Extensile Exposure in Revision TKA: Mastering the Tibial Tubercle Osteotomy

Key Takeaway
This masterclass details the tibial tubercle osteotomy (TTO) for extensile exposure during revision total knee arthroplasty (TKA). We'll cover comprehensive anatomical considerations, precise patient positioning, and a step-by-step intraoperative guide, emphasizing meticulous soft tissue releases and advanced osteotomy techniques. Learn crucial pearls and pitfalls, ensuring robust fixation and optimal postoperative recovery to mitigate complications like extensor lag.
Comprehensive Introduction and Patho-Epidemiology
The landscape of adult reconstruction is rapidly evolving, with the burden of revision total knee arthroplasty (TKA) projected to grow exponentially over the next decade. As orthopedic surgeons, we are increasingly confronted with complex revision scenarios characterized by profound arthrofibrosis, compromised soft tissue envelopes, and well-fixed implants that demand extraction. In these hostile surgical environments, achieving adequate exposure without compromising the integrity of the extensor mechanism is the paramount challenge. The catastrophic complication of patellar tendon avulsion during forced eversion of a stiff patella is a devastating event that permanently alters the patient's functional trajectory. To circumvent this, the armamentarium of the revision arthroplasty surgeon must include mastery of extensile exposure techniques.
Among the available options for extensile exposure—namely the rectus snip (quadriceps snip), the V-Y quadriceps turndown, and the Tibial Tubercle Osteotomy (TTO)—the TTO has emerged as the gold standard for cases requiring maximal distal and proximal access. The patho-epidemiology of the stiff, multiply-operated knee dictates that the soft tissues are often inelastic, scarred, and contracted. While a quadriceps snip is excellent for mild to moderate stiffness, it offers limited assistance when the primary restriction is distal, such as in cases of patella baja or severe infrapatellar scarring. Conversely, the V-Y turndown, while providing excellent exposure, is historically associated with a high incidence of postoperative extensor lag, profound quadriceps weakness, and disruption of the extensor mechanism's vascularity.
The Tibial Tubercle Osteotomy, when executed with meticulous technique, offers a superior biomechanical and biological solution. By osteotomizing the bony insertion of the patellar tendon and maintaining a lateral periosteal hinge, the surgeon preserves the continuity of the extensor mechanism. This allows for bone-to-bone healing, which is inherently more robust and predictable than tendon-to-tendon or tendon-to-bone healing. Furthermore, the TTO provides unparalleled access to the proximal tibia and distal femur, facilitating the safe extraction of long-stemmed components and the management of massive metaphyseal bone loss.
Mastering the TTO requires not only technical precision but also a profound understanding of the underlying patho-anatomy. The surgeon must navigate altered joint lines, osteolytic defects, and distorted neurovascular anatomy. This chapter will serve as an exhaustive, step-by-step masterclass on the Tibial Tubercle Osteotomy, detailing the anatomical considerations, preoperative planning, precise surgical execution, rigid fixation techniques, and the management of potential complications.
Detailed Surgical Anatomy and Biomechanics
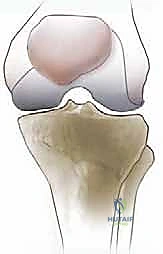
A profound mastery of the anterior knee anatomy and the biomechanics of the extensor mechanism is non-negotiable before undertaking a Tibial Tubercle Osteotomy. The extensor mechanism is not merely a collection of tendons and bone; it is a highly dynamic, load-bearing unit that transmits immense forces—often exceeding several times body weight—across the patellofemoral joint during routine activities like stair climbing and rising from a chair.
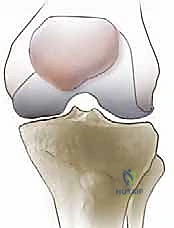
The Extensor Mechanism and Patellofemoral Articulation
The extensor mechanism comprises the quadriceps femoris musculature (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius), the quadriceps tendon, the patella, the patellar ligament (tendon), and the medial and lateral retinaculae. The patella acts as a crucial fulcrum, increasing the moment arm of the quadriceps force and thereby enhancing the mechanical advantage of knee extension. In the revision setting, the normal excursion of these structures is often obliterated by dense, unyielding scar tissue.
The patellar tendon itself is a robust, inelastic structure that originates from the inferior pole of the patella and inserts broadly onto the proximal and anterior aspect of the tibial tuberosity. The strength of this insertion is critical. The TTO leverages the principle that it is far safer to move the bony attachment of the tendon than to risk avulsing the tendon from the bone or stretching it beyond its physiological limits.
Osteology and Vascularity of the Tibial Tuberosity
The tibial tuberosity is a distinct triangular prominence located on the proximal, anterior aspect of the tibial diaphysis. It is characterized by a proximal smooth area, which serves as the primary footprint for the patellar tendon, and a distal rough area that is subcutaneous.
When designing the osteotomy, we must consider the vascular supply to the anterior tibia and the extensor mechanism. The primary blood supply to the patella and the anterior soft tissues is derived from an anastomotic ring fed by the superior and inferior genicular arteries, as well as the anterior tibial recurrent artery. A critical tenet of the TTO is the preservation of the lateral periosteal hinge. By leaving the lateral muscular and periosteal attachments intact (specifically the origin of the tibialis anterior muscle), we preserve the vascularity to the osteotomized bone fragment, drastically reducing the risk of non-union or avascular necrosis.
Neurovascular Proximity and Biomechanical Considerations
While the anterior surgical field of a TTO is relatively devoid of major neurovascular bundles, the surgeon must remain hyper-vigilant regarding peripheral structures. Medially, the saphenous nerve and great saphenous vein course distally. Subperiosteal dissection on the medial aspect of the tibia must be meticulous to avoid iatrogenic injury to these structures, which can result in painful neuromas or medial-sided numbness. Posterolaterally, the common peroneal nerve wraps around the fibular neck; while not directly in the operative field, excessive lateral retraction or prolonged limb malpositioning can induce traction neuropraxias.
Biomechanically, the fixation of the TTO must counteract immense forces. During active knee extension, the osteotomized fragment experiences massive tensile forces pulling it proximally. During knee flexion, particularly deep flexion, the fragment is subjected to shear and compressive forces against the tibial shaft. Therefore, the fixation construct—whether utilizing cerclage wires, cables, or cortical screws—must be biomechanically rigid enough to neutralize these multi-planar forces and maintain absolute stability until osseous union occurs.
Exhaustive Indications and Contraindications
The decision to proceed with a Tibial Tubercle Osteotomy should be made judiciously. It is not a routine maneuver but rather a powerful salvage technique reserved for specific, high-complexity scenarios where standard exposure is impossible or unsafe. The threshold for performing a TTO varies among surgeons, but the universal trigger is the inability to evert or laterally subluxate the patella without placing undue tension on the patellar tendon insertion.
Primary Indications for TTO
The classic indication for a TTO is the stiff, multiply-operated knee requiring revision arthroplasty. Patients presenting with severe arthrofibrosis, a preoperative range of motion less than 70 degrees, or patella baja are prime candidates. In patella baja, the shortened patellar tendon makes eversion nearly impossible; the TTO not only facilitates exposure but can also be utilized to proximally advance the tubercle, correcting the baja and restoring appropriate patellofemoral kinematics.
Furthermore, the TTO is exceptionally valuable when dealing with well-fixed, long-stemmed tibial components. Extracting a fully porous-coated or cemented long stem through a standard superior approach often results in catastrophic tibial bone loss or fracture. The TTO provides direct, anterior access to the implant-bone interface, allowing the surgeon to use high-speed burrs, flexible osteotomes, or ultrasonic tools to disrupt the fixation under direct visualization, thereby preserving the native tibial bone stock.
Contraindications and Risk Stratification
Despite its utility, the TTO is not universally applicable. The most significant absolute contraindication is the presence of an active, untreated local infection, as creating a fresh osteotomy in an infected field invites osteomyelitis and guarantees failure.
Relative contraindications revolve around the mechanical integrity of the proximal tibia. Severe tibial osteopenia, profound osteolysis from wear debris, or a history of previous proximal tibial fractures can compromise the structural integrity of the osteotomized fragment. If the bone is too thin or structurally deficient, it will likely fracture during the osteotomy or fail to hold the fixation hardware, leading to proximal migration of the extensor mechanism.
| Category | Specific Condition | Rationale / Clinical Consequence |
|---|---|---|
| Indications | Severe Arthrofibrosis / Stiff Knee | Allows exposure without risking patellar tendon avulsion. |
| Indications | Patella Baja | Facilitates exposure and allows for proximal advancement of the tubercle. |
| Indications | Well-fixed Tibial Stem Extraction | Provides direct anterior access to the implant-bone interface, preserving bone stock. |
| Indications | Massive Metaphyseal Bone Loss | Allows for the safe placement of metaphyseal cones or sleeves under direct vision. |
| Absolute Contraindications | Active Local Infection | High risk of introducing infection into the osteotomy site, leading to osteomyelitis. |
| Relative Contraindications | Severe Tibial Osteopenia | High risk of fragment fracture or failure of fixation hardware. |
| Relative Contraindications | Massive Anterior Osteolysis | Insufficient bone stock to create a viable osteotomy block. |
| Relative Contraindications | Compromised Anterior Soft Tissues | High risk of wound breakdown, skin necrosis, and exposed hardware. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complex revision TKA utilizing a TTO is heavily predicated on meticulous preoperative planning. The surgeon must anticipate the challenges of exposure, implant extraction, and subsequent fixation long before the patient enters the operating theater.
Advanced Imaging and Templating
Standard anteroposterior and lateral radiographs are the baseline, but they are often insufficient for complex revisions. High-quality, digitally templated radiographs are essential to assess the length and diameter of existing stems, the extent of osteolysis, and the quality of the anterior tibial cortex. The length of the planned osteotomy must be templated to ensure it bypasses the most well-fixed portion of the existing tibial stem, typically requiring a length of 8 to 10 centimeters.
In cases of massive bone loss or distorted anatomy, a CT scan with metal artifact reduction software (MARS) is invaluable. This allows for 3D visualization of the tibial tubercle's bone stock, ensuring there is sufficient thickness (ideally >1.5 cm) to create a robust bony fragment that can withstand the forces of early rehabilitation.
Patient Positioning and Surgical Preparation
Patient positioning must facilitate both standard arthroplasty maneuvers and the specific demands of the extensile approach. The patient is placed supine on a radiolucent operating table to allow for intraoperative fluoroscopy if needed. A pneumatic tourniquet is applied to the proximal thigh. While some surgeons prefer a tourniquet-less approach to minimize ischemic complications, in a complex revision with a TTO, a tourniquet is often inflated to 300-350 mmHg to ensure pristine visualization during the delicate osteotomy cuts and implant extraction.
Leg stabilization is critical. A lateral thigh post or a specialized leg holder is utilized to control rotation, and a distal sandbag or foot peg is placed to prevent the leg from sliding distally during vigorous extraction maneuvers. The entire limb is prepped and draped free, from the toes to the proximal thigh, ensuring that the surgeon can manipulate the knee through a full range of motion. Careful attention must be paid to previous surgical scars; the incision should ideally incorporate the most lateral, well-healed previous incision to minimize the risk of skin necrosis, maintaining as broad a skin bridge as possible.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the Tibial Tubercle Osteotomy is a highly orchestrated sequence of events. We begin with standard releases, escalating to the osteotomy only when the soft tissue envelope dictates its necessity.
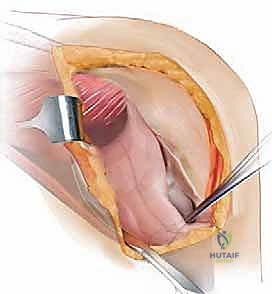
Phase 1: Initial Soft Tissue Release and Arthrotomy
We typically utilize a standard medial parapatellar incision, extending it proximally into the quadriceps tendon and distally 8 to 10 cm below the tibial tubercle to accommodate the planned osteotomy. The arthrotomy is performed, and we immediately encounter the dense fibrous pseudocapsule characteristic of revision scenarios.
Our first objective is to mobilize the suprapatellar pouch. Using electrocautery, we meticulously dissect the adhesions binding the quadriceps tendon to the anterior femur. This restores the proximal excursion of the extensor mechanism.
Next, we address the lateral gutter. Dense fibrous bands often tether the patella to the lateral femoral condyle, preventing medial translation and eversion. These must be sharply excised, freeing the lateral retinaculum from the underlying capsule.
We then proceed to a comprehensive medial release. Using a Cobb elevator, we perform a subperiosteal elevation of the medial retinaculum and the deep medial collateral ligament.

This dissection must be carried posteriorly around the proximal tibia, reaching the insertion of the semimembranosus. This maneuver is critical; it allows the tibia to externally rotate, significantly reducing tension on the extensor mechanism.

The medial pseudocapsule, often thickened and unyielding, is completely excised to recreate the medial gutter.
Finally, we identify the interval between the patellar tendon and the infrapatellar fat pad. The fat pad is often fibrotic and contracted. We carefully release the inferior pole of the patella and excise the retropatellar scar tissue down to the tibial tubercle.
If, after these exhaustive releases, the patella cannot be safely everted or laterally subluxated past the midline of the lateral femoral condyle without undue tension on the patellar tendon, we commit to the Tibial Tubercle Osteotomy.
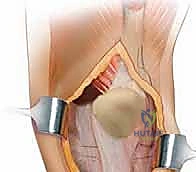
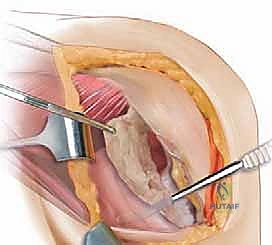
Phase 2: Executing the Tibial Tubercle Osteotomy
The osteotomy must be precise. We mark the planned cuts with electrocautery. The osteotomy should be 8 to 10 cm in length to ensure a massive surface area for healing and to bypass existing tibial stems. The width should be approximately 2 cm, encompassing the entire footprint of the patellar tendon.
Using an oscillating saw, we initiate the medial cut. The saw blade is directed laterally and slightly posteriorly. It is imperative to angle the cut to create a broad, flat surface, avoiding a steep V-shape which is prone to fracture. The distal aspect of the osteotomy must be tapered—or "feathered"—into the anterior tibial cortex to prevent a sharp stress riser that could precipitate a postoperative tibial shaft fracture.
As the saw cut deepens, we transition to wide, flexible osteotomes. This prevents thermal necrosis from the saw blade and allows for tactile feedback. We carefully lever the osteotome to complete the bone cut, ensuring we do not violate the lateral periosteum.

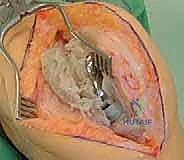
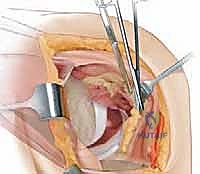
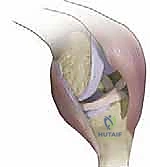
The crucial step is the mobilization of the fragment. We gently pry the osteotomized tubercle laterally, opening it like a book. The lateral periosteum and the anterior tibial musculature act as a living hinge. This hinge preserves the blood supply to the bone fragment, which is the biological cornerstone of a successful TTO.
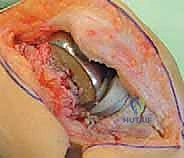
With the tubercle mobilized laterally, we now have unparalleled, extensile exposure of the entire knee joint, allowing for safe extraction of implants, thorough debridement, and precise reimplantation of revision components.
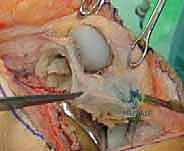
Phase 3: Rigid Fixation of the Osteotomy
Following the successful implantation of the revision TKA components, the TTO must be anatomically reduced and rigidly fixed. The bone surfaces are cleared of any debris or cement. The tubercle is reduced back to its anatomical bed. If patella baja was present preoperatively, the fragment can be advanced proximally by 1 to 1.5 cm before fixation.
We prepare for fixation by utilizing heavy reduction forceps to hold the fragment in absolute compression against the tibial shaft.
Fixation can be achieved with heavy-gauge cerclage wires, braided cables, or cortical screws. In cases with a stemmed tibial implant, passing screws through the bone and around the stem can be challenging; therefore, cerclage wires or cables are often preferred. We typically use two to three 18-gauge cerclage wires or Luque wires.
The wires are passed through drill holes in the lateral tibial cortex, routed medially across the anterior surface of the reduced tubercle, and tightened using a wire tensioner.

The tension must be sufficient to achieve absolute rigid compression, eliminating any micromotion that could lead to non-union. The knots or crimps are carefully buried in the soft tissue to prevent skin irritation.

Once the fixation is complete, we test the construct by taking the knee through a full range of motion, observing the osteotomy site for any gapping or instability. The soft tissues are then meticulously closed in layers over a closed suction drain to prevent hematoma formation, which can compromise the delicate anterior skin envelope.

Complications, Incidence Rates, and Salvage Management
While the Tibial Tubercle Osteotomy is an incredibly powerful tool, it is not without significant risks. The surgeon must be acutely aware of potential complications, their incidence rates, and the appropriate salvage strategies. Informed consent must explicitly cover these risks, as they can drastically alter the postoperative recovery.
Bony and Mechanical Complications
The most feared mechanical complication is proximal migration of the osteotomized fragment, which occurs in 1% to 3% of cases. This is typically the result of technical errors, such as inadequate fixation, a fragment that is too thin, or aggressive early postoperative flexion against resistance. If proximal migration occurs, it results in a profound extensor lag and requires immediate reoperation for revision fixation, often necessitating the use of tension band wiring or even extensor mechanism allograft reconstruction if the bone fragment is destroyed.
Non-union of the osteotomy site is reported in 1% to 4% of cases. This risk is heavily mitigated by preserving the lateral periosteal hinge and ensuring rigid, compressive fixation. Non-unions are often asymptomatic if fibrous stability is achieved, but painful non-unions require bone grafting and revision internal fixation.
Fracture of the tibial shaft distal to the osteotomy (stress riser fracture) is a devastating complication. This highlights the critical importance of "feathering" or tapering the distal aspect of the osteotomy cut to smoothly transition stress forces. If a fracture occurs, it must be addressed with long-stemmed revision implants or lateral locked plating.
Soft Tissue and Wound Complications
The anterior aspect of the knee has a notoriously tenuous blood supply, making wound complications a significant concern. Skin necrosis over the prominent hardware or the osteotomy site occurs in up to 5% of cases. Careful handling of the soft tissues, utilizing full-thickness flaps, and burying wire knots are essential preventive measures. If superficial necrosis occurs, aggressive wound care is required; deep necrosis exposing hardware or bone necessitates urgent debridement and often requires a medial gastrocnemius rotational flap for coverage.
| Complication | Estimated Incidence | Primary Prevention Strategy | Salvage Management |
|---|---|---|---|
| Proximal Migration | 1% - 3% | Rigid fixation (cables/wires), adequate fragment thickness (>1.5cm). | Reoperation, revision fixation, possible extensor mechanism allograft. |
| Non-Union | 1% - 4% | Preserve lateral periosteal hinge, absolute rigid compression. | Bone grafting, revision internal fixation. |
| Tibial Shaft Fracture | < 2% | Taper/feather the distal osteotomy cut; avoid sharp transverse cuts. | Lateral locked plating, long-stemmed revision TKA. |
| Wound Necrosis | 2% - 5% | Full-thickness flaps, meticulous closure, bury hardware knots. | Local wound care, medial gastrocnemius rotational flap. |
| Patellar Tendon Avulsion | < 1% | Avoid excessive tension; perform TTO before forced eversion. | Primary repair with Marlex mesh augmentation or allograft. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a TTO in a revision TKA is a delicate balancing act. The surgeon must protect the osteotomy site from catastrophic failure while simultaneously preventing the recurrence of severe arthrofibrosis. Communication with the physical therapy team is paramount; they must understand that this is not a standard primary TKA protocol.
Phase I: Maximum Protection (Weeks 0-2)
Immediately postoperatively, the patient is placed in a hinged knee brace locked in full extension. This neutralizes the tensile forces of the quadriceps on the osteotomy fragment. Weight-bearing is typically restricted to toe-touch (TTWB) or partial weight-bearing (PWB) with an assistive device, depending on the rigidity of the fixation and the quality of the host bone.
