sustains multiple traumatic injuries compared with a premenopausal female, who sustained similar polytrauma, is most likely to have which of the following?
1) Higher quality-of-life scores than females
2) Increased rates of complex regional pain syndrome
3) Require more psychiatric counseling and pharmacologic management than females
4) Take more absentee days at work as a result of illness than females
5) Decreased incidence of lower extremity amputation
Ten or more years after severe polytrauma, premenopausal women, compared to men, demonstrate a higher incidence of posttraumatic stress disorder (PTSD) and take more sick leave time from work.
Depression following polytrauma should be screened for by treating orthopaedic surgeons. Depression commonly arises from a protracted injury and can compound the disability by increasing the perception of more physical illness.
Probst et al. present a Level 4 review of over 600 polytrauma patients. They found that quality-of-life was significantly lower in women (Short form-12 psychologic F = 48.6 +/- 10.8 vs. M = 50.8 +/- 9.4; p = 0.02), but the same rate of women (75.3%) and men (75.4%; p = 0.995) felt well rehabilitated.
Holbrook et al. report a Level 4 study of 1,048 polytrauma patients. They found that females had lower quality-of-life scores and were significantly more likely to develop early combined depression.
Incorrect Answers:
Answer 4: Females take more absentee days at work.
Answers 2, 3, 5: There is no data supporting these answer options.
A 29-year-old healthy Caucasian female presents to the emergency department with her boyfriend with a left anterior shoulder dislocation and several facial abrasions after tripping in the shower approximately three hours prior to arrival. She is 5’7’’ and weights 120 lbs (BMI 18.8). The patient notes that she has not had a menstrual period in three months and that she is training for a long-distance triathlon. Physical examination reveals no other obvious injuries. Basic serum laboratory values are unremarkable. A urine pregnancy test is positive. In addition to treating her shoulder dislocation, the orthopaedic surgeon should
1) Perform a skeletal survey to evaluate for other fractures or dislocations
2) Question the patient in private about the specific details of this injury and her sense of safety in the home
3) Refer the patient to a nutritionist given the patient’s BMI of 18.8
4) Obtain additional laboratory studies and admit the patient to the hospital for treatment of anorexia nervosa
5) Obtain advanced imaging of the shoulder to evaluate for underlying pathologic lesions
for her current injury, it is imperative for health care providers to inquire into the safety of the home environment in potential cases of intimate partner violence (IPV).
Risk factors for female victims IPV include being in the 2nd or 3rd decade of life, current pregnancy, having 1 or more prior children, and low socioeconomic status. Reporting requirements for adult abuse are not standardized amongst most states and physicians must understand the importance of identification and documentation in cases of suspected IPV.
Bhandari et al. state that musculoskeletal injuries are the second most common form of IPV (28%) after head and neck injuries (40%).
Musculoskeletal injuries can be variable, including sprains, fractures, dislocations, and foot injuries.
Della Rocca et al. conducted a survey and found orthopaedic surgeons have several misconceptions regarding victims of IPV and further, nearly half of their survey respondents reported identifying a victim of IPV while only 4% reported that they currently screen their injured female patients for IPV.
Zillmer presents a review of the issues surrounding IPV including proper identification, documentation, appropriate questioning and how to involve community services.
Illustration A shows some basic facts regarding IPV during pregnancy as reported by the CDC. Additional information can be found at the following link.
[htt](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[p](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)
Incorrect Answers:
Answer 1. There is no indication for a skeletal survey and it would be inappropriate to subject this pregnant patient to additional radiation.
Answer 3. There is no need to refer a patient to a nutritionist for a normal BMI Answer 4. There is no indication for admission or other laboratory studies in this otherwise healthy patient.
Answer 5. There is no need for advanced imaging in the emergency department in the case of an isolated traumatic shoulder dislocation
A 19-year-old military recruit complains of 7 weeks of right heel pain. He notes the pain is worse with jumping and long distance running. He has completed a course of plantar fascia and Achilles tendon stretching with no significant improvement in his symptoms. He denies constitutional symptoms. On examination, his body mass index is 22, he has a normal foot posture and can perform a single leg heel rise without difficulty. There is no pain with palpation of the lateral border of the foot or with external rotation stress to the midfoot. There is tenderness with medial and lateral compression of the hindfoot and there is a negative syndesmosis squeeze test. There is a negative Tinel's sign at the tibial nerve. Axial and lateral radiographs are shown in Figures A and B. What is the most appropriate next step in management?
1) Heel pad cortisone injection
2) Platelet rich plasma injection and 6 weeks of physical therapy
3) Restricted weight bearing and magnetic resonance imaging of the foot
4) Release of the first branch of the lateral plantar nerve
5) ASTYM or Graston physical therapy techniques to the achilles and plantar fascia
Restricted weight bearing and magnetic resonance imaging of the foot is indicated in this military recruit with a positive heel compression test and suspicion for calcaneal stress fracture.
Calcaneal stress fractures occur as a result of repetitive loading and are more common in females with the female athlete triad (anorexia athletica) of disordered eating, amenorrhea, and osteoporosis. On exam tenderness is obtained with medial and lateral compression of the calcaneus.
Sormaala et al. performed a Level 4 review over 8 years of the Finnish military. They found 34 calcaneal stress fractures with 19 occurring in the posterior part of the calcaneus. Only 15% of the patients had the stress fracture visualized on plain radiography. They conclude that MRI is warranted if plain radiography does not show abnormalities in a physically active patient with exercise-induced pain in the ankle or heel. A nuclear medicine bone scan is also appropriate for diagnosis but MRI may give greater detail.
Gehrmann et al. present a Level 5 review of foot stress fractures. They report that with calcaneal stress fractures the fracture lines are oriented vertically or obliquely in the tuberosity of the calcaneus.
Figures A and B show some sclerosis in the central calcaneus with no evidence of overt fracture and an enthesophyte at the Achilles tendon insertion.
Illustration A and B are T2 sagittal and coronal images demonstrating a stress fracture in the superior calcaneal tuberosity with surrounding edema.
Incorrect Answers:
Answer 1: Heel pad cortisone injections are typically avoided due to risk of fat pad atrophy and are not indicated in calcaneal stress fractures.
Answer 2: Platelet rich plasma is not indicated in calcaneal stress fractures. Answer 4: The patient presents with a negative Tinel's at the tibial nerve and presentation is not consistent with first branch of the lateral plantar nerve entrapment.
Answer 5: ASTYM and Graston physical therapies are not indicated for calcaneal stress fractures.
A 35-year old male is involved in a fall from height and present with the isolated injury shown in Figures A and B. The body of the talus is extruded medially through a large linear open wound. Along with irrigation and debridement, what is the most appropriate definitive management of this injury?
1) Reimplantation of the talar body followed by cast immobilization
2) Reduction of talar body, fracture fixation with smooth Steinman pins, and spanning fixator placement
3) Talar body allograft with internal fixation to native talar head
4) Fragment removal, antibiotic spacer placement and external fixation
5) Reduction of native talar body and ORIF of talar neck fracture
The patient is presenting with a displaced talar neck fracture with extrusion of the talar body. Reimplantation of the talar body and ORIF of the talar neck fracture is the most appropriate treatment.
Talar extrusions are rare injuries and are caused by high energy mechanisms. Complete dislocation without a concomitant fracture is extremely rare. The talus is prone to dislocation as there are no muscular attachments. These injuries need to be treated with anatomic reduction and internal fixation to prevent avascular necrosis and post-traumatic arthritis.
Smith et al. investigated the clinical results and functional outcome after reimplantation of the extruded talus. They concluded that salvage and reimplantation of the talus is a relatively safe procedure with only 2 of the 27 patients developing an infection. No association was found between outcome and associated talar fracture.
Van Opstal et al. reported on two cases of talar extrusions following high energy injuries and reviewed the associated literature. Both cases were treated with wound I&D, reduction and external fixation. After 1 year they had pain free ROM with no signs of AVN or arthritis. Review of the literature showed that anterolateral dislocations are more common than anteromedial. Total talar dislocation is thought to be the endpoint of maximum pronation or supination injuries.
Figures A and B show an extruded talar body in the setting of a Hawkins III talar neck fracture. Illustration A shows a clinical photo of an extruded talus.
Incorrect Answers:
Answer 1: Displaced talar neck fractures should not be treated in a cast, especially open fractures
Answer 2: Definitive treatment of this injury is most effectively accomplished with formal ORIF. Steinman pin fixation is not adequate, even in the presence of an external fixator.
Answer 3: There is no data supporting removal of fragment and use of allograft overuse of native talar body
Answer 4: There is no data supporting removal of the fragment. The associated
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
. All displaced olecranon fractures should be considered for internal fixation. Displacement alone does not direct choice of implant.
Answer 2. Intra-articular extension is an indication for surgery to re-establish articular congruity but does not dictate implant selection.
Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown
Answer 4. This fracture is comminuted, without a distinct fracture line.
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?
1) Bilateral open reduction and internal fixation
2) Open reduction internal fixation on the right, reamed intramedullary nailing on the left
3) Temporizing external fixation on the right, open reduction and internal fixation on the left
4) Bilateral reamed intramedullary nailing
5) Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Answer 1-3: Open reduction internal fixation would not be indicated in damage control orthopaedics.
Answer 4: Bilateral reamed intramedullary nailing would be indicated in early total care of these injuries. As this patient is hemodynamically unstable, with a high injury severity score and bilateral lung contusions, damage control orthopaedics would be indicated.
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
1) Removal of locking screws
2) Removal of small fragment plates
3) Removal of metaphyseal implants
4) Removal of implants less than 1 year after insertion
5) Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:
Answer 1: Removal of locking screws does not increase the risk of refracture. Answer 2: Removal of large fragment plates (4.5mm) are at increased risk of refracture as compared to small fragment plates (3.5mm).
Answer 3: Metaphyseal implant removal has a decreased risk of refracture compared to diaphyseal implant removal.
Answer 5: Protective splinting for 6 weeks is all that is generally recommended for these patients.
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?
1) Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
2) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
3) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
4) Irrigation, debridement and placement external fixator right ankle, femur and tibia
5) Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
Answer 1: A pelvic binder would not be helpful in this scenario and actually may worsen the deformity.
Answer 2: Definitive plate fixation of the anterior pelvis will be needed, but only when the patient is adequately resuscitated.
Answer 3: An anterior external fixator may actually do more harm than good as it may require more time than placing skeletal traction, and also have difficulty controlling the posterior pelvis from the front.
Answer 5: Percutaneous SI screws may be placed later, once the patient is resuscitated and stable.
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?
1) Foot drop
2) Injury to the anterior tibial artery
3) Septic arthritis
4) Flexion contracture of the knee
5) Patellar tendon rupture
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
Answer 1: Foot drop would occur secondary to common peroneal nerve injury, which is not at risk with very proximal pin placement.
Answer 2: The anterior tibial artery is not at risk with very proximal pin placement.
Answer 4: The knee is free to move and therefore should not develop a flexion contracture secondary to the external fixator.
Answer 5: Patellar tendon rupture is not complication of external fixator pin placement in the tibia.
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
1) Radial nerve palsy
2) Intra-articular extension
3) 2mm fracture distraction, 5 degrees of rotational malignment
4) Ipsilateral proximal both bone forearm fracture
5) Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
Answer 1,2,3,5: These associated injuries are NOT an absolute indication for surgery. An area of controversy is the occurrence of new-onset radial nerve injuries after closed manipulation. However, the current algorithm does not support early open nerve exploration and fixation.
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
1) Posterior-stabilized total knee implant
2) Cruciate retaining total knee implant
3) Spiral fracture pattern
4) Distal femoral replacement
5) Knee flexion contracture of 15 degrees
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?
1) Full pronation
2) 25 degrees pronation
3) Neutral
4) 25 degrees supination
5) Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
1) Bilateral femur fractures
2) Rib fractures
3) Lactate of 5.2
4) Urine output of 20 cc/hr
5) Heart rate and blood pressure
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
Answer 1: Bilateral femur fractures are an indication to practice damage control orthopaedics and delay definitive fixation
Answers 3,4,5: All of these answers suggest that the patient is underresuscitated. Definitive fixation should be delayed
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
Answers 1,2,3, and 5: Posterior sided injuries, especially for these injuries, would probably be best approached via the Kocher-Langenback approach. Surgical dislocation with a trochanteric slide may help visualization in answer 1.
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?
1) Hand dominance
2) Angulation of fracture
3) Smoking
4) Early physical therapy
5) Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Answers 1,2,4: These factors do not have a significant influence on bone healing.
Answer 5: Diet has shown to improve bone healing but this does not have the greatest impact.
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?
1) Abduction brace for three weeks, followed by therapy
2) Right shoulder MR arthrogram
3) Open reduction and internal fixation
4) Hemiarthroplasty
5) Early range of motion
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
Answer 1: The GT fragment is displaced more than 5-10mm which would warrant surgical reduction and stabilization of the fracture.
Answer 2: MR arthrogram may be indicated to rule out an intra-capsular soft-tissue injury. However, this would not be warranted prior to fixation of the fracture.
Answer 4: Hemiarthroplasty would be indicated in some 4-part proximal humerus fractures or elderly patients. Considering this patient's age and valgus impaction of the fracture, ORIF would be most appropriate.
Answer 5: Early range of motion would be warranted AFTER fixation of the fracture.
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
1) Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
2) Left ASIS to mid-symphysis, right lateral window incision
3) Subumbilical incision
4) ASIS to ASIS bilaterally
5) Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
Answers 1,2: While these approaches may give access to the pelvic brim, each only give access to one side; one needs to circumferentially access and pack the pelvis.
Answer 4: An ASIS to ASIS skin incision is an unnecessary dissection with too many important structures that lie very close to the skin, including the femoral vessels.
Answer 5: A pararectus incision is an alternative approach to access the quadrilateral plate for acetabular fractures and does not play a role in pelvic packing.
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
1/.
1) 30-40%
2) 40-50%
3) >50%
This patient has likely lost 30-40% of his blood volume and is likely in stage III hemorrhagic shock on the basis of his heart rate, blood pressure, and urine output.
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal 100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
Answer 1: Schatzker II tibial plateau fractures can be treated with a single lateral plate.
Answer 2: Proximal third tibial shaft fractures can be treated with an intramedullary nail or percutaneous plating
Answer 3: Schatzker IV tibial plateau fractures can be treated with a single medial or posteromedial plate.
Answer 5: Tibial tubercle fractures in children can be treated with anterior to posterior screws.
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?
1) Immediate surgical intervention
2) Postoperative epidural analgesia
3) Postoperative antibiotics
4) Pre-operative medical optimization
5) Choosing total hip arthroplasty instead of hemiarthroplasty
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Answer 1: Most studies have shown an association between operative delay of
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
Answer 2: Post-operative epidural anaesthesia has shown to decrease postoperative delirium but does not affect 30-day mortality.
Answer 3: Postoperative antibiotics have not shown to reduce the 30-day mortality.
Answer 5: Total hip arthroplasty has shown to improved functional outcomes at 1 year compared with hemiarthroplasty. However, there has been no change in mortality.
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?
1) Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
2) Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
3) Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
4) Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
5) Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
Answer 1: A patient cannot do touch-down weight bearing on one side and non-weightbearing on the other side simultaneously.
Answer 3: The LC-I injury pattern is stable and can undergo immediate weightbearing as tolerated.
Answer 4: The LC-I pattern is stable and would allow immediate weightbearing, and the right pilon fracture would require non-weightbearing. Answer 5: The right pilon fracture would require non-weightbearing at this time.
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
1) Moore I
2) Moore II
3) Schatzker III
4) Schatzker V
5) OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:
Answer 1: Moore Type I is a coronal split fracture of the medial tibia plateau which displaces distally. It does not cross over to the contralateral side of the eminence.
Answer 3: Schatzker Type III is a pure lateral plateau depression.
Answer 4: Schatzker Type V is a bicondylar fracture where the metaphysis and diaphysis remain intact.
Answer 5: OTA type 41B3 is a partial articular fracture with a split-depression of the unilateral plateau.
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:
Answer 2: Vertical medial malleolar fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Juvenile Tillaux fractures occur typically in patients with open physes. They do not occur in patients with closed physes, and are not associated with tibial shaft fractures.
Answer 4: Spiral/oblique tibial shaft fractures are not associated with talus fractures.
Answer 5: Knee dislocations are considered high energy injuries, and are not associated with tibial shaft fractures.
What would be the most appropriate treatment for this patient at this time?
1) Observation only
2) Referral to physiotherapy
3) MRI spine and hip
4) Total hip arthroplasty
5) Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Answer 1: Symptomatic lateral femoral cortical stress fractures, known as "dreaded black lines", should be treated with early stabilization to prevent subtrochanteric fracture.
Answer 2: Referral to physiotherapy would not be indicated.
Answer 3: Symptoms are related to a subtrochanteric stress fracture, which has been identified on radiograph. MRI would not be indicated.
Answer 4: This patient has mild arthritis. Treatment with a long bridging femoral stem may stabilize the fracture, However, the gold standard treatment would be intramedullary nailing.
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?
1) Age greater than 70 years.
2) Fracture pattern in Figure A
3) Significant medical comorbidities.
4) Fracture pattern in Figure B
5) Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Answers 1, 2, 3, and 5 are all factors that would favor non-operative management for a proximal humerus fracture.
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?
1) HR >110
2) Bilateral pulmonary contusions seen on chest radiograph
3) SBP = 90mmHg
4) Unilateral femur fracture
5) Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Answer 1: Heart rate alone (even elevated severely) is not an indicator to
implement DCO.
Answer 3: A systolic BP of 90 mmHg is not an indicator to implement DCO. A SBP of 70mmHg or lower may indicate a patient in extremis (along with other parameters) indicating the benefits of DCO.
Answer 4: A unilateral femur fracture alone in a stable patient is not an indicator of DCO; a patient with bilateral femur fractures, however, may benefit from DCO.
Answer 5:A lactate of 2.5 mMol/L, while slightly elevated, does not warrant DCO. A lactate value of greater than 6 alone would indicate the need for DCO.
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?
1) Young-Burgess APC Type II
2) Young-Burgess LC Type I
3) "U" Type Spinopelvic Dissociation
4) Denis Zone-I
5) Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
Answer 1: APC Type II fractures do not classify fracture extensions into the sacral canal. The posterior SI ligaments are considered intact. There is usually disruption of sacrospinous and sacrotuberous ligaments.
Answer 2: LC Type I is an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture.
Answer 4,5: Figures A-C demonstrate a "U" type fracture of the sacrum.
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?
1) Ulnar neuropathy
2) Posterior interosseous nerve injury
3) Early loss of fixation
4) Elbow flexion contracture
5) Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:
Answers 1,2,3,5: All of these may be complications with this surgery. These complications are not as common as elbow contracture or stiffness.
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?
1) Chronic suppressive, culture-directed, antibiotic therapy
2) Above knee amputation
3) Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
4) Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
5) Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Answer 1: Chronic suppressive therapy would be considered in a patient that is unable to undergo surgical intervention
Answer 2: Amputation is a primary option for patients unable to undergo lengthy or multiple surgical interventions.
Answer 3: After removing the hardware, the fracture non-union will need to be stabilized.
Answer 5: This patients has a chronic infection that requires radical bone debridement and local infection control. The use of acute bone grafting in a single stage procedure in the distal 1/3 tibia (poor blood supply) is less ideal, especially in the setting of infection.
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?
1) Fracture classification
2) Number of blood transfusions in the first 24 hours
3) Gender
4) Time to operative fixation
5) Use of pelvic binders
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
Answers 1,3-5: Gender, fracture pattern, time to operative fixation or use of pelvic blinders do not correlate directly with mortality.
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?
1) Early range of motion
2) Hinged elbow brace for 4 weeks
3) Repair lateral collateral ligament
4) Remove and upsize implant
5) Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Answer 1: Early range of motion is supported after radial head arthroplasty. However, the next most appropriate step in this scenario would be the intraoperative assessment for radiohumeral joint overstuffing.
Answer 2: Hinged braces may be used in the post operative period. However, overstuffing the radiohumeral joint is of first priority.
Answer 3: There is no indication in this question for lateral collateral ligament repair
Answer 4: Removing the implant and upsizing the radial head would be the opposite of what is needed in this scenario.
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?
1) Medial only
2) Lateral only
3) Anterior and medial
4) Posterior and medial
5) Posterior and lateral
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
Answer 1: would prevent varus malalignment Answer 2: would prevent valgus malalignment alone
Answer 3: would prevent varus and recurvatum malalignment Answer 4: would prevent varus and procurvatum malalignment
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
1) A fracture of the radial head requiring ORIF
2) A highly comminuted radial head fracture requiring radial head arthroplasty or resection
3) An MCL injury requiring repair
4) A type I avulsion fracture of the coronoid
5) An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
Answers 1, 2, 3: Radial head fractures, and MCL injuries are not seen in varus/posteromedial mechanisms. They are seen in terrible triad elbow injuries which are due to valgus and posterolateral rotatory forces.
Answer 4: The coronoid fracture seen in these injuries is an anteromedial facet fracture, and not an avulsion fracture of the tip of the coronoid.
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?
1) Femoral skeletal traction
2) CT scan
3) Hip spica cast application
4) Observation only
5) Serial neurovascular examinations
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:
Answer 1: Femoral skeletal traction would be considered if there was an associated acetabular fracture or loose body.
Answer 3: Hip spica casts are not used with these injuries.
Answer 4: Observation would be considered after the CT scan is performed. Answer 5: There was no mention of neurovascular injury. This patient has a normal neurovascular examination. There is no fracture or risk of hematoma formation. This would not be necessary.
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?
1) MRI angiography of leg
2) Four-compartment fasciotomy
3) Follow-up examination the following day
4) Continued monitoring and serial examinations
5) EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) 30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
1) Repeat closed reduction under conscious sedation
2) Selective compartment fasciotomies
3) External fixation and compartment monitoring
4) 4-compartment fasciotomies with fracture fixation done emergently
5) Modify the cast to reposition the ankle into slight plantarflexion
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
Answers 1, 3: The stem does not suggest that the reduction was lost, so neither repeating a closed reduction or placement of an external fixator is indicated at this time.
Answers 2, 4: While suspicion should remain elevated for the development of compartment syndrome, simple conservative measures such as cast modification are ideal first steps to avoid onset of compartment syndrome. The clinical vignette given does not portray clinical compartment syndrome requiring emergent fasciotomy. It would be reasonable to maintain a high level of suspicion given the injury, but non-invasive cast modification is a simple, safe and quick first step.
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
Answers 2,3,4,5: Any pelvic or lower limb fracture can cause a disruption in a patients activities of daily living. This may include sexual dysfunction, for both men and women. The injury pattern that has the greatest potential for sexual dysfunction are APC type pelvic injuries.
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
1/. 18
1) 25
2) 33
3) 41
4) 48
This patients Injury Severity Score (ISS) is 41. In this patient, the highest AIS scores were from the head (AIS=4), abdomen (AIS=4) and pelvis (AIS=3).
Therefore, the calculation for the ISS score was 4^2 + 4^2 + 3^2 = 41.
The ISS score is calculated as the sum of the square values from the highest Abbreviated Injury Score [AIS] scores in the three most severely injured ISS body regions. ISS scores range from 1 to 75. A single score of 6 on any AIS region results in automatic score of 75. ISS scores > 15 are associated with mortality of 10%.
Poole et al. found that the AIS and ISS appropriately reflect the impact of extraskeletal injuries in patients with femur fractures, but they do not adequately reflect the increased morbidity associated with multiple lower extremity fractures.
Balogh et al. aimed to compare the scoring efficacy of the injury severity score (ISS) and the new injury severity score (NISS) in predicting post-injury outcomes. They found that multiple orthopaedic injuries, as used in the NISS system, had a significantly greater impact on reported poor post-injury outcomes. They suggest that NISS should replace the traditional ISS when grading trauma related outcomes.
Illustration A shows a table of the various ways to score injury severity in trauma patients.
Incorrect Answers:
Answers 1,2,3,5: ISS = A^2 + B^2 + C^2, where A, B, C are the AIS scores of the three most severely injured ISS body regions. The only correct answer is ISS=41.
A 60-year-old otherwise healthy female sustains the fracture in Figure A. Immediate surgical treatment would most likely prevent which of the following complications?
1) Malunion.
2) Regional osteopenia.
3) Skin necrosis.
4) Posttraumatic arthritis.
5) Refracture.
The patient has a calcaneal tuberosity fracture. The Achilles tendon is attached to the displaced fragment, which can cause soft tissue compromise and skin necrosis if not treated promptly.
Displaced calcaneal tuberosity and tongue-type calcaneus fractures have a high incidence of wound complications if not treated urgently. Recommended management includes surgical fixation often performed percutaneously. Lag screws are typically directed from the posterior superior tuberosity inferiorly and distal. In cases of skin sloughing and skin necrosis, flaps may be needed.
Gardner et al. reviewed 139 tongue-type calcaneus fractures, and found that 21% had some degree of posterior skin compromise. Additionally, there was a statistically significant increase in posterior skin compromise with delayed presentations.
Hess et al. reviewed 3 cases of calcaneal tuberosity avulsion fractures that let to skin necrosis because of a delay in treatment.
Tornetta reviewed the indications for percutenaous treatment of calcaneus fractures, and found it was successful and most useful in tongue-type calcaneus fractures.
Figure A shows a lateral radiograph of a R ankle showing a calcaneal tuberosity fracture. Illustration A shows an AP radiograph of a R ankle following percutaneous reduction and internal fixation of the calcaneus fracture with two cannulated screws. Illustration B shows a lateral radiograph of a R ankle showing interval reduction and fixation of the calcaneus fracture. Illustration C shows a clinical photograph of posterior skin compromise associated with a calcaneal tuberosity fracture.
Incorrect Answers:
Malunion, regional osteopenia, posttraumatic arthritis, and refracture risk would not be significantly altered with immediate surgical intervention as opposed to operative management within a reasonable time frame.
When elevating the joint surface in the injury pattern seen in Figure A, what material has the highest compressive strength when filling the metaphyseal void?
1) Calcium phosphate
2) Tricalcium phosphate
3) Cancellous autograft
4) Cancellous allograft
5) rhBMP-7
Figure A illustrates a depressed lateral tibial plateau. One of the key components of fixing a depressed articular segment is maintaining the reduction.
Trenholm et al reviewed an experimental study where a split depression (Schatzker II) fracture was created in a cadaveric model. The stiffness of the elevated fragment in cadavers using calcium phosphate cement versus cancellous bone graft as support showed no difference, but calcium phosphate cement was found to have greater compressive strength than cancellous bone alone.
The review article by Hak reviews the composition, advantages, and disadvantages of commerically available bone graft substitutes.
Incorrect answers:
2: Tricalcium phosphate is a bone graft substitute that is osteoconductive, but has less compressive strength.
3-4: Cancellous bone has less compressive strength than calcium phosphate. 5: rhBMP-7 is not used as a bone filling agent in this instance, as it is typically provided on a easily compressible collagen sponge.
A 42-year-old male sustains multiple abdominal injuries along with the fractures shown in Figures A and B. Which of the following factors is most useful to determine the patient's resuscitation and ability to undergo early definitive fixation of these two fractures?
1) Pulse pressure
2) Respiratory rate
3) Urine output
4) Platelet count
5) Base deficit
The base deficit, or lactate level, has been shown to best reflect the resuscitation status and survival after trauma.
Normalization of hemodynamic parameters does not accurately reflect the resuscitation status and a patient can be in compensated shock (occult tissue hypoperfusion) despite normalization of the heart rate and blood pressure. The use of temporizing measures with delayed definitive fracture treatment has been shown to decrease systemic complications in these patients with occult hypoperfusion.
Crowl et al. performed a retrospective study of 127 patients with femoral shaft fractures undergoing intramedullary nailing, assessing for occult hypoperfusion. Patients with occult hypoperfusion preoperatively had a twofold increase in postoperative complications and significant increase in postoperative infections.
Tisherman et al. present a review of hemodynamic parameters and their use in assessment of resuscitation. They report that hyperlactatemia is common among critically ill patients, and lactate levels and their trend may be reliable markers of illness severity and mortality. Therefore, measurement of blood lactate is recommended to stratify patients based on the need for fluid resuscitation and the risks of multiple organ dysfunction syndrome and death. They conclude that lactate is a reliable indicator of sepsis severity and a marker of resuscitation; however, it is an unreliable quantitative marker of tissue hypoxia/hypoperfusion.
Pallister et al. present a review of the effect of early stabilization of long bone fractures. They note that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure, both of which are caused by activation of the systemic inflammatory response. This activation results in tissue recruitment of and injury by circulating polymorphonuclear leukocytes.
Figure A is a radiograph showing a femoral shaft fracture, while Figure B shows an open tibial shaft fracture.
Incorrect Answers:
Answers 1-4: Normalization of these factors does not always predict adequate resuscitation.
Interleukin-6 levels have been shown to be a reliable measure of which of the following?
1) Osteoporosis
2) Severity of injury
3) Sarcomatous tumor burden
4) Bone turnover
5) Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production.
Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
A 31-year-old male sustained a displaced proximal humerus fracture after a motor vehicle accident. Which of the following factors has the lowest association with humeral head ischemia in these injuries?
1) Four-part fracture
2) Head-splitting fracture
3) Neck fracture with a long calcar segment
4) Disrupted medial periosteal hinge
5) AO type C3 fracture
A long calcar fracture segment, also known as the posteromedial metaphyseal head extension, is a good prognostic sign against the development of osteonecrosis in displaced proximal humerus fractures.
The humeral head is directly supplied by the anterior and posterior humeral circumflex arteries. Disruption of these vessels can result in humeral head osteonecrosis. Fracture patterns with long medial metaphyseal segments (greater than 8 mm) have not shown to critically disrupt the vascular supply to the humeral head causing osteonecrosis. Other factors shown to be protective against osteonecrosis after trauma include an intact medial hinge and simple fracture patterns.
Hertel et al. examined the factors predictive of osteonecrosis of the humeral
head after fracture. These include four-part fragments, angular displacement
>45 degrees of the head, displacement of the tuberosities greater than 10 mm, glenohumeral fracture-dislocation, and head-splitting fractures.
In Hertel's second paper and follow up study they noted that the initial post-fracture humeral head ischemia does not predict development of necrosis.
Illustration A shows an example of a long and short calcar fracture segment. Illustration B shows the AO classification of proximal humerus fractures.
Incorrect Answers:
Answers 1,2,4,5: All these factors are predictive of osteonecrosis.
A 50-year-old female has been diagnosed with osteomyelitis of her left tibia. The infection is isolated to the meduallary canal of the bone, and her past medical history is significant for heavy smoking and chronic venous stasis. Based on the clinical staging of osteomyelitis, what would be her Cierney-Mader classification?
1) Stage 2A
2) Stage 1B
3) Stage 1C
4) Stage 3B
5) Stage 4C
The Cierny-Mader classification is a clinical classification based on clinical and anatomic features. This patient's Cierny-Mader classification is Stage 1B.
The Cierney-Mader classification system characterizes osteomyelitis in one of four anatomic stages. Stage 1 is confined to the medullary cavity of the bone. Stage 2 involves only cortical bone. Stage 3 is a localized infection to cortical and medullary bone. However, the bone remains stable. Stage 4 involves the entire thickness of the bone, with loss of bone stability. The Cierny-Mader system also sub-characterizes patients as A, B, or C. The [A} patients have no systemic or local immune compromising factors. The [B] patients have one or more systemic or local compromising factors. The [C] patients are severely immunocompromised and treatment will lead to greater morbidity than the infection.
Mader et al. described the treatment algorithm of osteomyelitis using the Cierny-Mader classification. Treatment involves both antibiotic and surgical debridement. For type 1 infection, thorough intramedullary reaming and unroofing is usually performed.
Illustration A shows a table for the Cierny-Mader classification. Illustration B shows a schematic illustration of the anatomical involvement of osteomyelitis using the Cierny-Mader classification.
Incorrect Answers:
Answer 1: This would be a cortical infection only in a healthy patient. Answer 3: This would be a medullary cavity infection only in a severely compromised patient.
Answer 4: This would be a localized infection to cortical and medullary bone in a patient with one or more systemic or local compromising factors.
Answer 5: This would be a diffuse infection involving the entire bone in a severely compromised patient.
A 68-year-old female sustains a fall to her dominant arm and sustains the fracture seen in Figure A. She undergoes uneventful open reduction internal fixation with a locked plate and screw construct. Which of the following radiographs (Figures B, C, D, E, or F) show the most common complication associated with this treatment modality?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Figure B shows screw penetration of the articular surface, which is the most common complication following locked plate and screw fixation.
Inadequate fixation, typically in the humeral head, subsequently fails leading to varus deformity and screw penetration. This most commonly occurs in fixation for 3 and 4 part fractures, but can also occur following fixation for 2 part fractures.
Egol et al. retrospectively reviewed 51 patients following locked plating of 3-and 4-part proximal humerus fractures, they found 16% had screw penetration. The authors recommended ensuring appropriate number and length of the screws placed to prevent cut-out.
Brunner et al. reviewed 158 proximal humerus fractures. They found at 1 year follow-up noted 14% screw penetration rate. They recommended close followup to monitor for cut-out.
Figure A shows a 3-part proximal humerus fracture. Figure B exhibits varus cut-out and screw penetration. Figure C exhibits non-union and fixation failure. Figure D exhibits avascular necrosis and complete head collapse. Figure E (arrow) exhibits changes consistent with heterotopic ossification.
Figure F exhibits non-union and fixation failure at the level of the shaft.
Incorrect answers:
Answer choice 2/5 (figure C/F): Non-union and fixation failure can also occur, but at a relatively low rate.
Answer choice 3 (Figure D): Avascular necrosis also occurs, but at a lower rate than screw penetration.
Answer choice 4 (Figure E): Heterotopic ossification (arrow) can occur but is rare.
Figure A shows an acute, isolated and closed, left knee injury in a 40-year-old male struck by a motor vehicle. What would be the most
appropriate surgical fixation for this injury?
1) Definitive external fixation
2) Temporary external fixation then lateral percutaneous screws
3) Lateral nonlocking plate +/- bone graft substitutes
4) Medial and lateral locking plate +/- bone graft substitutes
5) Lateral percutaneous screws with assisted arthroscopy
This patient has sustained a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. The most appropriate treatment of this fracture would be fixation with a lateral nonlocking plate +/- bone graft substitute.
Displaced, widened and depressed tibia plateau fractures are an indication for operative intervention. The aim of surgery is to restore anatomic articular congruity, length, alignment and rotation of the proximal tibia. This is best achieved by (1) direct reduction of the articular surface, and (2) fixation of the interfragmentary piece with a plate and screw construct, which provides subarticular support, interfragmentary compression, and prevents shearing of the fracture. In patients with good bone quality, this is best achieved with an undercontoured lateral nonlocking plate in buttress mode.
Karunakar et al. showed that there was no significant difference between split depression tibial plateau fractures (Shatzker II) fixed with either (1) buttress plate with rafting screws versus (2) periarticular plate with built in rafting screw hole options.
Gardner et al. examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Figure A provided a sequence of coronal CT scan images of a left knee. There is a lateral split depression tibial plateau fracture with significant joint
depression, articular impaction and condylar widening.
Incorrect Answers:
Answer 1: Definitive external fixation of tibial plateau fractures may be considered in patients who are unable to tolerate definitive surgery, severe open fractures, infections, or significant bone loss.
Answer 2: Temporary external fixation would be considered in patients with significant soft tissue injury.
Answer 4: Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure. Medial plating would support a bicondylar fracture.
Answer 5: Screws alone are unlikely to be adequately stable in this patient. Although not commonly employed, knee arthroscopy is considered by some surgeons to be a valuable method to assist in obtaining the best articular surface reduction during surgery.
An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two non-locking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?
1) Absolute stability with direct healing by callus formation
2) Relative stability with indirect healing by callus formation
3) Absolute stability with direct healing by internal remodeling
4) Relative stability with indirect healing by internal remodeling
5) Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Restoration of the radial bow, length, and alignment in conjunction with primary bone healing would optimize the restoration of pronation/supination in the forearm. Compression plating and anatomic reduction of articular fractures are examples of absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting.
Moed et al. reviewed 56 patients with open diaphyseal forearm fractures treated with immediate internal fixation. The complications included deep infection in 2 patients and non-union in 6. This study indicated immediate stable plate fixation was a beneficial method of treatment for open diaphyseal forearm fractures.
Jones et al. discussed current literature on treating adult diaphyseal forearm fractures with open reduction internal fixation versus intramedullary nailing, and concluded a randomized prospective study is needed. They stated current literature is inconclusive.
Figure A shows a both bone forearm fracture fixed with absolute stability. The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Incorrect Answers:
Answers 1-2, 4-5: Absolute stability is a biological process of osteonal bone remodelling. This is predominantly intramembranous ossification. Enchondral bone formation occurs in non-rigid fracture healing (secondary bone healing).
A 27-year-old man sustains a tibial plateau fracture as pictured in Figure A-D. Which combination of fixation constructs and stability
would optimize his outcome?
1) Intramedullary nailing for a relative stability construct
2) Posteromedial buttress plating for an absolute stability construct
3) Locked lateral plating an absolute stability construct
4) Medial antiglide plating for a relative stability construct
5) Spanning external fixation for an absolute stability construct
Intraarticular tibial plateau fractures require absolute stability constructs to maintain anatomic joint reductions without callus formation. This condylar split fracture is ideally treated with buttress fixation at the apex of the fracture to avoid the high likelihood of shear failure with a laterally placed fixed-angle construct.
Tibial plateau fractures in young adults are high energy injuries, and the condylar split components of the fractures occur due to shear failure. The mechanism of failure - axial loading combined with a varus or valgus moment with the knee extended or flexed - dictates the orientation of the condylar split fracture line(s). There are multiple fracture classification schemes that assist with surgical decision making, particularly with placement of buttress plate fixation to resist shear failure. Articular impaction and joint depression must also be addressed.
Bai et al. performed a biomechanical study on fresh cadavers to simulate residual articular step-offs after fixation. With a >5 mm step-off, contact pressures increased over 200%.
AO guidelines of tibial plateau fracture management are discussed in depth in AO Principles of Fracture Management, and up-to-date principles can be found on the AO surgery reference. Anatomic reduction and absolute stability are important elements of all intraarticular proximal tibia fractures.
Figures A and B are injury films of a tibial plateau fracture with a large posterior split of the medial condyle. Figure C shows an axial CT cut displaying the same fracture. Illustrations A-C show how the injury was treated. Through a posterior incision, an under-contoured anti-glide plate was used to reduce the fracture at the apex. Subsequently, a pre-contoured posteromedial buttress plate was placed to maintain the reduction. The articular reduction was finalized with rafting screws outside of the plating construct to optimize the angle of subchondral support.
Incorrect Answers:
Answers 1, 4: Relative stability is inappropriate for intraarticular fractures that require anatomic reductions
Answer 3: Laterally-based locked plating for a medial condyle fracture creates large moments about the screw-plate interface, and the construct is apt to fail in shear
Answer 5: Spanning external fixation is most commonly used for temporizing tibial plateau fractures when significant soft tissue is present - in the absence of additional fixation for a hybrid construct, it would provide relative stability
Surgical fixation with absolute stability would be most appropriate for which of the following fracture patterns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Anatomic reduction and fixation with absolute stability is appropriate for articular fractures, such as posterior malleolar ankle fractures with significant joint involvement.
Compression plating and anatomic reduction of periarticular fractures yield absolute stability. Fractures treated with absolute stability achieve primary bone healing. Posterior malleolar ankle fractures comprising greater than 25% of the joint and non-comminuted lateral malleolar ankle fractures are typically treated with internal fixation to achieve absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting. In fractures with significant comminution and in lower extremity diaphyseal long bone fractures, relative stability is employed.
Gardner et al. surveyed members of the Orthopaedic Trauma Association (OTA) and American Orthopaedic Foot and Ankle Society (AOFAS) regarding treatment of posterior malleolus ankle fractures. They found that size influenced decision making, with 97% electing to treat those posterior malleolus fractures that comprised 50% of the joint. The most common used
approach was the posterolateral approach, which utilizes the interval between the flexor hallucis longus and peroneals.
Forsberger et al. reviewed 45 consecutive patients treated with surgical fixation of the posterior malleolus through the posterolateral approach. This approach allowed excellent exposure with few soft tissue complications.
De Vries et al. reviewed 45 patients with ankle fractures that had a posterior malleolar component. Those patients that had the posterior malleolar fragment fixed did not have statistically better functional scores than those who did not have the fragment fixed. They concluded that those patients with fragment sizes less than 25% did not require fixation and had good functional outcomes at 13 year follow-up.
Figure A shows an AP and lateral radiograph of a right comminuted distal third radial shaft fracture. Figure B shows an AP and lateral radiograph of a lateral and posterior malleolar ankle fracture in addition to a deltoid rupture. Figure C shows an AP and lateral radiograph of a comminuted middle third tibial shaft fracture. Figure D shows an AP radiograph of a minimally displaced greater trochanter fracture. Figure E shows an AP and lateral radiograph of a pediatric distal radial metaphyseal fracture. Illustration A shows an AP, mortise, and lateral radiograph of a posterior and lateral malleolus ankle fracture treated with open reduction and internal fixation.
Incorrect answers:
Answer 1: Significant comminuted radial shaft fractures are treated with bridge plating, which would achieve relative stability.
Answer 3: Diaphyseal tibial fractures are treated with intramedullary nailing, which achieves relative stability.
Answer 4: Minimally displaced greater trochanter fractures are treated nonoperatively.
Answer 5: Pediatric distal radius fractures are typically treated with closed reduction and casting, which achieves relative stability.
Figures A and B are radiographs of a 72-year-old male who presented to hospital 3 days after an unwitnessed fall. He presents with pain and the inability to mobilize since the fall. The patient lives independently and has no significant past medical history. Physical examination reveals an alert and oriented patient. This is an isolated injury with no other focal or systemic deficits. What would be the most important investigation to be obtained before taking this patient to the operating room?
1) Pelvic inlet and outlet views
2) CT head
3) Duplex ultrasound of both lower extremities
4) CT hip and pelvis
5) MRI hip and pelvis
The most appropriate investigation to order in this patient would be a duplex ultrasound of both lower extremities.
Immobilized elderly patients with a delay of more than two days from the fracture to presentation at the hospital are at a higher risk of deep-vein thrombosis (DVT). The risk can be higher in patients with factors that predispose to clot formation, such as malignancy. Patients with a delayed presentation to hospital should be investigated for DVT. The most common screening modality is duplex ultrasound of both lower extremities.
Hefley et al. looked at the effect of delayed admission to the hospital on the preoperative prevalence of DVT associated with hip fractures. They found that 6 out of 11 patients with a delay of more than two days between the fracture and admission to the hospital had evidence of thrombosis. They conclude all patients with delayed admission, after a hip fracture, should be evaluated for DVT preoperatively.
Figure A and B are AP and lateral radiographs that show a displaced left subcapital hip fracture.
Incorrect Answers:
Answer 1: There is no indication of pelvic inlet and out views. Generally speaking, pelvic inlet and outlet views assess the pelvic ring and pelvic bone stock, which are normal in this patient.
Answer 2: CT head would be indicated after an unwitnessed fall if the patient admitted to head injury, had neurological symptoms or acute focal/systemic deficits on exam. None of these are present in this patient.
Answer 4 and 5: A CT or MRI of the hip and pelvis are not indicated in a displaced fracture, but may be useful in diagnosing nondisplaced fractures.
A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?
1) Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
2) Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
3) Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
4) A delay in surgery greater than 48 hours is acceptable if the patient has multiple medical comorbiditiesm which are not fully optimized
5) Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months.
Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of early surgery on incidence of AVN. However, delay of internal fixation of more than 24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Answer 1: Patients treated with hemiarthroplasty or total hip arthroplasty
demonstrated no statistically significant difference in mortality.
Answer 2: Arthroplasty consistently has better outcomes compared to internal fixation for the treatment of unstable/displaced (Garden III and IV) femoral neck fractures in elderly patients.
Answer 3: Outcomes of unipolar and bipolar hemiarthroplasty for unstable femoral neck fractures are similar.
Answer 5: Dislocation rates are higher with total hip arthroplasty compared to hemiarthroplasty.
An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?
1) Intramedullary nail
2) Hemiarthroplasty
3) Closed reduction percutaneous pinning
4) Total hip arthroplasty
5) Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture
Incorrect answers:
Answers 1, 3, 5 are not the treatment standards for displaced femoral neck fractures in the elderly.
Answer 4 is incorrect because the patient is minimally ambulatory at baseline with little independence.
A 20-year-old female arrives to the trauma bay following a motor vehicle accident. She was a restrained driver and has bilateral chest tubes placed in the trauma slot. Initial laboratory values are significant for a hematocrit of 45.5 g/dL and a lactate of 7 mmol/L. Both lower extremities exhibit grossly open wounds. Radiographs are shown in Figure A and B. What is the best initial management of her orthopaedic injuries?
1) Irrigation and debridement of left femur and right tibia with bilateral external fixator placement
2) Irrigation and debridement of left femur and right tibia with left external fixator placement and right tibial intramedullary nail placement
3) Irrigation and debridement of left femur and right tibia with left femoral and right tibial intramedullary nail placement
4) Irrigation and debridement of left femur and right tibia with left femur open reduction and internal fixation and right tibial intramedullary nail placement
5) Irrigation and debridement of left femur and right tibia with bilateral long leg splint placement
Presenting as an unstable patient, damage control orthopaedics (DCO) should be performed by placing bilateral external fixators following irrigation and debridement.
Signs of clinical instability include an elevated lactate level as well as injuries to both lungs, necessitating bilateral chest tubes. Furthermore, while the patient is young and her hematocrit reflects a 'normal' number, more likely is a hypovolemic state due to bilateral open long bone injuries. Resuscitation is required and early total care (ETC) should be avoided.
Pape et al. review the early data regarding DCO and ETC. Identification of patients in extremis, borderline, unstable or stable patients is critical to determining appropriate management. Adequate resuscitation, by tracking lactate, as well as full evaluation of the multiply injured patient is crucial in determining application of DCO versus ETC. DCO is necessary as a temporizing stage to improve mortality in critically injured patients.
Renaldo and Egol revisit the evolution of trauma care where early, acute treatment evolved to ETC, and again to the development and implementation of DCO and staged fixation. Reviewing the initial post-traumatic inflammatory response, the authors review literature that supports the implementation of DCO in the unstable patient, especially the role of the 'second hit' phenomenon and the spike in inflammatory cascade that occurs between days 2-5 following injury.
Figure A is a lateral x-ray of a comminuted, displaced, open distal femur fracture. Figure B is an anteroposterior radiograph of a spiral, oblique, open tibia fracture.
Incorrect Answers:
Answers 2-4: Due to the elevated lactate levels and unstable nature of the patient, DCO should be applied via placement of external fixators. Definitive fixation at this time could worsen the patient's acute condition and subsequent
morbidity and mortality.
Answer 5: This patient, while unstable, is not in extremis, therefore temporary skeletal stabilization should be placed with external fixators.
Figure A is a radiograph of a 31-year-old male cyclist who was struck by a vehicle. Physical examination revealed a 2 cm opening in the skin over the anteromedial leg. He was treated operatively with an unreamed intramedullary nail. What outcome can be expected using this operative modality when compared with reamed intramedullary nailing?
1) Higher rates of nonunion
2) Higher rates of malunion
3) Higher rates of infection
4) Lower rates of infection
5) No difference
The best definitive surgical fixation option for an open fracture of the tibia would be either a reamed or unreamed intrameduallary nail.
Treatment of open tibia fractures require immediate antibiotics and early
irrigation and debridement. Surgical fixation options are vast, but largely based on the severity of injuries both locally or systemically. External fixation devices are mainly used for provisional fixation in polytrauma patients or definitively in proximal or distal metaphyseal fractures. Plating may be used in a staged fashion after a period of external fixation. The most common fixation method is intramedullary nailing. The use of a reamed or unreamed nail technique does not affect union rates, infection rates, or need for additional surgeries in open tibia fractures.
Bhandari et al conducted a multicenter, blinded randomized trial of 1319 adults in whom a tibial shaft fracture was treated with either reamed or unreamed intramedullary nailing. When comparing outcomes in open and closed injuries at twelve months, they found a benefit for reamed intramedullary nailing in patients with closed fractures, but found no difference between approaches in patients with open fractures.
Finkenmeier et al conducted a randomized controlled study of reamed vs. unreamed nails in open and closed tibia fractures (excluding Grades IIIB and IIIC). They found that the use of reamed insertion of IM nails for the treatment of closed tibia fractures lead to an earlier time to union without increased complications. The authors reported no differences in infection rate, compartment syndrome rate, or percent needing additional surgeries to obtain union. More secondary procedures were needed with unreamed nails in closed fractures only.
Figure A shows a mid-shaft tibia fracture. Incorrect Answers:
Answers 1, 2, 3, 4: All prospective studies show no difference in the rates of
non-union, malunion, or infection when using a reamed or unreamed nails to treat open tibia fractures.
A 27-year-old male presented to the trauma bay following a motor vehicle crash and was diagnosed with a comminuted open tibia fracture. He was subsequently treated with an irrigation and debridement, and un-reamed intramedullary nail. At 4 months followup, despite some signs of healing, the fracture is not fully united. Which of the following is true?
1) Patient should be scheduled for exchange nailing.
2) Use of an un-reamed nail increased this patients risk of infection.
3) Use of an un-reamed nail increased this patient's risk of non-union.
4) Patient should continue to be observed without intervention.
5) Use of an un-reamed nail decreased this patient's risk of infection.
Tibia fractures, open or closed, when treated with an intramedullary nail can take 6 months or longer to achieve clinical and radiographic healing, and should be observed for at least 6 months before secondary intervention is considered.
Open tibia fractures should be managed with debridement and irrigation initially. The choice of definitive fixation between reamed and unreamed nailing remains controversial. Recent randomized controlled studies have examined the outcomes of reamed and unreamed nailing for both closed and open tibia shaft fractures.
Bhandari et al. present a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. Surgeons participating in the study were mandated to delay intervention for delayed union/nonunion until 6 months after the initial procedure. The authors found that many tibia fractures in both the reamed and unreamed nailing groups progressed to union without secondary intervention with this 6 month delay.
Finkemeier et al. present a prospective randomized trial of tibia fractures treated with reamed or un-reamed intramedullary nails. For closed fractures they found a higher rate of union at 4 months in the reamed group, but no difference at 6 or 12 months. There was no difference in union rates for open fractures at any time point. They found no differences in other variables such as infection or compartment syndrome.
Incorrect answers:
Answer 1: This fracture has signs of healing at 4 months, and should continue to be observed until at least 6 months before a secondary operation is considered.
Answers 2 and 5: There is no difference in infection risk between reamed and un-reamed nails for open tibia fractures
Answer 3: There is no difference in rate of eventual union between reamed and un-reamed nails for open tibia fractures.
A 27-year-old male sustains a type I open both bone forearm fracture as seen in Figure A. During irrigation and debridement a 1 cm of cortex is removed leaving a segmental gap. Which of the following adjuvants is recommended to supplement your internal fixation?
1) Bone grafting
2) Tricalcium phosphate
3) Calcium phosphate
4) Calcium sulphate
5) BMP-3
Bone grafting in the primary fixation of fractures is typically limited to those with segmental defects. While the increased surface area of a comminuted fracture may aid in the healing potential, the segmental defect is a limiting factor to fracture healing. Calcium sulphate, tricalcium phosphate, BMP-3, and calcium phosphate are not indicated in this clinical picture. BMP-2,4,6, and 7 all have osteoinductive activity but BMP-3 does not demonstrate osteoinductive activity.
In their retrospective review of 198 fracture, Wright et. al found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental bone defect.
Wei et. al also performed a retrospective review of 64 fractures in 49 patients and found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental defect.
Finally, Schemitsch and Richards determined that optimal outcome post forearm fracture depends on restoration of the radial bow.
A 30-year-old female falls onto her outstretched arm and sustains the injury shown in Figures A and B. After intra-articular lidocaine injection, her elbow range of motion is 30°-95° extension/flexion, 45° supination, 65° pronation. There is no wrist tenderness and the radius pull test is symmetric to the contralateral forearm. What is the most appropriate treatment?
1) Fragment excision via the extensor carpi ulnaris / anconeus approach
2) Internal fixation with headless compression screws via the brachialis / pronator teres approach
3) Internal fixation with a periarticular plate via the extensor carpi ulnaris /
anconeus approach
4) Radial head arthroplasty via the brachialis / pronator teres approach
5) Sling and early elbow range of motion
This patient has a Mason type III radial head fracture composed of two articular fragments with a mechanical block to motion and should be treated with open reduction internal fixation (ORIF) using a lateral approach to the radial head.
Treatment of radial head fractures depends on fracture anatomy, elbow/forearm motion and ipsilateral forearm injury. Minimally displaced fractures with no mechanical block to motion (Type I; see Illustration C) are most common and are treated with a sling and early motion. Displaced fractures with one fragment (Type II) and block to motion are often managed with ORIF. Fragments less than ~30% of the articular surface may be excised, provided there is no concern for ipsilateral forearm instability. Displaced multi-fragmentary fractures (Type III) are usually managed with radial head arthroplasty, but may be treated with ORIF in young patients with less than three fragments.
Ring et al. performed a retrospective study of 56 patients who underwent radial head ORIF. Patients with more than three articular fragments had significantly poorer patient outcome scores, loss of forearm rotation and required more secondary procedures to ultimately resect the radial head. The authors concluded that ORIF is effective for fractures with less than three articular fragments and that fractures with three or more fragments are better managed with prosthetic replacement.
Ruchelsman et al. reviewed radial head and neck fractures. Choice of treatment is impacted by fragment number, size (percentage of articular disc), comminution and stability, as well as radiocapitellar alignment and block to motion. When feasible, ORIF allows restoration of anatomic congruity and initiation of early motion. Radial head arthroplasty is preferred for radial head fractures with multiple fragments or if stable fixation cannot be ensured.
Figures A and B are the AP and lateral radiographs of the left elbow showing a displaced complete articular radial head fracture with two articular fragments [Ruchelsman et al.]. Illustrations A and B are fluoroscopic images showing subsequent fixation of the fracture with a periarticular plate [Ruchelsman et al.]. Illustration C is the Mason classification of radial head fractures.
Illustration D is an intraoperative photograph showing exposure of the radial head fracture via the Kocher approach (extensor carpi ulnaris / anconeus
interval).
Incorrect Answers:
Answer 1: While the patient has no evidence of ipsilateral distal radioulnar joint or interosseous membrane injury (no wrist tenderness, normal radius pull test), fragment excision is reserved for partial articular fractures involving less than 30% of the articular surface. Complete radial head resection can lead to long-term elbow dysfunction and should be reserved for elderly, low-demand patients.
Answer 2: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. ORIF can be performed with either headless compression screws or periarticular plates. Use of headless compression screws has been associated with improved postoperative ROM compared to plates.
Answer 4: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. Radial head arthroplasty should be reserved for older patients and fractures with three or more articular fragments.
Answer 5: Nonoperative treatment is not appropriate for this patient with a displaced fracture and mechanical block to motion.
What nerve is most at risk when applying the external fixator shown in Figure A using a minimally invasive fluoroscopic technique of pin insertion?
1) Ilioinguinal nerve
2) Obturator nerve
3) First branch of the femoral nerve
4) Lateral femoral cutaneous nerve
5) Superior gluteal nerve
Pelvic external fixation with supraacetabular pins through the AIIS can be utilized to stabilize a pelvic fracture. While using this technique, care must be taken not to injure the lateral femoral cutaneous nerve (LFCN). Gardner et al describe the technique for placement of supraacetabular external fixation pins and state that pins in this location are more stable biomechanically compared to other locations in the iliac crest. Grothaus et al performed a cadaveric study to determine the anatomic detail and variation of the LFCN and the distances it traveled from various landmarks.The found the nerve to potentially be at risk as far as 7.3 cm medial to the anterior superior iliac spine along the inguinal ligament and as much as 11.3 cm distal on the sartorius muscle from the anterior superior iliac spine. Riina et al performed a cadaveric study to define the neurovascular structures at risk with the placement of anterior-posterior locking screws in the proximal femur. They found that risks to the neurovascular structures during anterior-posterior locking in the proximal femur are diminished if locking is performed above the level of the lesser trochanter.
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?
1) Sural nerve injury
2) Tethering of the flexor hallucis longus by fracture fragments
3) Medial plantar nerve neuropathy
4) Weakness of the tibialis posterior
5) Unrecognized foot compartment syndrome
Contracture of the intrinsic flexor muscles of the foot can be the result of unrecognized foot compartment syndrome. Foot compartment syndrome is a known complication of calcaneus fractures.
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal.
The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
A 25-year-old male sustains a closed elbow dislocation after falling during a soccer game. Two months later, the patient continues to complain of pain and instability. Radiographs and physical exam are concerning for posteromedial instability. Which of the following fracture patterns is most consistent with this diagnosis?
1) Coronoid tip
2) Coronoid anteromedial facet
3) Radial head
4) Olecranon
5) Capitellar impaction injury
of coronoid fractures, they indicate that identification of anteromedial facet injuries is often difficult and that treatment should be instituted promptly to limit persistent instability and subsequent arthritis.
Illustration A shows an AP radiograph of the affected elbow. An event of posteromedial instability is evidenced by the fracture through the anteromedial facet of the coronoid. Illustrations B and C show the AP and lateral radiographs of a patient who developed significant arthrosis after inadequate treatment of varus posteromedial rotatory instability.
Incorrect answers
Answers 1, 3, 5: These injuries may be seen as the sequlae of posterolateral rotatory instability.
Answer 4: Large coronoid fractures are seen in olecranon fracture-dislocations around the elbow.
A 7-year old boy presents to the emergency room following a ATV accident with complaints of left pelvic pain. In the emergency room he is alert and oriented and is hemodynamically stable. On physical exam he is unable to bear weight on his left lower extremity. There is no tenderness to palpation at the posterior pelvis. A radiograph is performed and shown in Figure A and CT examination shows the posterior ring is stable and age-appropriate. What is the most appropriate treatment for this injury pattern?
1) Nonoperative management with weight bearing as tolerated
2) Percutaneous sacroiliac screw
3) Pelvic external fixation
4) Anterior pelvic ring plating
5) Anterior and posterior pelvic ring plating
The clinical presentation is consistent for a mildly displaced parasymphyseal fracture in a pediatric patient with an open triradiate cartilage. Weight bearing as tolerated is the most appropriate treatment.
In skeletally immature pelvic ring fractures, the majority of cases can be treated nonoperatively. Open reduction and internal fixation is required for acetabular fractures with >2 mm of fracture displacement and for any intraarticular or triradiate cartilage fracture displacement >2 mm. External fixation is necessary for pelvic ring displacement of >2 cm to prevent limb-length discrepancies.
Holden et al. emphasize that children with open triradiate cartilage have
different fracture patterns than do children whose triradiate cartilage has closed. They report because of the immaturity of the pelvis, the iliac wing is weaker than the elastic pelvic ligaments, resulting in bone failure before pelvic ring disruption has a chance to occur. For this reason fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment.
Spiguel et al. reviewed 2850 pediatric trauma admissions at their institution and reviewed cases with a pelvic ring fracture. They found that although pelvic fractures are an uncommon injury in pediatric trauma patients, the morbidity associated with these injuries is significant. They report while the majority of pelvic fractures in children are treated nonoperatively, more than one-half of these patients have concomitant injuries requiring operative management.
Figure A shows an inferior rami fracture in a pediatric patient with an open triradiate cartilage.
Incorrect Answers:
Answers 1,3,4,5: These treatment options are not appropriate in a stable pelvic ring fracture in a child with open triradiate cartilage.
A 75-year-old-male presents after being struck by a vehicle while crossing the street. He complains of right leg pain, and physical exam reveals no evidence of an open fracture. Initial radiographs are shown in Figures A and B, and intramedullary nailing of the fracture is planned. What is the proper blocking screw technique to prevent apex anterior and valgus deformity of the fracture?
1) Insertion of blocking screws lateral and posterior to the nail
2) Insertion of blocking screws medial and posterior to the nail
3) Insertion of blocking screws lateral and anterior to the nail
4) Insertion of blocking screws medial and anterior to the nail
5) Insertion of blocking screws medial, lateral, and posterior to the nail
Apex anterior and valgus deformity of the proximal tibia fracture can be prevented by inserting blocking screws lateral and posterior to the nail in the proximal segment.
Blocking screws may be used to prevent deformity when performing intramedullary fixation of proximal tibia fractures. Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to prevent valgus deformity. Stability screws can be placed prior to insertion of the nail to prevent deformity during nail passage, or after nail insertion to prevent postoperative deformity from developing.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibial shaft. Post-operatively, all patients in their series had less than 5 degrees
of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Figures A and B demonstrate a segmental tibial shaft fracture. Illustration A shows an intraoperative fluoroscopic image demonstrating insertion of the blocking screws intraoperatively. Illustrations B and C show post-operative radiographs demonstrating placement of the blocking screws and adequate alignment of the proximal segment.
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. As an alternative to lactate and base deficit measurements, which of the following would best indicate adequate resuscitation has been achieved?
1) Systolic blood pressure > 120
2) Heart rate between 60-100
3) Urine output equals 0.4 cc/kg/hr
4) Gastric intramucosal pH of 7.4
5) Potassium between 3.5-4.5
Of the following variables, only a normal gastric mucosal pH (>7.3) is associated with restoration of tissue oxygenation.
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism
with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Answers 1-3: A patient may have normalized blood pressure, heart rate, and urine output but may still be in a state of compensated shock requiring further resuscitation.
Answer 5: Potassium levels do not assess adequate resuscitation
A 32-year-old man sustains the knee injury seen in Figure A after falling from a ladder. Which of the following options is the most biomechanically stable and appropriate definitive surgical treatment?
1) Spanning knee external fixation
2) Lateral plateau locking plate
3) Posteromedial locking plate
4) Lateral plateau percutaneous lag screws and posteromedial plate
5) Lateral plateau and posteromedial plating
The above clinical scenario is consistent with a bicondylar tibial plateau fracture. Bicondylar tibial plateau fractures are best definitively treated with dual incision technique using separate lateral plateau and posteromedial plates.
Yoo et al perfored a biomechanical study comparing locking and nonlocking single and dual plating constructs in maintaining posteromedial fragment reduction in a bicondylar tibial plateau fractures. They found that the posteromedial fracture fragment tolerated higher loads with a posteromedial conventional plate construct. The superiority of this dual plating construct may be caused by unreliable penetration of the posteromedial fragment by the lateral locking screws alone.
Zeng et al also performed a biomechanical study comparing the biomechanical strength of four different fixation methods for the posteromedial tibial plateau split fracture. The four following constructs: anteroposterior lag-screws, an anteromedial limited contact dynamic compression plate (LC-DCP), a lateral locking plate, or a posterior T-shaped buttress plate were studied. They found that the posterior-based buttress plating technique was the most biomechanically stable fixation method allowing the least amount of fracture subsidence for posteromedial split tibial plateau fractures.
Figure A shows an AP radiograph of a bicondylar tibial plateau. Illustration A shows a post-operative radiograph following the dual-plating technique for bicondylar tibial plateau fractures.
Incorrect answers:
Answer 1: External fixation is not the most appropriate definitive care for bicondylar tibial plateau fractures.
Answers 2-4: Not as biomechanically stable as dual plating technique for bicondylar tibial plateau fractures.
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?
1) Intraoperative anterior compartment measurement of 29, with preoperative diastolic pressure 58
2) Preoperative anterior compartment measurement of 25, with preoperative diastolic pressure of 60
3) Intraoperative anterior compartment measurement of 25, with intraoperative diastolic pressure of 54
4) Intraoperative anterior compartment measurement of 28, with intraoperative diastolic pressure of 72
5) Preoperative anterior compartment measurement of 22, with mean arterial pressure of 70
A delta P (diastolic blood pressure minus compartment pressure measurement)of
A 44-year-old male is involved in a motorcycle collision and presents with the radiographs shown in Figure A. A CT scan is obtained which shows intra-articular extension of the fracture, and lateral locked plating with intercondylar lag screw fixation is planned. Which of the following is important intra-operatively to ensure that the
intercondylar screws are contained within the bone and are of appropriate length?
1) AP fluoroscopic imaging with the leg in 30 degrees of internal rotation
2) AP fluoroscopic imaging with the leg in 30 degrees of external rotation
3) AP fluoroscopic imaging with the knee in full extension
4) Lateral fluoroscopic imaging with the knee in 30 degrees of internal rotation
5) Lateral fluoroscopic imaging with the knee in 15 degrees of flexion
Figure A illustrates a comminuted distal femur fracture. AP fluoroscopic imaging with the leg in 30 degrees of internal rotation is important to prevent intercondylar screw prominence.
Hardware irritation is a common post-operative complication of distal femoral plate fixation. Two common sites of pain are laterally where the iliotibial band is in contact with the plate, and medially where intercondylar screws may penetrate the cortex if they are of inappropriate length. Iliotibial irritation most commonly presents with activities requiring knee flexion and extension. It is important to remember that the lateral metaphysis of the distal femur is angulated 10 degrees from the sagittal plane, and the medial metaphysis is angulated 25 degrees from the sagittal plane. Therefore, if a straight AP view is obtained, a distal screw can appear to be inside the bone even if it is too long. In order to assess the exact length of the screw, one must obtain an AP view with 30° internal rotation of the lower extremity.
Gwathmey et al discuss distal femoral fractures in their review article. They state that the goal of surgical management is to promote early knee motion while restoring the articular surface, maintaining limb length and alignment,
and preserving the soft-tissue envelope with a durable fixation that allows functional recovery during bone healing. They describe a variety of surgical exposures, techniques, and implants developed to treat these injuries, including intramedullary nailing, screw fixation, and periarticular locked plating, possibly augmented with bone fillers.
Illustration A demonstrates the sagittal plane angulation of the medial and lateral cortex of the distal femur. Illustration B shows a knee in external rotation, with the intercondylar screw appearing to be of appropriate length. Illustration C shows the knee in internal rotation, which indicates that the screw is penetrating the medial cortex.
A 68-year-old male falls onto his outstretched hand and suffers the injury shown in Figures A and B. He undergoes operative treatment of his fracture, and immediate post-op radiographs are shown in Figure C. Two weeks later he presents with significantly increased pain and deformity. He denies any new trauma, and has followed all postoperative activity restrictions. Current radiographs are shown in Figure D and a clinical photograph of the affected wrist is shown in Figure E. Which of the following is the most likely cause for failure of fixation in this patient?
1) Failure to support the lunate facet with fragment specific fixation
2) Use of a non-locking plate
3) Lack of volar tilt restoration
4) Lack of radial styloid column plating
5) Use of only three bicortical screws in the intact radial shaft proximally
The failure of this patient's fixation post-operatively is caused by failure to support the lunate-facet fragment noted on the injury radiographs.
The stability of comminuted fractures of the distal part of the radius with volar fragmentation is determined not only by the reduction of the major fragments but also by the reduction of the small volar lunate fragment. The distal volar lunate fragment is the site of origin of the strong volar radiolunate ligaments which insert onto the lunate, and so displacement of this small piece volarly will allow the lunate and the rest of the carpus to subluxate volarly. The unique anatomy of this fragment may prevent standard fixation devices for distal radial fractures from supporting the entire volar surface effectively, as a standard volar plate cannot capture this small distal piece without risking injury to the flexor tendons. Fragment specific fixation of the volar lunate facet fragment with commercially available small plates, or with a tension-band construct or augmentation with K-wires may be required to reduce and stabilize this fragment.
Harness et al. reported on a cohort of 7 patients with a volar shearing fracture of the distal radius who lost fixation of a volar lunate facet fragment with subsequent carpal displacement after open reduction and internal fixation. Five patients underwent revision surgery with adequate results. The authors concluded that with regards to lunate facet fracture fragments, it is preferable to recognize the complexity of the injury prior to the initial surgical intervention and to plan accordingly to prevent early post-operative failure.
Taylor et al. compared the biomechanical stability of a fixed-angle volar plate versus a fragment specific fixation system in the treatment of an intraarticular, dorsally comminuted distal radius fracture model. They found that both fixed-angle volar plate and fragment-specific fixation systems performed comparably in a simulated early postoperative motion protocol. Fragment-specific fixation had improved stiffness characteristics only with respect to the smaller ulnar-sided fragment.
Figures A and B show a shearing radiocarpal-fracture subluxation with small lunate-facet fracture. Figure C shows an immediate post-operative radiograph. Figure D shows subluxation of the radiocarpal joint caused by failure to support lunate-facet fragment. Figure E shows the clinical appearance of a volarly subluxated wrist.
Incorrect Answers:
Answer 2: The use of a non-locking plate in this situation did not directly lead to the failure of fixation, and applying a similar construct with locking fixation
would not have prevented volar subluxation of the lunate facet fragment. Answer 3: Volar tilt was grossly restored post-operatively.
Answer 4: Radial styloid plating would not have prevented volar subluxation of the lunate facet fragment.
Answer 5: Three bicortical screws in the intact radial shaft proximally is adequate fixation.
Which of the following is most commonly associated with both simple and complex elbow dislocations?
1) radial head fracture
2) radial neck fracture
3) loss of terminal extension
4) repeat dislocation
5) coronoid base fracture
Elbow dislocations are classified as either simple (no associated fracture) or complex (associated fracture). The goal of treatment is a stable joint that tolerates early motion. The initial range of motion is the stable arc found on postreduction examination. Studies have demonstrated a better outcome when simple elbow dislocations are treated non-surgically rather than with surgical repair. Simple elbow dislocations usually have an excellent outcome (return of functional range of motion with normal strength). A loss of terminal extension is the most common sequelae.
Ross et al. reported on 20 patients with simple closed posterior elbow dislocations who were treated with immediate active ROM under close supervision. They found a final arc of motion of -4 to 139 degrees, with final motion reached a mean of 19 days after dislocation. Only 1 patient had recurrent instability.
A 36-year-old female sustains a knee injury after falling from a ladder onto her flexed knee; she cannot do a straight leg raise after a lidocaine injection into her knee. A radiograph is shown in Figure A. Which of the following treatment options has been shown to have the best outcomes with this injury?
1) Long leg cast
2) Hinged knee brace use with functional rehabilitation protocol
3) Open treatment with internal fixation or excision with patellar tendon advancement
4) Distal patellar resection and allograft reconstruction
5) Placement of a cerclage wire from patella to proximal tibia
The clinical presentation is consistent with and inferior pole patella fracture. Open reduction and internal fixation or excision with patellar tendon advancement is the most appropriate treatment of this injury pattern.
Whenever possible, salvage of the inferior pole through open reduction internal fixation is favored over simple excision and patellar tendon advancement, as this has been shown to be associated with improved outcomes. This is not always possible, however, and pole resection can be performed if the inferior comminution precludes fixation. Inferior outcomes of the partial distal patellectomy and patellar tendon advancement are (aside from the possible resulting patella baja) probably not directly related to the patellofemoral articulation. On the undersurface, the proximal 75% of the patella is covered with articular cartilage; however, the distal 25% is not, and does not articulate with the femoral trochlea.
Kastelec et al. performed a retrospective review of ORIF v. pole resection followed over 4.6 years postoperatively. There was a significant increase (better) in patellofemoral score with ORIF; significant differences in knee pain,
tolerated activity levels, and ROM were also noted. Patella baja was frequently noted with pole resection and correlated with worse functional outcomes.
Matejcic et al. performed a retrospective review of ORIF v. pole resection followed over 5.3 years postoperatively. Results were excellent/good in 90.1% of the ORIF and only 73.1% of the pole resection patients. In addition, significant differences between the groups were noted with regard to knee pain, swelling, level activity, compression pain, range of motion, muscular atrophy, muscular strength, and final patellofemoral score (all better with ORIF).
Figure A is a lateral knee radiograph showing an inferior pole patella fracture.
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?
1) Sling immobilization
2) Displacement and comminution
3) Age less than 40 years old
4) Immediate motion exercises
5) Male
Robinson et al have shown that lack of cortical apposition, comminution, female gender, and advancing age are the 4 factors that contribute to nonunion.
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p
A 34-year-old male presents after falling off a roof at his job. He has an obvious deformity of his left lower extremity, and injury radiographs are shown in Figures A and B. He has no other injuries. Which of the following definitive treatment algorithms will most likely lead to the best outcomes in this patient?
1) Closed reduction and percutaneous screw fixation of the femoral neck, followed by reamed antegrade nailing of the femur fracture
2) Reamed antegrade nailing of the femoral shaft fracture, followed by open reduction and percutaneous screw fixation of the femoral neck fracture
3) Reamed retrograde nailing of the femoral shaft fracture, followed by closed
reduction and percutaneous screw fixation of the femoral neck
4) Open reduction and screw fixation of the femoral neck, followed by reamed retrograde nailing of the femoral shaft fracture
5) Open reduction and screw fixation of the femoral neck, followed by plating of the femoral shaft fracture
The clinical presentation is consistent with a femoral shaft fracture with an ipsilateral femoral neck fracture. Of the options presented, the most appropriate treatment is open reduction and lag screw fixation of the femoral neck fracture followed by reamed retrograde nailing of the femoral shaft fracture.
Ipsilateral femoral neck/shaft fractures are an uncommon injury estimated to occur in 2-6% of all femoral shaft fractures. It is generally agreed upon that due to the potentially devastating complications of the femoral neck fracture in young patients, the neck fracture should be treated first and the shaft fracture second. Anatomic reduction of the femoral neck fracture is paramount in obtaining successful healing, and therefore open reduction is recommended in the setting of fracture displacement. Provisional reduction of the femoral neck fracture, followed by antegrade nailing with subsequent addition of definitive fixation of the femoral neck is also acceptable.
Peljovich et al. present a review article on ipsilateral femoral neck and shaft fractures. The treatment algorithm they propose consists of first treating the femoral neck fracture, and then addressing the femoral shaft fracture with retrograde nailing. They also highlight the risk and benefits of each treatment approach.
Watson et al. reviewed 13 patients who had healing complications after undergoing surgical fixation of their ipsilateral femoral neck and shaft fractures. They found that lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications. Therefore, this approach was recommended as the treatment of choice.
Figures A and B demonstrate an ipsilateral comminuted femoral shaft fracture, and a displaced femoral neck fracture. Illustrations A-C show an example of a femoral shaft fracture with an ipsilateral femoral neck fracture treated with lag screws of the femoral neck fx and retrograde nailing.
Incorrect Answers:
Answer 1: Open reduction of the femoral neck fracture with anatomic
alignment is preferred to closed reduction in this case.
Answer 2,3: The femoral neck fracture should be addressed first.
Answer 5: Nailing of the femoral shaft fracture would be preferred initially in this case to prevent disruption of the biology and fracture healing around the comminuted segments.
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?
1) Medial to lateral screw placement across lateral femoral condyle
2) Anterior to posterior screw placement across medial femoral condyle
3) Medial to lateral screw placement across medial femoral condle
4) Anterior to posterior screw placement across lateral femoral condyle
5) Anterior to posterior screw placement across intercondylar notch
The most common variation of a Hoffa fracture is a coronal fracture of the lateral femoral condyle. The most appropriate screw placement of the above answer choices in the treatment of the most common Hoffa fracture variant would be anterior to posterior screws across the lateral condyle for fixation.
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Illustration A shows sagittal and axial CT scan cuts showing a Hoffa fracture of the lateral femoral condyle. Illustration B shows multiple anterior to posterior, and posterior to anterior oriented screws for ORIF of the Hoffa fracture.
A 26-year-old right hand dominant male is involved in a motor vehicle collision and sustains the left humerus injury demonstrated in Figure A. The brachial artery is disrupted and requires urgent attention in the operating room. The patient's preoperative nerve evaluation demonstrates that the patient is unable to initiate extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis brevis, extensor digitorum, extensor indicis proprius, and extensor pollicis longus motor activity. What is the most likely etiology for this observed neurologic examination?
1) Neurapraxia of the median nerve
2) Axonotmesis of the radial nerve
3) Neurotmesis of the ulnar nerve
4) Neurotmesis of the radial nerve
5) Axonotmesis of the ulnar nerve
The most likely cause of the radial nerve palsy in a high energy open humerus fracture is laceration or complete disruption of the radial nerve (Neurotmesis).
Neurotmesis is complete disruption of nerve and is associated witn no spontaneous recovery without intervention. Axonotmesis constitutes axon disruption, but the surrounding neural connective tissue is intact and nerve regeneration can occur(Wallerian or antegrade degeneration). Neurapraxias occur often by compression and the axon maintains continuity but local demyelination and ischemia occur.
Ring et al. present a Level 4 study of 24 patients that had radial nerve palsy associated with a humerus fracture. All 6 patients with a transected radial nerve had an open humerus fracture also. The results of primary nerve repair in this circumstance found that there was no recovery in any of the patients.
Foster et al. authored a Level 4 review of 14 patients had a radial nerve palsy and an associated open humerus fracture. 64% of the 14 patients had a radial nerve that was either lacerated or interposed between the fracture fragments. They recommend exploration of the radial nerve in the setting of a radial nerve palsy and concomitant open humerus fracture in contrast to observation of a radial nerve palsy in closed humerus fractures.
Figure A demonstrates an open left humerus fracture.
Incorrect Answers:
Answer 1,3,5: The radial nerve provides distal motor activity to the ECRL, ECRB, EPB, EIP, and EPL.
Answer 2: Axonotmesis of the radial nerve is not the most common form of injury associated with closed or open humerus fractures.
Which of the following is true regarding the center of rotation of angulation (CORA) as it refers to tibial diaphyseal angular deformity?
1) It is the point at which the proximal mechanical axis and distal mechanical axis meet
2) It is the point at which the proximal anatomical axis and proximal mechanical axis meet
3) It is always the point on the cortex at the most concave portion of the deformity
4) It is the point at which the distal anatomical axis and distal mechanical axis meet
5) It is always the point on the cortex at the most convex portion of the deformity
The center of rotation of angulation(CORA) in diaphyseal tibial deformity is defined as the intersection of the proximal mechanical(PMA) or anatomical axis(PAA), and the distal mechanical(DMA) or anatomical axis(DAA).
Angular deformity of the femur or tibia involves angulation not only of the bone but also of its axes. When a bone is divided and angulated, the mechanical and anatomic axis of the bone are also divided into proximal and distal segments.
The pairs of proximal and distal axis lines intersect to form an angle. The point at which the proximal and distal axis lines intersect is called the CORA.
The axis line of the proximal bone segment is called the PMA or PAA, and axis line of the distal segment is called the DMA or DAA. In the tibia, because the mechanical and anatomical axes are almost the same, the PMA and PAA lines overlap, as do the DMA and DAA lines.
Illustration A shows the CORA as it relates to the axes of an angulated tibia.
Incorrect Answers:
2-5:These do not describe the CORA or any other specific anatomical points as they related to long bone deformity.
At long term follow-up, a male who sustains multiple traumatic injuries compared with a premenopausal female, who sustained similar polytrauma, is most likely to have which of the following?
1) Higher quality-of-life scores than females
2) Increased rates of complex regional pain syndrome
3) Require more psychiatric counseling and pharmacologic management than females
4) Take more absentee days at work as a result of illness than females
5) Decreased incidence of lower extremity amputation
Ten or more years after severe polytrauma, premenopausal women, compared to men, demonstrate a higher incidence of posttraumatic stress disorder (PTSD) and take more sick leave time from work.
Depression following polytrauma should be screened for by treating orthopaedic surgeons. Depression commonly arises from a protracted injury and can compound the disability by increasing the perception of more physical illness.
Probst et al. present a Level 4 review of over 600 polytrauma patients. They found that quality-of-life was significantly lower in women (Short form-12 psychologic F = 48.6 +/- 10.8 vs. M = 50.8 +/- 9.4; p = 0.02), but the same rate of women (75.3%) and men (75.4%; p = 0.995) felt well rehabilitated.
Holbrook et al. report a Level 4 study of 1,048 polytrauma patients. They found that females had lower quality-of-life scores and were significantly more likely to develop early combined depression.
Incorrect Answers:
Answer 4: Females take more absentee days at work.
Answers 2, 3, 5: There is no data supporting these answer options.
A 29-year-old healthy Caucasian female presents to the emergency department with her boyfriend with a left anterior shoulder dislocation and several facial abrasions after tripping in the shower approximately three hours prior to arrival. She is 5’7’’ and weights 120 lbs (BMI 18.8). The patient notes that she has not had a menstrual period in three months and that she is training for a long-distance triathlon. Physical examination reveals no other obvious injuries. Basic serum laboratory values are unremarkable. A urine pregnancy test is positive. In addition to treating her shoulder dislocation, the orthopaedic surgeon should
1) Perform a skeletal survey to evaluate for other fractures or dislocations
2) Question the patient in private about the specific details of this injury and her sense of safety in the home
3) Refer the patient to a nutritionist given the patient’s BMI of 18.8
4) Obtain additional laboratory studies and admit the patient to the hospital for treatment of anorexia nervosa
5) Obtain advanced imaging of the shoulder to evaluate for underlying pathologic lesions
for her current injury, it is imperative for health care providers to inquire into the safety of the home environment in potential cases of intimate partner violence (IPV).
Risk factors for female victims IPV include being in the 2nd or 3rd decade of life, current pregnancy, having 1 or more prior children, and low socioeconomic status. Reporting requirements for adult abuse are not standardized amongst most states and physicians must understand the importance of identification and documentation in cases of suspected IPV.
Bhandari et al. state that musculoskeletal injuries are the second most common form of IPV (28%) after head and neck injuries (40%).
Musculoskeletal injuries can be variable, including sprains, fractures, dislocations, and foot injuries.
Della Rocca et al. conducted a survey and found orthopaedic surgeons have several misconceptions regarding victims of IPV and further, nearly half of their survey respondents reported identifying a victim of IPV while only 4% reported that they currently screen their injured female patients for IPV.
Zillmer presents a review of the issues surrounding IPV including proper identification, documentation, appropriate questioning and how to involve community services.
Illustration A shows some basic facts regarding IPV during pregnancy as reported by the CDC. Additional information can be found at the following link.
[htt](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[p](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)
Incorrect Answers:
Answer 1. There is no indication for a skeletal survey and it would be inappropriate to subject this pregnant patient to additional radiation.
Answer 3. There is no need to refer a patient to a nutritionist for a normal BMI Answer 4. There is no indication for admission or other laboratory studies in this otherwise healthy patient.
Answer 5. There is no need for advanced imaging in the emergency department in the case of an isolated traumatic shoulder dislocation
A 19-year-old military recruit complains of 7 weeks of right heel pain. He notes the pain is worse with jumping and long distance running. He has completed a course of plantar fascia and Achilles tendon stretching with no significant improvement in his symptoms. He denies constitutional symptoms. On examination, his body mass index is 22, he has a normal foot posture and can perform a single leg heel rise without difficulty. There is no pain with palpation of the lateral border of the foot or with external rotation stress to the midfoot. There is tenderness with medial and lateral compression of the hindfoot and there is a negative syndesmosis squeeze test. There is a negative Tinel's sign at the tibial nerve. Axial and lateral radiographs are shown in Figures A and B. What is the most appropriate next step in management?
1) Heel pad cortisone injection
2) Platelet rich plasma injection and 6 weeks of physical therapy
3) Restricted weight bearing and magnetic resonance imaging of the foot
4) Release of the first branch of the lateral plantar nerve
5) ASTYM or Graston physical therapy techniques to the achilles and plantar fascia
Restricted weight bearing and magnetic resonance imaging of the foot is indicated in this military recruit with a positive heel compression test and suspicion for calcaneal stress fracture.
Calcaneal stress fractures occur as a result of repetitive loading and are more common in females with the female athlete triad (anorexia athletica) of disordered eating, amenorrhea, and osteoporosis. On exam tenderness is obtained with medial and lateral compression of the calcaneus.
Sormaala et al. performed a Level 4 review over 8 years of the Finnish military. They found 34 calcaneal stress fractures with 19 occurring in the posterior part of the calcaneus. Only 15% of the patients had the stress fracture visualized on plain radiography. They conclude that MRI is warranted if plain radiography does not show abnormalities in a physically active patient with exercise-induced pain in the ankle or heel. A nuclear medicine bone scan is also appropriate for diagnosis but MRI may give greater detail.
Gehrmann et al. present a Level 5 review of foot stress fractures. They report that with calcaneal stress fractures the fracture lines are oriented vertically or obliquely in the tuberosity of the calcaneus.
Figures A and B show some sclerosis in the central calcaneus with no evidence of overt fracture and an enthesophyte at the Achilles tendon insertion.
Illustration A and B are T2 sagittal and coronal images demonstrating a stress fracture in the superior calcaneal tuberosity with surrounding edema.
Incorrect Answers:
Answer 1: Heel pad cortisone injections are typically avoided due to risk of fat pad atrophy and are not indicated in calcaneal stress fractures.
Answer 2: Platelet rich plasma is not indicated in calcaneal stress fractures. Answer 4: The patient presents with a negative Tinel's at the tibial nerve and presentation is not consistent with first branch of the lateral plantar nerve entrapment.
Answer 5: ASTYM and Graston physical therapies are not indicated for calcaneal stress fractures.
A 35-year old male is involved in a fall from height and present with the isolated injury shown in Figures A and B. The body of the talus is extruded medially through a large linear open wound. Along with irrigation and debridement, what is the most appropriate definitive management of this injury?
1) Reimplantation of the talar body followed by cast immobilization
2) Reduction of talar body, fracture fixation with smooth Steinman pins, and spanning fixator placement
3) Talar body allograft with internal fixation to native talar head
4) Fragment removal, antibiotic spacer placement and external fixation
5) Reduction of native talar body and ORIF of talar neck fracture
The patient is presenting with a displaced talar neck fracture with extrusion of the talar body. Reimplantation of the talar body and ORIF of the talar neck fracture is the most appropriate treatment.
Talar extrusions are rare injuries and are caused by high energy mechanisms. Complete dislocation without a concomitant fracture is extremely rare. The talus is prone to dislocation as there are no muscular attachments. These injuries need to be treated with anatomic reduction and internal fixation to prevent avascular necrosis and post-traumatic arthritis.
Smith et al. investigated the clinical results and functional outcome after reimplantation of the extruded talus. They concluded that salvage and reimplantation of the talus is a relatively safe procedure with only 2 of the 27 patients developing an infection. No association was found between outcome and associated talar fracture.
Van Opstal et al. reported on two cases of talar extrusions following high energy injuries and reviewed the associated literature. Both cases were treated with wound I&D, reduction and external fixation. After 1 year they had pain free ROM with no signs of AVN or arthritis. Review of the literature showed that anterolateral dislocations are more common than anteromedial. Total talar dislocation is thought to be the endpoint of maximum pronation or supination injuries.
Figures A and B show an extruded talar body in the setting of a Hawkins III talar neck fracture. Illustration A shows a clinical photo of an extruded talus.
Incorrect Answers:
Answer 1: Displaced talar neck fractures should not be treated in a cast, especially open fractures
Answer 2: Definitive treatment of this injury is most effectively accomplished with formal ORIF. Steinman pin fixation is not adequate, even in the presence of an external fixator.
Answer 3: There is no data supporting removal of fragment and use of allograft overuse of native talar body
Answer 4: There is no data supporting removal of the fragment. The associated
Scientific References
- support retaining the fragment.
An 18-year-old male sustains a right hip injury after being tackled on the football field. Figure A shows his radiograph upon presentation to the emergency room three hours later. On physical exam, he is noted to have a foot drop and decreased sensation globally throughout his entire lower leg. Closed reduction under conscious sedation is immediately performed, and the hip is able to be ranged through a stable arc of motion following reduction. A post-reduction radiograph is shown in Figure B. Shortly after the reduction, the patient continues to have a foot drop, but his sensation is slightly improved. Which of the following is the most appropriate next step in management?
1) Exploration of his sciatic nerve
2) EMG
3) CT scan of his right hip
4) Touch-down weight bearing of his right leg and observation of his sciatic nerve palsy
5) Skeletal traction on the distal femur to relax tension on the sciatic nerve
Following successful reduction of a traumatic hip dislocation, a CT scan must be obtained to evaluate for any entrapped osteochondral fragments.
Traumatic hip dislocations are typically the result of high-energy trauma and are frequently associated with posterior wall acetabular fractures. Initial management of a traumatic hip dislocation, with or without a fracture, is immediate closed reduction under conscious sedation. If closed reduction is unsuccessful, immediate open reduction in the operating room should be performed. Following successful reduction, a CT scan is necessary to rule-out
intra-articular osteochondral fragments, even in the absence of fracture on radiographs. The incidence of sciatic nerve palsy following a traumatic hip dislocation is roughly 10%.
Pascarella et. al. review 127 traumatic hip dislocations with and without associated fractures. 5 were anterior dislocations, 13 were central dislocations, and 109 were posterior dislocations. In 45 of the cases, an intra-articular fracture fragment was found after successful closed reduction. They stress the importance of post-reduction CT scans given the large incidence of intraarticular fragments.
Bartlett et al. present a case study of a man who sustained cardiac arrest after attempted arthroscopic removal of a loose body in the hip following a traumatic hip fracture-dislocation. They believe that arthroscopic fluid extravasated through the fracture site under pump pressure and resulted in an intraabdominal compartment syndrome that presented as cardiopulmonary arrest. They do not support arthroscopic procedures of the hip following acute or healing acetabular fractures.
Figure A shows an AP pelvic radiograph with a R hip dislocation. Figure B shows the post-reduction radiograph with a concentrically reduced hip joint and no evidence of fracture.
Incorrect Answers:
Answer 1: Acute exploration of the sciatic nerve is controversial, and shouldn't be entertained before a CT scan has been completed.
Answer 2: EMG scan may be useful if the sciatic nerve fails to recover after a period of weeks to months.
Answer 4: CT scan must be obtained, even in the absence of a fracture on radiographs. In the absence of entrapped fragments, and if a concentric reduction is obtained, the next step would be TDWB and observation of the sciatic palsy.
Answer 5: Skeletal traction is not necessary if the hip is stable after concentric reduction and there are no associated fractures.
Which of the following injuries is anticipated to have a 20% chance of mortality and 50% chance of loss of independence at one year when sustained by an 85-year-old female?
1) Intra-articular distal humerus fracture
2) Distal radius fracture
3) Femoral neck fracture
4) Trimalleolar ankle fracture-dislocation
5) Periprosthetic distal femur fracture
A femoral neck fracture has been shown to have an estimated mortality rate of 20% or more at one year after injury, and estimates regarding loss of independence are at 50%.
Most literature on the topic points out the highest mortality rate is in the first 3-6 months, with mortality rates of 14-36% at one year; mortality rates have been found to return to normal, age-matched controls after that.
Egol et al. provide a review of the factors involved in functional recovery of patients with femoral neck fractures. They report the successes of integrated care pathways and review the risk factors (institutionalization, comorbidities, etc.) that go into the outcomes of these patients. They recommend comanagement of these patients with a medical or geriatric service in order to improve patient outcomes.
Incorrect Answers:
Answer 1,2,4,5: These can be debilitating injuries, but no evidence exists to show these injuries are associated with these levels of morbidity and mortality at one year.
A 17-year-old male falls from a retaining wall onto his left arm. He sustains the injury shown in Figure A. The patient undergoes open reduction and internal fixation of the fracture. Upon discharge from the hospital the medication reconciliation includes an order for daily Vitamin C 500mg supplementation. This medication is given in an effort to decrease the incidence of which of the following?
1) Upper extremity deep vein thrombosis (DVT)
2) Acute carpal tunnel syndrome (ACTS)
3) Complex regional pain syndrome (CRPS)
4) Lower extremity deep vein thrombosis (DVT)
5) Surgical site infection (SSI)
The patient has the clinical presentation of a distal radius fracture and Vitamin C administration has been associated with a lower incidence of complex regional pain syndrome (CRPS) in this group of patients.
Vitamin C administration is associated with a lower risk of complex regional pain syndrome (CRPS), formerly known as reflex sympathetic dystrophy (RSD), after wrist fractures. Vitamin C is thought to reduce lipid peroxidation, scavenge free hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability.
Zollinger et al. performed a prospective randomized trial that included 317 adult patients who sustained 328 distal radius fractures and were treated conservatively. They had allocated treatment groups to 200mg, 500mg, or 1500mg vitamin C dosages for 50 days. RSD/CRPS occurrence was lowest in the 1500mg group, however the 500mg dosage for 50 days was recommended at the conclusion of the study. The prevalence of CRPS was 2.4% in the vitamin C group and 10.1% in the placebo group. They found that all of the affected patients were elderly women.
Besse et al. performed a study of 392 patients that underwent foot surgery. They found that the group that received 1 gram daily of Vitamin C following foot surgery had a CRPS incidence of 1.7% compared to a control group that
did not receive Vitamin C and had a CRPS incidence of 9.6%. Figure A is a clinical photo of a distal radius fracture.
A 34-year-old female requests a second opinion following open reduction internal fixation (ORIF) of her left ankle three weeks ago. Which of the following is most appropriate step based on Figures A and B?
1) Progressive weightbearing in 3-4 weeks based on radiographs
2) Deltoid ligament repair vs reconstruction
3) Revision ORIF of fibula with lengthening
4) Revision ORIF of fibula and syndesmosis
5) Removal of syndesmotic screws in 3-6 months
The above clinical scenario shows acute postoperative fibular malrotation and tibiofibular syndesmotic malreduction. Restoration of the proper syndesmotic relationship involves regaining fibular length as well as reestablishing correct
rotation and position of the fibula relative to the tibia. In addition, removal of interposed tissue (deltoid ligament) in the medial joint space may be necessary. However, deltoid reconstruction is not routinely required.
Syndesmosis screw fixation in ankle fractures with syndesmotic disruption is indicated if there is residual or dynamic instability with stress testing of the tibiofibular joint after fixation of the fibula. Syndesmotic screws are commonly maintained in place for at least 12 weeks before removal, if necessary or desired. Controversy exists over use of 1 or 2 screws, screw size, and purchase of 3 or 4 cortices.
Gardner et al. compared radiographic measurements vs CT scans to assess reduction of the tibiofibular syndesmosis in ankle fractures. They found CT was better able to detect syndesmotic malreduction. Although they did not seek to correlate this with functional outcomes, they recommended heightened vigilance for assessing accurate syndesmosis reduction.
Zalavras et al. performed a review on ankle syndesmotic injuries. In their review, they highlight that syndesmotic injuries may occur in isolation or may be associated with ankle fractures. In the absence of fracture, physical examination findings suggestive of injury include ankle tenderness over the anterior aspect of the syndesmosis and a positive squeeze or external rotation test. They recommend stress testing for detecting syndesmotic instability with fixation of the syndesmosis when evidence of a diastasis is present.
Figures A and B show an ankle fracture treated with ORIF and syndesmotic repair, with syndesmotic and fibular malreduction.
Incorrect Answers:
Answer 1&5: Would not address the current syndesmotic malreduction which should be addressed.
Answer 2: Would not address the syndesmotic malreduction.
Answer 3: Fibular length appears appropriate on AP and lateral radiographs.
A 45-year-old patient sustains the injury shown in figure A. What radiographic finding most highly suggests a lateral meniscal injury?
1) Joint depression of 3mm
2) Ipsilateral femoral shaft fracture
3) Joint widening of 6mm
4) Ipsilateral tibial shaft fracture
5) Displaced tibial spine fracture
Figure A shows a Schatzker II tibial plateau fracture. Joint widening of 6mm is commonly asociated with a lateral meniscal injury.
Tibial plateau fractures are commonly associated with soft tissue injuries and the operative surgeon needs to be aware of these commonly associated injuries.
Gardner et al. (2005) examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Gardner et all. (2006) that looked at MRIs for 103 consecutive patients with all types of tibial plateau fractures, only one patient had no soft tissue injuries. 94 (91%) patients had a lateral meniscal injury, 79 (77%) patients had cruciate ligament injury and 70 (68%) patients had a posterior lateral corner injury.
Figure A: shows a Schatzker type II fracture of a tibial plateau.
Incorrect Answers:
Answer 1: The above mentioned articles only found associations with lateral meniscal injuries when joint depression was at least 6mm.
Answer 2: No known association with soft tissue injuries after tibial plateau fractures.
Answer 4: No known association with soft tissue injuries after tibial plateau fractures.
Answer 5: Suggestive of an ACL injury, not an injury to the lateral meniscus.
A 37-year-old male is struck by a car while walking at night. He is hemodynamically unstable at initial evaluation in the trauma bay. Advanced Trauma Life Support protocols are started, and an initial survey is completed. A chest radiograph and a pelvis AP radiograph (Figure A) are obtained. What is the most appropriate next step?
1) The patient should be taken directly to the OR for percutaneous placement of a pelvic external fixator
2) Dedicated inlet and outlet views of the pelvis to better classify the fracture
3) Continued resuscitation and immediate CT of the chest, abdomen and plevis
4) Emergent trip to interventional radiology for pelvic embolization
5) Immediate application of pelvic binder, continued resuscitation and re-evaluation of hemodynamic status
The patient has an Anterior-Posterior Compression type 3 pelvic ring injury (APC3), and this injury places the patient at risk of life- threatening hemorrhage. The most appropriate next step in the trauma bay is to place the patient in a pelvic binder in order to minimize pelvic volume and impart stability to the injured hemipelvis to allow for clot formation.
Pelvic fractures are high energy injuries with a high association of concomitant musculoskeletal trauma and damage to multiple organ systems. It is important that any patient with a high-energy pelvic ring injury undergo a complete
work-up including a CT of the chest abdomen and pelvis to look for alternative sources of bleeding. Application of a pelvic binder should occur once a pelvic ring injury is identified as part of the ongoing resuscitation of the patient.
Karadimas et al. retrospectively reviewed 34 patients at a single center who underwent pelvic arterial embolization as part of their resuscitation. APC injuries had the highest mean transfusion rate during the initial 24 hours, and the overall mortality for pelvic fractures requiring embolization was 23.5% in this series.
Manson et al. conducted a retrospective case-controlled study, evaluating mortality factors on LC-1 fractures. They found that in LC-1 fractures, the sacral fracture pattern does not predict mortality; however, mortality rate was increased in patients with a brain injury, chest injury, or abdominal injury.
Figure A demonstrates an APC3 pelvic ring injury with widening of both the symphysis and the right SI joint. Illustration A demonstrates the same injury as seen in Figure A after application of a pelvic binder with improved alignment of the pelvic ring. Illustration B shows appropriate application of a pelvic binder in a multiply injured patient.
Incorrect Answers:
Answer 1: While this patient may need to go emergently to the OR for multiple reasons, the work-up needs to be completed. However, the patient’s pelvis should be stabilized with a pelvic binder in the interim.
Answer 2: These images should be obtained, but the pelvis should be closed with a pelvic binder first.
Answer 3: While the pelvis may not be the only location of bleeding, the patient has a known source for bleeding, and it can be quickly stabilized with a pelvic binder. After the pelvic binder is placed, continued resuscitation and investigation of other possible locations of bleeding should occur.
Answer 4: While this patient may benefit from embolization, the first step is to close down the pelvis. Closing down the pelvis may prevent the need for embolization.
A 33-year-old man sustains blunt trauma to his forearm and presents with the injury seen in Fig A and B. Definitive management of this injury involves the following:
1) Perform closed reduction of the radius, then immobilize the forearm in a long arm cast in supination.
2) Perform open reduction and internal fixation of the radius, then assess the proximal radioulnar joint for instability, and percutaneously fix the proximal radioulnar joint if instability persists.
3) Perform open reduction and internal fixation of the radius, then assess the distal radioulnar joint for instability, and reconstruct the distal radioulnar joint with a looped palmaris longus autograft if instability persists.
4) Perform closed reduction of the radius, then assess the distal radioulnar joint for instability, and perform internal fixation of the radius if instability persists.
5) Perform open reduction and internal fixation of the radius, then assess the distal radioulnar joint for instability, and percutaneously fix the distal radioulnar joint if instability persists.
Galeazzi fracture-dislocations are fractures of necessity and must be managed surgically. The first step involves surgical fixation of the radial fracture. Next, the distal radioulnar joint (DRUJ) needs to be assessed for stability by looking for gross motion of the distal ulna in forearm supination. If DRUJ instability persists, this needs to be addressed with temporary percutaneous pin fixation with one or two 1.2- or 1.6mm K-wires placed transversely proximal to the sigmoid notch. This is followed by immobilization in above-elbow plaster casts
in forearm supination for 6 weeks postop. Anatomic reduction and rigid fixation of the radius alone does not guarantee DRUJ stability.
Rettig et al. found that the anatomical location of the radial shaft fracture could be used to predict DRUJ instability. Fractures within 7.5cm of the midarticular surface of the distal radius were more likely to require K wire stabilization (55%) compared with fractures more than 7.5cm away (6%).
Korompilias et al. found fractures of the distal third were more likely to require DRUJ stabilization (54%) than fractures of the middle third (12%) and proximal third (11%).
Giannoulis et al., in a review of Galeazzi fracture-dislocations, summarized the options as follows: (1) Stable DRUJ, cast in supination for 6 weeks; (2) Unstable DRUJ, TFCC repair and DRUJ pinning with a K wire in neutral rotation;
(3) Unstable DRUJ with ulnar styloid fracture, ORIF of ulnar styloid with tension band wire or lag screw; (4) Irreducible DRUJ because of tendon interposition (ECU, EDC or EDM), open reduction and TFCC repair.
Figures A and B are AP and lateral radiographs demonstrating a Galeazzi fracture-dislocation with marked disruption of the DRUJ. The radial head is visible in both radiographs and is not dislocated.
Incorrect Answers:
Answer 1: The radius fracture requires surgical fixation. While casting in supination may reapproximate DRUJ alignment, only pinning can prevent future subluxation.
Answer 2: Dislocation of the radial head and proximal radioulnar joint instability is characteristic of Monteggia fracture-dislocations. In this injury complex, the proximal ulnar shaft is fractured and not the radius. Galeazzi fracture-dislocations must not be confused with a Monteggia fracture-dislocation.
Answer 3: Tendon graft stabilization is an option for chronic DRUJ instability. Answer 4: The radial fracture must first be reduced and fixed with a plate.
Assessment of DRUJ stability is only possible after rigid fixation of the radial fracture has been performed.
Which of the following is true when comparing Figure A to Figure B?
1) Figure B is more likely to have an associated fracture
2) Figure A is more likely to be blocked from closed reduction by the extensor digitorum brevis
3) FIgure A is more likely to be open
4) FIgure B is more likely to be blocked from closed reduction by the posterior tibial tendon
5) Figure A more likely to be stable following closed reduction
While medial subtalar dislocations (Figure B) are more common, lateral subtalar dislocations (Figure A) are more likely to be open and have associated fractures.
Subtalar dislocations are devastating injuries with high rates of subtalar arthritis. Medial dislocations are more common and are occasionally blocked from closed reduction by the extensor digitorum brevis. Lateral dislocations are more likely to be open, have an associated fracture, and are occasionally blocked from closed reduction by the posterior tibial tendon, flexor digitorum longus, or flexor hallucis longus. Despite these differences, the injuries are treated similarly with closed reduction and immobilization followed by range-of-motion exercises.
DeLee et al. review 17 cases of subtalar dislocations. They found worse longterm results with lateral subtalar dislocations secondary to associated fractures and frequency of open injuries. They recommend cast immobilization for three weeks followed by early motion.
Heppenstall et al. review 20 cases of subtalar dislocations. They maintained reduction in a short-leg cast for 6 weeks following the injury and had 14 excellent results. The most common complications were restriction of motion and radiographic evidence of degenerative changes.
Goldner et al. review the long-term results of 15 patients who sustained a type III, open, subtalar dislocation. In contrast to closed injuries, they found that open subtalar dislocations are more likely to develop osteonecrosis of the talar body requiring pantalar arthrodesis.
Figure A shows a lateral subtalar dislocation. Figure B shows a medial subtalar dislocation.
Incorrect Answers:
Answer 1: Lateral subtalar dislocations are more likely to have associated fractures.
Answer 2: Lateral subtalar dislocations are most commonly blocked from closed reduction by the posterior tibial tendon.
Answer 4: Medial subtalar dislocations are more commonly blocked from closed reduction by the extensor digitorum brevis.
Answer 5: Medial subtalar dislocations are more likely to be stable, likely secondary to a decreased rate of associated fractures.
A 33-year-old motorcyclist is involved in a motor vehicle accident and sustains a Grade III open fracture of his tibia that is treated surgically. Over the next 35 years, he undergoes multiple debridements for a persistently draining wound. Over the last year, he has noticed "tissue growing out of the wound" and a malodorous smell. A photograph of the wound and a recent radiograph are seen in Figure A. A biopsy of the mass is shown in Figures B, and C. What is the most likely pathologic process?
1) Infection
2) Squamous cell carcinoma
3) Basal cell carcinoma
4) Melanoma
5) Soft-tissue sarcoma
A Marjolin's ulcer is a malignant tumor (Figure A) that develops around chronic osteomyelitis. The increasing size and foul smell suggest malignant change.
These tumors are most commonly squamous cell carcinoma (90%). Figures B and C confirm the diagnosis of squamous cell carcinoma.
Marjolin's ulcers can arise in the setting of burns, venous and decubitus ulcers, vaccination, snake bites and hidradenitis suppurativa. They usually involve the lower extremities. While squamous-cell carcinoma is most common, a small percentage of cases are basal-cell carcinoma, melanoma and sarcoma.
Copcu et al. examined 31 Marjolin's ulcers arising at burn sites. 58% were on the extremities, and had an average time lag of 19 years. Four of 31 cases had regional lymph node spread. They also drew attention to the fact that Marjolin's ulcers are more aggressive, with higher rates of metastasis, recurrence and fatality than other types of skin cancer.
Pandey et al. reviewed the literature on Marjolin's ulcers in chronic bone infections and found that the treatment of choice was still amputation (90% of cases). The challenges faced by the surgeon considering a more conservative approach include: wide resection of cancer for cure, resection of infected bone and soft tissue, preservation of limb function, and reconstruction.
Figure A shows the appearance of a fungating soft tissue tumor, together with a radiograph of chronic osteomyelitis. Figure B (low power) shows the
transition between normal epithelium (left) and squamous cell carcinoma (right), which is infiltrating downward. Figures C is a high power image of SCC. Illustration A shows basal cell carcinoma (Answer 3) with a cleft (red arrow) separating basaloid cells (green arrow) from the stroma. Illustration B shows melanoma with asymmetric proliferation of nests of melanocytes (red arrow), descending into the dermis (Answer 4).
Incorrect Answers:
Answer 1: While there is underlying chronic osteomyelitis, the more concerning disease process is malignant transformation into squamous cell carcinoma (Marjolin's ulcer)
Answer 3: There is no evidence of basal-cell carcinoma. Answer 4: There is no evidence of melanoma.
Answer 5: There is no evidence of sarcoma.
A 36-year-old male sustains an open segmental tibia fracture associated with an overlying 8 cm soft tissue avulsion that requires
skin grafting for soft tissue coverage. No vascular injury is identified. What is the most appropriate Gustilo-Anderson classification of this injury?
1) Type I
2) Type II
3) Type IIIA
4) Type IIIB
5) Type IIIC
An 8cm open segmental tibia fracture requiring skin grafting (but not a skin flap) qualifies as a Gustilo Type IIIA.
An open segmental tibia fracture meets criteria to be a type III injury, and subclassification as a IIIA is due to the lack of a need for free or regional tissue transfer for coverage. Classification as a type IIIB would require a free or regional soft tissue transfer (flap) for coverage. Also, remember that definitive classification is done intraoperatively, after full assessment of the fracture and wound are complete.
Gustilo et al. performed a retrospective review of 673 patients and a prospective review of 352 patients with open fractures. Infection rate of the type I and II in the retrospective series was 12%, and this decreased with use of a standardized modern treatment protocol to 2.5% in the prospective cohort. Type III deep infection rate was 44% in the retrospective study and 9% in the prospective study.
Incorrect Answers:
Answer 1: Involves a wound
A 25-year-old man sustains an open forearm fracture from an auger as depicted in Figures A and B. After debridement of nonviable bone, a 10cm bone defect is left. In planning future definitive treatment of the bone void, the use of an interposed strut allograft
instead of transfer of a vascularized fibula graft would most likely result in which of the following complications?
1) Higher incidence of infection
2) Lower nonunion rate
3) Decreased forearm arc of rotation
4) Complex regional pain syndrome
5) Synostosis
The patient has an open fracture with a large amount of bone loss. A higher incidence of infection would be expected with the interposed allograft strut graft treatment option.
Segmental bone loss in a limb secondary to trauma, tumor resection, or other disease require reconstruction to produce a functional limb. Bone loss of up under 5 centimeters is amenable to bone grafting. Larger defects will require vascularized grafts transfers or allografts. Other surgical options include
distraction osteogenesis and induced membrane technique. Vascularized fibular graft transfers have been shown to have good hypertrophy to support new biomechanical stresses and low rates of infection. Strut allografts have the advantage of unlimited size and no complications associated with donor site, however, complication rates including infection, fracture, and delayed union are higher than vascularized fibular grafts.
Wood et al. retrospectively assessed the outcomes of using vascularized fibula grafts for upper extremity reconstruction. The investigators reconstructed 21 limbs (clavicles, ulnas, radiuses, and humeruses) with defects greater than 6cm and measured rate of union. They experienced a primary healing rate of 71.4%. This rate went up to 81% after 2 patients underwent a secondary procedure revising the construct and adding iliac bone graft to the nonunion site. They concluded that the use vascularized fibular bone grafts are successful for reconstruction of limbs with large bony defects.
Falder et al. investigated the physiologic response to free vascularized fibula grafts. Thirty two graft outcomes were assessed for amount of hypertrophy of the fibular graft, bony union, and rate of limb salvage. They reported that 74% primary bony union occurred at a median of 4.75 months, median hypertrophy of the grafts was 71%, and 90% of patients regained the use of their affected limb within 12 months of the procedure. The authors concluded that vascularized free fibula flaps are an "excellent" option for limb salvage in patient with large bony defects and that these grafts respond well to biomechanical stresses.
Calkins et al conducted a Level 4 study looking at segmental bone defects of the upper extremity with open injuries. The investigators performed thorough debridement and irrigation to the extremities, applied iliac corticocancellous bone grafts with fixation, and secondary wound closure for all 22 patients.
They found a 60% rate of infection and 43% rate of union with use of corticocancellous strut grafts concluding that this technique translated well to the hand, but did not have satisfactory results in the arm and forearm for large defects.
Incorrect Answers:
Answer 2: There is a higher nonunion rate
Answer 3: Strut allograft has not been shown to have inferior forearm motion Answer 4: Strut allograft has not been shown to be associated with complex regional pain syndrome
Answer 5: Strut allograft has not been shown to have a higher rate of synostosis
A 46-year-old male falls 15 feet from a ladder while working. He presents with the radiographs shown in Figures A and B. The injury is closed, and soft tissues are intact upon arrival. Which of the following treatment regimens has been shown to decrease wound complications in the definitive management of these injuries?
1) Immediate definitive fixation of the tibia, and nonoperative treatment of the fibula
2) Immediate ankle-spanning external fixation device with consideration of immediate fixation of the fibula, followed by delayed reconstruction of the tibia
3) Placement of a temporary splint, elevation, and definitive fixation 1 week from injury
4) Immediate definitive fixation of the tibia and fibula
5) Immediate placement of a spanning Ilizarov fixator with limited internal fixation of the distal tibia and fibula
Studies have shown that a staged treatment protocol consisting of immediate fixation of the fibula with placement of an ankle-spanning external fixation device followed by delayed reconstruction of the tibia results in minimal surgical wound complications.
Historically, high rates of infection have been associated with open reduction and internal fixation of pilon fractures due to attempts at immediate fixation through swollen, compromised soft tissues. When a staged procedure is performed with initial restoration of fibula length and tibial external fixation, soft tissue stabilization is possible. Once soft tissue swelling has significantly diminished, anatomic reduction and internal fixation of the tibia can then be performed semi-electively with only minimal wound problems.
Sirkin et al performed a study to determine whether open reduction and internal fixation of intra-articular pilon fractures using a staged treatment protocol (defined in the above paragraph) resulted in improved surgical wound complications. In their cohort of 29 patients with closed pilon injuries treated in this manner, all wounds healed, and none exhibited wound dehiscence or full-thickness tissue necrosis requiring secondary soft tissue coverage postoperatively.
Patterson et al evaluated the use of a two-staged technique for the treatment of 21 consecutive patients with 22 C3 pilon fractures. All patients underwent immediate fibular fixation and placement of a medial spanning external fixator. After, on average, twenty-four days, patients underwent removal of the external fixator and formal open reduction and internal fixation of the pilon fractures. There were no infections or soft tissue complications.
Figure A and Figure B demonstrate orthogonal views of a high-energy intraarticular distal tibia fracture.
Incorrect Answers:
1,3,5: These treatment regimens have not been shown in the trauma literature to be associated with decreased wound complications in the fixation of complex pilon fractures.
A 42-year-old man sustains the injury shown in Figure A after a fall from 6 feet. Physical exam after the injury reveals a flaccid ipsilateral limb. An MRI is performed that reveals nerve root avulsions from C5-T1. Which of the following is the most appropriate management of his fracture at this time?
1) Closed management with a coaptation splint
2) Closed management with a coaptation splint followed by transition to a functional brace after 7-10 days
3) External fixation of humeral shaft fracture until brachial plexus injury resolves
4) Open reduction, surgical fixation with plating
5) Closed management with a sling until brachial plexus injury resolves
A coexisting brachial plexus injury is an absolute indication for open reduction and internal fixation of humeral shaft fractures.
A majority of humeral shaft fractures may be treated non-operatively in a
functional brace. Absolute indications of operative management include open fracture with severe soft tissue injury, vascular injury requiring repair, and a coexisting brachial plexus injury. Patients with a brachial plexus injury are more likely to go on to nonunion when treated non-operatively due to lack of muscular support controlling the fracture fragments.
Sarmiento et al. review 620 patients with humeral shaft fracture treated nonoperatively in a coaptation splint followed by a functional brace. Only 16 patients developed a non-union, and any residual deformity was usually functionally and aesthetically acceptable.
Rutgers et al. present a retrospective case series of 49 patients who had humeral shaft fractures that were treated non-operatively in a functional brace. 44 of 49 patients went on to successful union. Fractures of the proximal third of the humeral shaft were most likely to go on to nonunion.
Figure A shows a midshaft humerus fracture. Incorrect Answers:
Answer 1, 2, 5: operative management is indicated with a coexisting brachial
plexus injury.
Answer 3: a coexisting brachial plexus injury is not an indication for external fixation of humeral shaft fractures.
A 65-year-old diabetic male with forefoot gangrene is evaluated for possible amputation. When discussing the amputation levels with the patient, which of the following should be noted to require the greatest increase in energy expenditure for ambulation?
1) Syme amputation
2) Unilateral transtibial amputation
3) Transfemoral amputation
4) Bilateral transtibial amputations
5) Through the knee amputation
A transfemoral level amputation requires the greatest increase in energy expenditure of the amputation levels given, and a Syme amputation the least.
Biologic joints are energy couples. When performing amputation surgery, more
proximal amputations, accompanied by the removal of more joints, decreases the ability of patients to walk and live independently. Therefore a Syme amputation would require only a small increase in energy needed for ambulation. Bilateral transtibial amputee patients have an energy expenditure that is 40% above baseline levels. According to Miller's Review text, unilateral transfemoral amputee's require a 65% increase in energy expenditure.
Pinzur et al. retrospectively studied 97 adult patients with diabetes mellitus who underwent Syme ankle disarticulation because of a neuropathic foot with an infection or gangrene, or both, during an 11 year period. They found that overall 84.5% of the patients achieved wound healing. Their data support the value of Syme ankle disarticulation in diabetic patients with infection or gangrene.
Laughlin et al. retrospectively reviewed the surgical results and functional outcome of 52 patients treated with Syme amputations for forefoot gangrene. Wound healing was correlated with the preoperative status of the posterior tibial artery and follow-up averaged 27 months. The authors found that that posterior tibial artery Doppler examination is predictive of healing in the Syme amputation performed on diabetics, and that furthermore, diabetics can attain a functional level of ambulation with a Syme amputation.
Illustration A shows a clinical photo of a standard Syme amputation with a healthy heel pad which can allow for limited weight bearing in the absence of a prosthesis.
Incorrect Answers:
1,2,4,5: All of these amputation levels have lower energy expenditure increases than a transfemoral amputation.
A 76-year-old female with underlying osteoporosis presents with severe right leg pain after stepping off a curb. Current femur
radiographs are shown in Figure A. Review of the patient's medical records reveal that she had been evaluated 3 months prior for right hip pain, and work-up at that time was negative. Radiographs of the patient's femur from that previous visit are shown in Figure B. What is the most likely cause of this patient's femur fracture?
1) Fibrous cortical defect
2) Metastatic lesion
3) Acute trauma
4) Bisphosphonate treatment
5) Osteomyelitis
The patient's injury is most consistent with a bisphosphonate induced atypical femur fracture.
Atypical subtrochanteric femoral fractures have been identified as a potential complication of long-term bisphosphonate therapy for the treatment of osteoporosis. Prodromal symptoms of thigh pain are common prior to fracture, and bony failure is usually associated with low energy mechanisms.
Puhaindran et al. performed a retrospective review of the imaging studies and case notes for patients with skeletal malignant involvement who received a minimum of twenty-four doses of intravenous bisphosphonates. Patients were classified as having an atypical subtrochanteric femoral fracture if they had a transverse subtrochanteric fracture following low-energy trauma or an impending fracture, together with radiographic findings. In the study cohort of 327 patients, four patients developed an atypical subtrochanteric femoral fracture. All four patients were female, three had breast cancer, and one had myeloma.
Feldman et al. reviewed the imaging presentations on routine radiographs, alternate imaging modalities, and associated pitfalls in nine atypical femur fractures in six patients. The author states that effects may differ with each bisphosphonate's route of administration and prolongation of activity, despite discontinuation. The review also discusses the theoretical mechanisms of bisphosphonates as a class rather than with a specific alendronate association and provides a broader basis for evaluating the recently observed clinical and radiographic complications.
Figure A shows a transverse subtrochanteric femur fracture. Figure B shows diaphyseal cortical thickening and cortical beaking at the subtrochanteric area.
Incorrect Answers:
Answer 1: The radiographic findings are not consistent with a fibrous cortical defect.
Answer 2: The radiographic findings are not consistent with the presence of a metastatic lesion.
Answer 3: Subtrochanteric fractures are typically associated with high energy
trauma, and this patients mechanism of injury is atypical.
Answer 5: There is no radiographic or clinical evidence supporting the presence of chronic osteomyelits.
Risk factors for intimate partner violence after musculoskeletal injury includes all of the following EXCEPT?
1) Shorter length of relationship
2) Younger age
3) Current pregnancy
4) Alcohol dependency
5) History of prior divorce
History of marriage ending in divorce has not been identified in the literature as a risk factor for intimate partner violence (emotional, physical, and sexual abuse).
The approximate prevalence of intimate partner violence (emotional, physical, and sexual abuse) is 32% among females within the 1 year before they are seen by an orthopaedist for the treatment of musculoskeletal injuries.
Bhandari et al. performed a level 2 cohort study of 282 females presenting to their institution for orthopaedic injuries. The prevalence of intimate partner violence (emotional, physical, and sexual abuse) within the twelve months prior to presentation was 32%.
Bhandari et al. also performed a level 4 review of 263 females referred to the Minnesota Domestic Abuse Program. Identified risk factors for physical abuse included younger age, shorter length of relationship, emotional abuse, psychological abuse, sexual abuse, drug dependency, and alcohol dependency.
Illustration A shows a table that outlines the roles and responsibilities of orthopaedic surgeons according to the Canadian Orthopaedic Association 2012 position statement.
Incorrect Answers:
Shorter length of relationship, younger age, current pregnancy, and alcohol dependency have all been indentified as risk factors for intimate partner violence.
A 30-year-old woman falls onto an outstretched arm while rollerblading. She presents to the emergency room with the elbow deformity shown in Figure A. On physical examination she is unable to range her elbow. She is distally neurovascularly intact. Her radiograph is shown in Figure B. What is the next step in management of this patient?
1) Closed reduction, hinged external fixator
2) Closed reduction, acute surgical repair of the lateral collateral ligament complex
3) Open reduction and surgical repair of the lateral collateral ligament complex
4) Closed reduction, splinting & early passive ROM
5) Closed reduction, splinting & early active ROM
The clinical presentation is consistent with a simple elbow dislocation. Initial management should include closed reduction, splinting or sling placement for comfort and early active ROM exercises.
Simple elbow dislocations should be reduced and treatment guided by the relative stability of the joint during the arc of motion. The elbow should be splinted where it is most stable. After 5-7 days the splint can be discontinued and active ROM started to apply compressive stability to the joint. A hinged brace with an appropriate extension block can facilitate motion through the stable arc.
Armstrong discusses pathomechanics and basis for treatment in simple elbow dislocations. She emphasizes delineating the arc through which the elbow is stable and using this to guide initial management. Early surgical management may be warranted when the elbow is unstable with 60 degrees or more of flexion.
Josefsson et al. studied 30 patients who had sustained simple elbow dislocations and prospectively randomized the patients into non-operative and operative study arms. Operative intervention included reattachment of avulsed ligaments/muscles from the distal humerus. They found no statistical difference in clinical outcomes between the groups regardless of the severity of the instability.
Figure A demonstrates a clinical photo of a patient having sustained an elbow dislocation. Figure B is a radiograph demonstrating a posterolateral elbow dislocation, which is named based on the direction that the ulna/radius move relative to the humerus. Illustration A is a video that reviews the pathomechanics of elbow dislocations.
Incorrect Answers
Answer 1, 2: While use of a hinged external fixator may be appropriate when instability persists after repair/reconstruction of the LCL complex, it is not the first step in the initial management of a simple elbow dislocation.
Answer 3: Open reduction may be warranted if closed reduction is unsuccessful, however an initial attempt at conservative measures should be made.
Answer 4: Closed reduction needs to be followed by splinting to give the tissues a chance to recover from the initial injury; use of ACTIVE range of motion exercises early, will help to provide dynamic compressive stability to the joint.
A 21-year-old male undergoes intramedullary nailing of the closed tibial shaft fracture shown in Figure A. At his 6-week follow-up,
he is noted to have peroneal nerve deficits that were not present preoperatively. Which of the following findings is most consistent with a diagnosis of transient peroneal nerve neurapraxia as the result of his intramedullary nailing?
1) Decreased lateral hindfoot sensation
2) Decreased Achilles reflex
3) Decreased peroneus longus strength
4) Decreased extensor hallucis longus strength
5) Decreased plantar forefoot sensation
Decreased extensor hallucis longus strength is the physical exam finding most consistent with transient peroneal nerve neurapraxia.
Transient peroneal nerve neuropraxia has been noted in up to 5% of patients undergoing closed nailing of tibial shaft fractures. This is of unknown etiology, although injury to the peroneal nerve branches can be from placement of the interlocking screws into the nail. In this syndrome, extensor hallucis longus weakness is noted and decreased sensation is seen in the 1st dorsal webspace (deep peroneal nerve distribution). These symptoms generally begin improving by 3 months and have variable rates of recovery.
Robinson et al. reported on 'dropped hallux' syndrome, with weakness of extensor hallucis longus and numbness in the first web space, without clinical involvement of extensor digitorum longus or tibialis anterior. They found this in 5% of their patients after tibial nailing of closed tibia fractures, and all recovered either partially or completely by 4 months.
Lawrence et al. performed an anatomic study that reported the deep peroneal nerve was located superficial to the anterior tibial artery between the tibialis anterior and extensor hallucis longus muscles in the distal one third of the leg. They also found that the deep peroneal nerve crossed deep to the extensor hallucis longus tendon to enter the interval between the extensor hallucis longus and extensor digitorum longus at an average distance of 12.5 mm proximal to the ankle.
Figure A shows a tibial shaft fracture with mild displacement. Incorrect Answers:
Answer 1: Lateral hindfoot sensation is generally via the sural nerve.
Answer 2: Achilles reflex is via S1 roots.
Answer 3: The peroneus longus is innervated by the superficial peroneal nerve. Answer 5: Plantar forefoot sensation is via the tibial nerve along with the medial and lateral plantar branches.
A 24-year-old male presents after being shot in the lower back. Radiographs and advanced imaging show that the bullet traversed the paraspinal musculature, entered the pelvis below the pelvic brim, did not cross the midline, and is currently lodged in the ilium. No intraarticular involvement was noted, and the bony injury is stable. No occult blood is noted on the rectal examination. The police report indicates that the bullet was fired from a low-velocity weapon. Which of the following is the most important treatment for this patient assuming he is hemodynamically stable?
1) Immediate exploratory laparotomy and bullet removal
2) Bullet removal followed by surgical stabilization of the ilium
3) Immediate surgical debridement of the bullet tract and delayed closure of the soft tissue wound
4) Empiric antibiotic therapy and observation
5) Sigmoidoscopy
Based on the clinical presentation, this patient should be treated initially with empiric antibiotic therapy and observation.
The available literature shows that transabdominal GSW with intra-articular contamination should be urgently débrided and irrigated; extra-articular transabdominal GSW with stable fracture patterns may be managed with observation and empiric antibiotics. Bullets lodged in intra-articular locations should be removed, but retained bullets in other anatomic locations do not necessarily warrant removal.
Watters et al. retrospectively collected Information regarding surgical débridement of pelvis low velocity gunshot wounds, retained foreign bodies, and/or concomitant gastrointestinal (GI) injury was analyzed for relationships of such events to infection rate in 56 patients. The authors found that there was no increased incidence of infection in the absence of aggressive surgical débridement of pelvis gunshot wounds. The study also demonstrated that retained bullets and bullet fragments did not increase the risk of infection, even after penetrating the GI tract organs.
Zura et al. completed a review article on the treatment of gunshot wounds to the hip and pelvis. The authors state that antibiotic treatment usually is indicated for patients with gunshot wounds to the pelvis, but is controversial in patients with low-energy wounds. Furthermore they state that fractures are treated based on their stability and wound care should be determined by the personality of the injury, and not solely based on the velocity of the missile.
Miller et al. completed a recent review article on transabdominal gunshot wounds to the hip and pelvis. They state that extra-articular transabdominal GSW with stable fracture patterns may be managed with observation and empiric antibiotics.
Incorrect Answers:
Answer 1: Immediate exploratory laparotomy would be indicated in the setting of persistent hemodynamic instability or positive peritoneal signs.
Answer 2: There is no evidence that bullet removal is necessary when it is in an extra-articular location. Furthermore the bony injury is stable, and does not warrant fixation.
Answer 3: Immediate surgical debridement is not necessary without intraarticular involvement or severe soft tissue injury.
Answer 5: Sigmoidoscopy would be necessary if occult blood was noted on rectal examination or if the bullet crossed the midline below the pelvic brim.
She lives in an assisted living facility, and reports no other major medical problems. The best functional outcome can be expected with which of the following definitive treatment options?
1) Open reduction internal fixation of the distal humerus fracture
2) Nonsurgical management with early passive range of motion exercises
3) Initial nonsurgical management followed by interpositional arthroplasty when the fracture has healed
4) Total elbow arthroplasty
5) Excision of the capitellar fragments and fixation of the trochlear fragments
This elderly, low demand patient is presenting with a distal and comminuted distal humerus fracture in the setting of poor bone quality. These are extremely difficult to reconstruct and rehabilitate from, and therefore in this particular case total elbow arthroplasty is the best option.
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humerus fractures in patients older than age 70. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight more than 10-15 pounds must be followed to avoid loosening.
Kamineni et al. retrospectively reviewed 49 acute distal humerus fractures in 48 patients who were treated with total elbow arthroplasty as the primary option. Forty-three of these fractures were followed for 2 years. At the latest follow-up examination, the average flexion arc was 24 degrees to 131 degrees
and the Mayo elbow performance score averaged 93 of a possible 100 points. This review supports a recommendation for total elbow arthroplasty for the treatment of an acute distal humerus fracture when strict inclusion criteria are observed.
Frankle et al. compared open reduction and internal fixation (ORIF) with total elbow arthroplasty (TEA) for intraarticular distal humerus fractures in women older than 65 years of age. Follow-up was a minimum of two years. Using the Mayo Elbow Performance score, the outcomes of the 12 patients treated with ORIF were as follows: 4 excellent, 4 good, 1 fair, and 3 poor. Outcomes of the 12 patients treated with TEA were as follows: 11 excellent and 1 good. There were no fair or poor outcomes in the TEA group, and no patients treated with TEA required revision surgery.
The AP and lateral elbow radiographs shown in Figures A demonstrate a severely comminuted and displaced distal humerus fracture.
Incorrect Answers:
Answer 1: Stable ORIF is nearly impossible to attain in the setting of a very distal fracture of the humerus with comminution and poor bone quality.
Answer 2: Although nonsurgical management of these injuries showed some favor in the past, range of motion and pain control are ultimately better with TEA in the appropriate patient.
Answer 3: Interpositional arthroplasty is indicated in younger patients who may not be able to comply with the strict weight lifting restrictions of a TEA. Answer 5: Fixation of the trochlear fragments would be extremely difficult in this case, and capitellar excision would likely lead to an unstable elbow joint in the setting of a compromised ulnohumeral articulation.
A 52-year-old carpenter falls off of a balcony while at work and sustains the injury shown in Figure A. The patient's BMI is 52 and he smokes 2 packs of cigarettes per day; a clinical photograph of the limb is shown in Figure B. What is the most appropriate next step in management?
1) Short leg splint placement and transition to short leg cast at 2 weeks
2) Closed reduction and spanning external fixation of the ankle
3) Open reduction and internal fixation of the fibula and tibia
4) Open reduction and internal fixation of the fibula with Blair arthrodesis of the ankle
5) Open reduction and internal fixation of the tibia and articulating external fixation of the ankle
Closed reduction with spanning external fixation of the ankle is the most appropriate next step in management with planned definitive tibia ORIF when soft tissue swelling allows. Fixation of the fibula at the time of external fixation has been well-described but is a controversial subject.
Pilon fracture treatment with a staged procedure is performed with initial restoration of length and tibial external fixation. Once soft tissue swelling has significantly diminished, anatomic reduction and internal fixation of the tibia can then be performed semi-electively with only minimal wound problems.
Sirkin et al performed a Level 4 retrospective review of open reduction and internal fixation of intra-articular pilon fractures using a staged treatment protocol. The protocol consisted of ORIF of the fibula and application of an external fixator spanning the ankle joint within twenty-four hours. Patients then underwent formal open reconstruction of the articular surface by plating when soft tissue swelling had subsided at around the 2 week mark. This protocol resulted in improved surgical wound complications. In their cohort of 29 patients with closed pilon injuries treated in this manner, all wounds healed, and none exhibited wound dehiscence or full-thickness tissue necrosis requiring
secondary soft tissue coverage postoperatively.
Illustration A shows an external fixator used for initial stabilization of a pilon fracture.
Incorrect Answers:
Answer 1: Nonoperative management is not indicated in displaced pilon fractures.
Answer 3 & 5: Immediate ORIF of the tibia plafond fracture has a higher incidence of wound complications.
Answer 4: Blair fusion of the ankle is not indicated in pilon fractures
A 23-year-old male right hand dominant minor league hockey player sustains the injury shown in Figure A and B. The patient is apprised of the risks and benefits of both conservative and surgical treatments. He chooses to undergo surgical intervention and wishes to minimize the chance of requiring a second operation. Which of the following is the most appropriate surgical procedure for this patient?
1) Distal clavicle resection
2) Transacromial wire fixation with possible coracoclavicular ligament reconstruction
3) Coracoclavicular screw fixation
4) Hook plate fixation with coracoclavicular ligament reconstruction
5) Small fragment plate fixation with possible coracoclavicular ligament reconstruction
Small fragment plate fixation with possible coracoclavicular ligament reconstruction is the most appropriate treatment for a displaced distal clavicle fracture in a patient that wishes to avoid a second procedure.
The Neer classification describes lateral third distal clavicle fractures. Type II fractures (where the proximal fragment is detached from the CC ligaments and the distal fragment remains attached to the scapula via the AC joint capsule) and Type V (where a inferior clavicular fragment remains attached to the CC ligaments) are often displaced and are believed to have a higher rate of nonunion. Treatment of distal third as well as midshaft clavicle nonunions is best treated with open reduction and internal fixation of the nonunion.
Banerjee et al performed a Level 5 review of the management of distal clavicle fractures. They recommend primary nonsurgical management of type I, type III, and nondisplaced type II distal clavicle fractures. For patients with displacement, the authors offer surgical treatment but counsel them that the current evidence suggests equivalent outcomes between surgical and nonsurgical treatment.
Oh et al. performed a Level 4 systematic review of 425 cases from 21 studies. With surgical treatment, the nonunion rate was not significantly different among the modalities (p = 0.391). The complication rate was significantly higher in cases of the hook plate (40.7%) and the K-wire plus tension band wiring (20.0%) than those of the coracoclavicular stabilization (4.8%), the intramedullary (2.4%) and the interfragmentary fixation (6.3%).
Jin et al present a Level 4 review of 17 patients that underwent CC screw fixation of their distal clavicle fracture. They routinely removed the CC screw at 8 weeks as a second procedure and noted that all but one patient had a good outcome based on the UCLA score.
Figures A and B demonstrate displaced Type V distal clavicle fractures. Illustration A and B demonstrate an example of the use of a hook plate for distal clavicle fixation. Illustration C shows an example of a CC screw fixation and Illustration D demonstrates a distal clavicle plate fixation. Illustration E depicts the Neer classification for distal clavicle fractures. Illustration F displays a distal clavicle fracture ORIF with small fragment locking plate.
Incorrect Answers:
Answer 1: Isolated distal clavicle excision may lead to instability if the fragments are attached to the CC ligaments.
Answer 2: Transacromial wire fixation has a high rate of secondary procedure for wire removal and concern for hardware breakage and migration.
Answer 3: Coracoclavicular screw fixation routinely requires a secondary procedure for removal of the screw.
Answer 4: Hook plate fixation has a high rate of secondary procedure for plate removal to prevent acromial osteolysis.
A 32-year-old male sustains the injury shown in Figures A through D as the result of a high-speed motorcycle collision. He initially undergoes spanning external fixation and returns to the office for soft tissue evaluation prior to his definitive surgery. During this visit, you discuss that the most appropriate fixation is which of the following?
1) Lateral precontoured locked plating
2) Posterior buttress plating
3) Medial antiglide plating
4) Anterolateral and posteromedial plating
5) Posterolateral neutralization plating
Posterior tibial plateau fractures are typically sustained from an axial load with the knee in flexion, leading to a large posterior shearing force on the tibial plateau from the condyles. This most commonly leads to a posterior fracture fragment, with variable involvement of the posteromedial or posterolateral joint line. The shearing nature of this fracture leads to an unstable fracture pattern.
Bhattacharyya et al reviewed 13 patients who underwent fixation of posterior tibial plateau fractures and noted a consistent fracture pattern with a primary, inferiorly displaced posteromedial shear fracture. They reported excellent clinical outcomes at a mean of 20 months, with the quality of articular reduction being one factor that correlated with functional outcome scores.
Fakler et al. was the first English-language study to publish the surgical outcomes of posterior tibial plateau fractures using the Lobenhoffer approach. In their two case study, the authors suggest that the Lobenhoffer approach is less morbid to the soft-tissues in comparison to other commonly described posterior approaches.
Figures A, B, C, and D show a tibial plateau fracture with posterior shear involvement. Illustrations A and B are postoperative images showing the same fracture pattern after posterior buttress plating.
Incorrect Answers:
Answer 1: This fracture fragment is not adequately captured with a lateral based plate; the lateral cortex is also intact, which limits the indications for this plate.
Answer 3: The primary fracture fragment is posterior and not medial. Answer 4: No fracture is seen laterally; posteromedial plating can be utilized, however.
Answer 5: No fracture fragment is seen posterolaterally.
A 40-year-old female sustains the injury seen in Figure A. What other associated soft-tissue knee injury is most commonly associated with this fracture?
1) Anterior cruciate ligament midsubstance tear
2) Horizontal cleavage lateral meniscus tear
3) Peripheral lateral meniscus tear
4) Lateral collateral ligament and popliteofibular ligament tear
5) Lateral meniscus posterior root avulsion
Figure A shows a displaced Schatzker II (lateral split-depression) tibial plateau fracture. These injuries are commonly associated with peripheral meniscal tears.
According to the referenced article by Abdel-Hamid et al, the overall incidence of associated soft tissue injuries of the knee in tibial plateau fractures is 71%. The incidence of each injury in their study was: meniscal tears (57% - usually peripheral tears), ACL (25% - more common in more severe fractures), PCL (5%), LCL (3%), MCL (3%), peroneal nerve (1%). No vascular injury was seen in their collection of 98 patients.
The posterior wall of the acetabulum is best visualized on which of the following radiographic views?
1) Inlet pelvis
2) Outlet pelvis
3) Anteroposterior pelvis
4) Obturator oblique pelvis
5) Iliac oblique pelvis
The posterior wall is best visualized on the obturator oblique pelvic view.
The obturator oblique and iliac oblique views make up the Judet views that are used to evaluate acetabular fractures, along with a standard AP pelvis radiograph. The obturator oblique pelvic view is best to view the anterior column and posterior wall in detail. The iliac oblique shows the profile of involved iliac wing, the posterior column, and the anterior wall.
Letournel reviewed his classification and treatment protocols, based on his 22 years of experience at that time. He noted that perfect anatomical reduction of the acetabulum led to the best outcomes.
Patel et al reviewed of the Letournel classification, and they found moderate to high inter- and intra-observer reliability with this classification system. The presence of articular displacement, marginal impaction, incongruity, intraarticular fragments and osteochondral injuries to the femoral head were found to have less reliability (intra- and interobserver).
Illustration A shows a right-sided obturator oblique radiograph, while Illustration B shows a right-sided iliac oblique radiograph. Illustration C shows a diagram of the obturator oblique radiograph, with the radiographic lines marked out.
Incorrect Answers:
Answers 1: Inlet pelvic imaging is best for assessing pelvic ring injuries (rotation and anterior-posterior or medial-lateral translation).
Answers 2: Outlet pelvic imaging is best for assessing pelvic ring injuries (proximal-distal translation, rotation).
Answers 3: AP pelvis is a good screening tool for pelvic and acetabular fractures.
Answers 5: Iliac oblique pelvis is best for assessing the posterior column and anterior wall of the acetabulum.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon