Mastering Lateral Ankle Ligament Repair: A Modified Brostrom Intraoperative Guide

Key Takeaway
This masterclass guides fellows through Modified Brostrom and Brostrom-Evans lateral ankle ligament repair. We cover comprehensive anatomy, meticulous preoperative planning, precise patient positioning, and a granular step-by-step intraoperative execution from incision to closure. Detailed pearls, pitfalls, and postoperative management ensure optimal outcomes for chronic ankle instability, emphasizing technique and rationale as if you are scrubbed in alongside me.
Comprehensive Introduction and Patho-Epidemiology
Chronic lateral ankle instability (CLAI) represents a formidable challenge in orthopedic sports medicine, frequently demanding surgical intervention when conservative modalities are exhausted. The lateral ankle ligamentous complex is highly susceptible to injury, and while the majority of acute sprains resolve with functional rehabilitation, a significant epidemiological subset—ranging from 10% to 20% of patients—progresses to chronic, recurrent instability. This persistent instability is not merely a mechanical deficiency; it initiates a deleterious cascade of altered joint kinematics, asymmetrical cartilage loading, and subsequent early-onset osteoarthritis. As orthopedic surgeons, our objective is to meticulously restore the anatomical restraints of the lateral ankle, thereby reestablishing native joint congruence and mitigating the long-term sequelae of chronic microtrauma.


The pathogenesis of lateral ankle injuries is almost universally dictated by an inversion force applied to a plantarflexed ankle. In this specific biomechanical posture, the anterior talofibular ligament (ATFL) transitions from a relaxed state to becoming the primary restraint against talar inversion and anterior translation. Consequently, the ATFL is the inaugural structure to fail under supination-adduction stress. If the deforming force persists, the structural failure propagates posteriorly, compromising the calcaneofibular ligament (CFL). Ligamentous disruption typically manifests as midsubstance ruptures, though avulsions from the fibular origin or talar insertion are not uncommon, particularly in the pediatric or osteoporotic populations. The resulting laxity fundamentally alters the instantaneous center of rotation of the tibiotalar joint.


A critical component of our diagnostic and therapeutic algorithm is the differentiation between functional instability and mechanical instability. Functional instability is characterized by the patient's subjective perception of the ankle "giving way," often driven by proprioceptive deficits, peroneal weakness, and compromised neuromuscular control secondary to disrupted mechanoreceptors within the torn ligamentous tissue. Conversely, mechanical instability is defined by objective, supra-physiologic laxity measurable on clinical examination and stress radiography. The Modified Brostrom procedure, which we will detail exhaustively, is specifically designed to address mechanical instability by anatomically reconstructing the ATFL and CFL, while simultaneously providing secondary functional benefits through the restoration of tissue tension and subsequent proprioceptive feedback.


The evolution of lateral ankle reconstruction has heavily favored anatomic repair over non-anatomic tenodesis. Historically, procedures such as the Evans or Chrisman-Snook utilized the peroneus brevis tendon to recreate lateral stability, fundamentally altering hindfoot biomechanics and often resulting in restricted subtalar motion and accelerated degenerative changes. The Brostrom procedure, first described in 1966 and later modified by Gould in 1980 to include the advancement of the inferior extensor retinaculum (IER), has emerged as the unequivocal gold standard. This masterclass chapter will provide an intraoperative guide to executing this anatomic repair with precision, ensuring optimal outcomes for our demanding athletic and active patient cohorts.
Detailed Surgical Anatomy and Biomechanics
Ligamentous and Capsular Structures
A profound, three-dimensional comprehension of the lateral ankle anatomy is the absolute prerequisite for executing a successful Modified Brostrom repair. The lateral collateral ligamentous complex is composed of three distinct structures: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL, the most frequently compromised structure, originates from the anterior margin of the distal fibula, approximately 10 mm proximal to the fibular tip, and courses anteromedially to insert on the lateral articular facet of the talar neck. It is intimately blended with the anterior ankle joint capsule. In the setting of chronic instability, the ATFL often loses its distinct ligamentous architecture, presenting instead as a thickened, disorganized capsular expansion. Biomechanically, it restricts anterior translation of the talus within the mortise and acts as the primary check against inversion when the ankle is plantarflexed.


The calcaneofibular ligament (CFL) is a robust, cord-like structure originating from the anterior aspect of the distal fibular tip, just inferior to the ATFL origin. It courses posteroinferiorly to insert onto a small tubercle on the lateral wall of the calcaneus. Measuring approximately 4 to 6 mm in diameter and 13 to 20 mm in length, the CFL is unique as it spans both the tibiotalar and subtalar joints, thereby controlling inversion in both articulations. Crucially for the operating surgeon, the CFL lies extra-articular but is intimately associated with the medial wall of the peroneal tendon sheath. It is positioned directly deep to the peroneus longus and brevis tendons; thus, meticulous dissection is required to isolate the CFL without violating the peroneal sheath or inducing iatrogenic tendon injury.


The posterior talofibular ligament (PTFL) is the strongest of the lateral complex but is rarely injured except in the context of massive trauma or frank ankle dislocation. It originates from the posterior medial surface of the fibula and inserts onto the lateral tubercle of the posterior talar process. In standard CLAI, the PTFL remains intact and is not routinely addressed during a Brostrom procedure. Furthermore, the inferior extensor retinaculum (IER) plays a pivotal role in the Gould modification. The IER is a Y-shaped band of deep fascia; advancing its lateral root over the repaired ATFL and CFL provides a robust biological augmentation, limiting inversion, reducing anterior talar translation, and theoretically restoring local proprioceptive nerve endings to the lateral ankle.
Neurovascular and Osteological Considerations
Navigating the lateral ankle requires extreme vigilance regarding the local neurovascular topography. The superficial peroneal nerve (SPN) and the sural nerve are the primary structures at risk during surgical exposure. The SPN pierces the deep fascia of the lateral compartment approximately 10 to 12 cm proximal to the lateral malleolus, dividing into the medial and intermediate dorsal cutaneous nerves. The intermediate dorsal cutaneous branch frequently courses directly over the anterior aspect of the fibula and the ATFL footprint. Iatrogenic injury to this nerve via aggressive retraction or errant scalpel strokes can result in debilitating neuromas or complex regional pain syndrome (CRPS).


Posteriorly and inferiorly, the sural nerve travels alongside the small saphenous vein, passing posterior to the lateral malleolus. While typically posterior to the standard Brostrom incision, aberrant anatomy or overly aggressive posterior dissection—particularly when attempting to visualize the distal insertion of the CFL or when placing percutaneous anchors for internal bracing—can place the sural nerve in jeopardy. Meticulous blunt dissection and the use of precise, self-retaining retractors that avoid excessive pressure on the skin edges are mandatory to protect these vital sensory nerves.


From an osteological standpoint, the inherent stability of the ankle mortise is dictated by the trapezoidal shape of the talar dome. The anterior margin of the talus is significantly wider than its posterior margin. When the ankle is dorsiflexed, the wider anterior talus wedges tightly into the tibiofibular mortise, providing maximal bony stability. Conversely, in plantarflexion, the narrower posterior talus occupies the mortise, allowing for physiological rotational and translational play. This anatomical reality explains why the ankle is inherently vulnerable to inversion injuries when plantarflexed, and why our surgical repair must meticulously restore the soft-tissue restraints that govern this vulnerable position.
Exhaustive Indications and Contraindications
The decision to proceed with a Modified Brostrom repair must be predicated on a rigorous evaluation of the patient's clinical history, physical examination, and radiographic findings. The primary indication for surgical intervention is chronic, symptomatic lateral ankle instability that has proven refractory to a comprehensive, non-operative rehabilitation program lasting a minimum of 3 to 6 months. This conservative regimen must include aggressive peroneal strengthening, proprioceptive retraining, Achilles tendon stretching, and the use of functional bracing. Patients who continue to experience recurrent "giving way" episodes, persistent lateral-sided pain, and an inability to return to their desired level of athletic or occupational activity are prime candidates for anatomic reconstruction.


Surgical indications are further solidified by the presence of objective mechanical laxity. A positive anterior drawer test, demonstrating an absolute anterior translation of greater than 9-10 mm, or a side-to-side difference of greater than 5 mm compared to the contralateral asymptomatic ankle, strongly implicates ATFL incompetence. Similarly, a positive talar tilt test, evidenced by a talar tilt angle exceeding 10 degrees or demonstrating a 5-degree asymmetry, confirms concomitant CFL disruption. The presence of associated intra-articular pathology, such as osteochondral lesions of the talus (OCLs) or anterior tibiotalar impingement spurs, which are identified in up to 30-50% of chronic instability cases, also lowers the threshold for surgical intervention, as these can be addressed concurrently via ankle arthroscopy immediately preceding the open Brostrom repair.


While the Modified Brostrom is a highly successful procedure, it is not universally applicable, and recognizing absolute and relative contraindications is paramount to avoiding catastrophic failure. Absolute contraindications include active local or systemic infection, severe peripheral vascular disease precluding wound healing, and advanced, end-stage tibiotalar osteoarthritis where an arthrodesis or arthroplasty would be the definitive management. Furthermore, fixed osseous deformities, particularly an uncorrected varus hindfoot alignment, represent a critical biomechanical contraindication. A varus heel places continuous, excessive tension on the lateral ligamentous complex; performing a soft-tissue repair in the presence of a varus hindfoot will inevitably lead to premature stretching and failure of the reconstruction. Such patients require a concomitant lateralizing calcaneal osteotomy (e.g., Dwyer osteotomy).

Relative contraindications demand careful surgical judgment. Generalized ligamentous laxity, such as that seen in Ehlers-Danlos syndrome or Marfan syndrome, significantly compromises the quality of the native tissue available for repair. In these scenarios, a standard Brostrom may be insufficient, and the surgeon should strongly consider augmenting the repair with a robust allograft reconstruction or a synthetic internal brace. Similarly, patients with a body mass index (BMI) in the morbidly obese category or non-compliant patients who cannot adhere to strict postoperative non-weight-bearing protocols pose a high risk for early construct failure and require extensive preoperative counseling.
| Parameter | Indications for Modified Brostrom | Contraindications (Absolute & Relative) |
|---|---|---|
| Clinical History | Recurrent sprains, failure of >3-6 months PT | Non-compliance with postoperative rehab protocol |
| Physical Exam | Positive Anterior Drawer, Positive Talar Tilt | Generalized ligamentous laxity (Relative - requires augmentation) |
| Radiographic | >10° Talar tilt, >9mm Anterior translation | Severe tibiotalar osteoarthritis, fixed varus hindfoot |
| Associated Path | Concomitant OCLs or impingement (treat concurrently) | Active infection, severe peripheral neuropathy/vascular disease |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Pre-Operative Assessment
Meticulous preoperative planning begins with a highly detailed history and physical examination. The surgeon must ascertain the exact mechanism of the initial injury, the frequency of subsequent instability episodes, and the specific activities that provoke symptoms. Palpation must be systematic, assessing the ATFL, CFL, syndesmosis, medial and lateral malleoli, peroneal tendons, base of the fifth metatarsal, and the anterior process of the calcaneus to rule out concomitant fractures or tendinopathy. The anterior drawer and talar tilt tests are the gold standards for clinical assessment, ideally performed under fluoroscopy if the clinical exam is equivocal.


Radiographic evaluation must include weight-bearing anteroposterior, lateral, and mortise views of the ankle. These are scrutinized for joint space narrowing, loose bodies, marginal osteophytes, and subtle malalignment. Stress radiographs, while somewhat operator-dependent, provide quantifiable data regarding ligamentous incompetence. Magnetic Resonance Imaging (MRI) without contrast is routinely obtained to evaluate the integrity of the ATFL and CFL, though its primary utility often lies in detecting associated intra-articular pathology, such as osteochondral lesions of the talar dome, peroneal tendon tears, or loose bodies, which dictate the need for a concomitant diagnostic and therapeutic ankle arthroscopy.


Optimization of Patient Positioning
Intraoperative positioning is a critical, often underappreciated aspect of a successful lateral ankle reconstruction. Proper positioning dictates exposure, facilitates dynamic assessment of the repair, and minimizes the risk of iatrogenic nerve injury. The procedure is typically performed under general anesthesia, supplemented with a regional popliteal block for optimal postoperative pain control. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, though it is only inflated after exsanguination with an Esmarch bandage.

The patient is meticulously positioned in the lateral decubitus position, which affords unparalleled access to the lateral aspect of the ankle and hindfoot. The non-operative extremity must be carefully padded, particularly at the common peroneal nerve at the fibular head and the lateral malleolus, utilizing thick gel pads. An operative platform is constructed using folded blankets or a dedicated positioning device to elevate the operative leg, allowing the foot to clear the edge of the operating table for unrestricted manipulation.

A dynamic positioning strategy utilizing a sterile "bump" (typically composed of tightly folded surgical towels) is highly recommended. During the initial dissection, capsulotomy, and preparation of the fibular footprint, the bump is placed proximal to the ankle joint, under the distal tibia. This allows the foot to fall naturally into a varus and inverted position, maximizing the opening of the lateral gutter and placing the ATFL and CFL footprints under tension for easier identification. Conversely, during the critical phase of anchor placement, suture passing, and knot tying, the bump is repositioned distally, directly under the lateral border of the foot. This maneuver places the subtalar and tibiotalar joints into a slight valgus and everted posture, approximating the torn ligament ends to the fibula and removing tension from the repair, thereby ensuring a robust, non-strangulated fixation.

Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
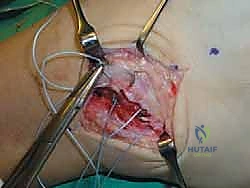
The surgical approach requires a delicate balance between adequate exposure and the preservation of soft tissue envelopes. A 4 to 6 cm curvilinear incision is made over the anterior border of the distal fibula, beginning approximately 2 cm proximal to the fibular tip and extending distally toward the sinus tarsi. This trajectory roughly parallels the course of the ATFL. The incision is carried sharply through the epidermis and dermis. Subcutaneous dissection must be performed with extreme caution, utilizing blunt spreading techniques with Stevens tenotomy scissors to identify and protect the branches of the superficial peroneal nerve dorsally and the sural nerve plantarly.


Once the superficial nerves are secured and protected with small Penrose drains or vessel loops, the dissection proceeds to the deep fascia. The inferior extensor retinaculum (IER) is identified as a distinct, obliquely oriented fascial band crossing the anterior aspect of the ankle. The lateral root of the IER is carefully mobilized and tagged with a non-absorbable traction suture; this structure will be crucial for the final Gould augmentation. Deep to the IER, the anterior joint capsule and the remnants of the ATFL are exposed. In chronic cases, the ATFL is often attenuated, presenting as a thickened scar mass rather than a discrete ligament.


Deep Dissection and Footprint Preparation
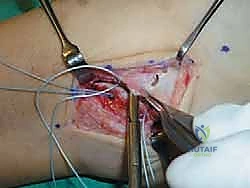
A vertical arthrotomy is performed approximately 2 to 3 mm anterior to the distal fibular margin, leaving a small cuff of tissue attached to the bone to facilitate later repair if suture anchors are not utilized (though modern techniques almost exclusively rely on anchors). The capsular flap, containing the ATFL, is sharply reflected anteriorly. The joint is inspected for any loose bodies, chondral flaps, or synovitis, which are debrided accordingly. Attention is then directed inferiorly to isolate the CFL. The peroneal tendon sheath is identified; the CFL lies immediately deep to the sheath. Meticulous dissection is required to separate the CFL from the sheath without violating the tendons.


The anatomic footprints of the ATFL and CFL on the anterior and inferior aspects of the distal fibula are then prepared. Using a curette, rongeur, or a high-speed motorized burr, the cortical bone at the anatomic origins is meticulously decorticated. The goal is to expose a bleeding, cancellous bone bed. This step is absolutely critical; it stimulates a robust healing response, allowing for fibroblastic proliferation and osteointegration of the repaired soft tissue directly to the fibula, maximizing the ultimate tensile strength of the reconstruction.


Suture Anchor Fixation and the Gould Modification
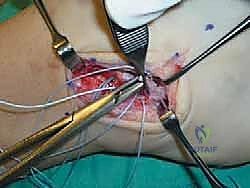
Fixation is achieved utilizing modern suture anchor technology. Typically, two double-loaded suture anchors (ranging from 2.5 mm to 3.5 mm in diameter, composed of bio-composite or PEEK material) are deployed. The first anchor is placed at the anatomic origin of the CFL on the inferior tip of the fibula. The second anchor is placed at the anatomic origin of the ATFL, approximately 10 to 15 mm proximal to the first anchor on the anterior fibular margin. The anchors must be inserted at an angle that bisects the fibula to ensure maximum pull-out strength and to avoid penetrating the articular surface of the lateral gutter.
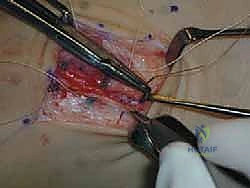

Using a free needle or a dedicated suture-passing device (such as a lasso or a crescent hook), the sutures are passed through the proximal stumps of the ATFL and CFL in a horizontal mattress or Krackow configuration. It is imperative to capture healthy, robust tissue, often requiring the surgeon to bite slightly distal into the ligamentous substance. Once all sutures are passed, the assistant repositions the bump to place the ankle in neutral dorsiflexion and slight eversion. This posture anatomically reduces the ligaments to the fibular footprint. The sutures are then tied sequentially, ensuring excellent tissue-to-bone apposition without over-constraining the joint.


The final, critical step is the Gould modification. The previously
Clinical & Radiographic Imaging Archive






















