Revision Total Knee Arthroplasty with Extensile Exposure: V-Y Quadricepsplasty Masterclass
Key Takeaway
This masterclass provides a granular, intraoperative guide to V-Y quadricepsplasty for revision total knee arthroplasty. We'll meticulously cover preoperative planning, patient positioning, and a graduated approach to extensile exposure, from initial incision to advanced quadriceps turndown. Critical surgical anatomy, instrument use, and real-time decision-making are emphasized, alongside comprehensive pearls, pitfalls, and postoperative management strategies to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to a definitive exploration of one of the most demanding scenarios encountered in the adult reconstruction operating theater: the revision total knee arthroplasty (TKA) in the setting of severe ankylosis or profound arthrofibrosis. Gaining adequate surgical exposure in these complex revision scenarios, or even in primary TKA for a completely fused knee, presents an exceptional biomechanical and technical challenge. While contemporary literature suggests that upwards of 90% of routine revision TKAs can be managed through a standard medial parapatellar approach with graduated soft tissue releases, it remains absolutely critical for the academic and high-volume orthopaedic surgeon to possess absolute proficiency in extensile exposure techniques. Failure to master these approaches invites catastrophic iatrogenic extensor mechanism disruption, compromised component positioning, and ultimately, dismal postoperative functional outcomes.
The patho-epidemiology of the stiff or ankylosed knee requiring revision is multifactorial and dictates the necessity for an extensile approach. Arthrofibrosis following primary TKA, recurrent hemarthrosis, chronic low-grade periprosthetic joint infection (PJI), and extensive heterotopic ossification can all lead to a severely contracted extensor mechanism. In these patients, the quadriceps muscle undergoes fibrotic infiltration, losing its inherent elasticity and excursion capabilities. When the surgeon attempts to evert the patella or hyperflex the knee during a standard arthrotomy, the tension transmitted through the patellar tendon insertion at the tibial tubercle exceeds the ultimate tensile strength of the tissue, risking an avulsion fracture or mid-substance tendon rupture—complications that are notoriously difficult to salvage and carry a high morbidity burden.
The philosophy of extensile exposure is rooted in a graduated, stepwise escalation. We do not immediately resort to a V-Y quadricepsplasty or a tibial tubercle osteotomy (TTO) without first exhausting standard soft tissue releases, including extensive synovectomy, lateral retinacular release, and distal subperiosteal elevation of the medial collateral ligament (MCL). However, when the patella cannot be safely everted or laterally subluxated to allow for orthogonal visualization of the medullary canals and joint spaces, the surgeon must confidently transition to an extensile technique. The V-Y quadricepsplasty, originally popularized by Coonse and Adams and later modified by Insall, serves as a powerful tool in this armamentarium, providing not only unparalleled exposure of the joint but also offering a mechanism to functionally lengthen a severely contracted extensor mechanism.
This masterclass chapter will dissect the V-Y quadricepsplasty, detailing its anatomical foundations, precise surgical execution, and the nuanced postoperative rehabilitation required to optimize outcomes. We will explore the critical decision-making matrix that guides a surgeon to select a V-Y advancement over a quadriceps snip or a TTO, focusing on patient-specific variables such as bone stock, patellar height, and prior surgical incisions. By mastering the principles outlined herein, the reconstructive surgeon can navigate the treacherous waters of the ankylosed revision TKA with confidence, ensuring both the preservation of the extensor mechanism and the precise implantation of revision arthroplasty components.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the extensor mechanism's layered anatomy and its precarious vascular supply is the absolute prerequisite for performing a safe and effective V-Y quadricepsplasty. The quadriceps femoris tendon is a trilaminar structure. The superficial layer is formed by the rectus femoris; the robust middle layer represents the confluent aponeuroses of the vastus medialis and vastus lateralis; and the deep layer is comprised of the vastus intermedius. During the creation of the V-Y turndown flap, the surgeon must appreciate these distinct layers to ensure a full-thickness mobilization of the extensor apparatus. Failure to incorporate all layers into the turndown flap will result in a flimsy, mechanically inferior repair that is highly susceptible to postoperative rupture or severe extensor lag.
The vascular anatomy of the anterior knee is arguably the most critical consideration during extensile exposures. The patella relies on an anastomotic ring fed primarily by the superior lateral, superior medial, inferior lateral, and inferior medial geniculate arteries, along with contributions from the descending genicular artery. The superior lateral geniculate artery (SLGA) is of paramount importance. It courses transversely from lateral to medial, passing just superior to the lateral pole of the patella. When performing a lateral retinacular release—a mandatory step preceding the quadriceps turndown—the SLGA is highly vulnerable. Iatrogenic transection of the SLGA, combined with the medial parapatellar arthrotomy, effectively devascularizes the lateral and superior aspects of the patella, drastically increasing the incidence of postoperative patellar osteonecrosis, fragmentation, and component loosening.
Biomechanically, the V-Y quadricepsplasty fundamentally alters the resting tension and excursion of the extensor mechanism. By converting the V-shaped turndown incision into an inverted Y during closure, the surgeon effectively lengthens the quadriceps tendon. While this lengthening is highly beneficial for achieving postoperative flexion in a previously ankylosed knee, it comes at the direct cost of extensor power. The lengthened muscle-tendon unit operates at a mechanically disadvantageous position on the Starling curve, frequently resulting in a postoperative extensor lag. The surgeon must meticulously balance the desire for increased flexion with the absolute necessity of maintaining active terminal extension.
Furthermore, the altered kinematics post-V-Y quadricepsplasty impact patellofemoral contact forces. The lengthening of the tendon can alter the patellar tracking trajectory, potentially leading to maltracking or instability if the lateral retinacular release is not carefully managed. The repair must be robust enough to withstand the immense tensile forces generated during early rehabilitation, yet precise enough to maintain the patella centralized within the trochlear groove of the revision femoral component. Understanding these biomechanical trade-offs is essential for intraoperative decision-making regarding the exact degree of advancement (typically 1% to 2% of total length) permitted during the final closure.
Exhaustive Indications and Contraindications
The decision to employ a V-Y quadricepsplasty must be strictly evidence-based and tailored to the individual patient's pathoanatomy. The primary indication for this extensile approach is a revision TKA in the setting of severe global arthrofibrosis or true bony ankylosis where standard graduated releases fail to provide safe exposure. Specifically, if the knee cannot be flexed beyond 45 to 60 degrees after a thorough medial and lateral gutter clearance, extensive synovectomy, and lateral retinacular release, an extensile approach is mandatory. The V-Y technique is particularly advantageous in patients with profound quadriceps contracture where the surgeon actively desires to lengthen the extensor mechanism to improve postoperative flexion arcs, a benefit not inherently provided by a standard quadriceps snip.
Relative indications include cases requiring massive revision components (such as total distal femoral replacements or complex hinged prostheses) where unimpeded orthogonal access to the femoral and tibial metadiaphyses is required. Additionally, the V-Y approach may be selected over a tibial tubercle osteotomy (TTO) in patients with severe proximal tibial osteopenia or osteoporosis. In such osteoporotic bone, the fixation of a TTO block with wires or screws is highly prone to mechanical failure, nonunion, or proximal tibial fracture. Therefore, soft-tissue-based extensile exposures like the V-Y quadricepsplasty become the safer alternative, shifting the risk profile from bony nonunion to soft tissue extensor lag.
Conversely, absolute and relative contraindications must be rigorously respected. A primary contraindication is compromised anterior soft tissue envelopes or precarious skin vascularity, as the extensive subcutaneous dissection required for the V-Y flap can precipitate catastrophic full-thickness skin necrosis. Furthermore, the V-Y approach is relatively contraindicated in patients with a pre-existing severe extensor lag or profound quadriceps weakness (e.g., prior poliomyelitis, severe neuropathy), as the inherent lengthening of the procedure will invariably exacerbate the extensor deficit, rendering the patient unable to achieve a functional straight-leg raise. In cases of active periprosthetic joint infection requiring a two-stage exchange, a V-Y should be avoided during the first stage if possible, as the devascularized tendinous edges are highly susceptible to persistent colonization.
| Clinical Scenario / Factor | V-Y Quadricepsplasty | Tibial Tubercle Osteotomy (TTO) | Quadriceps Snip |
|---|---|---|---|
| Severe Quadriceps Contracture | Highly Indicated (allows lengthening) | Moderately Indicated | Poorly Indicated (no lengthening) |
| Severe Proximal Tibial Osteopenia | Indicated (soft tissue only) | Contraindicated (high fracture risk) | Indicated |
| Patella Baja (Infera) | Contraindicated (worsens baja) | Highly Indicated (allows proximalization) | Neutral |
| Need for Extensor Lengthening | Excellent | Poor | None |
| Risk of Post-op Extensor Lag | High | Low to Moderate | Low |
| Risk of Bony Nonunion | None | High | None |
Pre-Operative Planning, Templating, and Patient Positioning
Before the patient ever enters the operating theater, meticulous preoperative planning is the bedrock of a successful complex revision TKA. The clinical assessment must exhaustively detail the patient's prior surgical history, focusing on the number, orientation, and viability of previous skin incisions. The surgeon must evaluate the resting tension of the soft tissue envelope and document the preoperative range of motion, explicitly noting any fixed flexion deformities or existing extensor lags. A thorough vascular examination is mandatory; diminished distal pulses or signs of chronic venous stasis should prompt formal vascular studies, as the extensive dissection required for a V-Y quadricepsplasty places significant metabolic demand on the local soft tissues.
Radiographic evaluation must be comprehensive and multidimensional. High-quality standing anteroposterior (AP), lateral, and Merchant views are scrutinized to assess component loosening, the degree of osteolysis, overall mechanical alignment, and crucially, patellar height. The presence of true patella baja (infera) is a critical data point; a V-Y quadricepsplasty may exacerbate patella baja biomechanics, making a TTO a potentially superior choice in that specific anatomic scenario. Furthermore, computed tomography (CT) with metal artifact reduction sequence (MARS) is heavily utilized to quantify metaphyseal bone loss, map osteolytic cysts, and determine the exact rotational profile of retained components, which dictates the necessary extraction strategy and subsequent exposure requirements.
Digital templating is an absolute necessity, not a luxury. The surgeon must template the anticipated revision components, including diaphyseal engaging stems, metaphyseal cones or sleeves, and the potential need for varying levels of prosthetic constraint (e.g., constrained condylar or rotating hinge designs). By anticipating the size and trajectory of the required implants, the surgeon can accurately predict the necessary volume of surgical exposure. If the templating suggests the need for a 150mm tibial stem and a massive metaphyseal cone in a patient with 30 degrees of preoperative flexion, the surgical team must be pre-emptively prepared for an extensile exposure, ensuring all specialized retractors and heavy non-absorbable sutures are immediately available in the room.
Patient positioning and operating room setup must facilitate dynamic assessment of the limb throughout the procedure. The patient is positioned supine with a standard radiolucent knee positioner that allows for unhindered flexion past 120 degrees and stable support in terminal extension. A pneumatic tourniquet is applied high on the proximal thigh; however, its use should be judicious. In complex revisions requiring prolonged operative times, the tourniquet is often deflated after the initial exposure to minimize ischemic injury to the already compromised extensor mechanism and to allow for meticulous hemostasis prior to closure. A sterilely draped C-arm fluoroscope must be readily available to assist with complex hardware extraction and to verify the trajectory of long intramedullary stems, ensuring they bypass cortical stress risers without inducing iatrogenic fractures.
Step-by-Step Surgical Approach and Fixation Technique
Initial Incision and Graduated Arthrotomy
The surgical approach begins with a highly calculated skin incision. The surgeon must utilize the most lateral usable prior incision to preserve the medial vascular supply to the anterior skin flap, adhering strictly to the principle that the dominant blood supply to the anterior knee skin arises medially. If a previous incision must be intersected, it must be crossed at an angle of no less than 60 degrees to prevent the creation of ischemic skin bridges. Thick, full-thickness fasciocutaneous flaps are developed, ensuring the dissection plane remains strictly superficial to the deep investing fascia of the extensor mechanism. Meticulous excision of all avascular peripatellar scar tissue is performed using electrocautery, which not only aids in mobilization but also reduces the nidus for recurrent arthrofibrosis.
Following flap development, a standard medial parapatellar arthrotomy is executed. The incision begins at the junction of the medial and central thirds of the quadriceps tendon, extending distally over the medial border of the patella and alongside the patellar ligament down to the medial aspect of the tibial tubercle. Upon entering the joint, the surgeon immediately encounters dense, fibrotic adhesions characteristic of the revision setting. A thorough, systematic synovectomy is mandatory. The suprapatellar pouch, medial gutter, and lateral gutter must be meticulously reconstituted using sharp dissection and electrocautery.
At this juncture, the surgeon attempts a graduated exposure. The knee is gently flexed while the tibia is internally rotated and subluxated anteriorly. If tension remains excessive, a subperiosteal elevation of the superficial medial collateral ligament (MCL) from its proximal tibial insertion is performed to allow further external rotation and anterior translation of the tibia. Concurrently, a formal lateral retinacular release is executed from inside out, taking absolute care to visualize and protect the superior lateral geniculate artery (SLGA).
If these comprehensive graduated maneuvers fail to allow safe eversion or lateral translation of the patella without impending avulsion of the patellar tendon, the surgeon must formally declare the need for an extensile approach and proceed to the quadriceps turndown.
The Quadriceps Turndown Technique
The transition to the quadriceps turndown requires precise geometric incisions to create a viable, distally based flap. The surgeon first extends the proximal aspect of the medial parapatellar arthrotomy further proximally, following the medial border of the quadriceps tendon to the muscular insertion of the vastus medialis. It is critical to identify the anatomic boundaries between the vastus lateralis, vastus medialis, and the central rectus femoris tendon to ensure the subsequent incision incorporates the full thickness of the extensor apparatus.
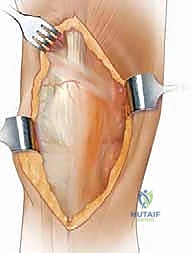
The defining incision of the quadriceps turndown is then made. Starting from the proximal apex of the extended medial arthrotomy, an oblique incision is directed distally and laterally across the quadriceps tendon. This incision is oriented at an angle of approximately 45 degrees, traversing the tendon and extending into the vastus lateralis insertion. This critical cut effectively connects the proximal medial arthrotomy to the previously performed lateral retinacular release, creating an inverted V-shape.

During the lateral extension of this oblique cut, the surgeon must be hyper-vigilant regarding the location of the SLGA. The incision should be planned to remain proximal to the artery's transverse course whenever anatomically possible. Once the full-thickness oblique incision is completed, the entire extensor mechanism—comprising the patella, the patellar tendon, and the distal quadriceps tendon flap—can be gently reflected or "turned down" anterolaterally. This maneuver completely unroofs the anterior compartment of the knee, providing spectacular, unimpeded, orthogonal access to the distal femur and proximal tibia for complex component extraction, meticulous bone preparation, and precise reimplantation of the revision prosthesis.
V-Y Advancement and Extensor Mechanism Repair
Following the successful implantation of the revision TKA components and thorough joint irrigation, the critical phase of extensor mechanism reconstruction commences. The initial step involves a provisional repair of the quadriceps in situ. The apex of the distally based flap is reapproximated to its original proximal position using several heavy, non-absorbable sutures (e.g., #2 or #5 Ethibond or FiberWire). With this provisional anatomical repair in place, the surgeon carefully ranges the knee, assessing the passive flexion arc. If the knee can achieve 90 to 100 degrees of flexion without placing catastrophic tension on the repair or the patellar tendon insertion, the surgeon may elect to close the tendon in this anatomical V-configuration, leaving the lateral release open.
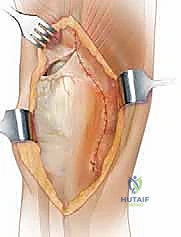
However, in the classic application of the V-Y quadricepsplasty for the severely ankylosed knee, the surgeon actively seeks to lengthen the extensor mechanism to permit greater functional flexion. To achieve this, the provisional apical sutures are removed, and the knee is flexed to the desired postoperative target angle (typically 70 to 90 degrees). As the knee flexes, the proximal V-shaped defect naturally opens, and the distally based flap retracts distally, converting the V-shaped gap into an inverted Y-shape. The apex of the distally based flap is now sutured to the medial and lateral margins of the proximal tendon defect at a more distal location.
This distal advancement typically yields a 1% to 2% functional lengthening of the quadriceps mechanism. The repair is meticulously formalized using a combination of modified Mason-Allen or Krackow locking stitches with heavy, non-absorbable sutures to secure the medial and lateral limbs of the inverted Y. The closure must be watertight and mechanically robust, capable of withstanding the forces of early postoperative rehabilitation. Following the repair, the tourniquet is deflated (if not done previously), meticulous hemostasis is achieved, and the knee is ranged one final time to verify patellar tracking and the structural integrity of the V-Y advancement before layered closure of the subcutaneous tissues and skin.
Complications, Incidence Rates, and Salvage Management
The decision to utilize a V-Y quadricepsplasty is not without significant inherent risks. The most frequent and functionally limiting complication is a postoperative extensor lag. Due to the intentional lengthening of the quadriceps tendon, the mechanical advantage of the extensor mechanism is compromised. Literature reports the incidence of a clinically significant extensor lag (greater than 10 degrees) ranging from 20% to 45% following V-Y quadricepsplasty. While many patients accommodate to a mild lag, severe cases result in a functionally unstable knee, requiring prolonged bracing and aggressive, targeted physical therapy focusing on closed-chain quadriceps strengthening. If the lag is profound and non-recovering, secondary procedures such as extensor mechanism reefing are rarely successful, highlighting the importance of precise intraoperative tensioning.
Vascular compromise leading to patellar osteonecrosis and subsequent fragmentation is a devastating complication unique to extensile exposures that disrupt the peripatellar vascular ring. The combination of a medial parapatellar arthrotomy, a lateral retinacular release, and the proximal transverse incision of the V-Y turndown completely isolates the patella from its superior and medial blood supply. If the superior lateral geniculate artery is inadvertently sacrificed, the incidence of patellar avascular necrosis skyrockets. Clinical presentation includes sudden onset anterior knee pain, crepitus, and radiographic evidence of patellar fragmentation or catastrophic failure of the patellar component. Salvage management in these catastrophic scenarios often necessitates complete patellectomy or complex extensor mechanism reconstruction using massive allografts or synthetic mesh.
Wound healing complications and deep periprosthetic joint infections (PJI) are also statistically elevated in patients undergoing V-Y quadricepsplasty. The extensive subcutaneous dissection required to mobilize the full-thickness flaps, combined with the prolonged operative times and the frequently compromised vascular status of the revision patient, creates a hostile environment for wound healing. Marginal skin necrosis can rapidly progress to full-thickness eschar, exposing the underlying joint capsule and hardware. Aggressive early intervention is mandatory; superficial necrosis requires prompt surgical debridement and potential soft tissue coverage (e.g., medial gastrocnemius rotational flap) to prevent the devastating progression to deep PJI, which would mandate a morbid two-stage revision process.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Extensor Lag (>10 degrees) | 20% - 45% | Intentional lengthening, muscle atrophy, altered biomechanics | Prolonged bracing, aggressive closed-chain PT, rarely surgical reefing |
| Patellar Osteonecrosis / Fracture | 5% - 15% | Disruption of SLGA, excessive devascularization during lateral release | Component removal, patellectomy, extensor mechanism allograft |
| Wound Healing Delay / Necrosis | 10% - 20% | Extensive subcutaneous dissection, prior incisions, poor vascularity | Early aggressive debridement, negative pressure wound therapy, local rotational flaps |
| Extensor Mechanism Rupture | 2% - 5% | Suture pull-out, aggressive early forced flexion, poor tissue quality | Synthetic mesh reconstruction (e.g., Marlex), Achilles tendon allograft |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a V-Y quadricepsplasty deviates significantly from standard primary or routine revision TKA protocols. The overriding principle is the absolute protection of the surgically lengthened and repaired extensor mechanism while simultaneously preventing the recurrence of severe arthrofibrosis. Phase I (0 to 2 weeks postoperatively) focuses on wound healing and strict protection of the repair. The limb is immediately placed in a hinged knee brace locked in full extension. Weight-bearing is typically restricted to toe-touch or partial weight-bearing with assistive devices, depending on the complexity of the bony revision and the security of the diaphyseal stems. Continuous Passive Motion (CPM) machines are highly controversial; if utilized, they are strictly limited to the intraoperatively determined safe arc of flexion (usually 0 to 45 degrees) to prevent catastrophic tension on the V-Y repair.
Phase II (2 to 6 weeks) introduces graduated, heavily monitored range of motion. The hinged brace remains locked in extension for ambulation but is unlocked during supervised physical therapy sessions. Passive and active-assisted flexion is gradually advanced, adding approximately 10 to 15 degrees per week, with a strict prohibition against forced, aggressive passive flexion. Crucially, active open-chain knee extension against gravity or resistance is absolutely contraindicated during this phase to prevent suture pull-out or stretching of the healing tendon. Patients are instructed to perform isometric quadriceps sets and straight-leg raises strictly within the locked brace to maintain basal muscle tone without stressing the repair site.
Phase III (6 to 12 weeks) marks the transition to active extensor mechanism engagement. Provided there is clinical and radiographic evidence of adequate soft tissue healing, the brace may be gradually unlocked for ambulation and eventually weaned entirely. Active knee extension exercises are initiated, starting with short-arc quads and progressing to full active extension. The physical therapist focuses heavily on closed-kinetic-chain exercises (e.g., mini-squats, leg presses with light resistance) to rebuild quadriceps strength and address the inevitable extensor lag. The patient must be counseled that achieving maximum flexion is secondary to regaining functional, active terminal extension.
Phase IV (3 months and beyond) is focused on maximizing functional capacity and managing residual deficits. Patients are cleared for activities of daily living and low-impact exercises. The surgeon and therapist must closely monitor the patient for persistent extensor lag. If a lag of 10 to 15 degrees persists, the patient is educated on compensatory gait mechanics and the continued necessity of lifelong quadriceps strengthening. It is imperative that the patient understands that the ultimate functional outcome following a V-Y quadricepsplasty may take up to 18 to 24 months to fully realize, requiring immense patience and strict adherence to the prescribed rehabilitation continuum.
Summary of Landmark Literature and Clinical Guidelines
The evolution of extensile exposures in total knee arthroplasty is deeply rooted in historical orthopaedic literature. The V-Y quadricepsplasty was originally conceptualized by Coonse and Adams in 1943 for the treatment of severe ankylosis following trauma or infection. However, it was John Insall's seminal modifications in the 1970s and 1980s that adapted the technique specifically for the burgeoning field of total knee arthroplasty. Insall's early reports highlighted the profound ability of the V-Y turndown to provide unparalleled exposure in the stiff knee, though he candidly acknowledged the high incidence of postoperative extensor lag, establishing the foundational biomechanical trade-off that surgeons still navigate today.
Modern comparative literature has extensively evaluated the V-Y quadricepsplasty against alternative extensile techniques, most notably the quadriceps snip and the tibial tubercle osteotomy (TTO). Landmark studies by Garvin et al. and Trousdale et al. have demonstrated that while the quadriceps snip is associated with fewer postoperative complications and requires no alteration in standard rehabilitation, it frequently fails to provide adequate exposure in cases of true ankylosis or when extensor mechanism lengthening is required. Conversely, studies comparing V-Y to TTO indicate that while TTO provides excellent exposure and preserves extensor power (resulting in less lag), it carries a significant risk of proximal tibial fracture and nonunion, particularly in the osteoporotic bone frequently encountered in revision scenarios.
Long-term outcome studies specifically evaluating the survivorship and functional scores of revision TKAs performed via V-Y quadricepsplasty reveal a sobering but realistic clinical picture. Research by Barrack and others indicates that while the survivorship of the revision components is generally comparable to standard revisions, the clinical functional scores (such as the Knee Society Score) are consistently lower in the V-Y cohort. This reduction in functional scoring is almost exclusively driven by the presence of residual extensor lag and diminished quadriceps power. These findings underscore the necessity of reserving the V-Y quadricepsplasty strictly as a salvage maneuver when standard exposures are impossible.
Current clinical consensus guidelines from major orthopaedic societies (such as the American Association of Hip and Knee Surgeons - AAHKS) advocate for a strict, graduated approach to surgical exposure. The guidelines dictate that surgeons should exhaust all standard soft tissue releases and consider a quadriceps snip before escalating to a V-Y turndown or TTO. When an extensile approach is deemed absolutely necessary, the choice between a V-Y and a TTO should be
