Revision Total Knee Arthroplasty: Mastering Tibial Bone Loss with Metal Augments

Key Takeaway
Join us in the OR for an immersive masterclass on revision total knee arthroplasty for proximal tibial bone loss. We'll meticulously cover preoperative planning, critical surgical anatomy, and a granular, step-by-step intraoperative execution using metallic augments. Learn to classify defects, manage neurovascular risks, and apply advanced techniques to restore knee function, along with essential pearls, pitfalls, and postoperative care.
Comprehensive Introduction and Patho-Epidemiology
Revision Total Knee Arthroplasty (TKA) represents one of the most formidable challenges in modern orthopedic surgery, demanding a synthesis of meticulous preoperative planning, profound anatomic knowledge, and exacting intraoperative execution. As the volume of primary TKAs continues to grow exponentially, driven by an aging population and expanding indications in younger, more active cohorts, the commensurate burden of revision procedures is rising in parallel. Among the myriad complexities encountered during revision arthroplasty, the management of significant proximal tibial bone loss stands paramount. This bone deficiency compromises the foundational support required for the tibial component, threatening the restoration of the joint line, coronal and sagittal alignment, and ultimately, the longevity of the reconstructive construct.
The pathophysiology of periprosthetic tibial bone loss is multifactorial, typically culminating from a cascade of mechanical and biological phenomena. Aseptic loosening, the most prevalent etiology, often initiates via particulate wear debris—primarily ultra-high-molecular-weight polyethylene (UHMWPE), polymethylmethacrylate (PMMA) cement, or metallic ions. These particulates incite a macrophage-mediated inflammatory response, leading to the local release of osteolytic cytokines (such as TNF-alpha, IL-1, and RANKL) and subsequent aggressive focal osteolysis. Furthermore, stress shielding beneath rigid tibial trays, particularly in the presence of robust diaphyseal stems, can lead to adaptive bone resorption in the proximal metaphysis. Other significant contributors include the destructive sequelae of periprosthetic joint infection (PJI), iatrogenic bone loss during the explantation of well-fixed primary components, and periprosthetic fractures compromising the metaphyseal envelope.
Historically, the armamentarium for managing these tibial defects included cement mantles augmented with screws, custom-fabricated implants, and structural bulk allografts. While cement alone is adequate for minimal defects (less than 5 mm), its use in larger voids is associated with high rates of thermal necrosis, cement mantle fracture, and premature catastrophic failure. Structural allografts, though biologically appealing for bone stock restoration, are plagued by risks of nonunion, late resorption, disease transmission, and technically demanding intraoperative shaping. Consequently, the advent of modular metallic augments revolutionized the management of contained and uncontained metaphyseal defects.
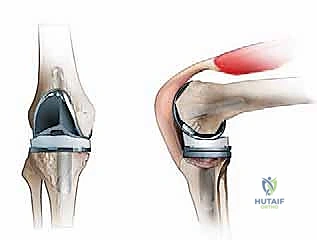
Modular metallic augments—typically fabricated from titanium alloys or highly porous tantalum—offer immediate structural support, precise modularity, and reproducible intraoperative application. They effectively bypass deficient metaphyseal bone, transferring axial and shear loads to more distal, competent host bone when used in conjunction with diaphyseal engaging stems. This chapter provides an exhaustive, step-by-step masterclass on the evaluation, classification, and surgical management of proximal tibial bone loss using metallic augments, equipping the reconstructive surgeon with the requisite knowledge to achieve stable, durable outcomes in the most challenging revision scenarios.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the native and altered surgical anatomy of the knee is non-negotiable for the revision arthroplasty surgeon. The proximal tibia is a complex, asymmetric structure designed to withstand immense dynamic loads while facilitating a wide arc of motion. In the coronal plane, the native tibial plateau exhibits a subtle 3-degree varus slope relative to the mechanical axis of the tibia, which harmonizes with the corresponding valgus alignment of the distal femur. In the sagittal plane, the proximal tibia demonstrates a posterior slope ranging from 4 to 12 degrees (averaging 9 to 10 degrees). This posterior slope is crucial for maximizing knee flexion and optimizing the biomechanics of the cruciate ligaments, particularly the posterior cruciate ligament (PCL) in cruciate-retaining designs, though in revision scenarios utilizing stemmed, constrained constructs, a neutral slope is frequently targeted.
Biomechanically, the load distribution across the proximal tibia is decidedly asymmetric. During the normal gait cycle, the mechanical axis passes medial to the center of the knee joint, resulting in approximately 60% to 70% of the compressive ground reaction forces being transmitted through the medial tibial plateau. This physiological loading pattern dictates the microarchitectural density of the subchondral and metaphyseal trabecular bone, which is significantly denser and more robust medially than laterally. Consequently, while the medial plateau is more resistant to central osteolytic cavitation, the higher stress concentrations make it highly susceptible to peripheral collapse and uncontained defects when the cortical rim is compromised. Conversely, the less dense lateral plateau is frequently the site of profound, expansive osteolysis, particularly in the setting of long-standing varus deformity or lateral compartment wear.
The neurovascular topography posterior to the proximal tibia is of paramount concern during revision TKA, particularly during aggressive debridement, reaming, and resection of the posterior tibial plateau. The popliteal artery and vein are tethered in close proximity to the posterior capsule. In full extension, these critical vessels lie merely 3 to 12 mm posterior to the articular surface. Flexing the knee to 90 degrees allows the vessels to fall posteriorly, increasing this safety margin to 6 to 15 mm. However, the presence of dense scar tissue, posterior capsular contractures, or extrusive osteophytes can distort this anatomy, tethering the vessels dangerously close to the resection plane. The surgeon must remain acutely vigilant, utilizing protective posterior retractors and avoiding any posterior plunging of the oscillating saw.
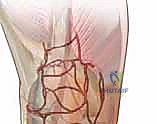
The vascular supply to the proximal tibia is dual-sourced, comprising both endosteal and periosteal networks. The endosteal supply relies on the nutrient artery, a branch of the posterior tibial artery, which enters the posterior cortex distal to the soleal line. The periosteal supply is a rich anastomotic network fed by the medial and lateral inferior genicular arteries, as well as the anterior recurrent tibial artery. Extensive periosteal stripping during revision exposure can severely compromise the viability of the remaining metaphyseal shell, hindering the potential for biologic incorporation of bone grafts or highly porous implants. Therefore, dissection must be judicious, preserving the soft tissue envelope whenever feasible.


Exhaustive Indications and Contraindications
The decision-making algorithm for addressing tibial bone loss hinges upon accurate, reproducible classification of the defect. The Anderson Orthopaedic Research Institute (AORI) bone defect classification system remains the gold standard, providing a pragmatic framework based on radiographic and intraoperative assessment of metaphyseal bone integrity. The AORI system dictates whether a defect can be managed with standard components, requires modular augments, or necessitates massive structural allografts or highly porous metaphyseal cones and sleeves.
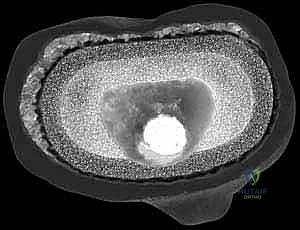
AORI Type I (TI) defects are characterized by intact metaphyseal bone with preserved cortical containment. The primary joint line is generally unaltered, and there is no significant component subsidence. These defects are typically small, central cavitary lesions resulting from localized osteolysis or minor iatrogenic damage during component extraction. Because the structural integrity of the metaphysis is robust, these defects do not require metallic augmentation. They are optimally managed with particulate cancellous autograft (from the revision cuts), allograft, or simply filled with PMMA cement, provided the cement mantle does not exceed 5 mm in thickness.
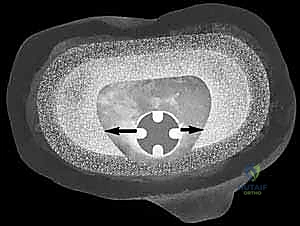
AORI Type II (TII) defects represent the primary indication for the utilization of modular metallic augments. These defects are defined by damaged or deficient metaphyseal bone, leading to component subsidence and alteration of the joint line. They are subdivided into TIIA (involving one condyle, usually the medial) and TIIB (involving both condyles). While the metaphyseal cancellous bone is compromised, the peripheral cortical rim and the insertions of the collateral ligaments remain largely intact. Modular metallic augments—available as blocks (step-cuts) or wedges—are specifically engineered to fill these defects, reconstituting the metaphyseal platform and restoring the joint line. Wedges are particularly useful for angular defects, while blocks provide excellent support for step-off defects and offer superior resistance to shear forces.
AORI Type III (TIII) defects are catastrophic, characterized by massive deficiency of the proximal metaphyseal segment, often accompanied by complete loss of cortical containment, collateral ligament detachment, and potential compromise of the extensor mechanism (tibial tubercle avulsion). In these severe scenarios, standard modular metallic augments are generally insufficient on their own, as there is inadequate host bone to support the augment-tray construct, even with a diaphyseal stem. TIII defects necessitate advanced reconstructive techniques, such as highly porous tantalum cones, titanium metaphyseal sleeves, structural bulk allografts, or, in extreme cases, tumor-type mega-prostheses.

| Parameter | Indications for Metallic Augments | Contraindications for Metallic Augments |
|---|---|---|
| AORI Classification | Type IIA, Type IIB | Type I (use cement/graft), Type III (requires cones/sleeves/allograft) |
| Defect Morphology | Contained or uncontained defects < 15-20 mm depth | Massive, uncontained defects > 20 mm depth lacking cortical rim |
| Ligamentous Status | Intact collateral ligament insertions | Complete loss of metaphyseal bone supporting collateral insertions |
| Infection Status | Aseptic loosening, or 2nd stage of PJI revision | Active Periprosthetic Joint Infection (PJI) |
| Bone Quality | Adequate diaphyseal bone for stem engagement | Severe diaphyseal osteomyelitis or obliterative osteopetrosis |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a revision TKA is largely predetermined before the patient enters the operating theater. Meticulous preoperative planning is the blueprint that guides implant selection, anticipates intraoperative challenges, and formulates contingency plans. The surgeon must act as a detective, obtaining the operative notes and implant records from the primary surgery whenever possible. Knowing the exact make, model, and size of the existing implants is critical for selecting the appropriate extraction tools and anticipating the specific patterns of bone loss associated with that implant's failure mode.
Radiographic evaluation must be exhaustive. A standard series includes weight-bearing anteroposterior (AP), lateral, and Merchant (patellofemoral) views. Full-length standing hip-to-ankle radiographs are mandatory to assess the overall mechanical axis, identify extra-articular deformities, and evaluate the diaphyseal anatomy for stem bowing and canal diameter. The surgeon must scrutinize these images for radiolucent lines indicating aseptic loosening, focal osteolysis, component subsidence, and the status of the cortical bone. If infection is suspected, a complete serological workup (ESR, CRP) and joint aspiration for cell count, differential, and extended cultures must be performed prior to any definitive surgical intervention.
Digital templating is a non-negotiable step in the preoperative workflow. Modern templating software allows the surgeon to superimpose revision implant templates over scaled radiographs. The primary goals of templating the tibia include determining the optimal size of the tibial tray to maximize cortical coverage without overhang, estimating the size and location of required metallic augments, and selecting the appropriate stem length and diameter. The stem must bypass the metaphyseal defect and engage the intact diaphyseal isthmus by at least 4 to 6 centimeters. Crucially, templating aids in planning the restoration of the joint line. The tip of the fibular head serves as a highly reliable, reproducible bony landmark; the native joint line typically lies 10 to 15 mm proximal to the fibular head apex.

Patient positioning must facilitate both excellent surgical exposure and intraoperative radiographic assessment. The patient is positioned supine on a radiolucent operating table. A standard leg holder or a lateral post is utilized, ensuring the knee can be freely manipulated through a full arc of motion, from hyperextension to maximum flexion (at least 120 degrees). A sterile tourniquet is applied high on the proximal thigh, though its inflation may be delayed or entirely avoided in patients with severe peripheral vascular disease or those requiring extensive soft tissue releases, to prevent ischemic complications and allow for continuous assessment of tissue perfusion. A fluoroscopy unit (C-arm) must be readily available and draped, positioned on the contralateral side to allow for orthogonal views of the diaphyseal stem engagement and augment seating without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
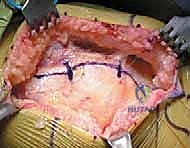
The surgical approach in revision TKA must balance the need for extensive exposure with the imperative to preserve the vascularity of the extensor mechanism and the remaining bone stock. We typically utilize the previous midline longitudinal incision, extending it proximally and distally into virgin tissue to avoid skin necrosis at the apices. A standard medial parapatellar arthrotomy is the workhorse approach. However, due to dense arthrofibrosis and patellar entrapment, eversion of the patella is frequently difficult and places the patellar tendon insertion at risk of catastrophic avulsion. In such instances, the surgeon must seamlessly transition to extensile measures. A quadriceps snip is the preferred first-line extensile approach, providing excellent exposure with minimal impact on postoperative rehabilitation. If exposure remains inadequate, a tibial tubercle osteotomy (TTO) should be performed, securing a robust, 6-8 cm bone block that can be rigidly repaired with wires or screws at the conclusion of the procedure.
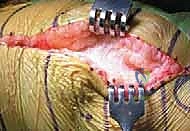
Component extraction is the most critical phase for bone preservation. Aggressive, impatient removal of well-fixed components will convert a manageable AORI Type II defect into a devastating Type III defect. The modular polyethylene insert is removed first to enhance visualization. For the tibial tray, thin, flexible osteotomes, oscillating saw blades, and Gigli saws are meticulously passed along the implant-cement or cement-bone interfaces. The surgeon must work circumferentially, progressively disrupting the interface until the component can be extracted with minimal force. Specialized extraction devices, such as slap hammers and dedicated implant-specific extractors, should be used judiciously, applying in-line traction to avoid fracturing the fragile metaphyseal shell.
Once the components and residual cement are removed, aggressive debridement of all fibrous tissue, granulomatous membranes, and osteolytic debris is performed using curettes and pulsed lavage. At this juncture, the AORI classification is definitively confirmed via direct visualization. The tibial resection is then performed using an intramedullary referencing guide. The goal is to create a clean, flat, viable bone bed while resecting the absolute minimum amount of host bone—typically aiming for a 2 mm resection below the deepest point of the intact plateau. The resection is made perpendicular to the mechanical axis in the coronal plane. In the sagittal plane, a neutral (0-degree) slope is generally targeted to accommodate the rigid diaphyseal stem and the constrained articulation typically required in revision settings.
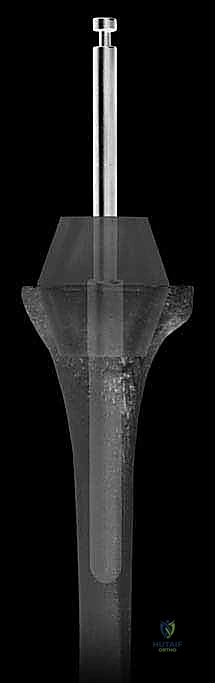
Canal preparation and stem trialing follow the initial resection. Sequential intramedullary reaming is performed, starting with a small diameter and progressing until rigid diaphyseal cortical chatter is achieved. The depth of reaming must correspond to the templated stem length, ensuring adequate bypass of the metaphyseal defect. Once the canal is prepared, a trial stem is inserted, and the tibial trial tray is applied. The defect is now reassessed to determine the exact dimensions of the required metallic augment. Trial augments (blocks or wedges) are attached to the trial tray, and the construct is seated. The surgeon evaluates the stability of the construct, the restoration of the joint line relative to the fibular head, and the rotational alignment of the tray (typically referencing the medial third of the tibial tubercle). If the diaphyseal canal is offset relative to the center of the metaphysis—a common scenario in severe deformities—an offset stem adapter must be utilized to ensure optimal cortical coverage of the tray without overhang.
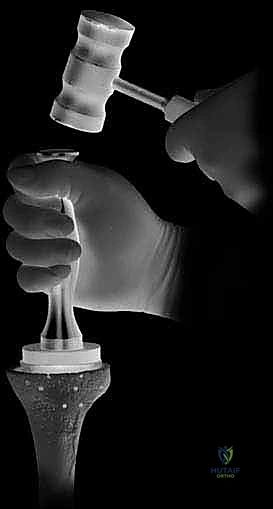
Final implantation utilizes the concept of "zonal fixation." The goal is to achieve rigid, immediate mechanical stability. The diaphyseal stem is typically press-fit (uncemented) to provide long-term biologic fixation and rotational stability, particularly when using splined or fluted titanium stems. Conversely, the undersurface of the tibial tray and the metallic augments are meticulously cemented to the prepared metaphyseal host bone. High-viscosity PMMA cement is applied to the undersurface of the tray and the augment, and the construct is impacted into place. Care must be taken to prevent cement from extruding into the diaphyseal canal, which could hinder the press-fit engagement of the stem. The construct is held under rigid axial compression until the cement is fully polymerized.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, revision TKA with metallic augmentation carries a higher complication profile than primary arthroplasty. The complexity of the host bone environment, extended operative times, and the massive presence of foreign material all contribute to elevated risks. Understanding these complications, their incidence, and the appropriate salvage pathways is critical for the revision surgeon.
Aseptic loosening remains a primary mode of long-term failure, though the use of diaphyseal engaging stems has significantly reduced the failure rate of augmented tibial trays. Loosening typically occurs at the cement-bone interface of the metaphysis, secondary to inadequate initial fixation, failure to bypass the defect with an appropriately long stem, or progressive stress shielding. When a metallic augment construct fails aseptically, the subsequent bone loss is often profound, frequently converting a Type II defect into a Type III. Salvage management in these cases almost universally requires transition to highly porous metaphyseal cones or sleeves to achieve biologic fixation in the compromised metaphysis, coupled with a longer, thicker diaphyseal stem.
Periprosthetic Joint Infection (PJI) is a devastating complication, with incidence rates in revision TKA ranging from 3% to 8%, significantly higher than in primary settings. The large surface area of modular junctions and metallic augments provides an extensive nidus for biofilm formation. Acute postoperative infections may be managed with aggressive Debridement, Antibiotics, and Implant Retention (DAIR), provided the modular components (polyethylene insert) are exchanged. However, chronic PJI necessitates a complete, two-stage revision protocol. This involves explantation of all components, aggressive debridement, placement of an articulating or static antibiotic-impregnated cement spacer, and a prolonged course of targeted intravenous antibiotics. Only after clinical and serological eradication of the infection is confirmed can a second-stage reimplantation be performed, often requiring even more extensive augmentation or metaphyseal cones due to the bone loss incurred during the explantation phase.
Periprosthetic fractures can occur intraoperatively or postoperatively. Intraoperative fractures typically involve the diaphyseal cortex during aggressive reaming or impaction of a press-fit stem, or the metaphyseal shell during component extraction. Diaphyseal fractures must be recognized immediately and bypassed with a longer stem, often supplemented with cerclage wiring or a strut allograft. Postoperative fractures are usually secondary to trauma in osteopenic bone, often occurring at the tip of the diaphyseal stem (stress riser). Management depends on the stability of the implant; well-fixed implants may be treated with open reduction and internal fixation (ORIF) utilizing locking plates and cables, while loose implants require a massive re-revision procedure.

| Complication | Estimated Incidence in Revision TKA | Primary Mechanism / Risk Factor | Salvage Strategy / Management |
|---|---|---|---|
| Aseptic Loosening | 4% - 9% | Inadequate stem length, stress shielding, poor cementing technique | Re-revision with highly porous metaphyseal cones/sleeves and longer stems |
| Periprosthetic Infection | 3% - 8% | Prolonged OR time, massive hardware, poor soft tissue envelope | Two-stage revision with antibiotic spacer; DAIR for acute cases |
| Intraoperative Fracture | 2% - 5% | Aggressive reaming, impaction of press-fit stems, fragile metaphysis | Bypass with longer stem (>2 cortical diameters), cerclage wiring |
| Extensor Mechanism Disruption | 1% - 3% | Aggressive patellar eversion, prior TTO failure, avascular necrosis | Allograft reconstruction (Achilles/extensor mechanism), synthetic mesh |
| Neurovascular Injury | < 1% | Posterior saw plunging, aggressive posterior capsule release | Immediate vascular surgery consultation, bypass grafting, fasciotomy |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a revision TKA with metallic augmentation is inherently more complex and must be highly individualized compared to primary TKA. The protocol is heavily dictated by the method of stem fixation (cemented versus press-fit diaphyseal engagement), the quality of the remaining host bone, and the necessity of any extensile surgical exposures (such as a quadriceps snip or tibial tubercle osteotomy). Close communication between the operative surgeon and the physical therapy team is vital to prevent catastrophic early failure of the construct or the soft tissue envelope.
Phase I (Acute Postoperative Phase, Weeks 0-2) focuses on medical stabilization, deep vein thrombosis (DVT) prophylaxis, wound healing, and early mobilization. If the tibial construct utilizes a fully cemented stem or a press-fit stem with excellent intraoperative rotational stability in robust diaphyseal bone, weight-bearing as tolerated (WBAT) with an assistive device (walker or crutches) is generally permitted immediately. However, if bone quality is poor or if a structural allograft was utilized in conjunction with the augments, protected weight-bearing (toe-touch or 20% partial weight-bearing) may be mandated for the first 6 weeks. Early emphasis is placed on achieving full active extension to prevent flexion contractures. Continuous Passive Motion (CPM) machines are rarely used today unless severe arthrofibrosis was encountered intraoperatively. Quadriceps activation exercises (isometric quad sets, straight leg raises) are initiated immediately, provided an extensile approach was not utilized.
Phase II (Subacute Phase, Weeks 2-6) marks the progression of range of motion and the normalization of gait mechanics. The goal is to achieve at least 90 to 100 degrees of active flexion by week 6. If a quadriceps snip was performed, active extension against gravity may be delayed for 2 to 3 weeks to protect the repair, though passive flexion is encouraged. For patients who underwent a tibial tubercle osteotomy, active terminal extension is strictly prohibited for 6 weeks, and the knee is often immobilized in a hinged brace locked in extension during ambulation to prevent avulsion of the osteotomy site. Strengthening exercises transition from isometric to closed-kinetic chain exercises (e.g., mini-squats, leg presses) as weight-bearing restrictions are lifted.
Phase III (Advanced Rehabilitation, Weeks 6-12+) focuses on advanced strengthening, proprioceptive training, and a return to activities of daily living (ADLs). Patients are weaned off assistive devices as their gait normalizes and quadriceps control becomes sufficient to prevent buckling. Balance and proprioceptive exercises
