Revision Total Knee Arthroplasty with Extensor Mechanism Reconstruction: An Achilles Allograft Masterclass

Key Takeaway
Welcome to the OR, fellows. Today, we tackle a challenging revision total knee arthroplasty with patellar tendon rupture. This masterclass details the preoperative planning, comprehensive anatomy, and meticulous intraoperative steps for Achilles allograft reconstruction. We'll cover primary repair augmentation, bone block fixation, precise allograft tensioning, and crucial postoperative rehabilitation, emphasizing critical pearls and pitfalls for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we confront one of the most formidable and devastating challenges encountered in the realm of adult reconstruction: a revision total knee arthroplasty (TKA) complicated by a complete, catastrophic disruption of the extensor mechanism. Specifically, we are addressing a complete patellar tendon rupture in the setting of a well-fixed, albeit mechanically demanding, revision arthroplasty construct. The loss of extensor continuity transforms a potentially functional, pain-free arthroplasty into a profoundly disabling condition, rendering the patient unable to ambulate without severe instability and reliance on assistive devices. The prevalence of this complication is historically reported to range from 0.17% to 2.5%, a seemingly small percentage that nonetheless represents a massive absolute number of patients given the exponentially rising volume of primary and revision TKA procedures performed globally.
When a patient presents with a suspected patellar tendon rupture following TKA, the clinical picture is rarely subtle. The classic presentation includes an acute onset of severe, localized anterior knee pain, frequently accompanied by an audible "pop" or tearing sensation during a seemingly benign eccentric loading event, such as descending stairs or recovering from a minor stumble. On physical examination, the hallmark finding is a profound inability to actively extend the knee against gravity, manifesting as a severe extensor lag. Palpation of the anterior knee will reveal a distinct, palpable defect in the substance of the patellar tendon or at its insertion site on the tibial tubercle, accompanied by a loss of normal resting tendon tension. Furthermore, an acute hemarthrosis is almost universally present, distending the joint capsule and exacerbating the patient's discomfort.
It is imperative to distinguish between patellar tendon ruptures and quadriceps tendon ruptures, as their management strategies, while sharing fundamental reconstructive principles, possess distinct technical and biomechanical nuances. Epidemiological data suggests that the patellar tendon is involved more frequently (approximately 0.22% incidence) than the quadriceps tendon (0.1%) in TKA-related extensor mechanism disruptions. Direct, primary repair of the native tendon can be highly successful in the unoperated, native knee. However, in the context of a previous TKA, primary end-to-end repair or transosseous reattachment alone is universally condemned as insufficient. The native tissue in a post-arthroplasty knee is invariably compromised by previous surgical trauma, altered vascularity, and degenerative tendinopathy, leading to unacceptably high failure rates when primary repair is attempted in isolation. Therefore, our definitive goal today is to perform a robust, structural reconstruction of the extensor mechanism utilizing a fresh-frozen Achilles tendon allograft with a calcaneal bone block, potentially augmented with autogenous hamstring grafts, to restore durable, long-term functional stability.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the extensor mechanism's complex, integrated anatomy is the foundation upon which successful reconstruction is built. The extensor mechanism is not merely a collection of tendons and bone; it is a highly sophisticated dynamic unit critical for bipedal ambulation, shock absorption, and joint stability. The primary motor unit is the quadriceps femoris muscle, a massive four-headed structure originating proximally from the femur and ilium. The rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius converge distally to form the trilaminar quadriceps tendon. The rectus femoris tendon represents the most superficial and central component, with its fibers traversing anterior to the patella to become contiguous with the main body of the patellar tendon.
The patella itself is the largest sesamoid bone in the human body, embedded within the substance of the quadriceps tendon. Its primary biomechanical function is to act as a dynamic fulcrum, anteriorly displacing the line of action of the quadriceps force away from the center of rotation of the knee joint. This anterior displacement significantly increases the moment arm of the extensor mechanism, amplifying the mechanical advantage of the quadriceps muscle by up to 30%. The patellar tendon, our primary focus in this reconstructive endeavor, originates at the inferior pole of the patella and inserts distally onto the tibial tuberosity. In a normal adult, it measures approximately 5 to 6 centimeters in length, 3 centimeters in width, and 5 to 7 millimeters in thickness. A complete rupture at any point along this continuum results in the catastrophic loss of the distal attachment, leading to unopposed proximal retraction of the quadriceps muscle and the classic radiographic sign of patella alta.
Furthermore, the medial and lateral retinacula are indispensable secondary stabilizers of the extensor mechanism. These fibrous expansions of the vastus medialis and vastus lateralis muscles insert into the superomedial and superolateral borders of the patella and the proximal tibia. They provide crucial coronal plane stability to the patella and contribute to the overall integrity of the extensor hood. When exposing a ruptured patellar tendon, the surgeon must meticulously assess the integrity of these retinacular structures, as their repair or reconstruction is vital to restoring balanced patellofemoral tracking. From a neurovascular standpoint, the blood supply to the patellar tendon is precarious, primarily derived from the genicular arterial plexus forming a peripatellar anastomotic ring. Previous midline incisions, extensive medial or lateral releases, and the presence of bulky arthroplasty components can severely compromise this microvascular network, predisposing the tendon to ischemic degeneration and eventual mechanical failure.
Exhaustive Indications and Contraindications
The etiology of extensor mechanism disruption following TKA is rarely a singular, isolated traumatic event; rather, it is a multifactorial cascade of predisposing anatomical, biological, and iatrogenic factors. Intraoperative challenges during the index arthroplasty frequently set the stage for future failure. Difficult exposure in a stiff, ankylosed knee often necessitates extensive, forceful retraction that can microscopically tear or crush the tendon fibers. Aggressive soft tissue releases, particularly skeletonization of the tibial tubercle or extensive lateral retinacular releases, can devascularize the tendon, leading to progressive necrosis. Furthermore, forceful manipulation under anesthesia (MUA) for postoperative stiffness exerts massive, uncontrolled tensile loads on a healing, potentially compromised tendon, significantly increasing the risk of iatrogenic rupture.
Biomechanical factors related to the arthroplasty construct itself also play a critical role. Malrotation of the femoral or tibial components, or overall limb malalignment, alters the dynamic Q-angle and leads to abnormal, asymmetric patellofemoral tracking. This places concentrated, eccentric stress on specific portions of the extensor mechanism, accelerating wear and eventual failure. Distal realignment procedures, such as tibial tubercle osteotomies performed to correct tracking issues, inherently weaken the bony insertion site and can be a nidus for avulsion fractures or tendon pull-off. Additionally, patient-specific systemic comorbidities profoundly impact tissue quality and healing capacity. Chronic systemic corticosteroid use, diabetes mellitus, end-stage renal disease, gout, and morbid obesity all compromise collagen synthesis and tensile strength, rendering the tendon highly susceptible to rupture under normal physiological loads.
Nonoperative management has an exceedingly limited, almost non-existent role in the treatment of complete patellar tendon ruptures following TKA. The natural history of a neglected rupture is dismal, characterized by persistent severe extensor lag, recurrent falls, and profound functional disability. A trial of nonoperative management—consisting of prolonged cylinder cast or rigid brace immobilization in full extension—is reserved strictly for the rare patient with a confirmed partial tear where patellar height is maintained, or for patients who are medically unfit to survive a surgical intervention. For the complete ruptures we are discussing, structural allograft reconstruction is the absolute standard of care.
| Category | Indications for Achilles Allograft Reconstruction | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Clinical Presentation | Complete patellar tendon rupture post-TKA; Complete quadriceps tendon rupture post-TKA; Failed primary repair of extensor mechanism. | Active, untreated periprosthetic joint infection (PJI); Overlying soft tissue compromise/active necrosis. | Severe peripheral vascular disease; Active local skin infection (cellulitis). |
| Patient Factors | Medically optimized for complex revision surgery; Adequate bone stock for calcaneal block fixation. | Profound inability to comply with strict postoperative immobilization protocols; Severe cognitive impairment preventing rehab adherence. | Morbid obesity (BMI > 40) complicating rehab; Chronic immunosuppression. |
| Biomechanical | Severe extensor lag (>30 degrees) with inability to actively maintain knee extension; Patella alta on radiographs. | Gross, unaddressed loosening of TKA components (must be revised concurrently or staged). | Severe, uncorrectable joint line elevation from previous surgeries. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous, exhaustive preoperative planning is the cornerstone of a successful extensor mechanism reconstruction. "Failing to plan is planning to fail" is an absolute truth in revision arthroplasty. The initial phase involves a rigorous review of the patient's clinical history, prior operative reports, and current physical examination findings. We must understand the exact implants currently in the patient, the approach used during the index surgery, and any intraoperative complications previously encountered. High-quality, orthogonal radiographs—specifically weight-bearing anteroposterior (AP) and true lateral views—are non-negotiable. On the lateral radiograph, the hallmark sign of a patellar tendon rupture is severe patella alta. We must compare current films with immediate postoperative images to establish the baseline patellar height and definitively diagnose the complete loss of distal continuity.
Crucially, the preoperative radiographic assessment must also scrutinize the existing TKA components. We are actively looking for any signs of aseptic loosening, osteolysis, component subsidence, or gross malalignment. If the tibial or femoral components are loose or malrotated, they must be revised concurrently with the extensor mechanism reconstruction. Grafting a new extensor mechanism onto a mechanically failing, malrotated arthroplasty construct guarantees failure of the allograft due to persistent abnormal kinematics. Therefore, fluoroscopic equipment and a full array of revision arthroplasty instruments, including extraction tools, augments, and stems, must be readily available in the operating theater.
The procurement and inspection of the Achilles tendon allograft require strict attention to detail. The gold standard graft is a fresh-frozen, nonirradiated Achilles tendon allograft that includes a substantial, intact calcaneal bone block. The bone block must measure a minimum of 3 centimeters in length to ensure adequate surface area for rigid press-fit fixation into the proximal tibia. Freeze-dried or heavily irradiated allografts are strictly avoided, as these sterilization processes severely degrade the collagen cross-linking, significantly compromising the biomechanical tensile strength and delaying biological incorporation. Before the patient is anesthetized, the surgeon must personally inspect the thawed allograft on the back table to confirm its dimensions, tissue quality, and the integrity of the bone-tendon junction.
Patient positioning and operating room setup must facilitate both the complex soft tissue reconstruction and any potential concurrent component revision. The procedure is performed in a laminar-flow operating room to minimize the risk of airborne contamination. The patient is positioned supine on a fully radiolucent operating table, allowing for unobstructed intraoperative fluoroscopy from the hip to the ankle. A pneumatic tourniquet is applied to the proximal thigh, typically inflated to 250 mm Hg (or 100 mmHg above systolic pressure) after exsanguination with an Esmarch bandage. If the previous surgical incision extends too proximally, interfering with a standard cuff, a sterile tourniquet is applied after the leg is prepped and draped. The limb is meticulously prepared using chlorhexidine-based solutions and draped with wide sterile margins, ensuring access to the iliac crest should autogenous bone grafting become necessary.
Step-by-Step Surgical Approach and Fixation Technique
The Surgical Approach and Initial Exposure
We begin by utilizing the patient's previous anterior midline incision to minimize the creation of devascularized skin bridges. The skin is incised sharply with a #10 blade, and the dissection is carried down through the subcutaneous tissues.

Subcutaneous flaps are elevated conservatively, maintaining full-thickness fasciocutaneous flaps to preserve the tenuous vascular supply to the anterior knee skin. We must remain hyper-vigilant regarding the superficial neurovascular structures, particularly the infrapatellar branch of the saphenous nerve medially. Aggressive electrocautery or excessive traction in this region can lead to painful neuromas or troublesome sensory deficits.
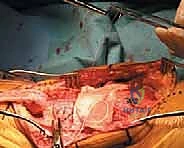
Upon reaching the deep fascia, we expose the retinaculum and the remnants of the extensor mechanism. The catastrophic nature of the injury is immediately apparent; a large, disorganized void exists where the patellar tendon should bridge the patella to the tibial tubercle.

We perform a thorough debridement of the rupture site, excising necrotic, fibrotic, and severely degenerated tendon edges back to healthy, bleeding tissue. A midline incision is made through any remaining patellar tendon remnant and extended proximally over the patella and distally over the tibial tubercle. Medial and lateral full-thickness retinacular flaps are mobilized. The joint space is frequently filled with organized hematoma and fibrinous debris, which is meticulously evacuated. Copious pulsatile lavage is employed to thoroughly irrigate the joint, reducing the bacterial bioburden and clearing the field for reconstruction.
Graft Preparation and Bone Trough Creation
Attention is now turned to the preparation of the host site and the allograft. The proximal tibia must be prepared to receive the calcaneal bone block. Using an oscillating saw and high-speed burrs, a precise, rectangular trough is created in the anatomical footprint of the tibial tubercle.

The dimensions of this trough must exactly match the templated dimensions of the calcaneal bone block to ensure a tight, interference press-fit. The trough is typically fashioned with a slight dovetail configuration, narrower at the anterior cortex and wider posteriorly, to resist anterior pull-out forces.
Simultaneously, on the back table, the Achilles allograft is meticulously prepared. The calcaneal bone block is trimmed and contoured with a saw to match the exact dimensions of the tibial trough.
The Achilles tendon itself is inspected, and any redundant muscle belly or adipose tissue is sharply excised. Heavy, non-absorbable, braided sutures (such as #2 or #5 FiberWire) are woven through the proximal and distal aspects of the allograft tendon using a locking Krackow technique.

This provides robust points of fixation for tensioning and securing the graft to the host tissues.
Allograft Implantation and Primary Repair Augmentation
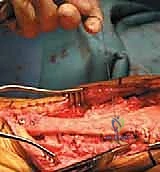
The contoured calcaneal bone block is now impacted into the prepared tibial trough. The fit should be exceptionally tight, providing immediate structural stability.
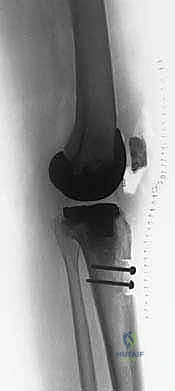
To supplement the press-fit, the bone block is rigidly fixed to the proximal tibia using two or three fully threaded, bicortical 3.5mm or 4.5mm cortical screws, or alternatively, heavy intraosseous cerclage wires.

Care must be taken to angle these screws to avoid the intramedullary stem of the tibial arthroplasty component.

Once distal bony fixation is absolutely secure, attention turns to the proximal fixation. If the native patella is retained and possesses adequate bone stock, we create two or three longitudinal, parallel drill tunnels through the patella using a 2.0mm or 2.5mm drill bit.

These tunnels must have an adequate bone bridge between them to prevent catastrophic pull-through during tensioning.

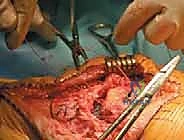
The Achilles tendon allograft is then routed proximally, passing either over the anterior surface of the patella or, in some techniques, woven through a coronal slit in the quadriceps tendon.
The heavy Krackow sutures previously placed in the allograft are passed through the patellar bone tunnels from distal to proximal.

This is the most critical phase of the operation: tensioning the graft. The knee is placed in maximal, rigid, full extension (0 degrees).

The allograft is pulled proximally with maximum manual tension, effectively pulling the patella distally to correct the patella alta and restore the normal anatomical resting length of the extensor mechanism. While maintaining this absolute maximum tension, the sutures are tied securely over the superior pole of the patella.

To further augment this construct, the medial and lateral retinacular flaps, along with any viable remnants of the native patellar tendon, are meticulously imbricated and sutured over the allograft using interrupted, heavy non-absorbable sutures.
This "pants-over-vest" closure provides secondary biological coverage, enhances the vascular supply to the allograft, and adds significant mechanical strength to the repair.

The entire construct is tested under direct visualization. The knee is very gently flexed to 30 degrees to ensure the repair holds under initial physiological tension, though extreme flexion is strictly avoided at this stage.

Finally, the wound is closed in standard layered fashion over a closed suction drain to prevent postoperative hematoma formation, which could compromise skin healing over the bulky allograft.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, extensor mechanism reconstruction with an Achilles allograft remains a salvage procedure fraught with significant complication risks. The most common and frustrating complication is a residual extensor lag, resulting from the viscoelastic "creep" or stretching out of the allograft over time. Even when tensioned maximally in full extension intraoperatively, the allograft is biologically dead tissue undergoing a prolonged process of creeping substitution. During this revascularization phase, the collagen matrix weakens before it remodels, leading to elongation. Studies indicate that up to 30-40% of patients will experience a clinically noticeable extensor lag (often 10 to 20 degrees) at long-term follow-up, though many remain functionally satisfied if they can maintain dynamic stability during the stance phase of gait.
Infection is a catastrophic complication in this setting, given the massive amount of avascular allograft tissue and the presence of revision arthroplasty hardware. Deep periprosthetic joint infection (PJI) or allograft infection occurs in approximately 5% to 10% of these complex cases. The avascular nature of the allograft makes it an ideal nidus for bacterial biofilm formation, rendering systemic antibiotics largely ineffective. If a deep infection occurs, the entire allograft must be completely excised, the joint aggressively debrided, and the patient placed on appropriate intravenous antibiotics, often necessitating a staged approach if the arthroplasty components are also involved.
Skin necrosis and wound breakdown over the anterior knee are also significant concerns. The combination of previous surgical scars, compromised microvasculature, and the added bulk of the allograft creates a high-tension environment for the overlying skin flaps. Meticulous soft tissue handling and the avoidance of early, aggressive knee flexion are critical to preventing wound dehiscence. If the reconstruction fails entirely—due to infection, massive graft rupture, or profound, unbraceable extensor lag—salvage options are severely limited.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Options |
|---|---|---|---|
| Residual Extensor Lag (>15°) | 30% - 45% | Maximal intraoperative tensioning in 0° extension; Strict adherence to prolonged extension bracing post-op. | Usually tolerated if patient is stable; AFO bracing; Rarely, revision allografting if functionally disabling. |
| Allograft Rupture / Failure | 10% - 15% | Use of fresh-frozen (not irradiated) grafts; Augmentation with autogenous hamstrings or synthetic mesh. | Repeat Achilles allograft reconstruction; Synthetic mesh (Marlex) reconstruction. |
| Deep Infection (PJI / Graft) | 5% - 10% | Laminar flow OR; Copious pulsatile lavage; Meticulous hemostasis to prevent hematoma. | Urgent radical debridement; Complete excision of allograft; Antibiotic spacer; Eventual staged reconstruction or arthrodesis. |
| Skin Necrosis / Wound Dehiscence | 5% - 8% | Maintain thick fasciocutaneous flaps; Avoid crossing previous incisions; Delay post-op flexion. | Local wound care; Vacuum-assisted closure (VAC); Gastrocnemius rotational flap coverage for exposed graft/hardware. |
| Ultimate Failure (Unsalvageable) | 2% - 5% | Rigorous patient selection; Optimization of medical comorbidities prior to index surgery. | Knee arthrodesis (using intramedullary nail); Above-knee amputation (AKA) as a definitive last resort. |
Phased Post-Operative Rehabilitation Protocols
The surgical procedure itself represents only half of the battle; the postoperative rehabilitation protocol is equally, if not more, critical to the ultimate success of the Achilles allograft reconstruction. The protocol is intentionally slow, highly restrictive, and demands absolute patient compliance. The primary objective during the first two months is the protection of the allograft-host bone and tendon junctions to allow for initial biological incorporation and to prevent catastrophic elongation or rupture of the graft.
Phase I: Absolute Protection (Weeks 0 to 6)
Immediately postoperatively, the patient's knee is locked in a rigid cylinder cast or a locked hinged knee orthosis in absolute, full extension (0 degrees). There is absolutely no active or passive knee flexion permitted during this phase. Weight-bearing status is typically restricted to toe-touch or partial weight-bearing with bilateral crutches or a walker, depending on the security of the tibial bone block fixation and any
