Orthopedic O Upper Extremity Review | Dr Hutaif General -...
Key Takeaway
For anyone wondering about ORTHOPEDIC MCQS O11 UPPER EXTREMITY, Anterolateral elbow arthroscopy risks radial nerve injury, primarily resulting in loss of digital extension. This symptom is the most likely indicator of damage, as digital extension tests radial nerve function, distinct from ulnar or median nerve pathways. The preferred response to question regarding nerve injury complications confirms loss of digital extension as the key clinical manifestation.
Orthopedic O Upper Extremity Review | Dr Hutaif General -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
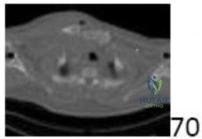
A 28-year-old semi-professional baseball pitcher presents with recurrent anterior glenohumeral instability despite dedicated rehabilitation. He has suffered 5 dislocations in the past 18 months. An axial CT scan reveals a glenoid bone loss of approximately 28% and an engaging Hill-Sachs lesion. The image provided shows a representative axial CT view of a shoulder with bone loss.
What is the most appropriate surgical management for this patient?

Explanation
Question 2
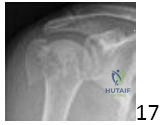
An 82-year-old female with severe osteopenia falls from a standing height, sustaining a 4-part valgus-impacted proximal humerus fracture, as shown in the image below. She has limited pre-injury shoulder function due to long-standing rotator cuff arthropathy and a low demand lifestyle.
What is the most appropriate surgical treatment option for this patient?

Explanation
Question 3
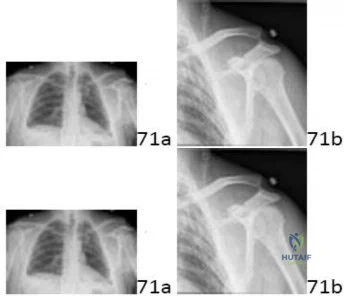
A 45-year-old male sustains a fall onto an outstretched hand, resulting in a complex elbow injury. Radiographs, similar to the one provided, confirm a posterior elbow dislocation, a Mason Type III radial head fracture, and a Regan-Morrey Type II coronoid fracture.
Which of the following represents the most appropriate sequence and combination of surgical interventions for this 'terrible triad' injury?

Explanation
Question 4
A 45-year-old right-hand dominant construction worker presents with chronic wrist pain, weakness, and limited range of motion 6 months after sustaining a distal radius fracture that was treated non-operatively. Radiographs, as depicted, demonstrate a healed distal radius malunion with 25 degrees of dorsal tilt, 8 mm of radial shortening, and a positive ulnar variance.
Given his symptoms and radiographic findings, what is the most appropriate surgical management?

Explanation
Question 5
A 30-year-old male presents with chronic right wrist pain and limited motion following a fall two years prior. Initial radiographs were negative, but subsequent imaging, including the provided X-ray, shows a scaphoid waist nonunion with evidence of proximal pole sclerosis and cystic changes, consistent with avascular necrosis (AVN). There is no signs of capitolunate or radioscaphoid arthritis.
What is the most appropriate surgical intervention for this patient?
Explanation
Question 6
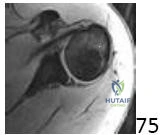
A 68-year-old male presents with chronic severe right shoulder pain and significant weakness, limiting his active abduction to 60 degrees. MRI imaging, similar to the one shown, confirms a massive, irreparable posterosuperior rotator cuff tear with significant superior migration of the humeral head and Goutallier Grade 3 fatty infiltration of the infraspinatus.
Given these findings and his age, what is the most appropriate surgical intervention?

Explanation
Question 7
A 55-year-old diabetic patient presents with a 6-month history of progressive right cubital tunnel syndrome. Clinical examination reveals severe intrinsic muscle atrophy in the hand (guttering between metacarpals), complete sensory loss in the ulnar nerve distribution, and a positive Froment's sign. Nerve conduction studies (NCS) and electromyography (EMG) confirm severe ulnar neuropathy at the elbow with evidence of axonal loss and denervation changes in the intrinsic muscles. What is the most appropriate surgical approach for this patient?
Explanation
Question 8
A 50-year-old concert pianist presents with severe, debilitating pain and progressive instability at the base of her right thumb, significantly impacting her ability to play. Radiographs, as shown, confirm Eaton-Littler Stage IV carpometacarpal (CMC) joint arthritis with subluxation and severe joint space narrowing. Conservative management, including injections and splinting, has failed. Maintaining excellent pinch strength and range of motion is paramount for her profession.
Which surgical intervention is most appropriate for this patient?
Explanation
Question 9
A 35-year-old patient sustains a clean laceration to the palmar aspect of the ring finger at the level of the proximal phalanx (Zone II), resulting in complete transection of both the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) tendons. Primary repair is performed within 6 hours. Which of the following post-operative rehabilitation protocols is generally considered most appropriate and evidence-based for optimizing outcomes in this injury?
Explanation
Question 10
A 28-year-old male presents to the emergency department 4 hours after a crush injury to his right forearm. He complains of excruciating pain in his forearm, disproportionate to the injury, which is markedly exacerbated by passive extension of his fingers. His forearm is tense and swollen, but radial and ulnar pulses are palpable, and capillary refill is brisk. Sensory examination is normal. What is the most appropriate immediate next step in management?
Explanation
Question 11
A 35-year-old male sustains a midshaft clavicle fracture. Which of the following radiographic or clinical findings is the most significant predictor of nonunion with nonoperative management?
Explanation
Question 12
An 80-year-old female with severe rheumatoid arthritis sustains a comminuted intra-articular distal humerus fracture (AO/OTA 13-C3). Radiographs show profound osteopenia. What is the most appropriate surgical management?
Explanation
Question 13
A 45-year-old heavy laborer presents with an irreparable massive rotator cuff tear involving the supraspinatus and infraspinatus. The subscapularis and teres minor are intact, and he lacks active external rotation. Which of the following is the most appropriate surgical option?
Explanation
Question 14
A 25-year-old male sustains a closed, spiral fracture of the distal third of the humeral shaft (Holstein-Lewis fracture). Upon initial presentation in the emergency department, he has weak wrist extension and numbness in the first dorsal web space. What is the most appropriate next step in management?
Explanation
Question 15
A 22-year-old male presents with radial-sided wrist pain after a fall. Imaging reveals a displaced fracture of the proximal pole of the scaphoid. Why is this specific fracture pattern at a high risk for avascular necrosis (AVN)?
Explanation
Question 16
Following a primary repair of a Zone II flexor tendon injury in the index finger, a patient undergoes an early active mobilization protocol. What is the primary biomechanical advantage of this rehabilitation strategy compared to static immobilization?
Explanation
Question 17
A 45-year-old male presents with acute anterior elbow pain and a palpable defect after feeling a 'pop' while lifting a heavy couch. The Hook test is positive. If the surgeon elects to perform a single-incision anterior approach for anatomic repair, which of the following nerves is at highest risk of iatrogenic injury?
Explanation
Question 18
A 22-year-old cyclist sustains a closed midshaft clavicle fracture with 2.5 cm of shortening.
The patient asks about the expected outcome if he chooses non-operative management. Which of the following is the most likely functional deficit associated with non-operative treatment of significantly shortened midshaft clavicle fractures?
Explanation
Question 19
A 28-year-old elite volleyball player complains of vague posterior shoulder pain. On examination, he has full active abduction but marked weakness in external rotation. MRI reveals a paralabral cyst at the spinoglenoid notch. Which muscle(s) will show denervation changes on EMG?
Explanation
Question 20
A 35-year-old male presents to the ER after a generalized seizure. His arm is locked in internal rotation and he cannot passively externally rotate past 0 degrees. An AP radiograph shows a symmetric, rounded humeral head ('lightbulb sign').
CT imaging is obtained. What specific osseous defect is most likely to be present on the humeral head?
Explanation
Question 21
A 21-year-old male falls on an outstretched hand and presents with anatomic snuffbox tenderness. Imaging confirms an acute, displaced fracture of the proximal pole of the scaphoid.
What is the most appropriate surgical approach for this specific fracture pattern, and why?
Explanation
Question 22
A 30-year-old carpenter presents with progressive, activity-related dorsal wrist pain. Radiographs reveal sclerosis, fragmentation, and collapse of the lunate (Kienböck's disease stage IIIA), with an ulnar variance of -3 mm. What is the most appropriate primary surgical intervention?
Explanation
Question 23
A 65-year-old osteoporotic female presents with a distal radius fracture featuring a displaced volar intra-articular fragment (Volar Barton's fracture).
If this fracture is treated with a dorsal spanning plate instead of a volar buttress plate, what is the most likely mechanism of failure?
Explanation
Question 24
A 28-year-old male falls from a roof. His lateral wrist radiograph demonstrates a 'spilled teacup' sign, with the capitate displaced dorsally to the lunate.
Which peripheral nerve is at the highest acute risk of compression in this clinical scenario?
Explanation
Question 25
A 55-year-old female presents with bilateral base of thumb pain, positive grind tests, and radiographic evidence of severe trapeziometacarpal joint space narrowing, osteophytes, and subchondral sclerosis (Eaton-Littler Stage III). Conservative management has failed. What is the gold standard surgical treatment?
Explanation
Question 26
A 32-year-old mechanic presents with an infected index finger after a puncture wound. Which of the following is NOT one of Kanavel's cardinal signs for acute pyogenic flexor tenosynovitis?
Explanation
Question 27
A 30-year-old male sustains a closed spiral fracture of the distal third of the humeral shaft (Holstein-Lewis fracture). On presentation, he exhibits a complete radial nerve palsy. What is the most appropriate initial management?
Explanation
Question 28
A 21-year-old collegiate baseball pitcher reports medial elbow pain during the late cocking and early acceleration phases of throwing. MRI confirms a full-thickness tear of the anterior bundle of the ulnar collateral ligament (UCL). To correctly reconstruct this ligament, where must the ulnar tunnel be primarily centered?
Explanation
Question 29
A 45-year-old heavy laborer presents with deep shoulder pain and mechanical catching. MRI arthrogram reveals a Type II SLAP tear. Given his age and occupational demands, current literature suggests which surgical intervention provides the most reliable return to work and pain relief?
Explanation
Question 30
A 25-year-old rugby player sustains a Type V acromioclavicular (AC) joint separation, characterized by >100% superior displacement of the clavicle into the trapezius fascia. What is the most widely accepted surgical approach for this severe injury?
Explanation
Question 31
A 30-year-old powerlifter feels a tearing sensation in his anterior chest while performing a heavy bench press. Examination reveals loss of the anterior axillary fold. When evaluating a pectoralis major rupture, where does the failure most commonly occur?
Explanation
Question 32
A 25-year-old military recruit presents with aching shoulder pain and notable medial prominence of his right scapula (medial winging) when asked to perform a wall push-up. Which nerve is most likely injured?
Explanation
Question 33
A 35-year-old skier falls while holding his pole, sustaining a hyperabduction injury to the thumb. Clinical examination reveals gross laxity of the metacarpophalangeal (MCP) joint to valgus stress. A Stener lesion is suspected. What anatomical structure prevents spontaneous healing of the torn ulnar collateral ligament (UCL) in this lesion?
Explanation
Question 34
A 24-year-old male is trapped under heavy machinery, resulting in a severe crush injury to his forearm. On examination, he has extreme pain with passive extension of his fingers. In acute compartment syndrome of the volar forearm, which muscle is most susceptible to irreversible ischemia and subsequent Volkmann's contracture?
Explanation
Question 35
A 20-year-old rugby player presents with the inability to actively flex the DIP joint of his ring finger after grabbing an opponent's jersey. Radiographs show a small bony avulsion fragment localized at the level of the PIP joint. What is the correct classification and recommended timeline for repair?
Explanation
Question 36
A patient presents with a 'terrible triad' of the elbow, which includes a posterior dislocation, radial head fracture, and coronoid fracture. When performing surgical reconstruction for this injury complex, what is the standard, biomechanically validated sequence of fixation?
Explanation
Question 37
A 42-year-old male bodybuilder feels a 'pop' in his antecubital fossa while performing heavy deadlifts. Clinical examination reveals a positive hook test. If a single-incision anterior surgical approach is chosen for repair, which structure is at the greatest risk of iatrogenic injury?
Explanation
Question 38
Reverse total shoulder arthroplasty (RTSA) is indicated for a 72-year-old with pseudoparalysis secondary to a massive irreparable rotator cuff tear. How does RTSA alter the shoulder biomechanics to allow the deltoid to initiate abduction?
Explanation
Question 39
A 35-year-old male sustains a distal third spiral humeral shaft fracture (Holstein-Lewis). Upon arrival at the emergency department, he is unable to extend his wrist or fingers. Closed reduction and splinting are performed, but post-reduction examination shows no change in his neurologic status. What is the most appropriate next step in management?
Explanation
Question 40
A 60-year-old female undergoes volar locking plate fixation for a displaced distal radius fracture. Six months postoperatively, she presents with an inability to actively flex the interphalangeal joint of her thumb. What is the most likely cause?
Explanation
Question 41
A 40-year-old male presents with severe wrist and elbow pain after falling from a ladder. Radiographs reveal a comminuted, unsalvageable radial head fracture. Wrist examination demonstrates DRUJ instability. Which of the following is absolutely contraindicated?
Explanation
Question 42
A 22-year-old male presents with a nonunion of a proximal pole scaphoid fracture 8 months after the initial injury. MRI reveals avascular necrosis (AVN) of the proximal pole. What is the most appropriate surgical management?
Explanation
Question 43
A 19-year-old male rugby player sustains a direct blow to the medial clavicle, resulting in a posterior sternoclavicular dislocation. He complains of mild dysphagia but has normal vital signs. What is the most appropriate initial management step?
Explanation
Question 44
During an in situ ulnar nerve decompression at the elbow, the surgeon must release multiple potential sites of compression. Which of the following is the most proximal site of potential ulnar nerve entrapment?
Explanation
Question 45
A 32-year-old carpenter presents with chronic dorsal wrist pain. Radiographs demonstrate Kienbock's disease with sclerosis of the lunate, no lunate collapse, and ulnar minus variance. What is the most appropriate surgical treatment?
Explanation
Question 46
Which of the following is an absolute indication for open reduction and internal fixation of an acute midshaft clavicle fracture?
Explanation
Question 47
A 25-year-old elite overhead throwing athlete undergoes arthroscopy for a symptomatic Type II SLAP tear that failed conservative management. What is the pathomechanical basis of this injury during the late cocking phase of throwing?
Explanation
Question 48
A 6-year-old child sustains a Bado Type I Monteggia fracture-dislocation. Closed reduction of the ulna fracture is achieved, but the radial head remains anteriorly dislocated. What is the most likely blocking structure preventing radial head reduction?
Explanation
Question 49
A 50-year-old diabetic female presents with 'frozen shoulder'. She has significant limitation of passive external rotation with the arm at the side. Contracture of which of the following structures is primarily responsible for this specific physical exam finding?
Explanation
Question 50
A 55-year-old female presents with base of thumb pain. Radiographs reveal Eaton-Littler Stage III basal joint arthritis. She is scheduled for a ligament reconstruction and tendon interposition (LRTI). Which tendon is most commonly harvested for this procedure?
Explanation
Question 51
A 42-year-old female presents with chronic lateral elbow pain. She has point tenderness 4 cm distal to the lateral epicondyle. Pain is exacerbated by resisted extension of the middle finger with the elbow extended. What is the most likely site of nerve compression?
Explanation
Question 52
Tension band wiring is an accepted treatment for simple transverse olecranon fractures. This fixation principle converts which type of force at the articular surface into compressive forces during active elbow flexion?
Explanation
Question 53
A 48-year-old female presents with numbness in her thumb, index, and middle fingers. Phalen's test is negative, but she has a positive Tinel's sign in the proximal forearm. She also reports pain in the proximal forearm with resisted forearm pronation. Which condition is most likely?
Explanation
Question 54
A 45-year-old weightlifter presents with a sudden 'pop' and ecchymosis in his right antecubital fossa. A reverse Popeye sign is noted. He undergoes a single-incision anterior approach for distal biceps tendon repair. Which of the following neurologic structures is at the highest risk of injury during this specific surgical approach?
Explanation
Question 55
A 40-year-old male presents with chronic wrist pain. Radiographs reveal a scaphoid nonunion with advanced radioscaphoid arthritis and narrowing of the capitolunate joint space, but preservation of the radiolunate articulation. Which of the following is the most appropriate surgical intervention?
Explanation
Question 56
A 22-year-old collegiate baseball pitcher reports medial elbow pain during the late cocking and early acceleration phases of throwing. On examination, he has valgus laxity when the elbow is flexed between 30 and 120 degrees. Which specific anatomical structure is most likely compromised?
Explanation
Question 57
A 32-year-old male sustains a closed distal-third humeral shaft fracture (Holstein-Lewis type). On initial evaluation, his radial nerve function is completely intact. Following closed reduction and splint application, he is found to have an inability to extend his wrist and fingers. What is the most appropriate next step in management?
Explanation
Question 58
A 25-year-old tennis player complains of shoulder weakness and a prominent shoulder blade following a viral illness. On physical examination, forward elevation of the arm against resistance demonstrates pronounced medial winging of the scapula. An injury to which of the following nerves is the most likely cause of this clinical presentation?
Explanation
Question 59
A 65-year-old female presents with an inability to flex her thumb interphalangeal joint six months after undergoing volar plate fixation for a distal radius fracture. Radiographs indicate the plate is positioned distally, bridging the watershed line. Which of the following tendons is most likely ruptured?
Explanation
Question 60
A 58-year-old female with advanced base of thumb arthritis undergoes a ligament reconstruction and tendon interposition (LRTI) procedure using the flexor carpi radialis (FCR) tendon. Which primary stabilizing ligament of the first carpometacarpal joint is this procedure attempting to reconstruct?
Explanation
Question 61
A 34-year-old manual laborer presents with dorsal wrist pain. Radiographs reveal sclerosis and fragmentation of the lunate, with an ulnar variance of minus 3 mm. Advanced imaging confirms stage IIIA Kienböck's disease without carpal collapse. Which of the following is the most appropriate surgical treatment?
Explanation
Question 62
In the evaluation of a displaced proximal humerus fracture, which of the following radiographic criteria is the most reliable predictor of subsequent avascular necrosis of the humeral head?
Explanation
Question 63
A 25-year-old male presents with persistent wrist pain 18 months after a fall onto an outstretched hand. Radiographs and subsequent MRI reveal a scaphoid proximal pole nonunion with signs of avascular necrosis, but no evidence of radiocarpal arthritis. What is the most appropriate surgical management?
Explanation
Question 64
During an anterior single-incision surgical repair of a distal biceps tendon rupture, the patient is at highest risk for injury to a specific peripheral nerve. Injury to this nerve typically results in which of the following clinical deficits?
Explanation
Question 65
A 32-year-old male sustains a closed, isolated, distal third spiral fracture of the humeral shaft (Holstein-Lewis fracture). On initial presentation, he is unable to actively extend his wrist or fingers. What is the most appropriate initial management?
Explanation
Question 66
A 28-year-old female undergoes open reduction and internal fixation of a displaced midshaft clavicle fracture. Postoperatively, she has normal motor function but complains of significant numbness over the anterior chest wall immediately inferior to the surgical incision. Injury to which nerve is the most likely cause?
Explanation
Question 67
A 72-year-old male presents with severe shoulder pain and an inability to actively elevate his arm above 40 degrees. Deltoid function is intact. Radiographs reveal advanced glenohumeral arthritis with severe superior migration of the humeral head (acetabularization of the coracoacromial arch).
What is the most appropriate definitive management?
Explanation
Question 68
A 30-year-old male with a severe traumatic brain injury sustains an elbow dislocation. He subsequently develops severe heterotopic ossification (HO) bridging the radiocapitellar joint, causing a rigid block to forearm rotation. When is the optimal time for surgical excision of the HO?
Explanation
Question 69
Six weeks after completing conservative management in a cast for a non-displaced distal radius fracture, a 55-year-old female experiences a sudden, painless inability to extend her thumb interphalangeal joint. What is the most appropriate surgical treatment?
Explanation
Question 70
A 45-year-old male presents with weakness in his intrinsic hand muscles and numbness in his small and ring fingers. Froment's sign is positive. Intraoperative exploration of the ulnar nerve at the elbow reveals compression by an anomalous muscle bridging the medial epicondyle and the olecranon. What is the name of this anatomical structure?
Explanation
Question 71
A 22-year-old overhead throwing athlete complains of deep shoulder pain during the late cocking phase of throwing. MR arthrography reveals a Type II Superior Labrum Anterior to Posterior (SLAP) tear. Which of the following best describes the specific anatomical pathology of a Type II SLAP lesion?
Explanation
Question 72
A 30-year-old male sustains a forced hyperabduction injury to his thumb metacarpophalangeal (MCP) joint while skiing. MRI confirms a complete tear of the ulnar collateral ligament (UCL) with the adductor aponeurosis interposed between the ruptured ligament and its anatomical insertion. What is this lesion called, and what is the indicated management?
Explanation
None
