Orthopedic With Answers Review | Dr Hutaif General Orth -...
14 Apr 2026
86 min read
73 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answers Review | Dr Hutaif Ge...
00:00
Start Quiz
Question 1High Yield
A 12-year-old boy at 5’5”, 180 pounds comes to the outpatient clinic with 2 months of left anterior knee pain without discrete injury. He has a slight antalgic gait on the left, has full knee range of motion, stable ligaments, and mild tenderness at his tibial tubercle. He has restricted hip internal rotation and worsening knee pain with hip motion. Knee radiographs are negative. What is the best next step in treatment?
Explanation
■
Knee pain in an overweight adolescent patient is a classic presentation for stable slipped capital femoral epiphysis (SCFE). Recognizing the exacerbation of knee pain with hip motion makes radiographic evaluation of the hip the appropriate next step in evaluation. Delaying the diagnosis with treatment focused on the knee such as the other answer options suggest, risks progression of the SCFE and potential long-term consequences.
Knee pain in an overweight adolescent patient is a classic presentation for stable slipped capital femoral epiphysis (SCFE). Recognizing the exacerbation of knee pain with hip motion makes radiographic evaluation of the hip the appropriate next step in evaluation. Delaying the diagnosis with treatment focused on the knee such as the other answer options suggest, risks progression of the SCFE and potential long-term consequences.
Question 2High Yield
Figures 46a and 46b are the radiographs of a 60-year-old man with gradual onset of right shoulder pain and motion loss 1 year after undergoing an uncomplicated right total shoulder arthroplasty
(TSA) for end-stage osteoarthritis. He denies trauma to his right shoulder and constitutional symptoms, but admits to difficulty performing activities of daily living. His surgical wound site is benign. He demonstrates active and passive forward flexion to 90 degrees, abduction to 60 degrees, external rotation to 30 degrees, and internal rotation to the lumbosacral junction. His rotator cuff strength is graded as normal and symmetrical to his unaffected left shoulder. Based upon the current evaluation, what is the most appropriate next step?
(TSA) for end-stage osteoarthritis. He denies trauma to his right shoulder and constitutional symptoms, but admits to difficulty performing activities of daily living. His surgical wound site is benign. He demonstrates active and passive forward flexion to 90 degrees, abduction to 60 degrees, external rotation to 30 degrees, and internal rotation to the lumbosacral junction. His rotator cuff strength is graded as normal and symmetrical to his unaffected left shoulder. Based upon the current evaluation, what is the most appropriate next step?


Explanation
This patient’s radiographs do not reveal prosthetic loosening, osteolysis, instability, or rotator cuff deficiency. History and examination findings suggest a possible indolent infectious process, and it is incumbent upon the treating surgeon to obtain screening laboratory studies (complete blood count with differential, erythrocyte sedimentation rate, and C-reactive protein) and proceed with obtaining cultures (via joint aspiration or arthroscopic soft-tissue biopsy) to rule out an infectious process. Cultures should be held for 2 weeks to evaluate for the possibility of a Propionibacterium acnes infection, which is the predominant organism elicited from painful and stiff TSAs for which revision is required. Immediate revision TSA is not indicated in this scenario because the components appear well fixed and positioned. Observation and therapy in the setting of deterioration of a previously well-functioning TSA also are not appropriate.
RECOMMENDED READINGS
66. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861. ](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
67. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
68. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
CLINICAL SITUATION FOR QUESTIONS 47 AND 48
A 42-year-old mechanic has right medial elbow pain that is worse with use at work. He denies any injury to the arm. He has no significant medical history, but he smokes a pack of cigarettes each day. He has filed a Workers’ Compensation claim and has hired an attorney. He is still working his full job duty, but he expresses dissatisfaction with his employer. An examination reveals tenderness to palpation maximally anterior to the medial epicondyle. Pain is worse with resisted wrist flexion and resisted forearm pronation.
RECOMMENDED READINGS
66. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861. ](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
67. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
68. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
CLINICAL SITUATION FOR QUESTIONS 47 AND 48
A 42-year-old mechanic has right medial elbow pain that is worse with use at work. He denies any injury to the arm. He has no significant medical history, but he smokes a pack of cigarettes each day. He has filed a Workers’ Compensation claim and has hired an attorney. He is still working his full job duty, but he expresses dissatisfaction with his employer. An examination reveals tenderness to palpation maximally anterior to the medial epicondyle. Pain is worse with resisted wrist flexion and resisted forearm pronation.
Question 3High Yield
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
The patient has a supple plantigrade foot that would benefit from a drop foot brace to prevent catching of the toes. Tendon transfer should not be considered until the patient has undergone bracing. Achilles tendon lengthening is not necessary because the foot is plantigrade and flexible. Nerve grafting is not indicated because of the length of time the peroneal nerve palsy has been present.
REFERENCES: Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int
1996;17:425-439.
REFERENCES: Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int
1996;17:425-439.
Question 4High Yield
The video in Figure 44 demonstrates a unilateral “piano key” sign, which indicates

Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments.
This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ.
Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
RECOMMENDED READINGS
39. [Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Orthop Clin North Am. 2007 Apr;38(2):289-97, vii. Review. PubMed PMID: 17560410.](http://www.ncbi.nlm.nih.gov/pubmed/17560410)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17560410)
40. [Moritomo H. The distal interosseous membrane: current concepts in wrist anatomy and biomechanics. J Hand Surg Am. 2012 Jul;37(7):1501-7. doi: 10.1016/j.jhsa.2012.04.037. Review. PubMed PMID: 22721462. ](http://www.ncbi.nlm.nih.gov/pubmed/22721462)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22721462)
This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ.
Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
RECOMMENDED READINGS
39. [Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Orthop Clin North Am. 2007 Apr;38(2):289-97, vii. Review. PubMed PMID: 17560410.](http://www.ncbi.nlm.nih.gov/pubmed/17560410)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17560410)
40. [Moritomo H. The distal interosseous membrane: current concepts in wrist anatomy and biomechanics. J Hand Surg Am. 2012 Jul;37(7):1501-7. doi: 10.1016/j.jhsa.2012.04.037. Review. PubMed PMID: 22721462. ](http://www.ncbi.nlm.nih.gov/pubmed/22721462)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22721462)
Question 5High Yield
A 20-year-old college student sustains a closed distal one-third tibia fracture when he falls while skiing. Which of the following would be the most common fracture pattern and mechanism:
Explanation
This college student has sustained a low-energy twisting injury, also known as a boot-top injury. The fracture pattern is a short spiral fracture and the mechanism of injury is torsion loading of the tibia.
The other patterns included:
Oblique fracture â uneven bending: This type of injury typically occurs following motorcycle accidents when the tibia is subjected to uneven bending forces.
Transverse fracture â pure bending: This fracture is typical of a soccer injury because the tibia is subjected to pure bending forces.
Oblique fracture with a butterfly fragment â bending and compression: This is a common fracture that occurs with low- and high-speed injuries. These fractures may occur from car bumpers and motorcycles.
Segmental fracture â four-point bending: This pattern is typical of high-energy injury, such as a pedestrian being struck by a car bumper.
The other patterns included:
Oblique fracture â uneven bending: This type of injury typically occurs following motorcycle accidents when the tibia is subjected to uneven bending forces.
Transverse fracture â pure bending: This fracture is typical of a soccer injury because the tibia is subjected to pure bending forces.
Oblique fracture with a butterfly fragment â bending and compression: This is a common fracture that occurs with low- and high-speed injuries. These fractures may occur from car bumpers and motorcycles.
Segmental fracture â four-point bending: This pattern is typical of high-energy injury, such as a pedestrian being struck by a car bumper.
Question 6High Yield
All of these findings are features of patients with Scheuermann kyphosis, except:
Explanation
Obesity is not any more common in patients with Scheuermann kyphosis than in the general population.
Vertebral wedging is a common feature of Scheuermann kyphosis. Endplate irregularity is a common feature of Scheuermann kyphosis.
Schmorl nodes are a manifestation of the disordered behavior of the vertebral endplates under load. Back pain is common in Scheuermann kyphosis.
Vertebral wedging is a common feature of Scheuermann kyphosis. Endplate irregularity is a common feature of Scheuermann kyphosis.
Schmorl nodes are a manifestation of the disordered behavior of the vertebral endplates under load. Back pain is common in Scheuermann kyphosis.
Question 7High Yield
Which muscles are in the superficial volar compartment of the forearm?
Explanation
- Pronator teres, flexor carpi radialis longus, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris_
Question 8High Yield
A 65-year-old right–hand-dominant woman has been experiencing thenar and wrist pain for 18 months. She has no history of trauma. The pain worsens during the opening of jars, grasping, writing, and repetitive thumb use. Examination reveals tenderness to palpation over the volar thenar eminence, just distal to the scaphoid tubercle, and along the flexor carpi radialis sheath. A Watson scaphoid shift test produces pain but no instability or clunk. Radiographs reveal isolated scaphotrapeziotrapezoidal (STT) arthritis with mild dorsal intercalated segment instability (DISI) deformity. She has worn a splint on and off for the past year, has had multiple cortisone injections, and has modified her activity, all of which helped initially. She wants to move forward with surgical intervention. STT arthrodesis is chosen over distal pole scaphoid excision. What factor in her evaluation indicates that arthrodesis would be preferred over distal pole excision?
Explanation
Isolated STT arthritis is common and can cause substantial patient disability and pain. After nonsurgical treatment has failed, surgical intervention is warranted. Surgical options include distal pole scaphoid excision, STT arthrodesis, or carpometacarpal (CMC) arthroplasty, if concomitant thumb CMC degenerative changes are present. Distal pole scaphoid excision is less commonly employed for the treatment of STT arthritis, because of the potential development of intercalated segmental instability. However, distal pole scaphoid excision is less technically demanding, engenders fewer surgical complications, and promotes a faster return to previous activity levels. In any patient with preoperative carpal malalignment, removing the distal pole of the scaphoid would exacerbate that deformity and could lead to symptoms from the DISI deformity. Thus, in this patient with mild DISI deformity seen on _preoperative radiographs, STT arthrodesis is the most appropriate treatment option._
Question 9High Yield
Which of the following molecules are present in a hematoma after a fracture and aid in modulating cell proliferation and differentiation:
Explanation
Important concepts to remember regarding signaling proteins include:
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF)
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF)
Question 10High Yield
Figures 18a and 18b are the radiographs of an obese 75-year-old man with a rigid acquired flatfoot deformity. What is the best treatment option?
Explanation
For stage III adult-acquired flatfoot deformity characterized by dysfunction of the posterior tibial tendon, rigid valgus deformity of the hindfoot, and arthritic changes of the hindfoot joints,arthrodesis is the favored procedure. In an overweight patient with degenerative changes affecting the subtalar and Chopart joints, triple arthrodesis is the best treatment option. Subtalar arthrodesis only addresses the talocalcaneal joint and continues to render the patient symptomatic in the talonavicular and calcaneocuboid joints. Advanced stage III disease precludes reconstructive procedures involving calcaneal osteotomy and tendon transfer.
Question 11High Yield
Which of the following types of bone behaves in an isotropiCmanner when loaded in different directions:
Explanation
Woven bone is immature bone that is found in newborns, fracture callus, and the metaphyses of growing bone. In woven bone, the collagen fibers are oriented in a completely random fashion. When woven bone is loaded, it performs in an isotropiCmanner. The other types of bone (lamellar, cortical, cancellous, and plexiform) contain collagen that is oriented along the long axis of the bone and cause the bone to perform anisotropically.
Question 12High Yield
A 19-year-old male sustains the injury shown in Figure A while skiing. Injury to what structure should be evaluated intraoperatively during fixation of the fibula?

Explanation
According to the referenced study by Jenkinson et al, up to 37% of operatively treated ankle fractures can have undetected syndesmotic instability when examined intraoperatively. This is important due to the negative effects of a displaced mortise and the abnormal loading forces seen on the talus with even a 2mm lateral shift. Also, fibular fractures >4.5cm proximal to the mortise are more likely to be associated with syndesmotic instability, especially when deltoid ligament tears are present. When fixing the syndesmosis, Tornetta et al's referenced study has shown that the syndesmotic compression has no negative effects on ankle range of motion.
Question 13High Yield
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?


Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
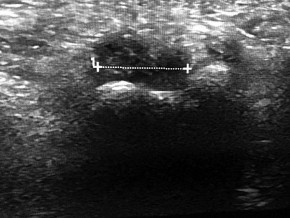
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
Question 14High Yield
When performing open reduction and internal fixation of radial neck fractures, the plate should be placed:
Explanation
The "nonarticular safe-zone" comprising only 90º of the radial head circumference is achieved by placing the plate posterior with the arm in supination.
Question 15High Yield
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?



Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
Question 16High Yield
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
33
33
Explanation
The patient's radiographs demonstrate bone loss of the medial humeral head. He has risk factors for both septic arthritis/osteomyelitis, and metastatic cancer, and it is important to understand the extent of his pathology before moving forward with surgical intervention. An MRI scan would assist in the diagnosis and demonstrate the extent of disease/tissue involvement. Administration of IV antibiotics prior to obtaining appropriate cultures would decrease the success rate of treatment in the setting of infection, and mistreat the pathology in the setting of metastasis. Similarly, obtaining cultures from the draining sinus tract would fail to account for the possible tumor diagnosis and may result in inaccurate culture results.
Question 17High Yield
Which of the following is the most common adverse event from intravenous bisphosphonate therapy:
Explanation
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0% Correct Answe Pyrexia and myalgia
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0% Correct Answe Pyrexia and myalgia
Question 18High Yield
A 20-year-old healthy female endurance athlete has lower leg pain and dorsal foot paresthesias after
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
| Compartment | Baseline | 1 Minute | 5 Minutes | |---|---|---|---| | Anterior | 7 | 32 | 25 | | Lateral | 8 | 29 | 23 | | Superficial Posterior | 12 | 25 | 17 | | Deep Posterior | 14 | 22 | 16 |
The patient decides to pursue surgical intervention. Which compartments should be released?
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
| Compartment | Baseline | 1 Minute | 5 Minutes | |---|---|---|---| | Anterior | 7 | 32 | 25 | | Lateral | 8 | 29 | 23 | | Superficial Posterior | 12 | 25 | 17 | | Deep Posterior | 14 | 22 | 16 |
The patient decides to pursue surgical intervention. Which compartments should be released?
Explanation
The diagnostic criteria for chronic exertional compartment syndrome is pressure >15 mm Hg at rest, or
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible _for the patient's symptoms and falls below current thresholds for diagnosis._
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible _for the patient's symptoms and falls below current thresholds for diagnosis._
Question 19High Yield
A
B
Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?
B
Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?


Explanation
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
[Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. ](http://www.ncbi.nlm.nih.gov/pubmed/17575617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17575617) Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
RECOMMENDED READINGS
[Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. ](http://www.ncbi.nlm.nih.gov/pubmed/17575617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17575617) Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
Question 20High Yield
A 17-year-old patient presents with pain in the second toe. Pain becomes worse with exercise and has been present for 6 months. On examination, swelling is present around the metatarsophalangeal joint, and pain is present over the joint and upon squeezing the forefoot. Radiographic evaluation demonstrates a lucency in the second metatarsal head. The most likely cause of this condition is:
Explanation
This patient has the typical features of Freibergâs osteochondrosis of the second metatarsal head. There is swelling present, which is not noted in association with a neuroma, even though the clinical findings may be similar. Synovitis is common but not associated with radiographic changes.
Question 21High Yield
If surgical intervention is delayed for 3 months and intraoperatively the surgeon finds that primary repair can be performed but hyperflexion of the elbow to 90 degrees is necessary, what is the likely long-term consequence?
Explanation
This patient classically depicts an acute complete distal biceps rupture. This injury typically results from an eccentric load applied to a flexed elbow. This occurs most often among middle-aged men. Often, a clinical examination is adequate to confirm the diagnosis. When needed, standardized MR imaging at the point at which the injured arm is flexed at the elbow and abducted at the shoulder with the forearm in supination can increase sensitivity for diagnosis of a complete tear.
Patients who do not undergo surgical repair have an approximate 40% loss of supination strength and 30% loss of elbow flexion strength. Some patients describe persistent painful cramping and difficulty with repetitive activities such as using a screwdriver. Others may be able to modify their activities and tolerate the functional loss.
Studies comparing single anterior repair to double-incision posterior repair have reported similar success rates for pain and function. Grewal and associates performed a prospective randomized clinical trial comparing single- vs double-incision distal biceps tendon repairs and reported that both techniques can provide equally successful results. However, the anterior single-incision approach resulted in a statistically significant higher incidence of transient lateral antebrachial nerve palsy (19/47 vs 3/43).
Studies have shown that primary repair may be possible for patients with subacute or chronic distal biceps tears. This may obviate the need for an additional interposition allograft reconstruction. Morrey and associates performed primary repair on 19 chronic distal biceps ruptures by hyperflexing the elbow to anatomically reattach the tendon to the biceps tuberosity. Surprisingly,
this did not lead to any significant loss of elbow range of motion or flexion contracture. Elbow flexion strength was improved.
RECOMMENDED READINGS
42. [Schmidt CC, Jarrett CD, Brown BT. The distal biceps tendon. J Hand Surg Am. 2013 Apr;38(4):811-21; quiz 821. doi: 10.1016/j.jhsa.2013.01.042. Epub 2013 Mar 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/23474326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23474326)
43. [Giuffrè BM, Moss MJ. Optimal positioning for MRI of the distal biceps brachii tendon: flexed abducted supinated view. AJR Am J Roentgenol. 2004 Apr;182(4):944-6. ](http://www.ncbi.nlm.nih.gov/pubmed/15039168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15039168)
44. [Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus nonoperative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. ](http://www.ncbi.nlm.nih.gov/pubmed/3972865)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3972865)
45. [Nesterenko S, Domire ZJ, Morrey BF, Sanchez-Sotelo J. Elbow strength and endurance in patients with a ruptured distal biceps tendon. J Shoulder Elbow Surg. 2010 Mar;19(2):184-9. doi: 10.1016/j.jse.2009.06.001. Epub 2009 Aug 6. PubMed PMID: 19664936. ](http://www.ncbi.nlm.nih.gov/pubmed/19664936)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19664936)
46. [Grewal R, Athwal GS, MacDermid JC, Faber KJ, Drosdowech DS, El-Hawary R, King GJ. Single versus double-incision technique for the repair of acute distal biceps tendon ruptures: a randomized clinical trial. J Bone Joint Surg Am. 2012 Jul 3;94(13):1166-74. doi: 10.2106/JBJS.K.00436. PubMed PMID: 22760383. ](http://www.ncbi.nlm.nih.gov/pubmed/22760383)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22760383)
47. [Morrey ME, Abdel MP, Sanchez-Sotelo J, Morrey BF. Primary repair of retracted distal biceps tendon ruptures in extreme flexion. J Shoulder Elbow Surg. 2014 May;23(5):679-85. doi: 10.1016/j.jse.2013.12.030. PubMed PMID: 24745316. ](http://www.ncbi.nlm.nih.gov/pubmed/24745316)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24745316)
Patients who do not undergo surgical repair have an approximate 40% loss of supination strength and 30% loss of elbow flexion strength. Some patients describe persistent painful cramping and difficulty with repetitive activities such as using a screwdriver. Others may be able to modify their activities and tolerate the functional loss.
Studies comparing single anterior repair to double-incision posterior repair have reported similar success rates for pain and function. Grewal and associates performed a prospective randomized clinical trial comparing single- vs double-incision distal biceps tendon repairs and reported that both techniques can provide equally successful results. However, the anterior single-incision approach resulted in a statistically significant higher incidence of transient lateral antebrachial nerve palsy (19/47 vs 3/43).
Studies have shown that primary repair may be possible for patients with subacute or chronic distal biceps tears. This may obviate the need for an additional interposition allograft reconstruction. Morrey and associates performed primary repair on 19 chronic distal biceps ruptures by hyperflexing the elbow to anatomically reattach the tendon to the biceps tuberosity. Surprisingly,
this did not lead to any significant loss of elbow range of motion or flexion contracture. Elbow flexion strength was improved.
RECOMMENDED READINGS
42. [Schmidt CC, Jarrett CD, Brown BT. The distal biceps tendon. J Hand Surg Am. 2013 Apr;38(4):811-21; quiz 821. doi: 10.1016/j.jhsa.2013.01.042. Epub 2013 Mar 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/23474326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23474326)
43. [Giuffrè BM, Moss MJ. Optimal positioning for MRI of the distal biceps brachii tendon: flexed abducted supinated view. AJR Am J Roentgenol. 2004 Apr;182(4):944-6. ](http://www.ncbi.nlm.nih.gov/pubmed/15039168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15039168)
44. [Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus nonoperative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. ](http://www.ncbi.nlm.nih.gov/pubmed/3972865)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3972865)
45. [Nesterenko S, Domire ZJ, Morrey BF, Sanchez-Sotelo J. Elbow strength and endurance in patients with a ruptured distal biceps tendon. J Shoulder Elbow Surg. 2010 Mar;19(2):184-9. doi: 10.1016/j.jse.2009.06.001. Epub 2009 Aug 6. PubMed PMID: 19664936. ](http://www.ncbi.nlm.nih.gov/pubmed/19664936)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19664936)
46. [Grewal R, Athwal GS, MacDermid JC, Faber KJ, Drosdowech DS, El-Hawary R, King GJ. Single versus double-incision technique for the repair of acute distal biceps tendon ruptures: a randomized clinical trial. J Bone Joint Surg Am. 2012 Jul 3;94(13):1166-74. doi: 10.2106/JBJS.K.00436. PubMed PMID: 22760383. ](http://www.ncbi.nlm.nih.gov/pubmed/22760383)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22760383)
47. [Morrey ME, Abdel MP, Sanchez-Sotelo J, Morrey BF. Primary repair of retracted distal biceps tendon ruptures in extreme flexion. J Shoulder Elbow Surg. 2014 May;23(5):679-85. doi: 10.1016/j.jse.2013.12.030. PubMed PMID: 24745316. ](http://www.ncbi.nlm.nih.gov/pubmed/24745316)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24745316)
Question 22High Yield
Quadriceps tendonitis
_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?












Explanation
--The patient is provided with a medial unloader brace that provides substantial pain relief and he is able to work while wearing the brace. After 4 months he returns to work and says that while the brace enable him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
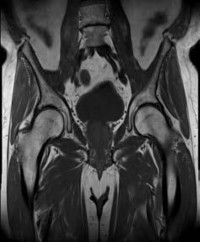
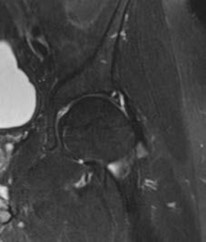
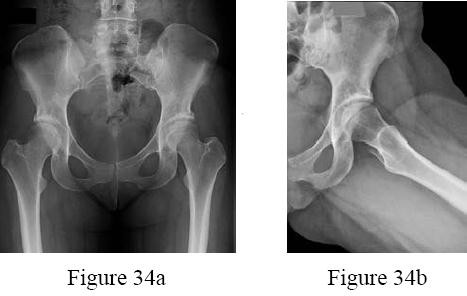
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
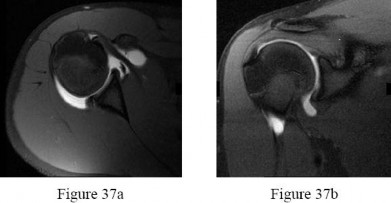
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
Question 23High Yield
A 35-year-old man with a 2-part anterior proximal humerus fracture-dislocation
Explanation
- Open reduction and internal fixation with or without bone grafting_
Question 24High Yield
This finding has been shown to be variably present in asymptomatic patients, and its incidence increases with age.
Explanation
- Figure 72a Figure 72b
Question 25High Yield
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 26High Yield
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?
Explanation
A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
REFERENCE: Mazzoca AD: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 308-309.
REFERENCE: Mazzoca AD: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 308-309.
Question 27High Yield
A 16-year-old football player reports the acute onset of pain in his left foot. An AP radiograph is shown in Figure
8. ##### What treatment is most likely to result in successful healing for this injury?
8. ##### What treatment is most likely to result in successful healing for this injury?
Explanation
DISCUSSION: Fractures in this region of the fifth metatarsal have been shown to be prone to delayed union and
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
Question 28High Yield
Figure 1 is the radiograph of a 10-year-old boy who has had insidious onset of right shoulder pain for 4 months. He plays baseball 3-4 times per week. He is right-hand dominant. His pain mostly occurs when throwing the ball, but can also occur with non-throwing activities. He is also reporting that his velocity is now decreasing. Physical examination and radiographs of the shoulder are normal. What is the best next best step in management of this patient?

Explanation
■
The patient is suffering from what is called Little League shoulder. It is a traction injury to the proximal humerus physis. Injury to this area is caused by repetitive stress seen in overhead throwing sports. The incidence of this condition is increasing as the frequency and intensity of organized youth sport have increased, and it most commonly presents between age 9 and 12 years before closure of the physis. It is most common in baseball pitchers, football quarterbacks, and tennis players.
Immobilization with brace or cast is necessary for the most severe cases in patients experiencing persistent pain at rest, which is not the presentation of the patient here. Physical therapy is usually started early after a short period of rest for early rehabilitation. MRI is rarely necessary to confirm the diagnosis. Radiographs can show widening of the physis, especially compared with the contralateral side, but is not required for diagnosis.
■
The patient is suffering from what is called Little League shoulder. It is a traction injury to the proximal humerus physis. Injury to this area is caused by repetitive stress seen in overhead throwing sports. The incidence of this condition is increasing as the frequency and intensity of organized youth sport have increased, and it most commonly presents between age 9 and 12 years before closure of the physis. It is most common in baseball pitchers, football quarterbacks, and tennis players.
Immobilization with brace or cast is necessary for the most severe cases in patients experiencing persistent pain at rest, which is not the presentation of the patient here. Physical therapy is usually started early after a short period of rest for early rehabilitation. MRI is rarely necessary to confirm the diagnosis. Radiographs can show widening of the physis, especially compared with the contralateral side, but is not required for diagnosis.
Question 29High Yield
A 23-year-old woman with juvenile rheumatoid arthritis presents for treatment of painful forefoot deformity. Painful hallux valgus is present and is associated with dislocation of the lesser metatarsophalangeal joints. The recommended surgical treatment is:
Explanation
The gold standard surgical treatment for rheumatoid patients with severe forefoot deformities is first metatarsophalangeal fusion with second through fifth metatarsal head resections.
Question 30High Yield
1222) Which of the following fluoroscopic views is used to assess
intra-articular screw penetration during volar fixation of a distal radius fracture?
intra-articular screw penetration during volar fixation of a distal radius fracture?


Explanation
Due to radial inclination, a true lateral view of the wrist will not show whether screws from a volar plate are intra-articular; a 23° elevated lateral view is needed to adequately assess this.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
Question 31High Yield
Figures 42a through 42c are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?



Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
Question 32High Yield
Figures 27a and 27b are the radiographs of a 2-month-old with a swollen ankle and abdominal bruising.
Explanation
- Plain radiographs
Question 33High Yield
Which pathology is associated with this condition?
Explanation
- Apophysitis of the tibial tubercle_
Question 34High Yield
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
The MRI scan reveals a transection of the biceps muscle. The underlying brachialis is intact. This injury can occur as a result of a cord wrapped around the upper arm. Care should be taken to ensure that there is no concurrent vascular injury. A posterior subcutaneous lipoma appears as a well-encapsulated mass on T2-weighted images.
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 35High Yield
A 15-year-old football player was diagnosed with infectious mononucleosis 2 weeks ago. Today he states that he is relatively asymptomatic and would like to return to play. At what point can the patient return to full contact practice?
Explanation
Infectious mononucleosis presents with fever, pharyngitis, fatigue and lymph node enlargement. It is common among individuals in their teens and early twenties. Participation in contact activities during an acute illness with unresolved splenomegaly increases the risk of splenic rupture. Evidence- based return to play criteria recommend that a patient may return to full- contact activities 4 weeks after the onset of their symptoms with resolution of splenomegaly. An ultrasonography of the spleen can help confirm that the spleen has returned to normal size.
75
75
Question 36High Yield
Figure 51 is the MR image of a 23-year-old Minor League pitcher who has dominant elbow pain. He reports a pop while throwing and loss of velocity and control. He has failed nonsurgical treatment that included rest and physical therapy. What is the most common complication following surgical treatment of this injury?
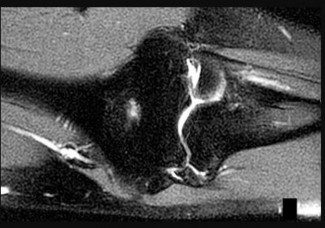
Explanation
This competitive thrower’s clinical picture and imaging findings are consistent with an ulnar collateral ligament (UCL) injury. For patients who fail nonsurgical treatment, UCL reconstruction is an accepted surgical solution. About 80% of overhead athletes return to at least the same level of competition. All of the responses are potential complications following UCL reconstruction, but ulnar neuritis is the most common, occurring in approximately 6% to 13% of patients.
RECOMMENDED READINGS
75. [Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008 Jun;36(6):1193-205. doi: 10.1177/0363546508319053. Review. PubMed PMID: 18490476. ](http://www.ncbi.nlm.nih.gov/pubmed/18490476)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18490476)
76. [Cain EL Jr, Andrews JR, Dugas JR, Wilk KE, McMichael CS, Walter JC 2nd, Riley RS, Arthur ST. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: Results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010 Dec;38(12):2426-34. doi: 10.1177/0363546510378100. Epub 2010 Oct 7. PubMed PMID: 20929932. ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20929932)
77. Watson JN, McQueen P, Hutchinson MR. A systematic review of ulnar collateral ligament reconstruction techniques. Am J Sports Med. 2014 Oct;42(10):2510-6. doi: 10.1177/0363546513509051. Epub 2013 Nov 12. Review. PubMed PMID: 24220014.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24220014)
RECOMMENDED READINGS
75. [Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008 Jun;36(6):1193-205. doi: 10.1177/0363546508319053. Review. PubMed PMID: 18490476. ](http://www.ncbi.nlm.nih.gov/pubmed/18490476)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18490476)
76. [Cain EL Jr, Andrews JR, Dugas JR, Wilk KE, McMichael CS, Walter JC 2nd, Riley RS, Arthur ST. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: Results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010 Dec;38(12):2426-34. doi: 10.1177/0363546510378100. Epub 2010 Oct 7. PubMed PMID: 20929932. ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20929932)
77. Watson JN, McQueen P, Hutchinson MR. A systematic review of ulnar collateral ligament reconstruction techniques. Am J Sports Med. 2014 Oct;42(10):2510-6. doi: 10.1177/0363546513509051. Epub 2013 Nov 12. Review. PubMed PMID: 24220014.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24220014)
Question 37High Yield
The following pair of tendons is affected in De Quervain disease:
Explanation
De Quervain disease affects the tendons in the first dorsal compartment, the extensor pollicis brevis and the abductor pollicis longus (consisting of 2 to 7 individual tendon slips). The extensor pollicis longus traverses the third dorsal compartment. The abductor pollicis brevis and the opponens pollicis are thenar muscles and do not lie within any of the dorsal compartments.
Question 38High Yield
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. 20
Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis
.
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
A. directly posterior to the posterior cruciate ligament (PCL).
B. posteromedial to the PCL.
C. posterolateral to the PCL.
D. in the posteromedial corner of the knee.
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Correct answer : C
A 70-year-old woman has severe stiffness of her knee following a primary total knee arthroplasty (TKA) 3 years ago. The patient has well-fixed femoral and tibial components, and a preoperative work-up for infection is negative. The decision is made to proceed with a revision TKA of both the femoral and tibial components. An extensile exposure is planned to facilitate removal of the components. What extensile exposure would require the least modification of postoperative rehabilitation with regards to weight bearing and range of motion?
A. Quadriceps snip
B. Lateral parapatellar approach
C. V-Y quadriceps turndown
D. Tibial tubercle osteotomy
Achievement of adequate exposure in revision TKA is critical as it reduces the surgical time, enhances the ability for both component removal and reconstruction, and avoids devastating complications such as extensor mechanism disruption. Numerous extensile exposures in revision TKA have been described.
21
A tibial tubercle osteotomy, V-Y tendon plasty, and V-Y quadriceps turndown all provide excellent exposure, but require a modification in postoperative rehabilitation as they often require a period of immobilization followed by limits in range of motion. In contrast, the quadriceps snip allows immediate weight bearing along with progressive range of motion; no modification of postoperative rehabilitation is required. Lateral parapatellar approach would offer no benefit for exposure.
Correct answer : A
Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis
.
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
A. directly posterior to the posterior cruciate ligament (PCL).
B. posteromedial to the PCL.
C. posterolateral to the PCL.
D. in the posteromedial corner of the knee.
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Correct answer : C
A 70-year-old woman has severe stiffness of her knee following a primary total knee arthroplasty (TKA) 3 years ago. The patient has well-fixed femoral and tibial components, and a preoperative work-up for infection is negative. The decision is made to proceed with a revision TKA of both the femoral and tibial components. An extensile exposure is planned to facilitate removal of the components. What extensile exposure would require the least modification of postoperative rehabilitation with regards to weight bearing and range of motion?
A. Quadriceps snip
B. Lateral parapatellar approach
C. V-Y quadriceps turndown
D. Tibial tubercle osteotomy
Achievement of adequate exposure in revision TKA is critical as it reduces the surgical time, enhances the ability for both component removal and reconstruction, and avoids devastating complications such as extensor mechanism disruption. Numerous extensile exposures in revision TKA have been described.
21
A tibial tubercle osteotomy, V-Y tendon plasty, and V-Y quadriceps turndown all provide excellent exposure, but require a modification in postoperative rehabilitation as they often require a period of immobilization followed by limits in range of motion. In contrast, the quadriceps snip allows immediate weight bearing along with progressive range of motion; no modification of postoperative rehabilitation is required. Lateral parapatellar approach would offer no benefit for exposure.
Correct answer : A
Question 39High Yield
An 82-year-old female sustains a valgus-impacted subcapital femoral neck fracture and undergoes cannulated screw fixation as shown in Figure A. She returns for her first follow-up visit one week later following another fall and now complains of severe hip pain. She is unable to bear weight on the limb, and a new radiograph reveals varus displacement of her fracture. She subsequently undergoes revision fixation but during this procedure, the femoral neck fracture displaces and becomes comminuted. Which is the most appropriate next step in management?

Explanation
In the scenario of an elderly patient with questionable fixation into the femoral head and a non-healed femoral neck fracture, proper treatment is arthroplasty. In a physiologically younger patient, reduction and fixation of the fractures (femoral neck and subtrochanteric, if present) with methods such as a valgus producing osteotomy at the level of the subtrochanteric fracture are
recommended.
Figure A shows cannulated screw fixation of a right femoral neck fracture.
The referenced study by Oakey et al evaluated strength of proximal femurs after cannulated hip screw placement and found that placement of an inverted triangle had a higher ultimate load to failure than placement in a standard triangle format (two screws distal).
recommended.
Figure A shows cannulated screw fixation of a right femoral neck fracture.
The referenced study by Oakey et al evaluated strength of proximal femurs after cannulated hip screw placement and found that placement of an inverted triangle had a higher ultimate load to failure than placement in a standard triangle format (two screws distal).
Question 40High Yield
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of
Explanation
The patient has extensor tendon ruptures at the level of the wrist that are the result of synovitis at the distal radioulnar joint (Vaughn-Jackson syndrome). Extensor indius proprius transfer appropriately matches strength and excursion of the ruptured extensor digiti quinti and extensor digitorum communis tendons. An extensor tenosynovectomy with distal radioulnar joint resection decreases the synovitis, which if left untreated may cause additional tendon ruptures. Radial head resection is used for posterior interosseous nerve compression secondary to radial head synovitis, and in this patient only two fingers are involved, which rules out this diagnosis. Dynamic splinting is not indicated for ruptured tendons. Metacarpophalangeal arthroplasties and imbrication of the sagittal bands are used for metacarpophalangeal arthritis and extensor tendon subluxation. If this was the problem, the patient should be able to maintain the fingers in extension after they are passively extended. Total wrist arthrodesis prevents the tenodesis effect, thus limiting effective tendon excursion and making the proposed transfer less effective.
REFERENCES: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999,
pp 1669-1684.
Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Leslie BM: Rheumatoid extensor tendon ruptures. Hand Clin 1989;5:191-202.
REFERENCES: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999,
pp 1669-1684.
Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Leslie BM: Rheumatoid extensor tendon ruptures. Hand Clin 1989;5:191-202.
Question 41High Yield
"C ollar button" abscess refers to:
Explanation
C ollar button abscess is an infection of web space and is usually a result of penetrating trauma. Treatment of such abscesses requires incision and drainage through dorsal and palmar incisions. C are must be taken to avoid the neurovascular bundles. Finger pulp infections are known as felon. Infections involving Parona's space is typically involved in a horseshoe abscess. Eponychial infections are limited to the nail fold. C ollar button abscesses do not include joint involvement.
Question 42High Yield
Blood cultures reveal methicillin-sensitive Staphylococcus aureus (MSSA). The patient's examination remains unchanged. In addition to outpatient serial laboratory studies and weekly observation for neurologic deterioration, which of the following is the most appropriate for nonoperative treatment?
Explanation
- An 8-week course of IV nafcillin
Question 43High Yield
Which radiographic finding indicates likely radial head replacement?
Explanation
- Wrist pain and asymmetry of the ipsilateral distal radioulnar joint_
Question 44High Yield
Figure 1 shows the radiograph obtained from a 67-year-old woman who has progressive wrist pain. She undergoes a salvage motion-sparing surgery that relies on the intact cartilage of the capitate head. It is necessary to preserve what structure during this procedure?


Explanation
---
EXPLANATION:
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be _required. The authors did cut through the dorsal intercarpal ligament in their exposure._
**Question 71of 100** At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
A. Radioscaphoid
1. Radiolunate
2. Scapholunate
3. Capitolunate
PREFERRED RESPONSE: A
EXPLANATION:
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal _involvement). The radiolunate joint is often spared._
EXPLANATION:
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be _required. The authors did cut through the dorsal intercarpal ligament in their exposure._
**Question 71of 100** At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
A. Radioscaphoid
1. Radiolunate
2. Scapholunate
3. Capitolunate
PREFERRED RESPONSE: A
EXPLANATION:
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal _involvement). The radiolunate joint is often spared._
Question 45High Yield
Which of the following findings on a neuromuscular examination is not characteristic of spasticity:
Explanation
Spasticity is a hallmark of upper motor lesions. Spasticity is characterized by hyperreflexia, clonus, and velocity-dependent resistance. After early childhood, muscle contracture also develops. Writhing movements are characteristic of athetosis, not spasticity.
Question 46High Yield
Slide 1
What structure is held in between the forceps in this photograph (Slide):
What structure is held in between the forceps in this photograph (Slide):
Explanation
The extensor retinaculum is an important structure in maintaining and possibly augmenting the stability of the lateral ankle and subtalar joint. The inferior root of the extensor retinaculum inserts in the floor of the sinus tarsi, improving stability of the subtalar joint. This structure can be used to augment a repair of ankle instability.
Question 47High Yield
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of**
Explanation
Following a CVA, the muscular imbalance often leads to a fixed contracture of the shoulder in adduction, internal rotation, and flexion. The responsible muscles include the pectoralis major, subscapularis, teres major, and latissimus dorsi. If stretching cannot produce enough improvement for axillary hygiene, then surgery is an option. If the shoulder resists external rotation during examination with the arm at the side, as in this patient, then the subscapularis is spastic and contributing to the deformity as well and needs to be released along with the pectoralis. Phenol nerve blocks are most effective and best given within 6 months of the initial CVA to be effective. Lidocaine blocks may be helpful in determining whether a deformity is caused by a fixed soft-tissue contracture or by spasticity but play no role once the contracture is present. The modified L’Episcopo procedure is indicated in patients with contracture secondary to brachial plexus birth palsies.
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 48High Yield
Figure 33 is the radiograph of a 62-year-old right-hand-dominant man who has wrist pain. When discussing surgical options with the patient, which radiographic finding, if present, would prevent scaphoid excision and 4-corner fusion from being the best course of treatment?

Explanation
Scaphoid nonunion advanced collapse is a common pattern of posttraumatic wrist arthritis. Treatment options include denervation, radial styloidectomy, excision of the distal nonunited scaphoid fragment, proximal row carpectomy (PRC), capitolunate arthrodesis, 4-corner arthrodesis, and complete wrist arthrodesis. Radial styloidectomy is not effective if there is degenerative change at the midcarpal joint. PRC is not an effective option when there is degenerative change at the proximal capitate. Four-corner arthrodesis is not an effective option if there is degenerative arthritic change at the lunate fossa; if this level of change is present, complete wrist arthrodesis is recommended.
RECOMMENDED READINGS
11. [Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis--update on evaluation and treatment. J Hand Surg Am. 2011 Apr;36(4):729-35. doi: 10.1016/j.jhsa.2011.01.018. Review. PubMed PMID: 21463735. ](http://www.ncbi.nlm.nih.gov/pubmed/21463735)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21463735)
12. [Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008 Oct;61(10):1210-8. Epub 2007 Oct 22. PubMed PMID: 17951122. ](http://www.ncbi.nlm.nih.gov/pubmed/17951122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17951122)
13. [Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am. 1994 Sep;19(5):751-9. PubMed PMID: 7806795. ](http://www.ncbi.nlm.nih.gov/pubmed/7806795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7806795)
RECOMMENDED READINGS
11. [Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis--update on evaluation and treatment. J Hand Surg Am. 2011 Apr;36(4):729-35. doi: 10.1016/j.jhsa.2011.01.018. Review. PubMed PMID: 21463735. ](http://www.ncbi.nlm.nih.gov/pubmed/21463735)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21463735)
12. [Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008 Oct;61(10):1210-8. Epub 2007 Oct 22. PubMed PMID: 17951122. ](http://www.ncbi.nlm.nih.gov/pubmed/17951122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17951122)
13. [Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am. 1994 Sep;19(5):751-9. PubMed PMID: 7806795. ](http://www.ncbi.nlm.nih.gov/pubmed/7806795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7806795)
Question 49High Yield
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
---
---










Explanation
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
---
---
Question 50High Yield
Figures 46a and 46b are the radiographs of a 20-year-old collegiate varsity athlete who reports lateral foot pain. What is the most appropriate management at this time?
---
---

Explanation
Fractures of the fifth metatarsal proximal metaphyseal-diaphyseal junction (Jones fracture)generally occur in young athletic patients and have relatively high rates of delayed union or nonunion with nonsurgical management. The fracture occurs in the hypovascular zone between the insertion of the peroneus brevis and tertius. These tendons cause a shearing across the fracture site, preventing stability and healing.
Nonsurgical functional bracing or casting may lead to a high rate of delayed union and nonunion. Internal fixation in the high-level athlete leads to the most predictable healing of the fracture in a timely fashion. The use of bone stimulators for this fracture is controversial.
---
Nonsurgical functional bracing or casting may lead to a high rate of delayed union and nonunion. Internal fixation in the high-level athlete leads to the most predictable healing of the fracture in a timely fashion. The use of bone stimulators for this fracture is controversial.
---
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon