Revision Total Knee Arthroplasty for Stiffness: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through revision total knee arthroplasty for stiffness. We cover critical preoperative planning, precise patient positioning, and an exhaustive step-by-step intraoperative technique. Emphasis is placed on meticulous soft tissue release, component removal, bone preparation, and balancing, alongside vital pearls and pitfalls. Postoperative rehabilitation and complication management are also detailed for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The stiff total knee arthroplasty (TKA) represents one of the most formidable and technically demanding challenges encountered by the reconstructive orthopedic surgeon. Unlike revision surgery for aseptic loosening or polyethylene wear, where the primary objective is the restoration of mechanical stability and bone stock, revision for stiffness requires a profound, multi-layered approach to soft tissue management, kinematic restoration, and the meticulous correction of subtle biomechanical errors from the index procedure. A TKA is universally classified as clinically stiff when active knee flexion fails to reach 90 degrees, or when a flexion contracture exceeding 15 degrees persists. This degree of impairment is not merely a numerical deficit; it is a profound functional liability that precludes the patient from executing the basic activities of daily living.
To contextualize the severity of this impairment, one must consider the strict kinematic requirements of human locomotion and daily function. Biomechanical studies consistently demonstrate that approximately 67 degrees of flexion is an absolute prerequisite for normal gait on level ground during the swing phase. Ascending stairs demands a minimum of 83 degrees of flexion, while descending stairs—a task requiring eccentric quadriceps control and greater posterior femoral rollback—necessitates between 90 and 100 degrees of flexion. Furthermore, standing from a standard-height chair requires at least 93 degrees of flexion, and advanced tasks such as tying a shoe demand upwards of 105 degrees. When a patient is restricted to a 70-degree arc of motion, they are effectively rendered disabled, forced into compensatory mechanisms that inevitably lead to secondary pathologies in the ipsilateral hip, contralateral limb, and lumbar spine.
Equally debilitating, and often more biomechanically destructive, are flexion contractures. A contracture exceeding 15 degrees is considered highly pathologic. It severely inhibits the normal biomechanics of the stance phase, forces the quadriceps to fire continuously to prevent collapse, and dramatically increases the energy expenditure of ambulation. This leads to profound fatigue, anterior knee pain, and an inability to stand upright for prolonged periods. The etiology of the stiff TKA is notoriously multifactorial. It requires the surgeon to differentiate between primary arthrofibrosis—an exaggerated, often genetically predisposed fibroblastic response to surgical trauma—and secondary stiffness. Secondary stiffness is typically iatrogenic, stemming from technical errors during the index procedure such as component malrotation, oversizing of the femoral or tibial components, joint line elevation, failure to restore the posterior condylar offset, or inadequate gap balancing. Furthermore, occult periprosthetic joint infection (PJI) must always be considered a primary culprit until definitively ruled out.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical intervention, a masterful command of the altered surgical anatomy is paramount. In the setting of a stiff revision TKA, normal anatomic planes are frequently obliterated by dense, unyielding scar tissue. The surgeon must navigate this hostile environment with a clear three-dimensional understanding of the extensor mechanism, the complex vascular networks, and the critical neurovascular structures that are placed at high risk during aggressive soft tissue releases.
The Extensor Mechanism and Soft Tissue Envelope
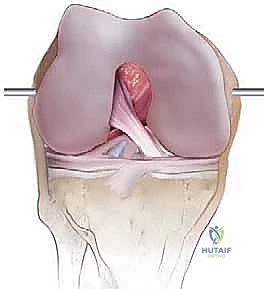
The primary impediment to adequate surgical exposure in a stiff TKA is the contracted, fibrotic extensor mechanism. We must conceptualize the surgical exposure not merely as an incision, but as a progressive, methodical "unleashing" of this mechanism. The extensor apparatus is tethered at four distinct anatomical zones, each requiring specific attention. Proximally, the quadriceps tendon and the muscular bellies of the rectus femoris, vastus medialis, and vastus lateralis become densely adherent to the anterior femur. Medially, the joint capsule, the medial patellofemoral ligament (MPFL) remnants, and the insertion of the vastus medialis obliquus (VMO) form a rigid medial tether. Laterally, the lateral retinaculum and the vastus lateralis insertion contribute to patellar maltracking and limit medial translation during exposure. Distally, the patellar tendon is at extreme risk of avulsion from the tibial tubercle—a catastrophic complication that must be avoided at all costs.
The skin and superficial soft tissue envelope present their own unique challenges. The blood supply to the skin overlying the anterior knee is not axial; rather, it travels perpendicularly from the deeper fascial layers up through the subcutaneous tissues. Consequently, any skin flaps raised during the approach must be full-thickness to preserve the delicate perforating vessels. In patients with multiple prior incisions, densely adherent skin, or a history of infection, the risk of postoperative skin necrosis and subsequent wound dehiscence is exponentially increased. The surgeon must respect the angiosomes of the knee, typically utilizing the most lateral usable prior incision to avoid creating narrow, ischemic skin bridges.
Patellar Vascularity and Neurovascular Considerations
The patella is highly susceptible to avascular necrosis (AVN) following revision TKA, particularly when aggressive soft tissue releases are required. The patellar blood supply is derived from an intricate anastomotic ring formed by the superior medial, superior lateral, inferior medial, and inferior lateral geniculate arteries, with additional contributions from the anterior tibial recurrent artery. The surgical approach inherently disrupts the medial blood supply. If a subsequent lateral retinacular release is performed to correct maltracking or improve exposure, the lateral geniculate contributions are severed, leaving the patella entirely dependent on the tenuous superior and inferior vessels. Extensive subperiosteal dissection or aggressive thermal ablation around the patellar rim must be strictly avoided to preserve this fragile vascular network.
Deep to the posterior capsule lies the popliteal neurovascular bundle, representing the "danger zone" of knee arthroplasty. This bundle, comprising the popliteal artery, popliteal vein, and tibial nerve, is separated from the posterior aspect of the knee joint only by the posterior capsule and a thin layer of adipose tissue. In the stiff knee, particularly when addressing a severe flexion contracture, the posterior capsule becomes contracted and thickened. During posterior capsular release or the removal of posterior femoral osteophytes, extreme caution is mandatory. The common peroneal nerve, coursing laterally around the fibular neck, is also at risk during lateral capsular releases or when correcting severe valgus deformities. Any instrumentation utilized in the posterior compartment must be directed anteriorly and medially, away from these vital structures, relying on careful digital palpation and meticulous, controlled releases.
Exhaustive Indications and Contraindications
The decision to proceed with revision TKA for stiffness is complex and requires a rigorous evaluation of the patient's symptoms, functional deficits, and the underlying etiology of the stiffness. A thorough understanding of the indications and absolute contraindications is essential to optimize patient outcomes and avoid exacerbating the patient's morbidity.
| Category | Specific Criteria / Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | Functional ROM < 90° flexion | Inability to perform ADLs (stairs, sitting, ambulation). |
| Severe Flexion Contracture (>15°) | Causes severe gait dysfunction, quadriceps fatigue, and back pain. | |
| Component Malposition | CT-proven internal rotation of femur/tibia, overstuffing, or joint line elevation causing mechanical block. | |
| Failed Conservative Management | Lack of improvement after aggressive physical therapy, dynamic splinting, and failed Manipulation Under Anesthesia (MUA) or arthroscopic lysis of adhesions. | |
| Relative Contraindications | Poor Patient Motivation / Non-compliance | Post-operative rehab is grueling; non-compliant patients will universally fail and re-stiffen. |
| Severe Neurologic Deficit | Conditions like Parkinson's or severe neuropathy that preclude active participation in rehabilitation. | |
| Complex Regional Pain Syndrome (CRPS) | Surgery may exacerbate the hyperalgesic state; requires aggressive pain management consultation first. | |
| Absolute Contraindications | Active Periprosthetic Joint Infection (PJI) | Requires a formal two-stage exchange arthroplasty; single-stage revision for stiffness in the face of infection is strictly contraindicated. |
| Inadequate Soft Tissue Envelope | Active wound drainage, impending skin necrosis, or lack of coverage requiring flap transfer prior to arthroplasty. | |
| Medically Unstable Patient | Severe cardiopulmonary comorbidities precluding safe administration of anesthesia and surgical stress. |
The most critical step in the evaluation process is the definitive exclusion of periprosthetic joint infection. A stiff knee must be considered an infected knee until proven otherwise. Even in the absence of classic signs such as erythema, fluctuance, or systemic fever, indolent organisms like Cutibacterium acnes or coagulase-negative Staphylococci can present solely as intractable stiffness and pain. A comprehensive serological workup (ESR, CRP) followed by a mandatory diagnostic arthrocentesis is required. The synovial fluid must be analyzed for cell count, differential, and extended aerobic and anaerobic cultures. Only when aseptic etiology is confirmed can the surgeon proceed with planning a single-stage revision for mechanical or fibrotic stiffness.
Pre-Operative Planning, Templating, and Patient Positioning
Success in revision TKA is predicated on exhaustive preoperative planning. The surgeon must enter the operating theater with a comprehensive understanding of the existing implants, the specific mechanisms of failure, and a detailed blueprint for reconstruction, including contingency plans for unexpected bone loss or ligamentous incompetence.
Diagnostic Imaging and Component Analysis
The cornerstone of preoperative planning is a meticulous radiographic evaluation. High-quality standing anteroposterior (AP), lateral, and Merchant (patellofemoral) views are mandatory. On the AP radiograph, the surgeon assesses the overall coronal alignment, the condition of the medial and lateral collateral ligament origins, and any signs of osteolysis or component subsidence. The lateral radiograph is heavily scrutinized for component sizing. An oversized femoral component, particularly in the AP dimension, results in "overstuffing" of the anterior compartment, increasing retinacular tension and physically blocking flexion. Furthermore, the lateral view allows for the assessment of the joint line relative to the fibular head and the inferior pole of the patella. A severe patella baja (inferred by a decreased Insall-Salvati ratio) can severely limit flexion and complicate exposure.





While plain radiographs provide a two-dimensional overview, computed tomography (CT) with metal artifact reduction sequence (MARS) is the gold standard for evaluating component rotation. Internal rotation of the femoral component relative to the surgical transepicondylar axis, or internal rotation of the tibial component relative to the medial third of the tibial tubercle, are prime culprits in the stiff TKA. This malrotation leads to asymmetric gap kinematics, patellar maltracking, and secondary arthrofibrosis. By pinpointing these rotational errors preoperatively, the surgeon can precisely plan the necessary corrective osteotomies or rotational adjustments during reimplantation.



Templating is subsequently performed to anticipate the required revision implants. The surgeon must ensure the availability of a comprehensive revision system, including diaphyseal engaging stems, metaphyseal sleeves or cones for bone loss, and various levels of constraint. While a constrained condylar knee (CCK) is often sufficient once the soft tissues are rebalanced, the surgeon must have a rotating hinge prosthesis available on standby, should the collateral ligaments prove incompetent following extensive debridement and gap balancing.
Patient Positioning and Operating Room Setup
Meticulous patient positioning is critical for optimal surgical exposure and the prevention of intraoperative complications. The patient is placed supine on a radiolucent operating table to allow for intraoperative fluoroscopy if necessary. A bump is placed underneath the ipsilateral hip. This slight internal rotation of the hip is a crucial technical detail; it prevents the natural tendency of the leg to externally rotate, ensuring that the limb rests in a neutral alignment. This neutral position is vital when utilizing extramedullary alignment guides for tibial preparation, preventing inadvertent malrotation of the new tibial baseplate.



A well-padded tourniquet is applied to the proximal thigh, though its inflation may be delayed until component cementation to minimize ischemic time and reduce the risk of postoperative deep vein thrombosis. A robust leg holder or a sterile sandbag is utilized to maintain the knee in varying degrees of flexion during the procedure. The entire limb is prepped and draped in a standard sterile fashion, ensuring access from the anterior superior iliac spine down to the toes, allowing for the assessment of overall limb alignment and rotational profile throughout the surgery.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of a revision TKA for stiffness is an exercise in patience, meticulous dissection, and profound biomechanical understanding. The surgeon must systematically dismantle the fibrotic environment, safely extract the offending hardware, and reconstruct the joint utilizing sound principles of gap balancing and joint line restoration.
Arthrotomy and Extensor Mechanism Management
The surgical approach begins with the skin incision, utilizing the most lateral of the previous anterior incisions to optimize blood supply to the skin flaps. A standard medial parapatellar arthrotomy is initially attempted. However, in the severely stiff knee, the extensor mechanism will resist eversion or lateral subluxation. Forcible eversion must be strictly avoided, as it places catastrophic tension on the patellar tendon insertion. If the patella cannot be easily subluxated laterally, the surgeon must immediately employ extensile measures.


The primary extensile technique is the quadriceps snip. This involves extending the proximal aspect of the medial parapatellar arthrotomy obliquely across the quadriceps tendon, directed towards the vastus lateralis. This simple, highly effective maneuver dramatically reduces tension on the extensor mechanism without altering postoperative rehabilitation protocols. If exposure remains inadequate, a formal tibial tubercle osteotomy (TTO) must be performed. A TTO provides unparalleled access to the joint and protects the patellar tendon, but it requires rigid internal fixation (typically with wires or screws) and necessitates modifications to postoperative weight-bearing and active extension.

Once the joint is accessed, the surgeon undertakes an aggressive, systematic debridement of the arthrofibrotic tissue. The medial and lateral gutters must be meticulously cleared of scar tissue, a process often referred to as "gull-winging" the gutters. The suprapatellar pouch must be re-established, excising all adhesions tethering the quadriceps tendon to the anterior femur. This radical synovectomy and scar excision is often the most critical step in restoring the passive arc of motion.
Component Removal and Joint Debridement
Following adequate exposure, the existing components must be extracted with extreme care to preserve the remaining bone stock. The interfaces between the bone, cement, and prosthesis are disrupted utilizing thin, flexible osteotomes, oscillating saws, and Gigli saws. The surgeon must resist the temptation to lever the components out, as this invariably leads to massive cavitary or segmental bone loss. The femoral component is typically addressed first, followed by the tibial polyethylene insert, which, once removed, provides additional working space to access the tibial baseplate.


Once the implants and all residual cement are removed, the joint is thoroughly irrigated, and the bone beds are assessed. If a flexion contracture was present preoperatively, the posterior capsule must be addressed at this stage. With the knee in flexion, the posterior capsule is carefully elevated off the posterior femur using a curved osteotome or electrocautery, working from the center outward. The surgeon must maintain a healthy respect for the popliteal vessels located immediately posterior to the capsule, ensuring all instruments are directed away from the danger zone. Any residual posterior femoral osteophytes, which can act as a physical block to extension and tent the posterior capsule, must be resected flush with the posterior cortex.
Gap Balancing and Component Reimplantation
The reconstructive phase begins with the establishment of the tibial platform. A revision tibial baseplate with a diaphyseal engaging stem is typically utilized to bypass proximal metaphyseal defects and provide rigid fixation. The tibial cut should be minimal, aiming only to create a flat, stable surface perpendicular to the mechanical axis. Once the tibial trial is in place, the surgeon turns their attention to the femur and the critical task of gap balancing.

The fundamental goal is to create symmetric, rectangular flexion and extension gaps while restoring the native joint line. The joint line is typically located 10 to 15 millimeters proximal to the fibular head. Elevation of the joint line, a common error in the index procedure, leads to mid-flexion instability and patella baja, contributing to stiffness. Distal femoral augments are utilized to restore the joint line to its anatomic position. The flexion gap is then assessed. If the previous femoral component was oversized, a smaller revision component is selected to reduce the AP dimension and decompress the extensor mechanism. Femoral rotation is set parallel to the surgical transepicondylar axis, correcting any internal malrotation from the primary surgery.
Given the extensive soft tissue releases required to overcome stiffness, a standard posterior-stabilized (PS) implant is rarely sufficient. A constrained condylar knee (CCK) prosthesis, featuring a taller, wider tibial post and a deeper femoral box, is typically required to provide varus-valgus stability. If the collateral ligaments are entirely attenuated or absent, a rotating hinge prosthesis becomes mandatory. Once the trials are perfectly balanced, the final components are cemented into place, utilizing stems to achieve diaphyseal fixation and offload the compromised metaphyseal bone.
Complications, Incidence Rates, and Salvage Management
Revision TKA for stiffness carries a significantly higher complication profile compared to primary arthroplasty or revision for aseptic loosening. The surgeon must be acutely aware of these risks and possess the technical repertoire to manage them effectively.
| Complication | Estimated Incidence | Mechanism / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Stiffness | 15% - 30% | Genetic predisposition to arthrofibrosis, inadequate intraoperative release, poor postoperative pain control leading to therapy non-compliance. | Aggressive early MUA (within 6 weeks). Arthroscopic lysis of adhesions. In refractory cases, acceptance of limited ROM. |
| Extensor Mechanism Disruption | 1% - 3% | Excessive tension during exposure, avulsion of patellar tendon, failure of quadriceps snip/TTO repair. | Catastrophic complication. Requires primary repair with robust augmentation (e.g., Marlex mesh, allograft) and prolonged immobilization. |
| Periprosthetic Joint Infection | 3% - 7% | Prolonged operative time, extensive soft tissue dissection, compromised skin flaps, multiple prior surgeries. | Acute: Debridement, antibiotics, and implant retention (DAIR). Chronic: Two-stage exchange arthroplasty |
