Full Question & Answer Text (for Search Engines)
Question 1:
A 6-year-old boy presents with a displaced lateral condyle fracture of the humerus. Which of the following describes the most likely long-term complication if this fracture goes on to nonunion?
Options:
- Cubitus varus and tardy radial nerve palsy
- Cubitus valgus and tardy ulnar nerve palsy
- Cubitus valgus and median nerve palsy
- Cubitus varus and tardy ulnar nerve palsy
- Premature physeal closure with limb length discrepancy
Correct Answer: Cubitus valgus and tardy ulnar nerve palsy
Explanation:
Nonunion of a lateral condyle humerus fracture often leads to progressive cubitus valgus deformity. Over time, the stretching of the ulnar nerve behind the medial epicondyle can cause a tardy ulnar nerve palsy. Cubitus varus is classically associated with supracondylar humerus malunions.
Question 2:
During a posterior-stabilized total knee arthroplasty, trial reduction reveals the knee is tight in full extension but perfectly balanced and symmetric in 90 degrees of flexion. Which of the following is the most appropriate next step in management?
Options:
- Recut the proximal tibia with more posterior slope
- Release the posterior cruciate ligament
- Resect more distal femur
- Decrease the size of the femoral component
- Translate the femoral component anteriorly
Correct Answer: Resect more distal femur
Explanation:
A knee that is tight in extension but balanced in flexion implies an extension gap that is too small compared to the flexion gap. Resecting more distal femur will enlarge the extension gap without affecting the flexion gap. Changing the tibial cut affects both gaps equally. Downsizing the femur increases the flexion gap.
Question 3:
According to Perren's strain theory, what is the maximum amount of interfragmentary strain that allows for primary bone healing (direct osteonal reconstruction without callus formation)?
Options:
- < 2%
- 2% to 10%
- 10% to 15%
- 15% to 20%
- > 20%
Correct Answer: < 2%
Explanation:
According to Perren's strain theory, primary bone healing (intramembranous/osteonal without callus) occurs only when interfragmentary strain is less than 2%. Strain between 2% and 10% promotes secondary bone healing via endochondral ossification (callus formation). Strain above 10-15% leads to fibrous tissue formation and nonunion.
Question 4:
A 32-year-old woman is diagnosed with an unresectable giant cell tumor of the sacrum. She is started on denosumab therapy. What is the precise mechanism of action of this medication?
Options:
- Inhibits matrix metalloproteinases to prevent tumor invasion
- Directly induces apoptosis of the neoplastic stromal cells
- Binds to the RANK receptor on osteoclasts
- Monoclonal antibody that binds to RANKL, preventing osteoclast activation
- Inhibits vascular endothelial growth factor (VEGF) to reduce tumor vascularity
Correct Answer: Monoclonal antibody that binds to RANKL, preventing osteoclast activation
Explanation:
Denosumab is a fully human monoclonal antibody that binds to RANK Ligand (RANKL), preventing it from interacting with the RANK receptor on the surface of osteoclasts and their precursors. This inhibits osteoclast-mediated bone resorption. Giant cell tumors of bone consist of neoplastic mononuclear stromal cells that express RANKL, which recruits the multinucleated osteoclast-like giant cells.
Question 5:
A 40-year-old man sustains a closed tibial shaft fracture. He complains of disproportionate pain. Intracompartmental pressure monitoring is performed. Which of the following values is the most universally accepted threshold for performing an emergency four-compartment fasciotomy?
Options:
- Absolute compartment pressure greater than 20 mmHg
- Absolute compartment pressure greater than 30 mmHg
- Delta P (Diastolic blood pressure minus compartment pressure) less than 30 mmHg
- Delta P (Mean arterial pressure minus compartment pressure) less than 45 mmHg
- Systolic blood pressure minus compartment pressure less than 30 mmHg
Correct Answer: Delta P (Diastolic blood pressure minus compartment pressure) less than 30 mmHg
Explanation:
The Delta P (diastolic blood pressure minus the intracompartmental pressure) is the most reliable indicator for acute compartment syndrome. A Delta P of less than 30 mmHg is the universally accepted threshold indicating the need for emergent fasciotomy. Absolute pressure readings alone can be misleading, especially in hypotensive patients.
Question 6:
When performing an anterior cruciate ligament (ACL) reconstruction, placing the femoral tunnel too far anteriorly (shallow) in the intercondylar notch will result in which of the following biomechanical consequences?
Options:
- The graft will be tight in extension and loose in flexion
- The graft will be tight in flexion and loose in extension
- The graft will be tight in both flexion and extension
- The graft will impinge on the PCL
- The graft will fail to control varus-valgus laxity
Correct Answer: The graft will be tight in flexion and loose in extension
Explanation:
Placing the femoral tunnel too anteriorly (shallow) is a common technical error in ACL reconstruction. This results in the graft being loose in extension and becoming excessively tight as the knee moves into flexion, often leading to limited knee flexion or graft rupture. Conversely, placing the tunnel too vertically fails to control rotational stability.
Question 7:
An 8-week-old infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). The mother notes that the child has stopped kicking the leg on the affected side. On examination, the quadriceps are weak and the patellar reflex is diminished. This complication is most likely due to:
Options:
- Excessive hip abduction in the harness
- Excessive hip flexion in the harness
- Insufficient hip flexion in the harness
- Excessive knee flexion in the harness
- Avascular necrosis of the femoral head
Correct Answer: Excessive hip flexion in the harness
Explanation:
Femoral nerve palsy in a Pavlik harness is typically caused by excessive hip flexion, which stretches or compresses the femoral nerve. The management involves adjusting the harness to decrease the amount of flexion or giving the infant a temporary break from the harness until neurologic function returns. Excessive abduction is associated with avascular necrosis (AVN) of the femoral head.
Question 8:
A 65-year-old man presents with progressive clumsiness of his hands, difficulty buttoning his shirt, and a broad-based, unsteady gait. Physical exam demonstrates a positive Hoffmann sign and hyperreflexia in the lower extremities. What is the most sensitive imaging study to evaluate the cause of this condition?
Options:
- CT scan of the cervical spine without contrast
- Flexion-extension radiographs of the cervical spine
- MRI of the cervical spine
- EMG and nerve conduction studies of the upper extremities
- Myelography of the lumbar spine
Correct Answer: MRI of the cervical spine
Explanation:
The patient's symptoms (clumsy hands, gait instability) and signs (Hoffmann sign, hyperreflexia) are classic for cervical spondylotic myelopathy (an upper motor neuron lesion). MRI of the cervical spine is the imaging modality of choice to evaluate spinal cord compression, signal changes in the cord (myelomalacia), and the exact level(s) of stenosis.
Question 9:
The 'watershed' area of the Achilles tendon is the most common site for spontaneous rupture. Approximately where is this zone of relative hypovascularity located relative to its insertion on the calcaneus?
Options:
- At the osteotendinous junction
- 2 to 6 cm proximal to the insertion
- 8 to 10 cm proximal to the insertion
- At the musculotendinous junction
- Directly posterior to the medial malleolus
Correct Answer: 2 to 6 cm proximal to the insertion
Explanation:
The 'watershed' area of the Achilles tendon is located approximately 2 to 6 cm proximal to its insertion on the calcaneus. This region has a relatively poor blood supply (hypovascularity), which contributes to its susceptibility to degeneration and rupture. The blood supply to the tendon comes from the musculotendinous junction proximally, the osteotendinous junction distally, and anteriorly via the paratenon.
Question 10:
Which of the following components of articular cartilage is primarily responsible for providing tensile strength to the extracellular matrix?
Options:
- Aggrecan
- Hyaluronic acid
- Type II collagen
- Type X collagen
- Chondroitin sulfate
Correct Answer: Type II collagen
Explanation:
In articular cartilage, Type II collagen forms a cross-linked fibrillar network that primarily provides the tissue with tensile strength and restrains the swelling pressure of the proteoglycans. Proteoglycans (such as aggrecan) draw water into the matrix via osmotic pressure, providing compressive stiffness and resistance.
Question 11:
In the flexor tendon pulley system of the fingers, which two annular pulleys are considered the most critical to prevent bowstringing of the flexor tendons and must be preserved or reconstructed during surgery?
Options:
- A1 and A3
- A2 and A4
- A3 and A5
- A1 and A5
- A2 and A3
Correct Answer: A2 and A4
Explanation:
The A2 and A4 pulleys are the major biomechanical pulleys in the digital flexor sheath. They arise directly from the periosteum of the proximal and middle phalanges, respectively. They are critical to prevent bowstringing of the flexor tendons, which would cause a significant loss of active flexion and mechanical disadvantage.
Question 12:
In metal-on-polyethylene total hip arthroplasty, the use of highly cross-linked polyethylene (HXLPE) was introduced to reduce wear. However, standard cross-linking involves irradiation that produces free radicals. How are these free radicals most commonly eliminated to prevent long-term oxidative degradation?
Options:
- Sterilization with ethylene oxide
- Adding cobalt-chromium particulate debris
- Melting or remelting the polyethylene
- Increasing the radiation dose to 10 Mrad
- Implanting the components in a vacuum environment
Correct Answer: Melting or remelting the polyethylene
Explanation:
Irradiation of polyethylene causes cross-linking (improving wear resistance) but also creates free radicals (causing oxidative degradation and embrittlement over time). To eliminate these free radicals, the polyethylene undergoes a thermal treatment, typically either melting (heating above the melting point) or annealing (heating below the melting point). Melting eliminates all free radicals but slightly reduces mechanical strength.
Question 13:
A 28-year-old man sustains a displaced, vertically oriented femoral neck fracture (Pauwels Type III) after a motor vehicle collision. He undergoes closed reduction and internal fixation with multiple cannulated screws. Biomechanically, this fracture pattern has the highest risk for failure due to which of the following forces?
Options:
- Compressive forces at the fracture site
- Rotational forces primarily
- High shear forces causing varus displacement
- Tension forces on the medial calcar
- Distraction forces from the abductor musculature
Correct Answer: High shear forces causing varus displacement
Explanation:
Pauwels Type III femoral neck fractures are highly vertical (>50 degrees to the horizontal). Biomechanically, this vertical orientation converts weight-bearing and muscle forces into extremely high shear forces across the fracture site. This makes them inherently unstable and prone to varus collapse, nonunion, and fixation failure when treated with standard parallel cannulated screws alone.
Question 14:
A 14-year-old girl is diagnosed with high-grade conventional osteosarcoma of the distal femur. She completes a course of neoadjuvant chemotherapy followed by wide surgical resection. Which of the following factors determined from the resected specimen is the most important prognostic indicator for overall survival?
Options:
- The absolute size of the initial tumor
- The distance of the closest surgical margin
- The percentage of tumor necrosis
- The presence of skip metastases in the medullary canal
- The histologic subtype (e.g., chondroblastic vs. fibroblastic)
Correct Answer: The percentage of tumor necrosis
Explanation:
In the treatment of conventional high-grade osteosarcoma, the degree of tumor necrosis in the resected specimen following neoadjuvant chemotherapy (the histologic response) is the single most important prognostic factor for long-term survival. A good response is typically defined as >= 90% tumor necrosis (Huvos grading system).
Question 15:
According to the Loder classification, an unstable Slipped Capital Femoral Epiphysis (SCFE) is defined by which of the following clinical criteria, and what is the primary risk associated with it?
Options:
- Displacement greater than 50%; high risk of chondrolysis
- Inability to ambulate even with crutches; high risk of avascular necrosis
- Duration of symptoms less than 3 weeks; high risk of contralateral slip
- Presence of an effusion on ultrasound; high risk of septic arthritis
- Slip angle greater than 60 degrees; high risk of osteoarthritis
Correct Answer: Inability to ambulate even with crutches; high risk of avascular necrosis
Explanation:
The Loder classification divides SCFE into stable and unstable categories based strictly on the clinical ability of the patient to bear weight (with or without crutches). An unstable SCFE means the patient cannot bear weight. This is highly clinically relevant because unstable SCFEs carry a substantially higher risk of developing avascular necrosis (AVN) of the femoral head (often approaching 50%).
Question 16:
A 68-year-old woman complains of bilateral leg and buttock pain that worsens when walking and improves when sitting or leaning forward over a shopping cart. The 'bicycle test of van Gelderen' is performed to differentiate neurogenic claudication from vascular claudication. In this test, neurogenic claudication is supported if the patient:
Options:
- Experiences pain equally while cycling with the spine flexed or extended
- Has onset of calf pain at exactly the same distance repeatedly
- Can pedal longer with the spine flexed compared to standing erect
- Develops diminished pedal pulses after 5 minutes of cycling
- Experiences relief of symptoms only after 10 minutes of complete rest
Correct Answer: Can pedal longer with the spine flexed compared to standing erect
Explanation:
In the bicycle test of van Gelderen, the patient pedals a stationary bike. If the pain is vascular, it is related to muscle work and will occur regardless of spine posture. If it is neurogenic claudication (lumbar spinal stenosis), leaning forward (flexing the spine) increases the cross-sectional area of the spinal canal and neural foramina, alleviating compression and allowing the patient to cycle longer without symptoms compared to when the spine is extended.
Question 17:
According to the Gustilo-Anderson classification, a diaphyseal tibia fracture with a 6 cm laceration, extensive soft tissue damage, periosteal stripping, and massive contamination, but with adequate soft tissue coverage requiring no flap, is classified as:
Options:
- Type II
- Type IIIA
- Type IIIB
- Type IIIC
- Type IV
Correct Answer: Type IIIA
Explanation:
Gustilo-Anderson Type III fractures are high-energy injuries with extensive soft tissue damage (often >10 cm, or defined by severe contamination/crush). Type IIIA indicates extensive soft tissue damage, but with adequate soft tissue coverage of the fractured bone despite the extensive laceration. Type IIIB requires a local or free flap for coverage due to inadequate soft tissue. Type IIIC involves an arterial injury requiring repair.
Question 18:
The blood supply to the scaphoid primarily enters the bone distally and travels proximally, which predisposes proximal pole fractures to avascular necrosis. Which artery is the primary source of this retrograde blood supply?
Options:
- Palmar carpal branch of the ulnar artery
- Dorsal carpal branch of the radial artery
- Superficial palmar arch
- Deep palmar arch
- Anterior interosseous artery
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The scaphoid receives 70-80% of its blood supply from branches of the radial artery (specifically the dorsal carpal branch), which enter the bone at the dorsal ridge near the scaphoid waist and supply the proximal pole in a retrograde fashion. The remaining 20-30% enters via the volar superficial palmar arch branch, supplying the distal pole.
Question 19:
A 22-year-old athlete sustains an acute tear of the medial meniscus. The tear is located in the peripheral 3 mm of the meniscus (the red-red zone). Which blood vessels provide the primary vascular supply to this region, making it amenable to surgical repair?
Options:
- Anterior and posterior tibial recurrent arteries
- Branches of the medial and lateral inferior and superior genicular arteries
- Middle genicular artery exclusively
- Sural arteries and their terminal branches
- Descending genicular artery
Correct Answer: Branches of the medial and lateral inferior and superior genicular arteries
Explanation:
The blood supply to the menisci originates predominantly from a perimeniscal capillary plexus supplied by the superior and inferior branches of the medial and lateral genicular arteries. (The middle genicular artery supplies the vascularity to the meniscal horns). This plexus supplies the peripheral 10% to 30% of the menisci (the red-red zone), providing a good healing potential for repairs.
Question 20:
A 35-year-old man injures his midfoot. Radiographs show a small bony avulsion fragment in the space between the base of the first and second metatarsals (the 'fleck sign'). The Lisfranc ligament, which is injured in this scenario, connects which two osseous structures?
Options:
- Base of the 1st metatarsal to the base of the 2nd metatarsal
- Base of the 2nd metatarsal to the medial cuneiform
- Base of the 2nd metatarsal to the middle cuneiform
- Medial cuneiform to the middle cuneiform
- Navicular to the medial cuneiform
Correct Answer: Base of the 2nd metatarsal to the medial cuneiform
Explanation:
The Lisfranc ligament is a strong interosseous ligament that connects the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. There is no direct interosseous ligamentous connection between the bases of the first and second metatarsals. The 'fleck sign' represents an avulsion of the Lisfranc ligament typically from the base of the 2nd metatarsal.
Question 21:
A 25-year-old male presents with chronic, dull posterior knee pain. Radiographs show a heavily ossified, lobulated mass attached by a broad base to the posterior cortex of the distal femur. MRI confirms no medullary involvement. Biopsy reveals a low-grade spindle cell stroma with well-formed woven bone trabeculae. What is the most likely diagnosis and its general prognosis compared to conventional osteosarcoma?
Options:
- Parosteal osteosarcoma; better prognosis
- Periosteal osteosarcoma; better prognosis
- High-grade surface osteosarcoma; worse prognosis
- Parosteal osteosarcoma; worse prognosis
- Periosteal osteosarcoma; worse prognosis
Correct Answer: Parosteal osteosarcoma; better prognosis
Explanation:
Parosteal osteosarcoma is a low-grade surface osteosarcoma that classically arises from the posterior aspect of the distal femur. It typically presents as a heavily ossified, broad-based mass with no medullary involvement in its early stages. It has a significantly better prognosis than conventional high-grade intramedullary osteosarcoma. Periosteal osteosarcoma is intermediate-grade, chondroblastic, and more commonly affects the anterior tibia.
Question 22:
During the surgical treatment of a severe, unstable slipped capital femoral epiphysis (SCFE) using in situ pinning, the surgeon performs an anterior capsulotomy of the hip. What is the primary biomechanical or physiologic benefit of this adjunctive procedure?
Options:
- Reduces the risk of postoperative chondrolysis
- Reduces intracapsular pressure and the risk of avascular necrosis (AVN)
- Improves direct visualization to achieve anatomical reduction
- Facilitates the placement of a completely intra-epiphyseal screw
- Prevents the future development of cam-type femoroacetabular impingement
Correct Answer: Reduces intracapsular pressure and the risk of avascular necrosis (AVN)
Explanation:
In an unstable SCFE, there is often an intracapsular hematoma that raises the pressure within the joint space. This increased pressure can compromise the tenuous retinacular vessels supplying the femoral epiphysis, increasing the risk of avascular necrosis (AVN). An anterior capsulotomy decompresses the hematoma, lowering intracapsular pressure and mitigating the risk of AVN.
Question 23:
A 30-year-old male is involved in a severe motorcycle collision and sustains an anteroposterior compression type III (APC-III) pelvic ring injury. After the application of a pelvic binder and initial fluid resuscitation, he remains hemodynamically unstable. An emergent angiogram is performed. Which of the following vessels is most likely to be the source of arterial bleeding in this specific injury pattern?
Options:
- Superior gluteal artery
- Internal pudendal artery
- Lumbar artery
- Inferior epigastric artery
- Iliolumbar artery
Correct Answer: Internal pudendal artery
Explanation:
Anteroposterior compression (APC) pelvic injuries cause symphyseal diastasis and disruption of the anterior pelvic structures. Hemorrhage in APC injuries is most commonly venous, but when arterial bleeding occurs, the anterior branches of the internal iliac artery—most notably the internal pudendal and obturator arteries—are most frequently injured. The superior gluteal artery is more commonly injured in posterior ring disruptions and lateral compression (LC) injuries.
Question 24:
A 45-year-old manual laborer presents with progressive wrist pain. Radiographs reveal a scaphoid nonunion with localized arthritis at the radial styloid-scaphoid articulation. The radioscaphoid joint is narrowed, but the midcarpal joint and the radiolunate articulation are completely preserved (SNAC Stage 1). Which of the following is the most appropriate surgical intervention?
Options:
- Proximal row carpectomy
- Four-corner arthrodesis
- Radial styloidectomy with scaphoid nonunion takedown and bone grafting
- Total wrist arthrodesis
- Scaphoid excision and capitolunate arthrodesis
Correct Answer: Radial styloidectomy with scaphoid nonunion takedown and bone grafting
Explanation:
Scaphoid nonunion advanced collapse (SNAC) Stage 1 is characterized by arthritis limited to the radial styloid. For Stage 1 SNAC, an organ-preserving procedure is indicated, specifically radial styloidectomy combined with open reduction, internal fixation, and bone grafting of the scaphoid. Salvage procedures like proximal row carpectomy (PRC) or four-corner fusion are indicated for SNAC Stage 2 (scaphocapitate arthritis) and Stage 3 (periscaphoid arthritis).
Question 25:
In modern total hip arthroplasty, the adoption of highly cross-linked polyethylene (HXLPE) has significantly reduced the rate of osteolysis and aseptic loosening. However, the cross-linking process alters the material's properties. Which of the following mechanical properties is typically decreased as a direct result of increased cross-linking?
Options:
- Ultimate tensile strength
- Wear resistance
- Oxidation resistance
- Young's modulus
- Creep resistance
Correct Answer: Ultimate tensile strength
Explanation:
The irradiation process used to highly cross-link polyethylene drastically improves its wear resistance. However, this comes at the expense of several mechanical properties, including a decrease in ultimate tensile strength, yield strength, ductility, and fracture toughness. Subsequent thermal treatments (remelting or annealing) are used to eliminate free radicals and improve oxidation resistance, but remelting can further decrease mechanical strength.
Question 26:
A 68-year-old male presents with deteriorating hand dexterity, a broad-based gait, and urinary urgency. Physical examination reveals hyperreflexia and a positive Hoffmann's sign. The examiner percusses the distal brachioradialis tendon, which elicits spontaneous flexion of the patient's fingers without wrist extension. What is the name of this clinical sign?
Options:
- Spurling's sign
- Lhermitte's sign
- Inverted supinator reflex
- Wartenberg's sign
- Tinel's sign
Correct Answer: Inverted supinator reflex
Explanation:
The inverted supinator reflex is highly specific for cervical spondylotic myelopathy. It occurs when tapping the brachioradialis tendon (innervated by C6) elicits no wrist extension/supination, but rather spontaneous finger flexion (innervated by C8). This indicates a lower motor neuron lesion at the C5-C6 level combined with an upper motor neuron lesion affecting the uninhibited segments below (C8).
Question 27:
A 22-year-old rugby player has recurrent anterior shoulder instability. A 3D CT scan reveals a 25% anterior glenoid bone loss along with a large, engaging Hill-Sachs lesion. What is the most appropriate surgical treatment to effectively restore stability and prevent future dislocations?
Options:
- Arthroscopic Bankart repair with remplissage
- Arthroscopic Bankart repair alone
- Latarjet procedure
- Putti-Platt procedure
- Arthroscopic capsular plication
Correct Answer: Latarjet procedure
Explanation:
In the setting of significant anterior glenoid bone loss (>20-25%), soft tissue stabilization (Bankart repair) alone has an unacceptably high failure rate. Bony augmentation, such as the Latarjet procedure (coracoid transfer), is the standard of care. It restores the anterior glenoid arc and provides dynamic stability via the 'sling effect' of the conjoint tendon. Remplissage can address an engaging Hill-Sachs lesion but does not replace missing glenoid bone.
Question 28:
Which of the following processes characterizes primary (direct) bone healing, such as that achieved through anatomical reduction and absolute stability with a dynamic compression plate?
Options:
- Endochondral ossification
- Intramembranous ossification
- Osteoclastic cutting cones crossing the fracture site
- Robust callus formation bridging the fracture gap
- Chondroid bone formation
Correct Answer: Osteoclastic cutting cones crossing the fracture site
Explanation:
Primary (direct) bone healing occurs under conditions of absolute stability and anatomical reduction. It bypasses the intermediate stages of callus formation and relies directly on osteoclastic 'cutting cones' that bore across the fracture line, followed immediately by osteoblasts that lay down lamellar bone. Secondary bone healing involves callus formation and endochondral ossification.
Question 29:
A 55-year-old female presents with a painful bunion. Weight-bearing radiographs demonstrate a hallux valgus angle (HVA) of 38 degrees and an intermetatarsal angle (IMA) of 17 degrees. Clinical examination reveals no first tarsometatarsal (TMT) hypermobility and no evidence of midfoot arthritis. Which of the following procedures is most appropriate for correcting this deformity?
Options:
- Distal chevron osteotomy
- Proximal metatarsal osteotomy with a distal soft tissue release
- Lapidus procedure (first TMT arthrodesis)
- Akin osteotomy alone
- Keller resection arthroplasty
Correct Answer: Proximal metatarsal osteotomy with a distal soft tissue release
Explanation:
The patient has a severe hallux valgus deformity (HVA >30, IMA >13). A distal chevron osteotomy cannot provide sufficient translation to correct an IMA of 17 degrees. A proximal osteotomy (e.g., Ludloff, crescentic, or proximal chevron) combined with a distal soft tissue procedure is required for this magnitude of deformity. A Lapidus procedure is also an option but is strictly indicated when TMT hypermobility or arthritis is present.
Question 30:
A 35-year-old male with a severely comminuted, closed tibial shaft fracture complains of agonizing leg pain out of proportion to the injury. The clinical suspicion for acute compartment syndrome is high, and intracompartmental pressures are measured. Which of the following pressure criteria is the most reliable and widely accepted indication for emergent four-compartment fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 30 mmHg
- Diastolic blood pressure minus compartment pressure < 30 mmHg
- Mean arterial pressure minus compartment pressure < 40 mmHg
- Systolic blood pressure minus compartment pressure < 30 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure < 30 mmHg
Explanation:
The delta pressure (Diastolic Blood Pressure - Compartment Pressure) is the most reliable objective indicator for acute compartment syndrome. A delta pressure of less than 30 mmHg signifies that the tissue perfusion pressure is inadequate, making it a universally accepted indication for emergent fasciotomy. Absolute pressure thresholds (e.g., >30 mmHg) are less accurate because they do not account for systemic perfusion pressure.
Question 31:
According to the 2018 International Consensus Meeting (ICM) criteria for periprosthetic joint infection (PJI), which of the following is considered a 'Major Criterion' that is definitive for the diagnosis of PJI?
Options:
- Synovial fluid white blood cell (WBC) count > 3,000 cells/uL
- Synovial fluid polymorphonuclear (PMN) percentage > 80%
- Two positive periprosthetic tissue cultures with phenotypically identical organisms
- A positive leukocyte esterase strip test (++ or greater)
- Elevated synovial alpha-defensin level
Correct Answer: Two positive periprosthetic tissue cultures with phenotypically identical organisms
Explanation:
Under the ICM criteria for PJI, there are two major criteria; the presence of either one is definitive for infection. These are: 1) A sinus tract communicating with the joint/prosthesis, or 2) Two positive periprosthetic tissue or fluid cultures growing the same organism. The other options (WBC count, PMN %, leukocyte esterase, alpha-defensin, CRP/ESR) are minor criteria that contribute points toward a diagnostic score.
Question 32:
A 4-month-old infant is being treated for developmental dysplasia of the hip (DDH) using a Pavlik harness. During a routine follow-up, the parents report the infant is not moving the affected leg as much. Physical examination reveals decreased active extension of the knee on the treated side, while hip movements and ankle movements appear normal. What is the most likely cause of this complication?
Options:
- Excessive hip abduction in the harness
- Excessive hip flexion in the harness
- Avascular necrosis of the femoral head
- Transient synovitis of the hip
- Inadequate hip flexion in the harness
Correct Answer: Excessive hip flexion in the harness
Explanation:
Decreased active knee extension in a child wearing a Pavlik harness is highly indicative of a femoral nerve palsy. This iatrogenic complication is caused by excessive flexion of the hip in the harness, which stretches or compresses the femoral nerve against the inguinal ligament. The correct management is to temporarily loosen or remove the anterior (flexion) straps until nerve function recovers. Excessive abduction, conversely, increases the risk of avascular necrosis (AVN).
Question 33:
A 65-year-old male presents with classic neurogenic claudication secondary to severe lumbar spinal stenosis at L4-L5. His symptoms are entirely activity-dependent, resolving completely when he sits or bends forward. He has no resting pain and his neurologic exam is normal. During counseling regarding non-operative management, what should the patient be told about the expected natural history of his condition over the next 5 years?
Options:
- He is at high risk for rapid progression to cauda equina syndrome
- He will experience predictable, steady neurological decline
- Symptomatic improvement is expected in the majority of patients
- His symptoms will likely remain stable with mild fluctuations, without severe deterioration
- The anatomical stenosis will spontaneously resolve due to disk resorption
Correct Answer: His symptoms will likely remain stable with mild fluctuations, without severe deterioration
Explanation:
The natural history of mildly-to-moderately symptomatic lumbar spinal stenosis is generally benign and stable. Longitudinal studies indicate that up to 70-80% of patients managed conservatively will remain stable or experience only minor fluctuations in their symptoms over several years. Rapid deterioration or progression to cauda equina syndrome is exceedingly rare.
Question 34:
A 28-year-old carpenter sustains a laceration over the volar aspect of the proximal phalanx of his index finger, severing both the FDS and FDP tendons. This anatomical area is designated as Zone II. Why was this specific zone historically referred to by Bunnell as 'no man's land'?
Options:
- Due to the completely avascular nature of the flexor tendons within this segment
- Because primary repair historically yielded poor results due to dense adhesions within the narrow fibro-osseous sheath
- Due to the lack of distinct anatomical landmarks making surgical exploration hazardous
- Because both the median and ulnar nerves arborize extensively in this exact location
- Due to the extremely high rate of purulent flexor tenosynovitis following any surgical intervention
Correct Answer: Because primary repair historically yielded poor results due to dense adhesions within the narrow fibro-osseous sheath
Explanation:
Zone II of the hand extends from the proximal edge of the A1 pulley to the insertion of the flexor digitorum superficialis (FDS). Historically, Sterling Bunnell termed this area 'no man's land' because primary repair of the flexor tendons within this tight fibro-osseous sheath resulted in dense adhesions and severely restricted motion. Modern microscopic techniques, better suture materials, and early active mobilization protocols have reversed this, making primary repair the standard of care.
Question 35:
A 25-year-old soccer player sustains a knee injury. Clinical examination reveals a positive posterior sag sign and a positive posterior drawer test. The tibia subluxates posteriorly at rest but reduces with an anterior drawer maneuver. Which of the following mechanisms of injury is most classically associated with this specific ligamentous injury?
Options:
- Non-contact pivoting with a firmly planted foot
- A direct blow to the anterior proximal tibia while the knee is flexed
- Hyperextension with sudden internal rotation
- Valgus stress applied to a partially flexed knee
- Varus stress applied to a fully extended knee
Correct Answer: A direct blow to the anterior proximal tibia while the knee is flexed
Explanation:
The patient's physical exam findings (posterior sag, positive posterior drawer) are diagnostic of a posterior cruciate ligament (PCL) injury. The classic mechanism of injury for a PCL tear is a direct, high-energy blow to the anterior aspect of the proximal tibia with the knee in a flexed position. This drives the tibia posteriorly, rupturing the PCL. This is frequently seen in dashboard injuries during motor vehicle accidents or falling onto a flexed knee in sports.
Question 36:
A 32-year-old female presents with distal femur pain. Radiographs reveal an eccentric, purely lytic lesion in the epiphysis extending to the subchondral bone. Biopsy confirms a Giant Cell Tumor (GCT) of bone. In cases where neoadjuvant treatment is indicated, Denosumab is often utilized. What is the precise mechanism of action of this medication in treating GCT?
Options:
- It inhibits vascular endothelial growth factor (VEGF) to starve the tumor
- It acts as a competitive antagonist of estrogen receptors in the stroma
- It is a monoclonal antibody that binds to RANKL, preventing the recruitment and activation of osteoclast-like giant cells
- It binds directly to the RANK receptor on the neoplastic mononuclear stromal cells to induce apoptosis
- It is a potent bisphosphonate that binds to hydroxyapatite and poisons osteoclasts
Correct Answer: It is a monoclonal antibody that binds to RANKL, preventing the recruitment and activation of osteoclast-like giant cells
Explanation:
Giant Cell Tumor of bone is composed of neoplastic mononuclear stromal cells that overexpress RANK Ligand (RANKL). This RANKL binds to RANK receptors on normal circulating monocytes, recruiting them and causing them to fuse into massive, bone-destroying osteoclast-like giant cells. Denosumab is a monoclonal antibody that binds directly to RANKL (not the RANK receptor), intercepting the signal and halting the bone destruction caused by the giant cells.
Question 37:
A 60-year-old patient with long-standing, poorly controlled diabetes presents with a unilaterally swollen, warm, and erythematous foot. Radiographs demonstrate dramatic tarsometatarsal joint subluxation, extensive bony fragmentation, and periarticular debris. Which classification system is strictly used to stage the radiographic progression of this specific neuroarthropathic condition?
Options:
- Brodsky classification
- Eichenholtz classification
- Hawkins classification
- Wagner classification
- Sanders classification
Correct Answer: Eichenholtz classification
Explanation:
The Eichenholtz classification describes the natural history and radiographic staging of Charcot neuroarthropathy. Stage 0 is clinical inflammation with normal x-rays. Stage 1 is the developmental/fragmentation phase (debris, dislocation). Stage 2 is the coalescence phase (absorption of debris, early fusion). Stage 3 is the consolidation/reconstruction phase. Brodsky classifies the anatomic location of Charcot joints, while Wagner is used for diabetic foot ulcers.
Question 38:
A 30-year-old male presents to the emergency department after sustaining a closed diaphyseal fracture of the humerus. In the context of humeral shaft fractures, which of the following is considered an absolute indication for operative fixation?
Options:
- Primary radial nerve palsy
- Transverse fracture pattern
- Open fracture
- Associated brachial plexus injury
- Holstein-Lewis fracture
Correct Answer: Open fracture
Explanation:
Absolute indications for operative management of a humeral shaft fracture include open fractures, fractures associated with a vascular injury requiring repair, compartment syndrome, and floating elbow injuries (ipsilateral humerus and forearm fractures). Primary radial nerve palsy, even in the setting of a Holstein-Lewis fracture (distal third spiral fracture), is generally considered a relative indication, as up to 90% of primary radial nerve palsies recover spontaneously with non-operative management.
Question 39:
When applying a dynamic compression plate (DCP) to stabilize a transverse diaphyseal fracture, the surgeon deliberately uses eccentric drilling for the screw holes nearest the fracture site. What is the primary biomechanical objective of this specific technique?
Options:
- To prevent stripping of the screw threads in osteopenic cortical bone
- To induce dynamic longitudinal interfragmentary compression across the fracture site
- To angle the screws away from intramedullary implants
- To minimize the stress-shielding effect on the underlying cortex
- To increase the axial pull-out strength of the cortical screws
Correct Answer: To induce dynamic longitudinal interfragmentary compression across the fracture site
Explanation:
Eccentric drilling in a dynamic compression plate (DCP) involves placing the drill hole on the side of the oval plate hole furthest from the fracture line. As the spherical head of the screw engages the sloped contour of the plate hole during tightening, it slides down the ramp, forcing the bone fragment to translate axially toward the fracture site. This generates dynamic longitudinal interfragmentary compression, optimizing the conditions for primary bone healing.
Question 40:
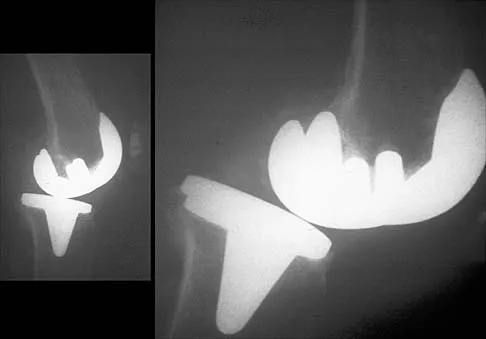
A 70-year-old female presents with a painful popping sensation in her knee 18 months following a primary posterior-stabilized total knee arthroplasty (TKA). The symptom occurs consistently as her knee extends from 45 degrees of flexion to full extension. She is diagnosed with 'patellar clunk syndrome.' What is the precise anatomical etiology of this phenomenon?
Options:
- A hypertrophic fibrous nodule on the deep surface of the quadriceps tendon catching in the femoral intercondylar box
- Dynamic subluxation of the extensor mechanism laterally due to an unreleased tight lateral retinaculum
- Impingement of the popliteus tendon on an oversized posterolateral femoral condyle
- Asymmetric polyethylene wear leading to sudden mediolateral translational instability
- An oversized femoral component causing severe overstuffing of the anterior compartment
Correct Answer: A hypertrophic fibrous nodule on the deep surface of the quadriceps tendon catching in the femoral intercondylar box
Explanation:
Patellar clunk syndrome is a known complication specific to posterior-stabilized total knee arthroplasty designs. It is caused by the formation of a hypertrophic fibrosynovial nodule on the undersurface of the quadriceps tendon, just proximal to the superior pole of the patella. As the knee extends from a flexed position, this nodule becomes incarcerated in the intercondylar box of the femoral component, popping out with a painful 'clunk' as extension continues.