Metatarsophalangeal Joint Arthroplasty: A Comprehensive Surgical Guide
Key Takeaway
Metatarsophalangeal (MTP) joint arthroplasty is a critical surgical intervention for severe forefoot deformities, including chronic dislocations and rigid hammer toes. By meticulously contouring the metatarsal head and utilizing precise intramedullary pinning, surgeons can restore functional alignment and alleviate pain. This guide details the biomechanical principles, step-by-step surgical techniques, and advanced alternatives like the Weil shortening osteotomy to optimize patient outcomes and minimize complications.
Comprehensive Introduction and Patho-Epidemiology
Metatarsophalangeal (MTP) joint arthroplasty represents a foundational, albeit highly complex, procedure in operative orthopaedics. It is primarily indicated for the correction of severe, rigid forefoot deformities that have proven refractory to conservative management. These deformities encompass a wide spectrum of pathology, including chronic MTP joint dislocations, advanced and rigid hammer toe deformities, and crossover toe syndromes. When conservative measures such as orthotic offloading, shoe modifications, and corticosteroid injections fail, the deformity typically becomes fixed. At this juncture, surgical intervention is absolutely required to decompress the joint, restore a functional and cosmetically acceptable alignment, and alleviate the debilitating plantar or dorsal forefoot pain that limits the patient's ambulatory capacity.
The primary goal of resection or contouring arthroplasty at the MTP joint is not necessarily to restore normal anatomical kinematics. In chronically contracted, dislocated, or severely arthritic joints, achieving native kinematics is often a biomechanical impossibility due to irreversible soft tissue contractures and cartilaginous degradation. Rather, the definitive surgical objective is to adequately decompress the articulation, allow for the concentric reduction of the proximal phalanx onto the metatarsal head, and restore a functional, pain-free arc of motion. A successful MTP joint arthroplasty should reliably restore 10 to 20 degrees of motion in an acceptable sagittal plane, ensuring the toe remains concentrically reduced on the metatarsal head without forceful impingement during the terminal stance phase of the gait cycle.

Clinical appearance of a severe hammer toe deformity with chronic dislocation of the metatarsophalangeal joint.
From an epidemiological standpoint, lesser MTP joint instability and subsequent dislocation disproportionately affect females, typically presenting in the fifth to seventh decades of life. The condition is frequently bilateral, though it may manifest asymmetrically depending on the patient's specific biomechanical foot type and occupational or footwear-related stressors. The second MTP joint is overwhelmingly the most commonly affected articulation, largely due to its unique anatomical position. It serves as the primary stabilizing strut of the forefoot during the propulsive phase of gait, subjecting it to immense sheer and axial loads. When the first ray is compromised—such as in the setting of severe hallux valgus or first tarsometatarsal hypermobility—transfer metatarsalgia ensues, shifting pathological forces directly onto the second MTP joint and accelerating the cascade of capsuloligamentous failure.

Preoperative radiographic evaluation demonstrating dorsal dislocation of the MTP joint.
The pathoanatomy of chronic lesser MTP joint dislocation is characterized by a progressive, predictable sequence of soft tissue failure. It typically initiates with the attenuation and ultimate rupture of the plantar plate and the collateral ligament complex. The plantar plate, a robust fibrocartilaginous structure, is the primary static restraint against dorsal subluxation of the proximal phalanx. As this structure fails, the intrinsic musculature (lumbricals and interossei) shifts dorsal to the axis of rotation, converting their normal plantarflexion force into a paradoxical dorsiflexion force. This is often exacerbated by a relatively long metatarsal (a positive metatarsal parabola) or a concomitant hallux valgus deformity, which mechanically crowds the lesser digits and dramatically increases sheer forces across the lesser MTP joints, culminating in rigid, irreducible dorsal dislocation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the forefoot is mandatory for the operating surgeon to execute an MTP joint arthroplasty successfully. The lesser MTP joints are condylar, biaxial diarthrodial joints that allow for flexion, extension, abduction, and adduction. The metatarsal head is uniquely shaped, being narrower dorsally than plantarly, which provides inherent bony stability during dorsiflexion (the close-packed position) but allows for greater laxity in plantarflexion. The plantar aspect of the metatarsal head features distinct plantar condyles separated by a central groove. These condyles act as a mechanical cam; during MTP joint dorsiflexion, they effectively lengthen the functional lever arm of the metatarsal, increasing tension on the plantar fascia and intrinsic musculature. Failure to address this cam effect during surgical resection is a primary cause of recurrent deformity.
The soft tissue envelope surrounding the MTP joint is an intricate network of static and dynamic stabilizers. The static stabilizers include the capsule, the collateral ligaments (proper and accessory), the plantar plate, and the deep transverse metatarsal ligament (DTML). The plantar plate is the single most critical stabilizing structure. It originates from the plantar metatarsal neck and inserts firmly onto the plantar base of the proximal phalanx. The DTML connects the adjacent plantar plates, creating a unified, load-sharing sling across the forefoot. The collateral ligaments originate from the dorsal-lateral aspects of the metatarsal head and fan out to insert onto the proximal phalanx and the margins of the plantar plate. In chronic dislocations, the plantar plate tears—most commonly at its distal insertion—and the collateral ligaments become severely contracted in a dorsally subluxated position.
Dynamically, the MTP joint is governed by the delicate balance between the extrinsic and intrinsic musculature. The extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) provide dorsal extension, while the flexor digitorum longus (FDL) and flexor digitorum brevis (FDB) provide plantar flexion. The intrinsic muscles, specifically the lumbricals and interossei, are critical for stabilizing the proximal phalanx against the metatarsal head during weight-bearing. In the presence of a plantar plate rupture, the proximal phalanx subluxates dorsally, altering the mechanical axis of the intrinsic muscles. They migrate dorsal to the center of rotation of the MTP joint, thereby exacerbating the dorsal contracture and creating an "intrinsic minus" functional state, characterized by MTP joint hyperextension and proximal interphalangeal (PIP) joint flexion (the classic hammer toe posture).
Biomechanically, the forefoot operates under the principles of the windlass mechanism, as famously described by Hicks. During the terminal stance phase of gait, dorsiflexion of the toes tightens the plantar fascia around the metatarsal heads, elevating the longitudinal arch and converting the foot into a rigid lever for propulsion. If an MTP joint is chronically dislocated, this mechanism is profoundly disrupted. The dislocated proximal phalanx can no longer engage the metatarsal head to tension the plantar aponeurosis effectively. Consequently, surgical reconstruction must not only realign the osseous structures but also restore the delicate tension-banding effect of the plantar soft tissues, ensuring that the metatarsal head can once again bear weight concentrically without driving the proximal phalanx into pathological dorsal impingement.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful MTP joint arthroplasty. The decision to proceed with operative intervention must be predicated on a thorough clinical evaluation, radiographic confirmation of structural pathology, and a documented failure of exhaustive conservative measures. Surgeons must weigh the severity of the deformity against the patient's physiological age, functional demands, vascular status, and capacity to adhere to strict postoperative rehabilitation protocols.
The primary indication for MTP joint contouring arthroplasty or shortening osteotomy is intractable metatarsalgia associated with a rigid, irreducible dorsal subluxation or frank dislocation of the MTP joint. Patients typically present with severe pain localized to the plantar aspect of the affected metatarsal head, often accompanied by dense, intractable plantar keratoses (IPKs). Additionally, dorsal ulcerations over the PIP joint due to shoe wear friction are common. Crossover toe deformity, where the second toe deviates medially and dorsally to override the hallux, is another definitive indication, particularly when the deformity has become fixed and cannot be passively reduced to a neutral alignment.
Conversely, absolute contraindications include active local or systemic infection, severe peripheral arterial disease (PAD) with an Ankle-Brachial Index (ABI) of less than 0.4, and an inadequate soft tissue envelope that would preclude primary wound closure. Relative contraindications include poorly controlled diabetes mellitus, profound peripheral neuropathy (such as Charcot neuroarthropathy), and heavy tobacco use, all of which exponentially increase the risk of delayed wound healing, nonunion, and catastrophic postoperative infection. In patients with severe systemic comorbidities, a more conservative approach or a minimalist soft-tissue release may be favored over extensive osseous resection and intramedullary pinning.
| Category | Specific Clinical Scenarios | Rationale / Clinical Context |
|---|---|---|
| Primary Indications | Rigid, chronic MTP joint dislocation | Joint is irreducible; requires osseous shortening and capsular release. |
| Intractable metatarsalgia with IPK | Plantar pressure must be relieved via metatarsal head elevation/resection. | |
| Severe, fixed crossover toe deformity | Medial/dorsal contractures require extensive release and realignment. | |
| Advanced hammer toe with dorsal ulceration | PIP joint contracture forces MTP extension; combined arthroplasty needed. | |
| Absolute Contraindications | Active osteomyelitis or cellulitis | High risk of deep space infection and hardware seeding. |
| Critical limb ischemia (ABI < 0.4) | Surgical dissection will inevitably lead to ischemic necrosis of the digit. | |
| Inadequate dorsal soft tissue envelope | High probability of wound dehiscence and exposed osseous structures. | |
| Relative Contraindications | Poorly controlled Diabetes (HbA1c > 8.0) | Impaired leukocyte function and microvascular disease delay healing. |
| Advanced Charcot Neuroarthropathy | Loss of protective sensation increases risk of hardware failure and breakdown. | |
| Active heavy smoking (>1 pack/day) | Nicotine-induced vasoconstriction drastically increases nonunion/necrosis risk. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is critical to anticipate anatomical challenges and select the appropriate surgical techniques. The clinical assessment must begin with a rigorous evaluation of the patient's neurovascular status. Palpation of the dorsalis pedis and posterior tibial pulses is mandatory. If pulses are diminished or absent, non-invasive vascular studies (ABI, toe pressures, or arterial Doppler ultrasound) must be obtained. Surgical correction of a chronically dislocated toe requires extensive soft tissue dissection, capsular release, and osseous shortening, which places significant tension on the delicate digital neurovascular bundles. A patient who requires extensive dissection on adjacent joints of the same toe must be explicitly advised preoperatively that loss of the toe from vascular compromise is a known, albeit rare, complication.
Radiographic templating is the next critical phase of preoperative preparation. Weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory. The AP view is utilized to assess the degree of medial or lateral deviation, the presence of degenerative joint disease, and, most importantly, the metatarsal parabola. The relative lengths of the metatarsals must be meticulously measured. A second metatarsal that projects significantly distal to the first and third metatarsals is highly predisposed to plantar plate failure and will almost certainly require a shortening procedure (such as a Weil osteotomy or aggressive contouring arthroplasty) to achieve a tension-free reduction. The lateral view is essential to quantify the degree of dorsal subluxation or frank dislocation of the proximal phalanx base relative to the metatarsal head.

Planned operative incision over the affected MTP and PIP joints.
On the day of surgery, meticulous attention to patient positioning and operating room setup facilitates a smooth procedure. The patient is placed in the supine position on a standard operating table. A small bump is often placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral, strictly vertical position, which greatly aids in assessing rotational alignment during pinning. A pneumatic tourniquet is typically utilized to ensure a bloodless surgical field. The choice of tourniquet location—thigh, calf, or ankle—depends on surgeon preference and the patient's vascular status; an ankle or calf tourniquet is generally preferred for isolated forefoot procedures to minimize systemic ischemic burden.
The foot is prepped and draped in a standard sterile fashion, ensuring exposure from the distal third of the tibia down to the tips of the toes. The surgeon must have unimpeded access to the dorsal and plantar aspects of the foot to manipulate the digits and assess the reduction dynamically. Intraoperative fluoroscopy (C-arm) must be positioned to allow for orthogonal views of the forefoot without compromising the sterile field. The surgeon should confirm that all necessary hardware, including various sizes of Kirschner wires (0.045-inch and 0.062-inch), wire drivers, bone rongeurs, and small joint sagittal saws, are readily available on the sterile back table prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Soft Tissue Releases
The surgical approach begins with precise incision planning. A dorsal longitudinal incision is most commonly utilized, centered over the affected MTP joint and extending distally over the PIP joint if concurrent correction of a hammer toe is required. In cases of severe dorsal skin contracture, an elliptical incision may be employed to excise redundant skin or facilitate a V-Y advancement, though this is less common. Dissection is carried down through the subcutaneous tissues, taking meticulous care to identify and retract the dorsal cutaneous nerve branches and delicate dorsal venous plexus.
The extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons are identified. In rigid deformities, these tendons are invariably contracted. A Z-lengthening of the EDL is performed, allowing the tendon ends to be retracted proximally and distally to expose the underlying dorsal capsule. The EDB tendon is typically tenotomized and allowed to retract. A thorough dorsal capsulotomy is then executed. The collateral ligaments, which are often severely contracted and tether the proximal phalanx in its dorsally dislocated position, must be meticulously released from their metatarsal origins. A McGlamry elevator or a small curved osteotome can be swept plantarly to release any remaining adhesions between the plantar plate and the metatarsal head, fully mobilizing the base of the proximal phalanx.
Proximal Interphalangeal (PIP) Joint Correction
In the presence of moderate or severe hammer toe deformities, the MTP joint cannot be accurately assessed, reduced, or pinned until the PIP joint contracture is fully addressed. The PIP joint is exposed through the distal extent of the same dorsal incision. The extensor apparatus is split longitudinally or tenotomized transversely. The collateral ligaments of the PIP joint are released, allowing the joint to be "shotgunned" (hyperextended) to expose the articular surfaces.

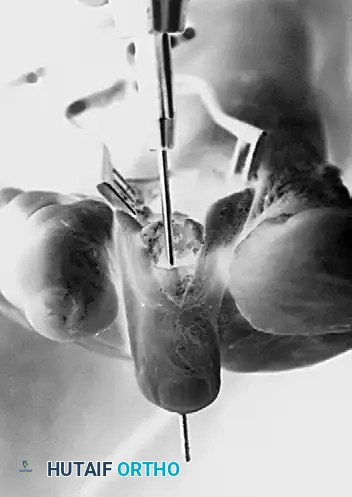
Exposure after resection of the head and neck of the proximal phalanx, dorsal capsulotomy at the MTP joint, and extensor tendon lengthening.
A sagittal saw or bone rongeur is used to resect the head and neck of the proximal phalanx. The amount of bone removed is dictated by the severity of the contracture; enough bone must be resected to allow the PIP joint to rest in a neutral, extended position without soft tissue tension. The articular cartilage at the base of the middle phalanx may be fenestrated or lightly planed to promote eventual fibrous or bony ankylosis, depending on whether an arthrodesis or a resection arthroplasty is desired at the PIP level. Once the PIP joint is decompressed, the surgeon can return their attention to the MTP joint.
Metatarsal Head Resection and Contouring
To achieve concentric reduction of a chronically dislocated MTP joint, the metatarsal head must be aggressively decompressed. Attempting to reduce the joint without adequate osseous shortening will result in extreme tension on the neurovascular bundles and inevitable recurrence of the deformity. Using a microsagittal saw, the distal 3 to 4 mm of the articular surface of the metatarsal head is resected perpendicular to the long axis of the metatarsal shaft.

Resection of the distal portion of the metatarsal head.
Equally critical to the distal resection is the execution of a comprehensive plantar condylectomy. The plantar condyles of the metatarsal head act as a mechanical cam; failing to resect them will maintain tension on the intrinsic musculature and prevent adequate decompression during dorsiflexion. The saw blade is directed obliquely from dorsal-distal to plantar-proximal to excise the prominent plantar condyles, effectively flattening the plantar aspect of the metatarsal head.

Plantar condylectomy of the metatarsal head to eliminate the cam effect and decompress the joint.
Surgical Pitfall: A word of caution concerning palpable grating of the arthroplasty: If, after contouring the metatarsal head, the MTP joint still feels tight with the proximal phalanx grating on the contoured bone during passive range of motion, more bone must be removed until the grating stops. You should be able to passively move the toe 30 to 40 degrees in both flexion and extension without forceful impingement or the need for excessive manual pressure.
Intramedullary Pinning Technique
Once adequate osseous decompression and soft tissue balancing are achieved, the joint must be stabilized with an intramedullary pin (Kirschner wire) for 3 to 4 weeks. This temporary fixation allows the periarticular soft tissues to heal in the anatomically corrected position, forming a robust fibrous pseudocapsule.
Antegrade Pinning:
The surgeon selects a 0.045-inch or 0.062-inch Kirschner wire, depending on the canal diameter of the patient's phalanges. The K-wire is inserted antegrade through the remaining shaft of the proximal phalanx. It is driven distally across the resected PIP joint, through the medullary canal of the middle phalanx, and out through the distal phalanx. The pin should exit the skin exactly in the midline of the toe tip, approximately 2 to 3 mm plantar to the nail bed, to avoid nail matrix injury.
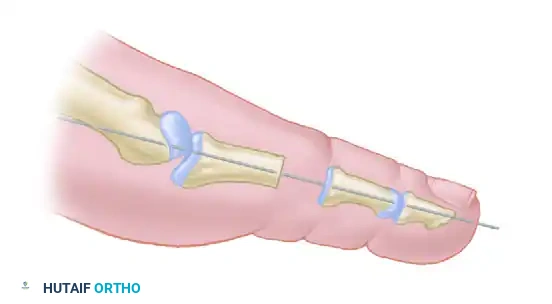
Diagrammatic representation: Pin inserted antegrade through the middle and distal phalanges.

Intraoperative view of antegrade pinning through the proximal interphalangeal joint.
Retrograde Pinning:
Once the pin has exited the distal tip of the toe, the wire driver is moved to the distal end of the pin. The drill is reversed, and the pin is driven retrograde until the proximal tip is flush with the resected articular surface of the proximal phalanx.
Technical Tip: Finding the medullary canal of the proximal phalanx can occasionally be difficult, particularly in sclerotic or severely osteopenic bone. Take a free 0.062-inch K-wire or a small straight hemostat to manually open the canal prior to passing the definitive pin. This creates a pilot track, allowing the definitive K-wire to find its way without inadvertently exiting the dorsal or plantar cortex before reaching the proximal articular surface.
Diagrammatic representation: Pin reversed and driven retrograde through the remaining portion of the shaft of the phalanx and across the MTP joint.
The surgeon then stands at the head of the operating table, holding the toe concentrically reduced at the MTP joint. Viewing the toe longitudinally (as the patient would see it) is crucial to ensure perfect rotational and mediolateral alignment. While the surgeon holds the reduction, an assistant drives the pin retrograde across the MTP joint and into the medullary canal of the metatarsal shaft.

Intraoperative view of retrograde pinning through the proximal phalanx across the metatarsophalangeal joint.
Critical Positioning Parameters:
* Pin the MTP joint in 10 degrees of extension relative to the metatarsal shaft. Pinning in neutral or flexion will result in a toe that catches on the ground during the swing phase of gait.
* The ankle must be held at 90 degrees (neutral dorsiflexion) during pinning. This accurately recreates the tension on the extensor apparatus that will be present during weight-bearing.
* Ensure the joint is perfectly reduced in the mediolateral plane to prevent crossover recurrence.
The Weil Shortening Osteotomy (Advanced Alternative)
As an alternative to contouring or resection arthroplasty of the metatarsal head, a shortening osteotomy of the metatarsal neck and head region—specifically the Weil osteotomy—is highly effective for correcting a dislocated MTP joint while preserving the native articular cartilage.
The Weil osteotomy is particularly useful if the length of the involved metatarsal is excessively long in relation to the adjacent rays. Its biomechanical advantages include longitudinal decompression of the joint and the alteration of the axis of the interosseous muscles, converting them from pathological dorsal subluxators back into functional plantarflexors, thereby restoring dynamic joint stability.

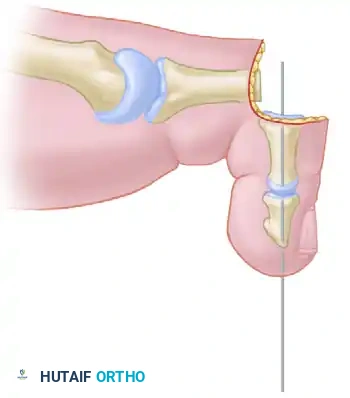
Diagram A: Preoperative state of a dislocated MTP joint prior to Weil osteotomy.
The osteotomy is performed intra-articularly. Using a microsagittal saw, the cut is initiated at the dorsal margin of the articular cartilage and directed proximally and plantarly. The trajectory of the cut should be perfectly parallel to the weight-bearing surface of the foot (the plantar aspect of the heel and the metatarsal heads).
Once the cut is complete, the capital fragment (the metatarsal head) is translated proximally along the osteotomy plane to achieve the desired amount of shortening (typically 3 to 5 mm, depending on preoperative templating).

Diagram B: Proximal displacement of the metatarsal head fragment, decompressing the joint.
The fragment is temporarily fixed with a K-wire. Definitively, it is secured with one or two small fragment snap-off screws (e.g., 2.0 mm or 2.7 mm). Following fixation, the proximal translation leaves a prominent overhanging dorsal lip of the proximal metatarsal shaft. This dorsal overhang must be resected flush with the articular fragment using a saw or rongeur to prevent severe dorsal impingement during MTP joint dorsiflexion.

Diagram C: Final construct after resection of the distal tip of the dorsal fragment.
Soft Tissue Balancing, Closure, and Vascular Assessment
Following osseous fixation (whether via arthroplasty or osteotomy), the tourniquet is deflated to allow for meticulous hemostasis and immediate vascular assessment. The Extensor Digitorum Longus (EDL) tendon is then addressed. With the ankle joint
Clinical & Radiographic Imaging Archive