
Introduction and Epidemiology
The burden of revision total knee arthroplasty (rTKA) continues to rise exponentially, driven by the increasing volume of primary arthroplasties performed globally, expanding indications in younger, more active patients, and increased life expectancy. While primary total knee arthroplasty demonstrates excellent long-term survivorship, failure can occur through a variety of mechanisms, necessitating complex reconstructive procedures. The most common mechanisms of failure vary temporally; early failures (within two years) are frequently attributed to periprosthetic joint infection (PJI) or mechanical instability, whereas late failures are typically secondary to aseptic loosening, polyethylene wear, and osteolysis.
Addressing instability, loosening, and wear in the revision setting requires a profound understanding of joint biomechanics, meticulous preoperative planning, and mastery of modular implant systems. The surgeon must navigate compromised soft tissue envelopes, massive cavitary and segmental bone defects, and altered kinematics.
Clinical Vignette and Patient Presentation
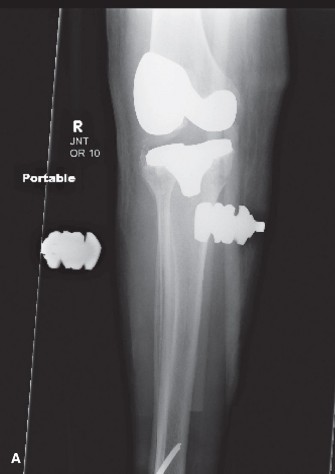
We are presenting a complex case of a 58-year-old male presenting with chronic, debilitating left knee pain, progressive instability, and recurrent effusions, 4 years following a primary total knee arthroplasty (TKA). The patient initially underwent TKA for severe tricompartmental osteoarthritis secondary to a remote history of tibial plateau fracture requiring ORIF 20 years prior. The initial TKA was performed at an outside institution using a posterior-stabilized (PS) design.
His post-operative course after the primary TKA was complicated by persistent discomfort, which was initially attributed to the normal recovery process. However, over the past two years, his pain significantly worsened, described as a dull ache at rest, intensifying with activity and weight-bearing. He reports mechanical symptoms including clunking and giving way, particularly when ambulating on uneven surfaces or descending stairs. He has experienced multiple falls due to perceived knee instability, necessitating the use of a cane for ambulation. The pain is consistently rated 7-8/10 on the Visual Analog Scale (VAS) despite regular use of NSAIDs and opioid analgesics. He reports daily swelling that temporarily improves with rest and elevation but never fully resolves. There has been no reported fever, chills, or systemic signs of infection, although he notes generalized fatigue.
His medical comorbidities include well-controlled Type 2 Diabetes Mellitus (HbA1c 6.8%), hypertension, and a body mass index (BMI) of 34 kg/m². He is an active smoker with a 30-pack-year history, though he claims to be reducing intake. Surgical history includes the aforementioned tibial plateau ORIF and primary left TKA. Allergies include penicillin. He works as an accountant, requiring prolonged sitting but also moderate ambulation. His functional limitations are severe, preventing him from performing routine activities of daily living and significantly impacting his quality of life. Previous non-operative management attempts by referring physicians included cortisone injections, aspiration of effusions (without diagnostic workup on fluid), and extensive physical therapy, all providing only transient or minimal relief.
On general inspection, the patient ambulates with a significant antalgic gait, exhibiting a noticeable varus thrust during the stance phase of the left knee. He uses a single point cane contralaterally. The left knee demonstrates chronic moderate effusion, with visible quadriceps atrophy compared to the contralateral limb. The surgical incision scar is well-healed, non-erythematous, and without signs of dehiscence, sinus tracts, or warmth. No superficial breakdown or signs of acute infection are noted.
Palpation reveals moderate warmth over the medial and lateral joint lines, consistent with chronic inflammation. A significant, firm effusion is palpable, but no discrete fluctuance is identified. Tenderness is elicited diffusely around the joint, particularly medially and laterally, and along the patellofemoral articulation. The posterior aspect of the knee is soft and non-tender.
Range of motion (ROM) of the left knee reveals a painful arc from 5 degrees of flexion contracture to 85 degrees of active flexion. Passive flexion achieves 90 degrees with significant end-range pain. Patellar tracking is notable for lateral tilt and mild subluxation with knee flexion, consistent with patellofemoral malalignment.
Ligamentous stability testing demonstrates significant findings. Varus stress testing at 0 degrees and 30 degrees of flexion elicits substantial laxity, graded as 2+ with a firm but indistinct endpoint, suggesting medial collateral ligament (MCL) insufficiency or elongation. Valgus stress testing reveals mild laxity at 0 degrees, but 1+ laxity at 30 degrees, suggesting some lateral collateral ligament (LCL) compromise or laxity, possibly secondary to the overall instability. Anterior-posterior stability testing reveals significant sagittal plane translation, indicating gross incompetence of the posterior-stabilized cam-post mechanism and chronic attenuation of the secondary capsular restraints, consistent with profound global instability and likely aseptic loosening.
Surgical Anatomy and Biomechanics
Successful revision arthroplasty hinges on the restoration of normal knee kinematics, which requires precise management of the joint line, gap balancing, and appropriate constraint selection. The anatomical structures of the knee are frequently distorted by previous surgery, osteolysis, and heterotopic ossification.
Joint Line Restoration
The native joint line sits approximately 10 to 15 millimeters proximal to the fibular head and 25 to 30 millimeters distal to the medial epicondyle. In the revision setting, the joint line is frequently elevated due to distal femoral bone loss and the use of thicker tibial polyethylene inserts to compensate for flexion instability. Joint line elevation alters the kinematics of the patellofemoral joint, leading to patella baja, increased patellofemoral contact forces, anterior knee pain, and restricted flexion. Restoration of the joint line to its anatomical position is critical and often requires the use of distal femoral augments.
The Constraint Ladder
Biomechanically, the surgeon must step up the "constraint ladder" only as far as necessary to achieve stability without transferring excessive stress to the implant-bone interface.
* Cruciate Retaining and Posterior Stabilized designs rely on an intact collateral ligamentous envelope.
* Constrained Condylar Knee systems feature a taller, wider post that engages a deeper femoral box, providing varus-valgus and rotational stability in the setting of collateral ligament attenuation, provided the epicondylar attachments remain functional.
* Rotating Hinge Knee prostheses provide linked constraint and are indicated for global instability, severe bone loss precluding collateral ligament function, or massive extensor mechanism deficiency.
Bone Loss Classification
Understanding bone loss is paramount. The Anderson Orthopaedic Research Institute classification remains the standard:
* Type 1: Intact metaphyseal bone with minor cavitary defects.
* Type 2: Damaged metaphyseal bone requiring augmentation (2A involves one condyle/plateau; 2B involves both).
* Type 3: Deficient metaphyseal segment compromising major component fixation, necessitating diaphyseal engaging stems, metaphyseal cones, or sleeves.
Indications and Contraindications
The decision to proceed with revision TKA must be based on a clear identification of the failure mechanism. Unexplained pain is a strict contraindication to revision surgery, as outcomes in these scenarios are universally poor.
Diagnostic Criteria for Revision
Indications for revision encompass septic and aseptic etiologies. Aseptic loosening presents with progressive radiolucent lines, component migration, or subsidence. Instability can be classified into extension, flexion, mid-flexion, or global instability, each requiring specific biomechanical corrections. Polyethylene wear and osteolysis may present asymptomatically on radiographs or with catastrophic component failure.
| Indication Category | Operative Indications | Non Operative Management |
|---|---|---|
| Aseptic Loosening | Progressive radiolucent lines >2mm in multiple zones, component subsidence, mechanical symptoms | Asymptomatic non-progressive radiolucencies, medically unfit patients |
| Instability | Global instability, severe flexion instability causing falls, failure of conservative bracing | Mild mid-flexion instability managed with bracing, non-ambulatory status |
| Periprosthetic Infection | Acute PJI (DAIR protocol), Chronic PJI (Two-stage or single-stage exchange depending on host) | Suppressive antibiotics in patients with absolute contraindications to surgery |
| Wear and Osteolysis | Impending pathologic fracture, massive cavitary defects, eccentric wear causing malalignment | Small, stable osteolytic lesions in low-demand patients (close radiographic monitoring) |
| Periprosthetic Fracture | Loose components, severe displacement, failure of conservative management | Stable fracture with well-fixed components (manage with ORIF or casting) |
Absolute and Relative Contraindications
Absolute contraindications include active systemic bacteremia (unless addressing the joint as the source), severe peripheral vascular disease precluding safe tourniquet use or wound healing, and a non-functioning extensor mechanism in a patient who is not a candidate for reconstruction or arthrodesis. Relative contraindications encompass severe medical comorbidities (e.g., recent myocardial infarction), active smoking (which significantly increases the risk of wound complications and infection), and morbid obesity.
Pre Operative Planning and Patient Positioning
Preoperative planning is the most critical phase of revision arthroplasty. The surgeon must anticipate bone defects, component extraction difficulties, and the need for specialized implants.
Ruling Out Infection
Every painful TKA must be considered infected until proven otherwise. The diagnostic algorithm begins with serum erythrocyte sedimentation rate and C-reactive protein. If elevated, or if clinical suspicion is high despite normal markers, a joint aspiration is mandatory. Synovial fluid should be analyzed for cell count, differential, and aerobic, anaerobic, and fungal cultures. The 2018 International Consensus Meeting criteria for PJI should be strictly applied. In equivocal cases, synovial alpha-defensin or next-generation sequencing may be utilized.
Radiographic Evaluation and Templating
A comprehensive radiographic series includes weight-bearing anteroposterior, lateral, Merchant, and full-length standing lower extremity radiographs. The full-length view is essential for assessing mechanical alignment and identifying extra-articular deformities or retained hardware (such as the prior tibial plateau ORIF plates in our vignette patient). Computed Tomography is highly recommended to quantify osteolysis, assess component rotation, and plan for metaphyseal fixation (cones or sleeves).
Templating determines the size of the diaphyseal stems, the required offset to achieve optimal intramedullary canal fill while maintaining appropriate component position, and the anticipated size of augments.
Patient Optimization and Positioning
Optimization of modifiable risk factors is mandatory. For the patient in our vignette, smoking cessation counseling and strict glycemic control are required prior to elective revision.
The patient is positioned supine on a radiolucent operating table. A high thigh tourniquet is applied but typically inflated only for cementation to minimize ischemic time, unless visualization is severely compromised. A lateral post or leg holder is utilized to allow stable positioning during hyperflexion and rigorous stress testing. The previous surgical incision should be utilized; if multiple parallel incisions exist, the most lateral usable incision is chosen to preserve the vascular supply to the anterior skin flap.
Detailed Surgical Approach and Technique
The surgical technique in rTKA is a highly orchestrated procedure requiring meticulous tissue handling, strategic component extraction, and precise biomechanical reconstruction.
Surgical Exposure and Extensile Approaches
The standard medial parapatellar arthrotomy is utilized initially. Due to scar tissue and altered mechanics, the extensor mechanism is often contracted. The surgeon must avoid avulsion of the patellar tendon at all costs. If exposure is inadequate or patellar eversion places excessive tension on the tibial tubercle, extensile measures must be employed.
A quadriceps snip is the first-line extensile approach, involving an oblique incision directed superolaterally through the rectus femoris tendon. It requires no alteration in postoperative rehabilitation. If exposure remains insufficient, a tibial tubercle osteotomy (TTO) is performed. The TTO provides exceptional exposure of the tibial metaphysis, facilitates extraction of well-fixed tibial stems, and allows for distal and medial advancement of the extensor mechanism if patella alta or maltracking is present. The osteotomy must be at least 6 to 8 centimeters in length to ensure adequate surface area for healing and is repaired with cerclage wires or screws.
Component Extraction
Extraction must prioritize the preservation of remaining bone stock. The interface between the implant and bone or cement is systematically disrupted. For cemented components, flexible osteotomes, oscillating saws with narrow blades, and ultrasonic cement removal tools are utilized. For cementless, porous-coated implants, specialized extraction devices, such as Gigli saws or offset osteotomes, are necessary to break the biologic fixation.
The femoral component is addressed by disrupting the distal, chamfer, and anterior interfaces. The tibial component often requires disruption of the metaphyseal keel or stem. If a well-fixed diaphyseal stem is present, a controlled anterior cortical window or TTO may be required to disimpact the implant without causing a catastrophic periprosthetic fracture.

Debridement and Defect Management
Following extraction, meticulous debridement of all particulate debris, pseudocapsule, and osteolytic membranes is performed. Tissue samples from multiple distinct intra-articular sites must be sent for permanent histologic sectioning and microbiological culture to rule out occult infection.
Management of bone defects dictates the stability of the final construct.
* Cavitary defects (AORI Type 1 and 2) can be managed with morselized allograft or cement if small.
* Segmental defects (AORI Type 2) require modular metal augments (distal femoral, posterior condylar, or tibial block augments).
* Massive cavitary or uncontained defects (AORI Type 3) necessitate highly porous titanium metaphyseal cones or stepped sleeves. These devices provide immediate rigid biologic fixation in the metaphysis, offloading the diaphyseal stem and the joint line reconstruction.
Reconstruction and Gap Balancing
The reconstruction phase typically follows a specific sequence, often beginning with the tibia to establish a stable platform.
- Tibial Preparation: The tibial canal is reamed to accommodate a diaphyseal engaging stem. The stem provides alignment and offloads the compromised metaphysis. Offset stems may be required to optimize tibial plateau coverage without causing cortical impingement.
- Femoral Preparation and Joint Line Restoration: The femoral canal is reamed. The distal femoral joint line is established using distal augments based on preoperative templating and intraoperative landmarks (e.g., medial epicondyle).
- Gap Balancing: This is the crux of a stable revision. The flexion gap is dictated by the anteroposterior dimension of the femoral component and posterior augments. The extension gap is dictated by the distal femoral resection and distal augments.
- If the flexion gap is loose and the extension gap is balanced, the femoral component size must be increased, or posterior augments added.
- If the extension gap is loose and the flexion gap is balanced, distal femoral augments are added.
- If both gaps are loose, a thicker tibial polyethylene insert is utilized.
- Constraint Selection: Once the gaps are balanced, trial components are inserted, and stability is assessed. If the collateral ligaments are incompetent despite gap balancing, a Constrained Condylar Knee (CCK) insert is chosen. If the epicondylar axis is compromised or global instability persists, the surgeon must escalate to a rotating hinge construct.
Component Fixation
Modern revision philosophy favors hybrid fixation: cementless diaphyseal engaging stems combined with cemented metaphyseal and articular surfaces. This approach provides immediate rigid fixation via the stem while sealing the joint space from particulate debris with cement. Highly porous cones or sleeves, if used, are impacted with a press-fit technique, and the definitive implants are cemented into the cones.
Complications and Management
Revision TKA is fraught with potential complications, demanding rigorous intraoperative vigilance and aggressive postoperative management.
| Complication | Estimated Incidence | Salvage and Management Strategies |
|---|---|---|
| Periprosthetic Joint Infection | 3% - 10% | Two-stage exchange arthroplasty with antibiotic spacer; suppressive antibiotics for poor operative candidates. |
| Extensor Mechanism Disruption | 1% - 5% | Primary repair with synthetic mesh augmentation (Marlex mesh); extensor mechanism allograft reconstruction; gastrocnemius flap for soft tissue coverage. |
| Periprosthetic Fracture | 2% - 6% | Intraoperative: Bypass fracture with longer stem, cerclage wiring. Postoperative: ORIF with locking plates or revision to distal femoral replacement. |
| Aseptic Loosening / Subsidence | 4% - 8% | Re-revision with enhanced metaphyseal fixation (cones/sleeves) and longer diaphyseal stems; optimization of bone quality. |
| Postoperative Stiffness | 5% - 12% | Aggressive physical therapy; manipulation under anesthesia (within 6-12 weeks); arthroscopic or open lysis of adhesions. |
| Wound Necrosis / Dehiscence | 2% - 5% | Negative pressure wound therapy; early plastic surgery consultation for local or free muscle flaps (e.g., medial gastrocnemius flap). |
Managing Extensor Mechanism Failure
Extensor mechanism disruption is a catastrophic complication. Direct repair is universally prone to failure. Current gold standards involve reconstruction using synthetic mesh (e.g., Marlex mesh) or a full extensor mechanism allograft (tibial tubercle, patellar tendon, patella, and quadriceps tendon). The mesh technique provides a scaffold for host tissue ingrowth and requires strict postoperative immobilization in full extension for 6 to 8 weeks to allow for biologic incorporation.
Post Operative Rehabilitation Protocols
Rehabilitation following complex rTKA must be tailored to the specific surgical interventions performed, particularly regarding the status of the extensor mechanism and the method of component fixation.
Immediate Postoperative Phase (Weeks 0-2)
The primary goals are pain control, edema management, prevention of deep vein thrombosis (DVT), and early mobilization.
* Weight Bearing: If hybrid fixation with diaphyseal stems and metaphyseal cones is achieved, patients are generally allowed weight-bearing as tolerated (WBAT) with an assistive device. If a tibial tubercle osteotomy was performed, weight-bearing may be restricted to toe-touch (TTWB) or partial weight-bearing for 4 to 6 weeks.
* Range of Motion: Continuous passive motion (CPM) is rarely used today. Active and active-assisted ROM exercises are initiated immediately. If an extensor mechanism reconstruction or quadriceps snip was required, active knee extension may be delayed or restricted to a specific arc of motion.
* DVT Prophylaxis: Risk stratification dictates the chemoprophylactic agent, typically aspirin, low-molecular-weight heparin, or direct oral anticoagulants, administered for 14 to 35 days.
Intermediate Phase (Weeks 2-6)
Focus shifts to restoring functional mobility, improving quadriceps strength, and achieving full extension. Flexion goals are typically 90 degrees by week 4 and 110 degrees by week 6. Modalities such as neuromuscular electrical stimulation (NMES) may be utilized to overcome quadriceps arthrogenic muscle inhibition.
Late Phase (Weeks 6-12 and Beyond)
Progression to closed kinetic chain exercises, proprioceptive training, and normalization of gait mechanics. Patients are weaned from assistive devices as quadriceps control normalizes. Maximum medical improvement following a complex revision may take up to 12 to 18 months, and patients must be counseled appropriately regarding these expectations.
Summary of Key Literature and Guidelines
The academic landscape of revision total knee arthroplasty is guided by robust clinical literature and consensus statements.
- Diagnosis of PJI: The Musculoskeletal Infection Society (MSIS) and the International Consensus Meeting (ICM) guidelines provide the definitive algorithmic approach to diagnosing periprosthetic joint infection, emphasizing the role of synovial fluid analysis over isolated serum markers.
- Bone Defect Management: Engh's original work on the Anderson Orthopaedic Research Institute (AORI) classification remains the foundation for managing bone loss. Recent literature heavily supports the transition from massive structural allografts to highly porous titanium metaphyseal cones and sleeves, demonstrating superior mid-to-long-term survivorship and biologic integration.
- Joint Line and Kinematics: Morgan-Jones et al. have extensively detailed the critical nature of joint line restoration and its direct correlation with postoperative functional scores and patellofemoral mechanics. Their work underscores the necessity of referencing bony landmarks rather than relying solely on soft tissue tensioning during revision surgery.
- Constraint Selection: The American Academy of Orthopaedic Surgeons (AAOS) appropriate use criteria emphasize utilizing the least constrained implant necessary to achieve stability. The literature demonstrates that over-constraining the knee significantly increases the risk of aseptic loosening and mechanical failure at the stem-bone interface.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding painful-total-knee-replacement