Revision Total Knee Arthroplasty: Mastering Femoral Bone Loss with Augments and Allografts

Key Takeaway
Join us in the OR for a detailed masterclass on Revision Total Knee Arthroplasty. We'll meticulously address femoral bone loss using metal augments and various grafting techniques. This guide covers comprehensive anatomy, precise planning, granular intraoperative steps, critical pearls, and comprehensive postoperative management, ensuring optimal outcomes for complex knee revisions.
Comprehensive Introduction and Patho-Epidemiology
The burden of revision total knee arthroplasty (TKA) is escalating at an unprecedented trajectory, driven by an aging population, the expansion of primary TKA indications to younger, higher-demand patients, and the inevitable lifespan of prosthetic components. Current epidemiological projections indicate that the volume of revision TKAs is skyrocketing, anticipated to increase at an annual rate of 19.3%. Within this expanding cohort, addressing significant femoral bone loss remains one of the most formidable challenges an orthopedic surgeon can face. This is the crucible where a profound understanding of three-dimensional anatomy, meticulous preoperative templating, and precise, adaptable intraoperative execution truly separate the good from the great. Mastering these advanced reconstructive techniques is no longer an optional subspecialty skill; it is paramount for any surgeon undertaking complex knee arthroplasty.
Femoral bone loss in the revision setting is a complex, multifactorial phenomenon, primarily affecting the distal and posterior aspects of the femur. This is a common scenario in revision surgery, contrasting sharply with primary cases where bone stock is typically preserved. The etiology of this bone deficiency includes osteolysis secondary to polyethylene wear debris, aseptic loosening with micromotion, catastrophic periprosthetic joint infection (PJI), periprosthetic fractures, and iatrogenic bone loss that inevitably occurs during the extraction of well-fixed primary components. The resulting defects are rarely uniform; they are often cavitary, segmental, and highly irregular, compromising the structural integrity of the metaphyseal envelope required to support a new implant.
Our reconstructive goals in the face of such devastation are unequivocally clear and biomechanically rigid: we must completely fill the osseous defect with biologically or mechanically stable material, accurately restore the femorotibial joint line, and meticulously re-establish the posterior condylar offset. Deviations in any of these parameters will inevitably compromise prosthetic kinematics, leading to mid-flexion instability, patella baja, restricted range of motion, and ultimately, premature failure of the revision construct. As a fundamental biomechanical rule, the native joint line typically sits approximately 25 mm distal to the medial and lateral femoral epicondyles, and the posterior femoral condyles project, on average, 25.8 mm posterior to the posterior femoral cortex.
Fortunately, the armamentarium available to the revision arthroplasty surgeon has evolved dramatically. Advances in prosthesis design, modularity, and biomaterials—particularly the advent of highly porous metaphyseal cones, titanium sleeves, and modular metallic augments—have significantly expanded our capabilities. When combined with traditional techniques such as cemented stems and structural allografts, modern modular revision systems allow for highly customized, patient-specific reconstructions that can achieve immediate rigid fixation and long-term survivorship even in the most profoundly deficient femurs.
Detailed Surgical Anatomy and Biomechanics
Before a single incision is made, a profound and exhaustive review of the critical anatomy of the distal femur and its surrounding neurovascular envelope is non-negotiable. Safe, effective, and reproducible revision surgery demands a threedimensional spatial awareness of this region.
Osteology and the AORI Bone Loss Classification
The distal femur comprises the medial and lateral condyles, which articulate with the tibial plateau, and the intercondylar notch, which houses the cruciate ligaments in the native knee and the cam-post mechanism or hinge in a revision prosthesis. Superiorly, the medial and lateral epicondyles serve as the absolute most critical landmarks for establishing the rotational alignment of the femoral component (the surgical transepicondylar axis). The adductor tubercle, located proximal to the medial epicondyle, is another vital landmark. Bone loss in this region is rarely straightforward; it often involves the distal weight-bearing surfaces (leading to joint line elevation), the posterior condyles (resulting in profound flexion instability), and the metaphyseal cancellous bone (compromising implant seating and fixation).
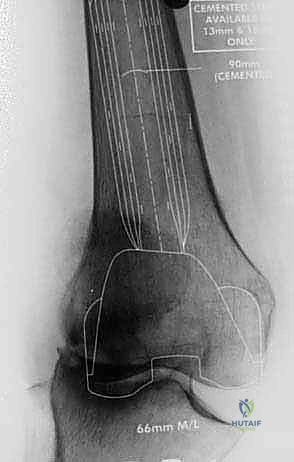
FIG 1 • A. AP radiograph of a knee with severe deformity that has resulted in severe bone loss.

FIG 1 • A. AP radiograph of a knee with severe deformity that has resulted in severe bone loss.
The Anderson Orthopaedic Research Institute (AORI) classification remains the gold-standard roadmap for categorizing femoral defects and guiding our reconstructive algorithms:
* Type I: Intact metaphyseal bone with minor, contained defects that do not compromise the stability of a standard revision component. These are typically managed elegantly with polymethylmethacrylate (PMMA) cement or morselized cancellous bone graft.
* Type II: Damaged metaphyseal bone that requires augmentation to establish a stable platform.
* Type IIA: Cancellous bone loss necessitating cement fill, modular augments, or bone graft to restore a reasonable joint line. Defects are typically less than 5 mm (managed with cement/bone graft) or 5-10 mm (managed with metallic augments). These defects usually involve only one condyle.
* Type IIB: More extensive defects involving both the medial and lateral condyles, universally requiring larger metallic augments or highly porous metaphyseal cones/sleeves to achieve stability.
* Type III: Profoundly deficient metaphyseal bone compromising a major portion of either condyle to the extent that standard augments are insufficient. This requires structural bone graft, highly porous metaphyseal cones, a hinged implant, or a custom megaprosthesis. This severe defect can be unicondylar (often treated with metal augments or a femoral head allograft) or bicondylar (necessitating massive metal augments, cones, or a distal femoral replacement).
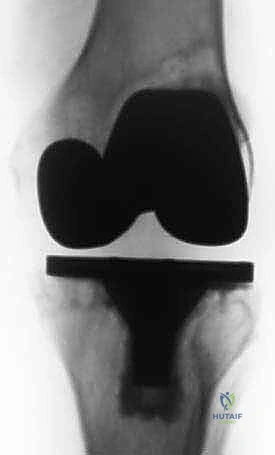
FIG 2 • A. AP radiograph of the knee before revision surgery. Large osteolytic defects involving both the femur and the tibia are visible.

FIG 2 • B. Lateral radiograph of the knee before revision surgery. Large osteolytic defects involving both the femur and the tibia are visible. Careful preoperative planning is required to be able to address bone loss encountered at the time of arthroplasty.
Neurovascular Structures: A Constant Vigilance
The popliteal fossa, situated immediately posterior to our surgical field, houses vital neurovascular structures that are at high risk during complex revisions, particularly when managing severe posterior condylar bone loss or extracting well-fixed stemmed components. The popliteal artery and vein are the most critical structures, running deep and directly posterior to the joint capsule. They are tethered proximally at the adductor hiatus and distally at the soleal arch, making them highly susceptible to traction injuries. Excessive posterior retraction, over-penetration with a saw blade, or aggressive levering during component removal can lead to catastrophic vascular injury, potentially resulting in limb loss.
The tibial nerve runs in close proximity to the popliteal vessels and is similarly at risk during aggressive posterior dissection. The common peroneal nerve courses laterally around the fibular neck, posterior to the lateral femoral condyle and lateral collateral ligament. It is highly vulnerable during extensive lateral releases, correction of severe valgus deformities, or excessive lateral retraction. The saphenous nerve, a sensory branch of the femoral nerve, accompanies the femoral artery through the adductor canal and emerges medially; it can be at risk during extensive medial dissection or when placing medial retractors. Always be mindful of your retractors. Avoid levering directly on bone, especially posteriorly. Maintain clear visibility and use broad, smooth retractors (such as a bent Hohmann or a posterior cruciate retractor) to gently protect the posterior soft tissue envelope.
Muscular Intervals and Tendinous Attachments
Our primary surgical approach, the standard medial parapatellar arthrotomy, utilizes the internervous and intermuscular interval between the vastus medialis obliquus (VMO) and the rectus femoris/quadriceps tendon. Protecting the integrity of the extensor mechanism—specifically the quadriceps tendon and the patellar tendon—is of paramount importance. During exposure, particularly in stiff knees, avoid undue tension or direct trauma to the patellar tendon insertion at the tibial tubercle, as an avulsion here is a devastating complication.
The origins of the medial collateral ligament (MCL) on the medial epicondyle and the lateral collateral ligament (LCL) on the lateral epicondyle must be meticulously preserved if a non-hinged (condylar constrained) prosthesis is planned. Their integrity is the cornerstone of coronal plane stability. When severe bone loss dictates the use of structural allografts, we must meticulously preserve a thin shell of native host bone with these ligamentous attachments to wrap around the graft. Furthermore, patellar maltracking and extensor mechanism dysfunction are ubiquitous in revision cases due to altered joint lines and scar tissue. The surgeon must be fully prepared to execute a quadriceps snip, a V-Y quadricepsplasty, or an extended tibial tubercle osteotomy (TTO) for severe contractures, fully understanding the biomechanical implications for postoperative rehabilitation.
Exhaustive Indications and Contraindications
The decision algorithm for managing femoral bone loss in revision TKA is dictated by the AORI classification, the patient's physiological age, functional demands, and the presence or absence of infection. The primary indication for utilizing modular metallic augments is the presence of uncontained, peripheral bone defects (AORI Type IIA and IIB) measuring between 5 mm and 15 mm. Augments provide immediate, rigid structural support, allow for precise restoration of the joint line, and seamlessly integrate with the revision femoral component. For contained cavitary defects (AORI Type I) less than 5 mm, PMMA cement, often reinforced with screws, or morselized cancellous bone allograft remains the standard of care.
When metaphyseal bone loss is profound and non-supportive (AORI Type IIB or III), modular augments alone are biomechanically insufficient. In these scenarios, the indications shift heavily toward highly porous metaphyseal cones (tantalum or 3D-printed titanium) or stepped titanium sleeves. These devices provide robust diaphyseal-metaphyseal fixation, bypass the deficient condylar bone, and offer a highly osteoconductive surface for long-term biologic ingrowth. Structural allografts (distal femoral replacements or femoral head allografts) are indicated for massive, uncontained Type III defects where host bone is virtually absent, though their use has declined in favor of porous metal cones due to the high rates of allograft non-union, resorption, and disease transmission risks.

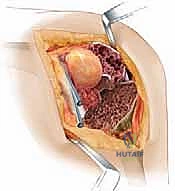
FIG 1 • B. Massive bone loss was encountered during revision surgery with severe osteolysis.

FIG 1 • B. Massive bone loss was encountered during revision surgery with severe osteolysis.
Contraindications to immediate reconstruction with augments or allografts are primarily biological. Active periprosthetic joint infection (PJI) is an absolute contraindication to a single-stage reconstruction with massive hardware or structural allograft; these cases mandate a two-stage approach with an antibiotic-loaded articulating spacer. Relative contraindications include an inadequate soft tissue envelope (requiring prior or concurrent flap coverage), severe peripheral vascular disease (which may preclude the safe use of a tourniquet or compromise wound healing), and profound neurological deficits (e.g., Charcot arthropathy) where a hinged megaprosthesis or arthrodesis might be more appropriate.
Table 1: Modalities for Managing Femoral Bone Loss
| Modality | Indication (AORI Type) | Advantages | Disadvantages / Risks |
|---|---|---|---|
| PMMA Cement / Morselized Graft | Type I (Contained, <5mm) | Inexpensive, readily available, technically simple. | Poor structural support for large defects, cement disease. |
| Modular Metallic Augments | Type IIA, IIB (Uncontained, 5-15mm) | Immediate structural support, precise joint line restoration. | Fretting/corrosion at modular junctions, limited to available sizes. |
| Highly Porous Metaphyseal Cones | Type IIB, Type III (Metaphyseal compromise) | Excellent biologic ingrowth, robust metaphyseal fixation. | Technically demanding preparation, difficult to extract if infected. |
| Structural Allografts | Severe Type III (Massive uncontained loss) | Restores bone stock for future revisions, allows ligament reattachment. | High rate of non-union, resorption, fracture, infection risk. |
| Distal Femoral Megaprosthesis | Catastrophic Type III, Oncologic resection | Immediate mobilization, bypasses all deficient bone. | High risk of aseptic loosening, hinge failure, infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Success in revision TKA is unequivocally forged in the preoperative planning phase. This is not merely an administrative formality; it is the critical blueprint for anticipating catastrophic challenges and ensuring the appropriate implants are available in the operating theater. The clinical evaluation must be exhaustive. We must definitively rule out infection in every single revision case. A complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) are mandatory. If there is even a microscopic suspicion of infection, or if inflammatory markers are elevated, a fluoroscopically guided joint aspiration for synovial fluid cell count, differential, and extended cultures is absolutely required.
Advanced imaging protocols form the bedrock of our templating. Standard standing AP, lateral, and Merchant views are obtained, but they are insufficient in isolation. We mandate full-length, weight-bearing hip-to-ankle radiographs to assess the overall mechanical axis, identify extra-articular deformities, and template the required length and trajectory of diaphyseal engaging stems. A CT scan with metal artifact reduction software (MARS) is heavily utilized to accurately quantify the volumetric size and spatial location of osteolytic defects, and to assess the rotational landmarks (epicondylar axis) which are often obscured on plain films.
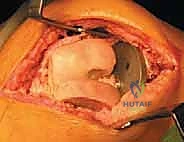
FIG 2 • C. Most cases of knee revision with bone loss can be addressed with the use of a long-stem prosthesis and metal augments.
Digital and manual templating are performed meticulously. We template the femoral component size based on the unaffected contralateral knee or the remaining AP dimension of the native femur. We determine the necessary stem length and diameter to achieve rigid diaphyseal fixation, adhering to the principle that the stem must bypass the most proximal cortical defect by a minimum of two cortical diameters. We proactively plan for the required distal and posterior augments to restore the joint line to its anatomic position (25 mm distal to the epicondyles). Furthermore, for severe cases, we ensure that highly porous cones, sleeves, structural allografts, and a fully constrained hinged prosthesis are sterilized and present in the room.




In the operating room, patient positioning must be flawless. The patient is positioned supine on a radiolucent operating table to accommodate intraoperative fluoroscopy. Meticulous padding is critical; we pad the heels, sacrum, and ensure the ulnar nerves are protected at the elbows. A small bolster is placed under the ipsilateral hip to prevent external rotation of the limb, ensuring a true AP alignment for imaging and component placement. A sterile tourniquet is applied high on the thigh, inflated only when necessary (typically during cementation) to minimize ischemic time. The C-arm is draped and positioned to allow for rapid AP and lateral views, which are crucial for confirming stem trajectory and preventing cortical perforation during canal preparation.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a complex revision with massive bone loss demands a systematic, step-wise approach. We begin with a standard midline skin incision, heavily utilizing previous incisions when possible, extending proximally and distally to ensure extensile exposure. The medial parapatellar arthrotomy is developed. In cases of severe stiffness or patella baja, we do not hesitate to perform a quadriceps snip or an extended tibial tubercle osteotomy early in the procedure to protect the patellar tendon from avulsion.
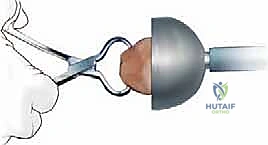
The extraction of the primary components must be performed with surgical finesse to preserve every millimeter of remaining host bone. We utilize flexible osteotomes, Gigli saws, and specialized extraction devices to disrupt the implant-cement or implant-bone interfaces. Once the components are removed, aggressive debridement of the reactive pseudocapsule, particulate debris, and all fibrous tissue from the osteolytic cysts is performed. This exposes the true extent of the AORI bone loss, which is often more severe than templated. We then prepare the diaphyseal canal. Using sequential reamers, we prepare the canal to accept a diaphyseal engaging stem. For cementless, press-fit stems (fluted, tapered), we typically ream line-to-line or under-ream by 0.5 to 1.0 mm to achieve rigid diaphyseal scratch-fit stability.

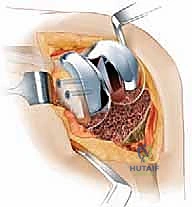
With diaphyseal stability established, we turn our attention to the metaphysis and the joint line. The femoral trial is attached to the stem trial. We assess the gap kinematics in flexion and extension. Distal augments are added to the femoral trial to bring the joint line down to the level of the inferior pole of the patella and 25 mm distal to the epicondyles, tightening the extension gap. Posterior augments are added to restore the posterior condylar offset, tensioning the collateral ligaments in flexion and establishing the AP dimension of the femur.



If the metaphyseal bone is too deficient to support the augments (AORI Type IIB/III), we proceed with metaphyseal cone preparation. The highly porous tantalum or titanium cone provides a structural bridge between the intact diaphysis and the joint line. We sequentially broach the distal femur over a reamer to shape the cavitary defect to match the geometry of the cone. The cone is impacted until a rigid, rotationally stable scratch-fit is achieved. The internal geometry of the cone will subsequently be filled with PMMA cement to bond it to the revision femoral component.





