Full Question & Answer Text (for Search Engines)
Question 1:
During in situ pinning of a slipped capital femoral epiphysis (SCFE), unrecognized pin penetration into the hip joint space is most directly associated with which of the following postoperative complications?
Options:
- Avascular necrosis
- Chondrolysis
- Coxa vara
- Femoroacetabular impingement
- Premature osteoarthritis
Correct Answer: Chondrolysis
Explanation:
Unrecognized pin penetration into the hip joint during in situ fixation of a SCFE is the most common cause of chondrolysis. It causes rapid loss of articular cartilage, leading to severe stiffness, pain, and a narrowed joint space on radiographs.
Question 2:
A 25-year-old male sustains a vertically oriented (Pauwels Type III) intracapsular femoral neck fracture. To maximize biomechanical stability and minimize shear forces across the fracture site during internal fixation, which of the following constructs is most appropriate?
Options:
- Three parallel cancellous screws in an inverted triangle configuration
- Dynamic hip screw (DHS) with an anti-rotation screw
- Proximal femoral nail antirotation (PFNA)
- Three parallel cancellous screws with a medially placed buttress plate
- A fully threaded 7.3mm single screw
Correct Answer: Dynamic hip screw (DHS) with an anti-rotation screw
Explanation:
A fixed-angle device such as a Dynamic Hip Screw (DHS), often supplemented with an anti-rotation screw, provides superior biomechanical stability for vertically oriented (Pauwels Type III) femoral neck fractures compared to multiple cancellous screws, as it better resists the high shear forces that predispose these vertical fracture patterns to varus collapse and nonunion.
Question 3:
Which of the following bearing surface combinations in total hip arthroplasty exhibits the lowest volumetric wear rate, but carries the highest risk of catastrophic failure due to fracture?
Options:
- Metal-on-highly cross-linked polyethylene
- Ceramic-on-polyethylene
- Metal-on-metal
- Ceramic-on-ceramic
- Oxinium-on-highly cross-linked polyethylene
Correct Answer: Ceramic-on-ceramic
Explanation:
Ceramic-on-ceramic (CoC) bearing surfaces have the lowest volumetric wear rates of all bearing combinations. However, due to the brittle nature of the ceramic material, they carry a unique risk of catastrophic component fracture, as well as a risk of audible 'squeaking' during movement.
Question 4:
A 72-year-old male falls from standing and sustains a Type II odontoid fracture with 5 mm of posterior displacement. If this patient is treated non-operatively with a rigid cervical collar, which of the following factors most strongly predicts the development of a nonunion?
Options:
- Age greater than 65 years
- Posterior displacement of 5 mm
- Concomitant C1 arch fracture
- Presence of osteoporosis
- Delay in diagnosis greater than 24 hours
Correct Answer: Age greater than 65 years
Explanation:
Advanced age (> 50-65 years, specifically > 65 in most modern literature) is the most significant independent risk factor for nonunion in Type II odontoid fractures treated non-operatively. Other risk factors include initial displacement > 5 mm, fracture angulation > 10 degrees, and delayed treatment.
Question 5:
A 32-year-old manual laborer presents with progressive dorsal wrist pain. Radiographs demonstrate sclerosis of the lunate, normal carpal height, and negative ulnar variance. MRI confirms osteonecrosis of the lunate without coronal fractures. According to the Lichtman classification, what is the most appropriate surgical intervention?
Options:
- Proximal row carpectomy
- Scaphoid-trapezium-trapezoid (STT) fusion
- Radial shortening osteotomy
- Total wrist arthrodesis
- Lunate excision and silastic replacement
Correct Answer: Radial shortening osteotomy
Explanation:
The patient has Lichtman Stage II Kienböck's disease (lunate sclerosis, normal carpal height) and negative ulnar variance. A joint-leveling procedure, such as a radial shortening osteotomy, is the treatment of choice in patients with negative ulnar variance and early-stage disease (Stages I, II, and early IIIa) to biomechanically decompress the lunate.
Question 6:
In the ultrasonographic evaluation of developmental dysplasia of the hip (DDH) using the Graf method, the alpha angle is used to assess acetabular development. Which of the following anatomical landmarks are used to measure the alpha angle?
Options:
- The bony roof of the acetabulum and the straight portion of the iliac bone
- The cartilaginous roof of the acetabulum and the iliac bone
- The triradiate cartilage and the labrum
- The femoral head and the iliac bone
- The labrum and the joint capsule
Correct Answer: The bony roof of the acetabulum and the straight portion of the iliac bone
Explanation:
In the Graf method for DDH, the alpha angle measures the concavity of the bony roof. It is formed by the intersection of the baseline (drawn along the straight portion of the ilium) and the bony roof line (drawn from the lower edge of the iliac bone at the triradiate cartilage tangent to the osseous rim). A normal alpha angle is greater than or equal to 60 degrees.
Question 7:
Articular cartilage is organized into multiple histological zones, each with specific biomechanical properties. Which zone is characterized by the largest diameter collagen fibrils oriented perpendicular to the articular surface, the highest concentration of proteoglycans, and the lowest water content?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified cartilage zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage contains the largest diameter collagen fibrils, which are oriented perpendicular to the articular surface. This zone also possesses the highest concentration of proteoglycans and the lowest water content, providing significant resistance to compressive forces.
Question 8:
A 65-year-old male presents with a pathologic fracture of the proximal humerus. Workup reveals hypercalcemia, renal insufficiency, normocytic anemia, and a monoclonal protein spike on serum electrophoresis. Histological examination of the fracture site is most likely to show which of the following?
Options:
- Small round blue cells with positive CD99 staining
- Atypical spindle cells producing malignant osteoid
- Sheets of atypical plasma cells with eccentric nuclei and clock-face chromatin
- Multinucleated giant cells in a background of mononuclear stromal cells
- Nests of epithelial cells with positive cytokeratin staining
Correct Answer: Sheets of atypical plasma cells with eccentric nuclei and clock-face chromatin
Explanation:
The clinical presentation (CRAB criteria: hyperCalcemia, Renal insufficiency, Anemia, Bone lesions) and monoclonal gammopathy are classic for Multiple Myeloma. Histologically, multiple myeloma is characterized by sheets of atypical, neoplastic plasma cells, which characteristically possess eccentric nuclei and a 'clock-face' chromatin pattern.
Question 9:
During the operative fixation of a primarily ligamentous Lisfranc injury involving the entire tarsometatarsal joint complex, which of the following represents the correct anatomical order and trajectory for the primary 'Lisfranc screw'?
Options:
- From the medial cuneiform to the base of the second metatarsal
- From the base of the second metatarsal to the medial cuneiform
- From the intermediate cuneiform to the base of the first metatarsal
- From the medial cuneiform to the base of the third metatarsal
- From the navicular to the base of the second metatarsal
Correct Answer: From the medial cuneiform to the base of the second metatarsal
Explanation:
The primary Lisfranc ligament is an intra-articular ligament that connects the medial cuneiform to the base of the second metatarsal. The anatomical and biomechanically optimal trajectory for the classic 'Lisfranc screw' mimics this ligament, starting from the medial cuneiform and directed laterally and distally into the base of the second metatarsal.
Question 10:
The anterior cruciate ligament (ACL) is composed of two primary bundles, the anteromedial (AM) and posterolateral (PL) bundles. During physiologic knee range of motion, how do the tension patterns of these distinct bundles behave?
Options:
- The AM bundle becomes tight in flexion, while the PL bundle is tight in extension
- Both bundles become equally tight in flexion
- The PL bundle becomes tight in flexion, while the AM bundle is tight in extension
- Both bundles are lax in flexion and tight in extension
- The tension of both bundles remains constant throughout the range of motion
Correct Answer: The AM bundle becomes tight in flexion, while the PL bundle is tight in extension
Explanation:
The anteromedial (AM) bundle of the ACL is primarily tight in flexion and is the main restraint to anterior tibial translation at 90 degrees of flexion. The posterolateral (PL) bundle is tightest in extension and is the primary restraint against rotatory instability.
Question 11:
A 55-year-old female undergoes volar locking plate fixation for a displaced distal radius fracture. Six months postoperatively, she presents with a sudden inability to actively flex the interphalangeal joint of her thumb. Which of the following plate placement errors most likely contributed to this specific complication?
Options:
- Placement of the plate proximal to the watershed line
- Placement of the plate distal to the watershed line
- Use of excessively long dorsal screws
- Failure to repair the pronator quadratus
- Inadequate reduction of the volar lunate facet
Correct Answer: Placement of the plate distal to the watershed line
Explanation:
Flexor pollicis longus (FPL) tendon rupture is a known complication of volar plating of the distal radius. It is most commonly caused by placement of the plate too distally (distal to the 'watershed line'), leading to mechanical attrition of the tendon against the prominent distal edge of the plate during active thumb motion.
Question 12:
During a posterior-stabilized total knee arthroplasty, the surgeon performs gap balancing using tensioners. The knee is noted to be symmetric and well-balanced in full extension, but significantly tight in 90 degrees of flexion. Which of the following is the most appropriate intraoperative adjustment to achieve a balanced gap?
Options:
- Recut the distal femur to remove more bone
- Release the posterior cruciate ligament
- Downsize the femoral component
- Release the medial collateral ligament
- Increase the thickness of the polyethylene insert
Correct Answer: Downsize the femoral component
Explanation:
A knee that is tight in flexion but balanced in extension indicates an isolated tight flexion gap. Downsizing the femoral component (often utilizing an anterior referencing guide to avoid notching) decreases the anteroposterior dimension of the femur by taking more posterior condylar bone. This opens the flexion gap without altering the distal femoral cut (which controls the extension gap).
Question 13:
A 68-year-old male complains of bilateral leg pain and cramping that worsens after walking two blocks. Which of the following clinical findings most reliably differentiates neurogenic claudication (due to spinal stenosis) from vascular claudication?
Options:
- Pain relief occurs immediately upon standing still
- Pain is relieved by walking up an incline or leaning forward on a shopping cart
- Absent distal pedal pulses
- Loss of hair on the distal lower extremities
- Pain consistently starts in the calves and radiates proximally
Correct Answer: Pain is relieved by walking up an incline or leaning forward on a shopping cart
Explanation:
Neurogenic claudication is exacerbated by lumbar extension (which decreases the cross-sectional area of the spinal canal) and relieved by lumbar flexion. Therefore, activities that promote lumbar flexion, such as walking uphill or leaning forward on a shopping cart (the 'shopping cart sign'), alleviate symptoms. Vascular claudication is workload-dependent and is relieved by simply standing still, regardless of posture.
Question 14:
A 6-year-old boy sustains a completely displaced (Gartland Type III) supracondylar humerus fracture. On initial presentation in the emergency department, his hand is warm and well-perfused (pink), but the radial pulse is absent on palpation and Doppler ultrasound. What is the most appropriate next step in management?
Options:
- Immediate surgical exploration of the brachial artery
- CT angiography of the upper extremity
- Urgent closed reduction and percutaneous pinning
- Application of a long arm cast in 90 degrees of flexion
- Observation and elevation for 24 hours
Correct Answer: Urgent closed reduction and percutaneous pinning
Explanation:
The standard of care for a 'pulseless, pink' hand in the setting of a displaced pediatric supracondylar humerus fracture is urgent closed reduction and percutaneous pinning (CRPP). Realigning the fracture relieves the tethering, kinking, or spasm of the brachial artery over the proximal fragment, often restoring the pulse. Vascular exploration is indicated if the hand is 'pulseless and pale' (ischemic) before or after reduction.
Question 15:
According to the modified Verdan classification of flexor tendon zones in the hand, which zone is historically referred to as 'no man's land' due to the high propensity for adhesion formation and poor surgical outcomes?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Zone II extends from the proximal edge of the A1 pulley to the insertion of the flexor digitorum superficialis (FDS). Historically, it was termed 'no man's land' by Sterling Bunnell because both the FDS and FDP tendons run tightly together within the narrow fibro-osseous sheath, making primary repair technically demanding and highly prone to restrictive adhesions.
Question 16:
A 24-year-old professional baseball pitcher undergoes shoulder arthroscopy. A Type II SLAP (Superior Labrum Anterior to Posterior) lesion is identified. Which of the following best describes the pathomechanics of a Type II SLAP lesion?
Options:
- Fraying of the superior labrum with an intact biceps anchor
- Detachment of the superior labrum and the origin of the long head of the biceps from the superior glenoid tubercle
- A bucket-handle tear of the superior labrum with an intact biceps anchor
- A bucket-handle tear of the superior labrum that extends into the biceps tendon
- An anteroinferior labral detachment with an associated Hill-Sachs lesion
Correct Answer: Detachment of the superior labrum and the origin of the long head of the biceps from the superior glenoid tubercle
Explanation:
A Type II SLAP lesion involves the detachment of the superior labrum and the origin of the long head of the biceps tendon from the superior glenoid tubercle. Type I is fraying; Type III is a bucket-handle tear with an intact anchor; Type IV is a bucket-handle tear extending into the biceps tendon.
Question 17:
In the initial ATLS resuscitation of a hemodynamically unstable patient with an Anteroposterior Compression Type III (APC-III) pelvic ring injury, what is the most appropriate anatomical landmark for the application of a non-invasive pelvic circumferential compression device (pelvic binder)?
Options:
- Over the anterior superior iliac spines (ASIS)
- Over the greater trochanters of the femurs
- Just proximal to the iliac crests
- Around the mid-thighs
- Directly over the pubic symphysis
Correct Answer: Over the greater trochanters of the femurs
Explanation:
Pelvic binders must be placed at the level of the greater trochanters to effectively close the pelvic ring and reduce pelvic volume. Placement over the ASIS or iliac crests is a common clinical error and can paradoxically open the true pelvis further in APC-type injuries by acting as a fulcrum.
Question 18:
A 14-year-old male presents with a painful mass in the diaphysis of the left femur. Radiographs show a permeative, destructive lesion with an 'onion-skin' periosteal reaction. A core needle biopsy is performed. Which of the following chromosomal translocations is most pathognomonic for this tumor?
Options:
- t(11;22)(q24;q12)
- t(X;18)(p11;q11)
- t(12;16)(q13;p11)
- t(9;22)(q34;q11)
- t(2;13)(q35;q14)
Correct Answer: t(11;22)(q24;q12)
Explanation:
The clinical and radiographic picture describes Ewing's sarcoma. The pathognomonic chromosomal translocation for Ewing's sarcoma is t(11;22)(q24;q12), which results in the EWS-FLI1 fusion protein. t(X;18) is seen in synovial sarcoma; t(12;16) in myxoid liposarcoma; t(9;22) in CML; and t(2;13) in alveolar rhabdomyosarcoma.
Question 19:
According to Perren's strain theory of bone healing, what is the maximum amount of interfragmentary strain that can be tolerated for primary (direct) bone healing to occur without the formation of a visible fracture callus?
Options:
- Less than 2%
- Between 2% and 10%
- Between 10% and 30%
- Greater than 30%
- 100%
Correct Answer: Less than 2%
Explanation:
According to Perren's strain theory, primary (direct) bone healing via cutting cones requires absolute stability. This corresponds to an interfragmentary strain of less than 2%. Secondary bone healing (which involves callus formation) occurs at strains between 2% and 10%. Granulation tissue forms at strains up to 100%.
Question 20:
A 60-year-old active male underwent a total hip arthroplasty using a ceramic-on-ceramic bearing surface two years ago. He now presents complaining of a high-pitched 'squeaking' sound emanating from the hip during walking, bending, and stair climbing. Which of the following component malpositions is most strongly associated with this phenomenon?
Options:
- Excessive cup anteversion and vertical cup inclination
- Cup retroversion and excessive cup adduction
- Femoral stem retroversion
- Excessive femoral offset
- Inadequate limb length restoration
Correct Answer: Excessive cup anteversion and vertical cup inclination
Explanation:
Audible 'squeaking' is a unique complication of ceramic-on-ceramic (CoC) bearing surfaces. It is most strongly associated with edge-loading of the components, which disrupts fluid film lubrication. Edge-loading is most commonly caused by component malposition, specifically excessive cup abduction (steep vertical cup inclination) and/or excessive cup anteversion.
Question 21:
A 14-year-old boy with an acute-on-chronic Slipped Capital Femoral Epiphysis (SCFE) is treated with in-situ single screw fixation. Six months later, he presents with severe hip stiffness, pain, and loss of all hip motion. Radiographs demonstrate uniform narrowing of the joint space to less than 3 mm. Which of the following is the most established primary risk factor for this specific complication?
Options:
- Unrecognized screw penetration into the joint
- Unstable slip classification at presentation
- Body Mass Index greater than the 95th percentile
- Underlying undiagnosed hypothyroidism
- Failure to perform prophylactic pinning of the contralateral hip
Correct Answer: Unrecognized screw penetration into the joint
Explanation:
The clinical presentation describes chondrolysis, a devastating complication of SCFE characterized by acute loss of articular cartilage and severe stiffness. The most strongly associated risk factor for chondrolysis following SCFE fixation is unrecognized pin/screw penetration into the joint space. An unstable slip is a risk factor for avascular necrosis (AVN), not primarily chondrolysis.
Question 22:
A 32-year-old female with a recurrent Giant Cell Tumor (GCT) of the distal femur is started on neoadjuvant medical therapy to facilitate joint-salvage surgery. She is given Denosumab, a human monoclonal antibody. What is the exact cellular target and mechanism of action of this medication in the context of GCT?
Options:
- Binds to the RANK receptor on the reactive osteoclast-like giant cells
- Binds to RANKL expressed by the neoplastic mononuclear stromal cells
- Acts as an analogue to Osteoprotegerin (OPG) on osteoblasts
- Inhibits Vascular Endothelial Growth Factor (VEGF) preventing angiogenesis
- Inhibits tyrosine kinase receptors in the neoplastic giant cells
Correct Answer: Binds to RANKL expressed by the neoplastic mononuclear stromal cells
Explanation:
Denosumab is a monoclonal antibody that targets Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL). In Giant Cell Tumor of bone, the neoplastic cells are the mononuclear stromal cells, which express high levels of RANKL. Denosumab binds this RANKL, preventing it from binding to the RANK receptor on the reactive (non-neoplastic) osteoclast-like giant cells, thereby halting their recruitment, maturation, and bone-resorbing activity.
Question 23:
A 45-year-old manual laborer presents with chronic right wrist pain. Radiographs reveal severe joint space narrowing at the radioscaphoid and capitolunate joints. The radiolunate joint is completely preserved. Given this specific pattern of arthritis, which of the following surgical procedures is considered contraindicated?
Options:
- Four-corner fusion with scaphoid excision
- Proximal row carpectomy (PRC)
- Total wrist arthrodesis
- Wrist denervation
- Scaphoid excision and capitolunate arthrodesis
Correct Answer: Proximal row carpectomy (PRC)
Explanation:
The radiographic findings describe Scapholunate Advanced Collapse (SLAC) Stage III, characterized by radioscaphoid and capitolunate arthritis with sparing of the radiolunate joint. Proximal row carpectomy (PRC) relies on a pristine capitate head to articulate with the lunate fossa of the radius. Because the capitate head is arthritic in Stage III SLAC, PRC is contraindicated. Four-corner fusion or total wrist arthrodesis are appropriate options.
Question 24:
During the acute trauma bay management of a hemodynamically unstable patient with an anteroposterior compression (APC) type III pelvic ring injury, a circumferential pelvic binder is applied. To achieve the maximal mechanical advantage for reducing pelvic volume, the binder must be centered exactly over which anatomical landmark?
Options:
- Iliac crests
- Anterior superior iliac spines (ASIS)
- Greater trochanters
- Level of the pubic symphysis
- Subtrochanteric femurs
Correct Answer: Greater trochanters
Explanation:
To effectively close the pelvic ring and reduce pelvic volume in open-book type fractures, the pelvic binder or sheet must be centered directly over the greater trochanters. Placement higher over the iliac crests is a common error and can paradoxically open the true pelvis further or fail to reduce the pubic symphysis effectively.
Question 25:
In total hip arthroplasty, periprosthetic osteolysis is primarily driven by a macrophage response to ultra-high-molecular-weight polyethylene (UHMWPE) wear particles. Which mechanism of wear is most responsible for generating the billions of submicron particles (0.1-1.0 micrometers) typically seen in a well-functioning metal-on-polyethylene articulation?
Options:
- Third-body wear
- Abrasive wear
- Adhesive wear
- Fatigue wear
- Corrosive wear
Correct Answer: Adhesive wear
Explanation:
Adhesive wear is the primary mechanism generating the biologically active submicron polyethylene particles in a well-functioning THA. It occurs when micro-asperities on the metal or ceramic head temporarily weld to the polyethylene surface and shear off during motion. Abrasive wear creates larger particles, and fatigue wear leads to delamination.
Question 26:
A 65-year-old male sustains a Type II odontoid fracture following a fall. Which of the following factors represents the strongest clinical predictor for nonunion if this injury is treated non-operatively with a halo vest?
Options:
- Concomitant anterior arch C1 fracture
- Anterior displacement of 3 mm
- Initial fracture displacement greater than 5 mm
- Patient gender
- Use of a rigid cervical collar instead of a halo vest
Correct Answer: Initial fracture displacement greater than 5 mm
Explanation:
Risk factors for nonunion in Type II odontoid fractures include initial displacement > 5 mm, age > 50 years, angulation > 10 degrees, posterior displacement, and delayed treatment. A displacement greater than 5 mm is a classic and highly significant predictor of nonunion, often prompting surgical management (e.g., anterior screw fixation or posterior C1-C2 fusion).
Question 27:
A 25-year-old athlete sustains a hyperplantarflexion injury to his midfoot. Weight-bearing radiographs demonstrate a 2 mm widening between the first and second metatarsal bases along with a subtle 'fleck sign'. The fleck sign represents a bony avulsion of the Lisfranc ligament from which specific anatomical structure?
Options:
- Base of the first metatarsal
- Base of the second metatarsal
- Medial cuneiform
- Middle cuneiform
- Navicular
Correct Answer: Base of the second metatarsal
Explanation:
The Lisfranc ligament is a strong interosseous ligament connecting the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. A 'fleck sign' on a radiograph represents an avulsion fracture of this ligament, almost exclusively pulling off from the base of the second metatarsal.
Question 28:
During an Anterior Cruciate Ligament (ACL) reconstruction, the surgeon tensions the quadrupled hamstring graft to a specific length and secures it. Over the next several minutes, the tension (force) required by the fixation device to maintain that exact length decreases. This physical phenomenon is characteristic of viscoelastic materials and is known as:
Options:
- Creep
- Stress relaxation
- Hysteresis
- Fatigue failure
- Isotropic elasticity
Correct Answer: Stress relaxation
Explanation:
Stress relaxation is the property of a viscoelastic material whereby the stress (internal force/tension) decreases over time when the material is held at a constant strain (length). Conversely, 'creep' is the increase in strain (deformation/length) over time when the material is subjected to a constant stress (load).
Question 29:
When evaluating graft choices for primary Anterior Cruciate Ligament (ACL) reconstruction, biomechanical studies demonstrate varying properties of ultimate tensile load. Which of the following graft constructs possesses the highest ultimate tensile load (strength) compared to the native ACL (~2160 N)?
Options:
- 10-mm Bone-Patellar Tendon-Bone (BPTB) autograft
- Quadrupled hamstring autograft
- 10-mm Quadriceps tendon autograft
- Achilles tendon allograft
- Native hamstring tendon (semitendinosus only)
Correct Answer: Quadrupled hamstring autograft
Explanation:
A quadrupled hamstring graft has an ultimate tensile load of roughly 4090 N, which is nearly twice that of the native ACL (~2160 N). By comparison, a 10-mm BPTB graft has an ultimate tensile load of approximately 2977 N, and a quadriceps tendon graft is about 2352 N. Therefore, the quadrupled hamstring graft is biomechanically the strongest of the standard autograft choices.
Question 30:
A 6-year-old boy presents with a Gartland Type III extension-type supracondylar humerus fracture. On initial exam, the hand is pink but lacks a palpable radial pulse. Following emergent closed reduction and percutaneous pinning in the operating room, the hand remains pink and pulseless, but capillary refill is brisk (<2 seconds). What is the most appropriate next step in management?
Options:
- Immediate removal of pins and transition to open reduction
- Emergent anterior approach for brachial artery exploration
- Observation and admission for 24-48 hours
- Doppler ultrasound of the radial artery in the PACU
- Formal angiography of the upper extremity
Correct Answer: Observation and admission for 24-48 hours
Explanation:
The management of a 'pink, pulseless' hand after satisfactory reduction and pinning of a pediatric supracondylar humerus fracture is observation. The brisk capillary refill indicates adequate collateral perfusion. Vascular exploration is strictly indicated if the hand is 'white and pulseless' (ischemic) after reduction.
Question 31:
In the modern treatment protocol for high-grade, non-metastatic intramedullary osteosarcoma, surgical resection is typically preceded by neoadjuvant chemotherapy. Following surgical resection, which of the following histological parameters is the most important prognostic factor for the patient's long-term overall survival?
Options:
- The histological subtype (osteoblastic vs. chondroblastic)
- The exact anatomic location of the tumor
- The percentage of tumor necrosis induced by chemotherapy
- The mitotic index of the residual tumor cells
- The presence of skip metastases on MRI
Correct Answer: The percentage of tumor necrosis induced by chemotherapy
Explanation:
The degree of tumor necrosis following neoadjuvant chemotherapy (graded by the Huvos system) is the single most important prognostic indicator for overall survival in patients with non-metastatic high-grade osteosarcoma. A necrosis rate of >90% (Huvos grade III or IV) defines a 'good responder' and correlates strongly with improved survival.
Question 32:
A 60-year-old male with a metal-on-metal total hip arthroplasty presents 5 years post-operatively with worsening groin pain and a palpable anterior soft tissue mass. Aspiration yields sterile, turbid fluid. Revision surgery is planned. Histological analysis of the pseudotumor (periprosthetic tissue) is most likely to demonstrate:
Options:
- Massive acute infiltration of polymorphonuclear leukocytes
- Birefringent particulate debris under polarized light with foreign body giant cells
- Extensive perivascular lymphocytic infiltration
- Sheets of lipid-laden macrophages (foam cells)
- Monoclonal B-cell proliferation
Correct Answer: Extensive perivascular lymphocytic infiltration
Explanation:
The clinical scenario describes an Aseptic Lymphocyte-Dominated Vasculitis-Associated Lesion (ALVAL), a delayed Type IV hypersensitivity reaction uniquely associated with metal-on-metal bearings. The hallmark histological finding is a dense perivascular infiltrate of T-lymphocytes. Birefringent particles with giant cells are typical of polyethylene wear (macrophage-mediated osteolysis).
Question 33:
During a primary Zone II flexor tendon repair, a surgeon considers the biomechanical trade-offs of different suture configurations. Increasing the number of core suture strands crossing the repair site primarily improves which specific biomechanical property of the repaired tendon?
Options:
- Resistance to gap formation under cyclic loading
- Tendon glide during early active motion protocols
- Work of flexion
- Ultimate tensile strength of the repair
- Intrinsic cellular healing rate
Correct Answer: Ultimate tensile strength of the repair
Explanation:
The ultimate tensile strength of a flexor tendon repair is directly proportional to the number of core suture strands crossing the repair site (e.g., a 4-strand repair is generally stronger than a 2-strand repair). However, increasing strands also increases the bulk of the repair, which can negatively impact tendon glide and increase the 'work of flexion' through the pulley system.
Question 34:
A 40-year-old female sustains a high-energy trauma and presents with an isolated coronal plane shear fracture of the distal femoral condyle. Regarding this specific injury (Hoffa fracture), which of the following statements is most accurate?
Options:
- It most commonly involves the lateral femoral condyle
- It is classified as an AO/OTA type 33-A fracture
- It primarily occurs as a result of a direct varus blow to an extended knee
- Non-operative management with a hinged knee brace is standard of care
- It is typically best visualized on a standard anteroposterior (AP) radiograph
Correct Answer: It most commonly involves the lateral femoral condyle
Explanation:
A Hoffa fracture is a coronal shear fracture of the distal femur (AO/OTA 33-B3). It most commonly involves the lateral femoral condyle due to the natural physiological valgus of the knee and the lateral vector of forces transmitted during the typical axial loading mechanism (often with the knee flexed). It is best visualized on a lateral radiograph or CT scan and requires surgical fixation.
Question 35:
A 55-year-old patient with long-standing poorly controlled diabetes presents with a unilaterally swollen, erythematous, and warm foot without skin ulceration. Radiographs demonstrate extensive periarticular debris, bony fragmentation, and early subluxation of the tarsometatarsal joints. According to the Eichenholtz classification of Charcot arthropathy, this presentation corresponds to:
Options:
- Stage 0
- Stage I
- Stage II
- Stage III
- Stage IV
Correct Answer: Stage I
Explanation:
The Eichenholtz classification of Charcot arthropathy includes: Stage 0 (high-risk foot, swelling, warmth, normal x-rays); Stage I (Developmental/Fragmentation: hyperemic, fragmentation, debris, subluxation); Stage II (Coalescence: decreased swelling/warmth, absorption of fine debris, early fusion); Stage III (Consolidation: remodeling, stable deformity). The clinical and radiographic findings match Stage I.
Question 36:
A 68-year-old man presents with bilateral leg heaviness, cramping, and pain that severely limits his walking distance. Which of the following historical features or clinical tests most reliably differentiates neurogenic claudication (due to lumbar spinal stenosis) from vascular claudication?
Options:
- Immediate pain relief simply by stopping walking and standing stationary
- Pain relief when leaning forward or riding a stationary bicycle
- Presence of severe pain at rest in the distal lower extremities
- Exacerbation of leg pain with lumbar flexion maneuvers
- Loss of protective sensation using a 10-g monofilament
Correct Answer: Pain relief when leaning forward or riding a stationary bicycle
Explanation:
The bicycle test of van Gelderen is a classic method to differentiate neurogenic from vascular claudication. In neurogenic claudication, spinal flexion (such as leaning forward on a bike) opens the central canal and neural foramina, relieving ischemia to the nerve roots and preventing pain. In vascular claudication, the increased metabolic demand of the leg muscles during cycling will provoke pain regardless of the flexed posture.
Question 37:
A 28-year-old football player is evaluated for acute knee instability. The tibial dial test is performed in the supine position. The examiner notes >10 degrees of increased external rotation on the injured side compared to the normal side when the knee is flexed at 30 degrees. However, when the knee is flexed to 90 degrees, the external rotation is symmetric bilaterally. This specific pattern confirms injury to which structure(s)?
Options:
- Isolated Posterolateral Corner (PLC)
- Combined Posterolateral Corner (PLC) and Posterior Cruciate Ligament (PCL)
- Isolated Posterior Cruciate Ligament (PCL)
- Anterolateral Ligament (ALL) and Anterior Cruciate Ligament (ACL)
- Medial Collateral Ligament (MCL) and Posterior Oblique Ligament (POL)
Correct Answer: Isolated Posterolateral Corner (PLC)
Explanation:
The dial test assesses external rotation of the tibia. Increased external rotation (>10 degrees compared to the contralateral side) at 30 degrees of flexion indicates an injury to the Posterolateral Corner (PLC). If the external rotation reduces and becomes symmetric at 90 degrees, the PCL is intact (isolated PLC injury). If external rotation is increased at both 30 and 90 degrees, it indicates a combined PCL and PLC injury.
Question 38:
Bone Morphogenetic Proteins (BMPs), specifically BMP-2 and BMP-7, are utilized clinically for their potent osteoinductive capabilities. Upon binding to their respective cell surface receptors, which specific intracellular signaling pathway is primarily activated to upregulate osteogenic gene transcription?
Options:
- Wnt / beta-catenin pathway
- JAK-STAT signaling pathway
- Smad signaling pathway
- MAPK / ERK signaling pathway
- Notch signaling cascade
Correct Answer: Smad signaling pathway
Explanation:
BMPs are members of the TGF-beta superfamily. When they bind to their specific serine/threonine kinase transmembrane receptors, they induce phosphorylation of receptor-regulated Smads (R-Smads, such as Smad 1, 5, and 8). These form a complex with the common-partner Smad 4, which then translocates to the nucleus to act as a transcription factor for osteogenic genes (e.g., Runx2).
Question 39:
The Ponseti method relies on a precise, sequential manipulation and casting technique to treat idiopathic congenital talipes equinovarus (clubfoot). Which of the following represents the correct anatomical order of deformity correction dictated by this method?
Options:
- Cavus, Adductus, Varus, Equinus
- Equinus, Varus, Adductus, Cavus
- Adductus, Cavus, Varus, Equinus
- Cavus, Varus, Adductus, Equinus
- Varus, Adductus, Cavus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The correct sequence of correction in the Ponseti method is easily remembered by the mnemonic CAVE: Cavus (corrected by supinating the forefoot and elevating the first ray), Adductus, Varus (adductus and varus correct together as the forefoot is abducted around the fulcrum of the talar head), and finally Equinus (which often requires a percutaneous Achilles tenotomy as the final step).
Question 40:
A surgeon is templating for a primary Total Hip Arthroplasty (THA) and wishes to maximize the primary arc of motion to delay mechanical impingement of the components, thereby reducing dislocation risk. Which of the following geometric modifications to the implant will most effectively achieve this goal?
Options:
- Maximizing the head-to-neck ratio
- Minimizing the head-to-neck ratio
- Increasing the femoral neck diameter
- Using a skirted modular femoral head
- Decreasing the lateral femoral offset
Correct Answer: Maximizing the head-to-neck ratio
Explanation:
The impingement-free primary arc of motion in a THA is mathematically driven by the head-to-neck ratio. Maximizing this ratio (by using a larger diameter femoral head and a smaller diameter femoral neck) allows for greater excursion of the neck before it contacts the acetabular rim. Skirted heads and thicker necks decrease this ratio, causing earlier impingement and increasing dislocation risk.
Question 41:
A 52-year-old mechanic presents with chronic, progressive wrist pain. Radiographs demonstrate scapholunate advanced collapse (SLAC) with severe narrowing of the radioscaphoid and capitolunate joints, while the radiolunate joint is preserved. A proximal row carpectomy (PRC) is being considered. Which of the following radiographic findings in this patient is an absolute contraindication to performing a PRC?
Options:
- A scapholunate interval greater than 3 mm
- Severe radioscaphoid arthritis
- Capitolunate arthritis
- Preservation of the radiolunate joint
- Ulnar positive variance
Correct Answer: Capitolunate arthritis
Explanation:
Proximal row carpectomy (PRC) relies on a healthy articulation between the lunate fossa of the distal radius and the proximal capitate. Capitolunate arthritis (which occurs in Stage III SLAC wrist) is a contraindication to PRC, as the new joint formed would be arthritic and painful. In such cases, a four-corner fusion with scaphoid excision is the preferred surgical option.
Question 42:
A 2-week-old infant with idiopathic clubfoot is undergoing correction via the Ponseti method. The treating physician applies the first cast. According to Ponseti principles, what is the primary goal of the very first cast application?
Options:
- Correction of the cavus deformity by elevating the first ray
- Correction of the forefoot adductus by manipulating the metatarsals
- Correction of the hindfoot varus by abducting the foot
- Correction of the hindfoot equinus by dorsiflexing the ankle
- Correction of internal tibial torsion
Correct Answer: Correction of the cavus deformity by elevating the first ray
Explanation:
The Ponseti method corrects the components of clubfoot in a specific sequence: Cavus, Adductus, Varus, and Equinus (CAVE). The first step requires elevation of the first ray (dorsiflexion of the first metatarsal) to correct the forefoot cavus. This aligns the forefoot with the hindfoot, allowing the foot to be treated as a single unit during subsequent abduction.
Question 43:
A 26-year-old male is brought to the emergency department after a motorcycle collision. Pelvic radiographs reveal an anteroposterior compression (APC) injury. Which of the following findings defines an APC III pelvic ring injury according to the Young-Burgess classification?
Options:
- Symphysis widening less than 2.5 cm with intact posterior ligaments
- Disruption of the anterior sacroiliac ligaments with intact posterior sacroiliac ligaments
- Complete disruption of the pubic symphysis and both the anterior and posterior sacroiliac ligaments
- Sacral fracture with an ipsilateral superior and inferior rami fracture
- A crescent fracture of the posterior ilium
Correct Answer: Complete disruption of the pubic symphysis and both the anterior and posterior sacroiliac ligaments
Explanation:
In the Young-Burgess classification, APC injuries are divided by severity. APC I is symphyseal diastasis <2.5 cm. APC II is symphyseal diastasis >2.5 cm with disruption of the anterior sacroiliac, sacrotuberous, and sacrospinous ligaments, but intact posterior sacroiliac ligaments. APC III involves complete disruption of both anterior and posterior sacroiliac ligaments, leading to a completely unstable hemipelvis.
Question 44:
During medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, accurate femoral tunnel placement is critical to avoid graft mal-tensioning. Radiographically, 'Schöttle/'s point' is used to identify the anatomic femoral footprint. Anatomically, where is this point located?
Options:
- 1 cm distal to the medial epicondyle
- In the saddle region between the adductor tubercle and the medial epicondyle
- Directly on the prominence of the adductor tubercle
- 2 cm anterior to the medial epicondyle
- At the insertion of the superficial medial collateral ligament
Correct Answer: In the saddle region between the adductor tubercle and the medial epicondyle
Explanation:
The anatomic femoral origin of the MPFL is located in the saddle-shaped depression between the adductor tubercle (proximal) and the medial epicondyle (distal). Radiographically, Schöttle's point is 1 mm anterior to the posterior cortex line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to Blumensaat's line.
Question 45:
A 58-year-old female with a history of a metal-on-metal total hip arthroplasty presents with groin pain and a palpable anterior mass. Aspiration yields sterile fluid, and revision surgery is performed. Histopathological examination of the periprosthetic tissue is most likely to reveal which of the following?
Options:
- Extensive polymorphonuclear leukocyte infiltration
- A dense monocyte/macrophage response laden with birefringent particles
- An aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL)
- Non-caseating granulomas with central necrosis
- Sheets of eosinophils and mast cells
Correct Answer: An aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL)
Explanation:
Adverse local tissue reactions (ALTR) or pseudotumors in metal-on-metal implants are characterized histologically by an aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL). This is a Type IV delayed hypersensitivity response to metal ions (cobalt and chromium), distinct from the macrophage-dominated response seen in traditional polyethylene wear (particle disease).
Question 46:
Biomechanical testing of a human anterior cruciate ligament graft is performed. When a constant load (stress) is applied to the ligament over an extended period, the ligament undergoes a gradual increase in length (strain). This viscoelastic property is best defined as:
Options:
- Stress relaxation
- Creep
- Hysteresis
- Fatigue failure
- Isotropy
Correct Answer: Creep
Explanation:
Creep is the viscoelastic property where a tissue undergoes continuous, time-dependent deformation (elongation or strain) under a constant applied load (stress). In contrast, stress relaxation is the decrease in stress over time when the tissue is held at a constant length (strain).
Question 47:
A 15-year-old male presents with painful thoracolumbar scoliosis. Imaging reveals a 7 mm radiolucent nidus with surrounding sclerosis in the pedicle of T11 on the concave side of the curve. The lesion is situated 2 mm from the traversing nerve root. What is the most appropriate definitive management?
Options:
- Radiofrequency ablation (RFA)
- Prolonged immobilization in a TLSO brace
- Percutaneous cryoablation
- En bloc spondylectomy
- Surgical curettage and/or excision
Correct Answer: Surgical curettage and/or excision
Explanation:
The diagnosis is an osteoid osteoma causing painful secondary scoliosis. While radiofrequency ablation (RFA) is the standard of care for most appendicular osteoid osteomas, it is relatively contraindicated for spinal lesions located within 1 cm of neural elements due to the high risk of thermal nerve injury. In such cases, open or minimally invasive surgical curettage/excision is preferred.
Question 48:
A 68-year-old male presents with progressive clumsiness in his hands and difficulty buttoning his shirts. Physical examination raises suspicion for cervical spondylotic myelopathy. The examiner tests for a Hoffmann sign. A positive response is indicated by which of the following movements when the nail of the patient/'s middle finger is briskly flicked downward?
Options:
- Extension of the thumb and index finger
- Flexion of the interphalangeal joint of the thumb and index finger
- Abduction of the little finger
- Rapid pronation of the forearm
- Isolated flexion of the middle finger
Correct Answer: Flexion of the interphalangeal joint of the thumb and index finger
Explanation:
Hoffmann's sign is an indicator of upper motor neuron damage, often seen in cervical myelopathy. It is elicited by stabilizing the patient's middle finger and briskly flicking the distal phalanx downward. A positive test is the reflexive flexion of the interphalangeal joint of the thumb and/or index finger.
Question 49:
A 45-year-old male sustains a high-energy varus directed force to his knee, resulting in a Schatzker IV tibial plateau fracture. CT scanning demonstrates a displaced coronal shear fracture of the posteromedial tibial plateau. Which surgical approach provides the most optimal visualization and biomechanical advantage for buttress plating of this specific fragment?
Options:
- Standard anterolateral approach
- Anterior midline approach
- Posteromedial approach
- Direct medial approach
- Lateral parapatellar approach
Correct Answer: Posteromedial approach
Explanation:
A displaced posteromedial fragment of a tibial plateau fracture (often seen in Schatzker IV) is notoriously difficult to reduce and fix from an anterior or direct medial approach. The posteromedial approach allows direct visualization of the fracture apex and permits the application of a posteromedial buttress plate, which mechanically opposes the deforming forces.
Question 50:
A 55-year-old patient with poorly controlled type 2 diabetes presents with a unilaterally swollen, erythematous, and warm foot without open ulcerations. Radiographs show periarticular fragmentation, subluxation, and bony debris at the tarsometatarsal joints. According to the Eichenholtz classification, what is the stage of this disease process and the standard initial management?
Options:
- Stage 0; rigid internal fixation
- Stage 1; total contact casting and non-weight bearing
- Stage 2; immediate midfoot arthrodesis
- Stage 3; custom accommodative shoe wear
- Stage 1; urgent surgical debridement and intravenous antibiotics
Correct Answer: Stage 1; total contact casting and non-weight bearing
Explanation:
The patient has Stage 1 (Developmental/Fragmentation stage) Charcot arthropathy, characterized by erythema, swelling, warmth, and radiographic evidence of fragmentation and subluxation. The standard of care for acute Stage 1 Charcot is immediate offloading, most effectively achieved with total contact casting (TCC) and non-weight bearing to prevent further collapse.
Question 51:
A 23-year-old elite collegiate gymnast presents with vague anterior shoulder pain and a catching sensation. MRI arthrogram demonstrates a detachment of the superior labrum and the origin of the long head of the biceps tendon from the glenoid, without extension into the anterior or posterior labrum. What is the classification of this injury and the historically accepted gold standard surgical treatment for a young athletic patient?
Options:
- Type I SLAP; simple debridement
- Type II SLAP; superior labral repair with suture anchors
- Type III SLAP; biceps tenodesis
- Type IV SLAP; biceps tenotomy
- Type II SLAP; open subpectoral biceps tenodesis
Correct Answer: Type II SLAP; superior labral repair with suture anchors
Explanation:
This describes a Type II SLAP tear (detachment of the superior labrum and biceps anchor). In young, high-demand athletes (like a 23-year-old gymnast), the traditional gold standard treatment is an arthroscopic superior labral repair using suture anchors. Tenodesis is increasingly favored in older patients (>35-40) or workers with heavy lifting requirements, but labral repair remains the standard for young athletes.
Question 52:
An 8-week-old female infant is undergoing treatment for developmental dysplasia of the hip (DDH) with a Pavlik harness. During a routine clinical check, the orthopedic surgeon notes that the infant has decreased active extension of the knee on the affected side, and the patellar reflex is diminished. What is the most likely cause of this finding and the appropriate harness adjustment?
Options:
- Femoral nerve palsy from excessive hip flexion; loosen the anterior straps
- Sciatic nerve palsy from excessive hip flexion; tighten the posterior straps
- Obturator nerve palsy from excessive hip abduction; loosen the posterior straps
- Avascular necrosis of the femoral head from excessive hip abduction; discontinue the harness
- Normal variant of Pavlik harness use; maintain current strap settings
Correct Answer: Femoral nerve palsy from excessive hip flexion; loosen the anterior straps
Explanation:
The clinical findings of decreased active knee extension and a diminished patellar reflex indicate a femoral nerve palsy. In the setting of a Pavlik harness, this is almost always caused by hyperflexion of the hips compressing the nerve. The appropriate management is to loosen the anterior straps to reduce the degree of hip flexion, which usually leads to complete resolution of the palsy.
Question 53:
In the context of fracture healing and bone grafting, various Bone Morphogenetic Proteins (BMPs) have been extensively studied. Which specific recombinant human BMP is currently FDA-approved for use as an adjunct in the treatment of acute, open tibial shaft fractures treated with an intramedullary nail?
Options:
- rhBMP-2
- rhBMP-3
- rhBMP-4
- rhBMP-7
- rhBMP-9
Correct Answer: rhBMP-2
Explanation:
rhBMP-2 (Infuse) is FDA-approved for use in acute, open tibial shaft fractures stabilized with an intramedullary nail, as well as for anterior lumbar interbody fusion (ALIF). rhBMP-7 (OP-1) was previously available under a Humanitarian Device Exemption for recalcitrant long bone nonunions but is no longer widely commercialized. The others are not FDA-approved for these indications.
Question 54:
A 6-year-old boy presents to the emergency department after falling off monkey bars. Radiographs demonstrate a fracture of the ulnar diaphysis with an associated anterior dislocation of the radial head. According to the Bado classification of Monteggia fracture-dislocations, what type of injury is this, and what is its relative frequency in the pediatric population?
Options:
- Type I; it is the most common type in children
- Type II; it is the most common type in children
- Type III; it is the least common type in children
- Type IV; it is the most common type in children
- Type I; it is exclusively seen in adults
Correct Answer: Type I; it is the most common type in children
Explanation:
The Bado classification describes Monteggia fractures based on the direction of radial head dislocation. Type I involves an anterior dislocation, Type II posterior, Type III lateral, and Type IV involves fractures of both the radius and ulna with an anterior radial head dislocation. Type I is the most common variant, especially in pediatric populations.
Question 55:
A 60-year-old male is evaluated for a medial unicompartmental knee arthroplasty (UKA) due to isolated medial compartment osteoarthritis. Which of the following is considered an absolute contraindication to proceeding with a medial UKA?
Options:
- Age greater than 55 years
- Body Mass Index of 30
- A flexible varus deformity of 5 degrees
- Inflammatory arthritis (e.g., Rheumatoid Arthritis)
- Intact anterior cruciate ligament (ACL)
Correct Answer: Inflammatory arthritis (e.g., Rheumatoid Arthritis)
Explanation:
Absolute contraindications for unicompartmental knee arthroplasty (UKA) include inflammatory arthropathies (such as Rheumatoid Arthritis), absent or deficient anterior cruciate ligament (though some modern debate exists, historically it is an absolute contraindication), tri-compartmental arthritis, fixed varus deformity > 10 degrees, fixed valgus > 5 degrees, and flexion contracture > 15 degrees. An intact ACL is an indication, not a contraindication.
Question 56:
In the anatomic classification of flexor tendon injuries of the hand, Zone II (historically termed 'no man/'s land' due to poor surgical outcomes in the past) presents significant challenges for repair. What are the proximal and distal anatomic boundaries that define Zone II?
Options:
- From the transverse carpal ligament to the proximal edge of the A1 pulley
- From the proximal edge of the A1 pulley to the insertion of the flexor digitorum superficialis (FDS)
- From the insertion of the FDS to the insertion of the flexor digitorum profundus (FDP)
- From the musculotendinous junction to the transverse carpal ligament
- From the A2 pulley to the A4 pulley
Correct Answer: From the proximal edge of the A1 pulley to the insertion of the flexor digitorum superficialis (FDS)
Explanation:
Zone II of the flexor tendon system begins at the proximal edge of the A1 pulley (at the level of the distal palmar crease) and extends distally to the insertion of the flexor digitorum superficialis (FDS) tendon on the middle phalanx. Both the FDS and FDP travel together within the narrow fibro-osseous sheath in this zone, making repairs prone to adhesions.
Question 57:
A 34-year-old construction worker falls 10 feet, sustaining a T12 burst fracture. He is neurologically intact. CT and MRI scans reveal a burst morphology with 25% canal compromise and an intact posterior ligamentous complex (PLC). Using the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the most appropriate treatment recommendation?
Options:
- Score 2; Non-operative management
- Score 4; Operative management
- Score 5; Operative management
- Score 7; Operative management
- Score 2; Operative management
Correct Answer: Score 2; Non-operative management
Explanation:
The TLICS system scores injuries based on three categories: Morphology, Neurologic Status, and PLC integrity. For this patient: Morphology is a burst fracture (2 points). Neurologic status is intact (0 points). PLC is intact (0 points). Total score = 2. A score of 3 or less dictates non-operative management. A score of 4 is equivocal, and 5 or more indicates surgery.
Question 58:
A 12-year-old girl presents with deep, achy leg pain. Radiographs demonstrate a permeative, lytic lesion in the diaphysis of the femur with an 'onion skin' periosteal reaction. Biopsy confirms Ewing sarcoma. Which of the following chromosomal translocations is the genetic hallmark of this malignancy?
Options:
- t(11;22)(q24;q12)
- t(X;18)(p11;q11)
- t(9;22)(q34;q11)
- t(2;13)(q35;q14)
- t(12;16)(q13;p11)
Correct Answer: t(11;22)(q24;q12)
Explanation:
Ewing sarcoma is characterized by the t(11;22)(q24;q12) translocation in about 85-90% of cases, resulting in the EWS-FLI1 fusion gene. t(X;18) is associated with synovial sarcoma; t(9;22) is the Philadelphia chromosome seen in CML; t(2;13) is seen in alveolar rhabdomyosarcoma; and t(12;16) is characteristic of myxoid liposarcoma.
Question 59:
Recent high-level evidence and meta-analyses comparing operative versus non-operative management of acute Achilles tendon ruptures highlight specific complication profiles. When modern functional rehabilitation protocols (early weight-bearing and motion) are utilized for both groups, which of the following is true?
Options:
- Operative treatment demonstrates significantly greater long-term plantarflexion power
- Non-operative treatment has a statistically higher rate of deep venous thrombosis
- Operative treatment eliminates the risk of sural nerve injury
- There is no clinically significant difference in re-rupture rates between the two groups
- Non-operative treatment has a zero percent re-rupture rate
Correct Answer: There is no clinically significant difference in re-rupture rates between the two groups
Explanation:
Historically, non-operative management of Achilles tendon ruptures (involving prolonged rigid immobilization) was associated with higher re-rupture rates. However, recent randomized controlled trials and meta-analyses demonstrate that when modern functional rehabilitation (early motion and weight-bearing in a boot) is employed, there is no significant difference in re-rupture rates between operative and non-operative groups, though operative management carries higher risks of infection and nerve injury.
Question 60:
Historical anatomical teachings suggested that the anterior circumflex humeral artery was the primary blood supply to the humeral head. However, recent quantitative anatomical studies utilizing gadolinium enhancement have redefined this vascularity. Which vessel has been definitively shown to supply the vast majority (over 60%) of the blood flow to the humeral head?
Options:
- Anterolateral branch of the anterior circumflex humeral artery
- Posterior circumflex humeral artery
- Acromial branch of the thoracoacromial artery
- Suprascapular artery
- Circumflex scapular artery
Correct Answer: Posterior circumflex humeral artery
Explanation:
Classic teachings by Gerber et al. suggested the arcuate branch of the anterior circumflex humeral artery provided the main blood supply to the humeral head. However, more recent landmark quantitative studies (e.g., Hettrich et al., Jbone Joint Surg Am, 2010) demonstrated that the posterior circumflex humeral artery supplies approximately 64% of the blood to the humeral head, challenging older concepts and changing our understanding of avascular necrosis risk in proximal humerus fractures.
Question 61:
A 12-year-old obese male presents with a left-sided Slipped Capital Femoral Epiphysis (SCFE). In which of the following scenarios is prophylactic in situ pinning of the contralateral asymptomatic right hip most strongly indicated?
Options:
- Male gender without other comorbidities
- Age greater than 14 years at initial presentation
- Initial presentation with a chronic slip
- Presence of an endocrine disorder such as hypothyroidism
- Slip angle less than 30 degrees on the affected side
Correct Answer: Presence of an endocrine disorder such as hypothyroidism
Explanation:
Prophylactic pinning of the contralateral hip in SCFE is strongly considered in patients with metabolic or endocrine disorders (e.g., hypothyroidism, renal osteodystrophy, growth hormone deficiency), as these conditions present a high risk for bilateral involvement. It is also considered in patients presenting at a younger age (males <12, females <10) or those with prior radiation therapy.
Question 62:
A 60-year-old male undergoes a total hip arthroplasty using a ceramic-on-ceramic bearing. Two years postoperatively, he complains of an audible squeaking sound from the hip during walking, but denies pain. Which of the following factors is most strongly mechanically associated with squeaking in ceramic-on-ceramic THA?
Options:
- Acetabular component retroversion
- Use of a smaller diameter femoral head
- Impingement and edge loading
- Increased femoral stem offset
- Use of a highly cross-linked polyethylene liner
Correct Answer: Impingement and edge loading
Explanation:
Squeaking in ceramic-on-ceramic total hip arthroplasty is multifactorial but is highly associated with edge loading due to component malposition, specifically acetabular cup malposition (steep cup inclination, excessive anteversion, or retroversion). This leads to impingement, micro-separation, and stripe wear, generating the characteristic squeaking sound.
Question 63:
A 45-year-old man presents with severe right anterior thigh pain and weakness. MRI reveals a far lateral (extraforaminal) disc herniation at the L3-L4 level on the right side. Which nerve root is most likely compressed, and what is the typical motor deficit?
Options:
- L3 nerve root; weakness in hip flexion and knee extension
- L4 nerve root; weakness in ankle dorsiflexion
- L3 nerve root; weakness in great toe extension
- L4 nerve root; weakness in knee extension and loss of patellar reflex
- L5 nerve root; weakness in hip abduction
Correct Answer: L3 nerve root; weakness in hip flexion and knee extension
Explanation:
In the lumbar spine, a far lateral (extraforaminal) disc herniation compresses the exiting nerve root at that same level. Therefore, an L3-L4 far lateral disc compresses the L3 nerve root. The L3 nerve root innervates the iliopsoas and quadriceps, presenting with anterior thigh pain and weakness in hip flexion and knee extension. A paracentral herniation at L3-L4 would compress the traversing L4 nerve root.
Question 64:
In an anteroposterior compression type II (APC II) pelvic ring injury, which of the following ligamentous structures is primarily disrupted to allow widening of the pubic symphysis greater than 2.5 cm, while vertical stability is maintained?
Options:
- Posterior sacroiliac ligament
- Sacrotuberous and sacrospinous ligaments
- Anterior sacroiliac, sacrotuberous, and sacrospinous ligaments
- Iliolumbar ligament
- Sacrospinous ligament only
Correct Answer: Anterior sacroiliac, sacrotuberous, and sacrospinous ligaments
Explanation:
An APC II pelvic ring injury is characterized by symphyseal diastasis > 2.5 cm and widening of the anterior SI joint. The anterior sacroiliac, sacrotuberous, and sacrospinous ligaments are torn, causing rotational instability. The strong posterior sacroiliac ligaments remain intact, which prevents vertical displacement and maintains vertical stability.
Question 65:
Which of the following flexor tendon pulleys is the most critical to preserve during hand surgery to prevent bowstringing of the flexor tendons in the digits?
Options:
- A1 and A3 pulleys
- A2 and A4 pulleys
- C1 and C2 pulleys
- A3 and A5 pulleys
- A1 and A5 pulleys
Correct Answer: A2 and A4 pulleys
Explanation:
The A2 and A4 pulleys are the most biomechanically critical annular pulleys in the digits. They insert directly onto the periosteum of the proximal and middle phalanges, respectively. Loss of both of these pulleys will invariably lead to bowstringing, decreased tendon excursion, and a significant loss of active flexion at the interphalangeal joints.
Question 66:
A 25-year-old athlete sustains a purely ligamentous Lisfranc injury. Current evidence comparing primary arthrodesis versus open reduction and internal fixation (ORIF) for purely ligamentous Lisfranc injuries suggests which of the following regarding primary arthrodesis?
Options:
- It results in a lower rate of return to competitive sports.
- It provides inferior midfoot functional scores at 2 years.
- It is associated with a lower rate of hardware removal and subsequent surgical procedures.
- It has a higher rate of nonunion than bony Lisfranc injuries.
- It requires a longer period of non-weight-bearing postoperatively compared to ORIF.
Correct Answer: It is associated with a lower rate of hardware removal and subsequent surgical procedures.
Explanation:
Multiple prospective studies (e.g., Ly and Coetzee) have demonstrated that primary arthrodesis for purely ligamentous Lisfranc injuries provides comparable or superior functional outcomes and significantly lower rates of subsequent surgeries, such as hardware removal or conversion to salvage arthrodesis, compared to ORIF. ORIF in purely ligamentous injuries often leads to progressive arch collapse and post-traumatic arthritis.
Question 67:
Following neoadjuvant chemotherapy for conventional high-grade osteosarcoma, surgical resection is performed. According to the Huvos grading system, what percentage of tumor necrosis is considered a 'good response' and is the most significant prognostic factor for long-term survival?
Options:
- Greater than 50%
- Greater than 75%
- Greater than 90%
- Greater than 95%
- 100% only
Correct Answer: Greater than 90%
Explanation:
The percentage of tumor necrosis following neoadjuvant chemotherapy is the most important prognostic factor for conventional osteosarcoma. A 'good response' is defined as at least 90% tumor necrosis (Huvos Grade III is 90-99% and Grade IV is 100% necrosis). Patients with >=90% necrosis have a significantly better 5-year survival rate compared to poor responders (<90% necrosis).
Question 68:
When performing an anterior cruciate ligament (ACL) reconstruction, drilling the femoral tunnel via an anteromedial (AM) portal instead of a transtibial technique is advantageous primarily because it allows for:
Options:
- A more vertical femoral tunnel, reducing rotational instability
- Independent placement of the femoral tunnel closer to the native ACL footprint
- Decreased risk of posterior wall blowout
- Longer femoral tunnel length for better graft incorporation
- Avoidance of the need to hyperflex the knee during drilling
Correct Answer: Independent placement of the femoral tunnel closer to the native ACL footprint
Explanation:
The primary advantage of the anteromedial (AM) portal technique over the traditional transtibial technique is that it uncouples the femoral tunnel from the tibial tunnel trajectory. This allows for independent, anatomic placement of the femoral tunnel at the native ACL footprint, which creates a more oblique graft that better restores rotational stability.
Question 69:
During the natural progression of tendon healing, the remodeling phase is characterized by the replacement of immature collagen with mature collagen. Which type of collagen transitions to which type during this phase?
Options:
- Type I transitions to Type II
- Type II transitions to Type I
- Type III transitions to Type I
- Type I transitions to Type III
- Type III transitions to Type IV
Correct Answer: Type III transitions to Type I
Explanation:
Tendon healing occurs in three phases: inflammatory, proliferative, and remodeling. During the proliferative phase, fibroblasts synthesize a large amount of Type III collagen, which is disorganized and weaker. During the remodeling phase, this is gradually replaced by Type I collagen, which is organized linearly along the axis of tension, providing greater tensile strength to the healed tendon.
Question 70:
In a pediatric patient with a lateral condyle fracture of the humerus, the Milch classification differentiates between two types based on the fracture anatomy. Where does the fracture line exit the articular surface in a Milch Type II fracture?
Options:
- Capitellotrochlear groove
- Lateral to the capitellum
- Medial to the trochlea apex
- Through the trochlear groove
- Radiocapitellar joint
Correct Answer: Through the trochlear groove
Explanation:
According to the Milch classification for lateral condyle fractures, a Milch Type I fracture line exits laterally through the capitellotrochlear groove (Salter-Harris IV equivalent), leaving the lateral trochlear ridge intact to stabilize the elbow. Milch Type II fractures exit medially through the trochlear groove (Salter-Harris II equivalent), violating the lateral trochlear ridge and resulting in a structurally unstable joint.
Question 71:
In a patient with a displaced proximal humerus fracture, which of the following Hertel criteria is the most reliable predictor for the development of avascular necrosis (AVN) of the humeral head?
Options:
- A posteromedial metaphyseal hinge measuring > 8 mm
- Displacement of the greater tuberosity by > 5 mm
- An intact medial calcar hinge
- A posteromedial metaphyseal head extension < 8 mm
- Varus angulation of the humeral head > 20 degrees
Correct Answer: A posteromedial metaphyseal head extension < 8 mm
Explanation:
Hertel described predictors for ischemia of the humeral head in proximal humerus fractures. The strongest predictors include a posteromedial metaphyseal extension (calcar length) of less than 8 mm, disruption of the medial hinge (>2mm displacement), and an anatomic neck fracture pattern. An intact medial hinge or calcar length > 8 mm is protective against AVN.
Question 72:
Which of the following best describes the intended biomechanical advantage of femoral roll-back in a posterior stabilized (PS) total knee arthroplasty?
Options:
- It increases the patellofemoral contact forces.
- It anteriorly displaces the axis of rotation to improve extension.
- It improves maximum knee flexion by clearing the posterior femur from the posterior tibia.
- It allows the collateral ligaments to loosen in deep flexion.
- It prevents anterior tibial translation during early flexion.
Correct Answer: It improves maximum knee flexion by clearing the posterior femur from the posterior tibia.
Explanation:
Femoral roll-back refers to the posterior translation of the femoral condyles on the tibial plateau during knee flexion. In a posterior stabilized (PS) TKA, the cam-post mechanism enforces this roll-back. The primary biomechanical advantage is that it shifts the contact point posteriorly, delaying impingement of the posterior femoral shaft on the posterior tibia, thereby increasing the maximum achievable knee flexion arc.
Question 73:
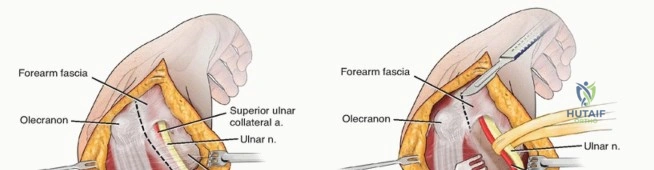
During an in situ ulnar nerve decompression at the elbow, the surgeon must divide several structures to fully release the cubital tunnel. Which of the following structures forms the roof of the cubital tunnel?
Options:
- The medial intermuscular septum
- Osborne's ligament
- The Arcade of Struthers
- The deep flexor pronator aponeurosis
- The medial collateral ligament of the elbow
Correct Answer: Osborne's ligament
Explanation:
The cubital tunnel is bounded by the medial epicondyle anteriorly, the olecranon laterally, and the elbow joint capsule and medial collateral ligament (MCL) as the floor. The roof is formed by Osborne's ligament (the cubital tunnel retinaculum), which spans from the medial epicondyle to the olecranon and blends with the fascia of the two heads of the flexor carpi ulnaris (FCU).
Question 74:
Superior capsular reconstruction (SCR) is a surgical option for massive, irreparable rotator cuff tears. The primary biomechanical goal of the graft in SCR is to:
Options:
- Reconstruct the anterior restraint to prevent anterior subluxation
- Restore active abduction through a dynamic tenodesis effect
- Depress the humeral head and prevent superior migration during shoulder elevation
- Act as a spacer to widen the subacromial space without attaching to the humerus
- Replace the subscapularis footprint to balance transverse force couples
Correct Answer: Depress the humeral head and prevent superior migration during shoulder elevation
Explanation:
In massive, irreparable posterosuperior rotator cuff tears, the loss of the supraspinatus and infraspinatus leads to superior migration of the humeral head due to unopposed deltoid pull. Superior capsular reconstruction (SCR) utilizes a graft (typically fascia lata or human dermal allograft) attached medially to the superior glenoid and laterally to the greater tuberosity. Its primary biomechanical role is to function as a static restraint to prevent superior migration of the humeral head, restoring the glenohumeral fulcrum to improve deltoid efficiency.
Question 75:
A 55-year-old male with poorly controlled diabetes presents with a swollen, erythematous, and warm left foot. Radiographs reveal periarticular debris, fragmentation, and subluxation of the tarsometatarsal joints. According to the Eichenholtz classification, what is the appropriate stage and recommended initial treatment?
Options:
- Stage 0; immediate primary arthrodesis
- Stage 1; total contact casting and non-weight bearing
- Stage 2; custom orthotics and weight-bearing as tolerated
- Stage 3; open reduction and internal fixation
- Stage 1; intravenous antibiotics and surgical debridement
Correct Answer: Stage 1; total contact casting and non-weight bearing
Explanation:
The patient's clinical presentation and radiographic findings (debris, fragmentation, subluxation) are pathognomonic for Eichenholtz Stage 1 (developmental/fragmentation stage) of Charcot neuroarthropathy. The gold standard initial treatment during this active inflammatory stage is rigid immobilization and offloading, typically achieved with a total contact cast (TCC) and non-weight bearing, to prevent further deformity. Reconstructive surgery is contraindicated in the acute phase.
Question 76:
A 70-year-old male sustains a Type II odontoid fracture after a ground-level fall. Which of the following radiographic findings is most strongly associated with a high risk of non-union if treated conservatively with a rigid cervical collar?
Options:
- Anterior displacement of 3 mm
- Fracture line extending into the vertebral body
- Posterior displacement of 6 mm
- An impacted fracture with 2 degrees of angulation
- Presence of an isolated, non-displaced C1 arch fracture
Correct Answer: Posterior displacement of 6 mm
Explanation:
Type II odontoid fractures (fractures at the base of the dens) have a high rate of non-union due to tenuous blood supply. Risk factors for non-union include: age > 50 years, initial displacement > 5 mm (anterior or posterior), angulation > 10 degrees, and posterior displacement direction. Therefore, posterior displacement of 6 mm is a major risk factor for non-union, often warranting surgical stabilization.
Question 77:
A trauma surgeon is selecting an intramedullary nail for a tibial fracture. Comparing titanium alloy (Ti-6Al-4V) to 316L stainless steel, titanium alloy exhibits:
Options:
- A higher modulus of elasticity, resulting in less stress shielding
- A lower modulus of elasticity, resulting in less stress shielding
- A higher modulus of elasticity, resulting in greater stress shielding
- A lower modulus of elasticity, resulting in greater stress shielding
- An identical modulus of elasticity but superior fatigue resistance
Correct Answer: A lower modulus of elasticity, resulting in less stress shielding
Explanation:
Titanium alloy (Ti-6Al-4V) has a lower modulus of elasticity (closer to that of cortical bone) compared to stainless steel or cobalt-chrome alloys. Because it is less stiff, it shares load better with the surrounding bone, thereby reducing stress shielding and theoretically promoting better fracture healing and minimizing bone resorption compared to the stiffer stainless steel implants.
Question 78:
When treating congenital idiopathic clubfoot (talipes equinovarus) using the Ponseti method, what is the correct sequence of deformity correction during serial casting?
Options:
- Equinus, Varus, Adductus, Cavus
- Cavus, Adductus, Varus, Equinus
- Varus, Cavus, Equinus, Adductus
- Adductus, Cavus, Equinus, Varus
- Equinus, Adductus, Varus, Cavus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method involves sequential correction of the clubfoot deformities using the mnemonic CAVE: Cavus (corrected first by elevating the first ray), Adductus, Varus, and finally Equinus. The equinus deformity is corrected last, often requiring a percutaneous Achilles tenotomy if dorsiflexion remains limited after the other deformities have been corrected.
Question 79:
A 62-year-old female with breast cancer presents with right thigh pain. Radiographs reveal a lytic metastatic lesion in the peritrochanteric region of the right femur, involving greater than 2/3 of the cortical diameter. She describes moderate pain with weight-bearing. Using Mirels' criteria, what is her score and the recommended management regarding prophylactic fixation?
Options:
- Score 8; radiotherapy alone is indicated
- Score 9; prophylactic internal fixation is highly recommended
- Score 10; prophylactic internal fixation is highly recommended
- Score 11; prophylactic internal fixation is highly recommended
- Score 7; conservative management with bisphosphonates
Correct Answer: Score 11; prophylactic internal fixation is highly recommended
Explanation:
Mirels' criteria assess the risk of impending pathologic fracture based on four categories, each scoring 1 to 3 points: Site (Upper extremity=1, Lower extremity=2, Peritrochanteric=3), Pain (Mild=1, Moderate=2, Functional=3), Lesion Nature (Blastic=1, Mixed=2, Lytic=3), and Size (<1/3 cortex=1, 1/3-2/3 cortex=2, >2/3 cortex=3). Calculation: Peritrochanteric (3) + Moderate pain (2) + Lytic (3) + Size >2/3 (3) = 11. A Mirels' score of >= 9 indicates a high risk of fracture, and prophylactic internal fixation is highly recommended.
Question 80:
A patient sustains a complex bicondylar tibial plateau fracture with a large posteromedial fragment. To adequately reduce and buttress this specific fragment, which surgical approach is most appropriate?
Options:
- Standard anterolateral approach with submeniscal arthrotomy
- Medial approach with elevation of the pes anserinus
- Posteromedial approach utilizing the interval between the medial head of the gastrocnemius and the pes anserinus
- Direct posterior approach through the popliteal fossa
- Anteromedial approach through the medial patellar retinaculum
Correct Answer: Posteromedial approach utilizing the interval between the medial head of the gastrocnemius and the pes anserinus
Explanation:
A posteromedial shear fragment in a tibial plateau fracture (frequently seen in Schatzker IV or VI patterns) cannot be adequately reduced or plated through a standard anteromedial or anterolateral approach. A posteromedial approach is required, which utilizes the internervous/intermuscular interval between the medial head of the gastrocnemius (posteriorly) and the pes anserinus (anteriorly). This allows direct visualization of the posteromedial cortex for optimal anti-glide plating.
Question 81:
A 45-year-old male presents with right arm pain and weakness. Physical examination reveals weakness in right elbow extension and wrist flexion. He has diminished pinprick sensation over the dorsal aspect of the middle finger. Which cervical nerve root is most likely compressed?
Options:
Correct Answer: C7
Explanation:
The C7 nerve root provides motor innervation for elbow extension (triceps) and wrist flexion (flexor carpi radialis). The dermatomal sensory distribution of C7 includes the middle finger. C5 supplies shoulder abduction and elbow flexion; C6 supplies wrist extension and sensation to the thumb and index finger; C8 supplies finger flexors and sensation to the ulnar side of the hand.
Question 82:
A 60-year-old male presents with a destructive radiolucent lesion in his proximal femur. Histological examination reveals two distinct morphological components: a well-differentiated hyaline cartilage tumor sharply juxtaposed against a high-grade, non-cartilaginous spindle cell sarcoma. What is the most likely diagnosis?
Options:
- Osteosarcoma
- Clear cell chondrosarcoma
- Dedifferentiated chondrosarcoma
- Mesenchymal chondrosarcoma
- Ewing sarcoma
Correct Answer: Dedifferentiated chondrosarcoma
Explanation:
Dedifferentiated chondrosarcoma is characterized by a bimorphic histological appearance featuring a low-grade cartilage tumor abruptly adjacent to a high-grade, non-cartilaginous sarcoma (often resembling osteosarcoma, fibrosarcoma, or undifferentiated pleomorphic sarcoma). This typically occurs in older adults and carries a poor prognosis.
Question 83:
A 28-year-old male sustains a high-energy multiligamentous knee injury with complete ruptures of the ACL, PCL, and MCL (Schenck KD-III M). Upon closed reduction in the emergency department, his pedal pulses are palpable, but his ankle-brachial index (ABI) is 0.85. What is the most appropriate next step in management?
Options:
- Observation and repeat the ABI in 4 hours
- Perform a CT angiogram of the lower extremity
- Immediate surgical exploration of the popliteal artery
- Apply a hinged knee brace and perform duplex ultrasound
- Initiate intravenous heparin infusion
Correct Answer: Perform a CT angiogram of the lower extremity
Explanation:
An ABI < 0.9 in the setting of a multiligament knee injury (knee dislocation) is highly suspicious for a popliteal artery injury, even if pedal pulses are palpable. A CT angiogram is the gold standard next step to evaluate the arterial tree before proceeding with possible vascular repair.
Question 84:
During surgical repair of a Zone II flexor tendon injury, maintaining the integrity of the A2 and A4 pulleys is crucial to prevent bowstringing. If the A2 pulley is inadvertently excised, what is the most significant biomechanical consequence regarding the function of the flexor tendon?
Options:
- Decreased moment arm
- Decreased required tendon excursion to achieve full digit flexion
- Increased required tendon excursion to achieve full digit flexion
- Increased active grip strength
- Decreased passive resistance to extension
Correct Answer: Increased required tendon excursion to achieve full digit flexion
Explanation:
The flexor pulleys keep the tendon closely applied to the bone. If the A2 or A4 pulley is excised, the tendon bowstrings away from the center of rotation of the joint. This increases the moment arm. Biomechanically, an increased moment arm means that a greater length of tendon excursion is required to achieve the same angular range of motion. Because the muscle's excursion is finite, this often results in incomplete active finger flexion.
Question 85:
A 65-year-old male with a metal-on-polyethylene total hip arthroplasty (titanium stem, large-diameter cobalt-chromium head) performed 6 years ago presents with groin pain and a large hip effusion. Aspiration is negative for infection but reveals dark, blackish debris. Serum cobalt levels are significantly elevated, while serum chromium levels are normal. What is the most likely diagnosis?
Options:
- Aseptic loosening of the acetabular component
- Mechanically assisted crevice corrosion at the head-neck junction
- Polyethylene wear-induced osteolysis
- Galvanic corrosion at the stem-cement interface
- Undiagnosed low-virulence periprosthetic joint infection
Correct Answer: Mechanically assisted crevice corrosion at the head-neck junction
Explanation:
The clinical presentation of a symptomatic effusion, black tissue debris, and a high cobalt/normal chromium ratio in a metal-on-polyethylene THA is classic for trunnionosis—specifically mechanically assisted crevice corrosion (MACC) at the modular head-neck junction (the trunnion). It is more common with large femoral heads on titanium stems.
Question 86:
An 8-year-old boy, who is in the 10th percentile for height and 90th percentile for weight, presents with an idiopathic unilateral slipped capital femoral epiphysis (SCFE). Given his young age, an underlying endocrinopathy is highly suspected. Which of the following laboratory profiles is most classically associated with the most common endocrine cause of SCFE in this age group?
Options:
- Elevated free T4 and low TSH
- Decreased free T4 and elevated TSH
- Elevated growth hormone and IGF-1
- Elevated serum calcium and decreased PTH
- Decreased testosterone and elevated FSH
Correct Answer: Decreased free T4 and elevated TSH
Explanation:
SCFE in children under the age of 10 or those with atypical presentations should prompt an evaluation for an underlying endocrine disorder. Hypothyroidism is the most common endocrinopathy associated with SCFE, characterized by a low free T4 and an elevated TSH.
Question 87:
The torsional rigidity of a solid cylindrical intramedullary nail is mathematically governed by its polar moment of inertia. Based on this formula, the torsional rigidity is proportional to which of the following regarding the radius of the nail?
Options:
- Radius
- Radius squared
- Radius to the third power
- Radius to the fourth power
- Inversely proportional to the radius
Correct Answer: Radius to the fourth power
Explanation:
The torsional rigidity of a solid cylinder is proportional to its polar moment of inertia (J), which is calculated as J = (pi * r^4) / 2. Therefore, the torsional rigidity is directly proportional to the radius to the fourth power (r^4).
Question 88:
A 55-year-old poorly controlled diabetic patient presents with a swollen, warm, and erythematous right foot. There is no open ulceration. Radiographs reveal focal osteopenia, joint subluxation, debris, and fragmentation around the tarsometatarsal joints. Which of the following corresponds to the correct Eichenholtz stage and the standard of care initial management?
Options:
- Stage 0; rigid internal fixation
- Stage I; total contact casting
- Stage II; total contact casting
- Stage III; custom orthotic footwear
- Stage I; immediate midfoot arthrodesis
Correct Answer: Stage I; total contact casting
Explanation:
The clinical and radiographic presentation describes Eichenholtz Stage I (Development/Fragmentation stage) of Charcot arthropathy, characterized by swelling, warmth, joint debris, subluxation, and fragmentation. The gold standard initial management is immobilization and offloading with a total contact cast (TCC).
Question 89:
In a patient presenting with hemorrhagic shock secondary to a severe anterior-posterior compression (APC-III) pelvic ring injury, what is the most common anatomical source of the massive retroperitoneal hemorrhage?
Options:
- Superior gluteal artery
- Internal pudendal artery
- Obturator artery
- Presacral venous plexus
- External iliac vein
Correct Answer: Presacral venous plexus
Explanation:
While arterial bleeding (such as from the superior gluteal or internal pudendal arteries) can occur and is life-threatening, up to 80-90% of pelvic hemorrhage in the setting of blunt trauma originates from the venous presacral and prevesical plexuses, as well as bleeding from the fractured cancellous bone surfaces.
Question 90:
A 34-year-old female presents with numbness and tingling in the radial three-and-a-half digits of her right hand, along with volar forearm pain. Which of the following clinical findings most specifically distinguishes Pronator Syndrome from Carpal Tunnel Syndrome?
Options:
- Positive Tinel's sign at the wrist crease
- Wasting of the thenar eminence musculature
- Numbness over the palmar aspect of the thenar eminence
- Exacerbation of symptoms that awaken the patient at night
- Weakness of the flexor pollicis brevis
Correct Answer: Numbness over the palmar aspect of the thenar eminence
Explanation:
The palmar cutaneous branch of the median nerve provides sensation to the skin over the thenar eminence. It branches from the median nerve proximal to the carpal tunnel and travels superficial to the transverse carpal ligament. Therefore, sensation over the thenar eminence is spared in Carpal Tunnel Syndrome but is diminished in more proximal compression neuropathies like Pronator Syndrome.
Question 91:
When planning corrective surgery for adult degenerative spinal deformity to optimize patient-reported outcomes and minimize the risk of adjacent segment breakdown, achieving appropriate sagittal balance is paramount. According to current biomechanical targets, the mismatch between Pelvic Incidence (PI) and Lumbar Lordosis (LL) should ideally be corrected to within:
Options:
- 0 degrees
- 10 degrees
- 20 degrees
- 30 degrees
- 40 degrees
Correct Answer: 10 degrees
Explanation:
The widely accepted threshold for an optimal spinopelvic relationship in adult spinal deformity surgery is a Pelvic Incidence minus Lumbar Lordosis (PI - LL) mismatch of less than 10 degrees. This helps restore physiologic sagittal alignment and correlates with better clinical outcomes.
Question 92:
The Ponseti method is the recognized gold standard for the conservative treatment of idiopathic clubfoot. According to this protocol, what is the very first component of the deformity that must be corrected during the initial casting phase?
Options:
- Adductus
- Equinus
- Varus
- Cavus
- Internal tibial torsion
Correct Answer: Cavus
Explanation:
The Ponseti method follows the CAVE mnemonic for the order of correction: Cavus, Adductus, Varus, Equinus. The very first step involves correcting the high arch (cavus) by elevating the first ray to align the forefoot with the hindfoot, which provides a solid lever arm to subsequently correct the adductus and varus.
Question 93:
During a posterior-stabilized total knee arthroplasty, the trial reduction reveals that the knee is well-balanced and symmetric in extension, but it is too tight in flexion, preventing adequate range of motion. Which of the following surgical modifications is the most appropriate next step to balance the knee?
Options:
- Perform a more aggressive distal femoral resection
- Downsize the femoral component utilizing an anterior referencing system
- Upsize the femoral component utilizing a posterior referencing system
- Release the posterior capsule from the femur
- Use a thicker polyethylene insert
Correct Answer: Downsize the femoral component utilizing an anterior referencing system
Explanation:
A knee that is tight in flexion but balanced in extension requires an increase in the flexion gap without altering the extension gap. Downsizing the femoral component using anterior referencing will remove more bone from the posterior condyles, effectively increasing the flexion gap while leaving the distal cut (extension gap) unaffected.
Question 94:
Denosumab is an established targeted therapy used in the management of unresectable or recurrent Giant Cell Tumor of Bone (GCTB). What is its precise mechanism of action?
Options:
- It binds directly to the ruffled border of mature osteoclasts, inhibiting their function.
- It is a monoclonal antibody that binds to RANKL, preventing activation of the RANK receptor.
- It directly induces apoptosis of the neoplastic mononuclear stromal cells.
- It selectively inhibits vascular endothelial growth factor (VEGF) to starve the tumor.
- It is a tyrosine kinase inhibitor that blocks c-KIT signaling.
Correct Answer: It is a monoclonal antibody that binds to RANKL, preventing activation of the RANK receptor.
Explanation:
Denosumab is a fully human monoclonal antibody that binds to Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL). By binding RANKL, it prevents it from activating the RANK receptor on the surface of osteoclast precursors, thereby inhibiting the formation, function, and survival of the giant osteoclast-like cells characteristic of GCTB.
Question 95:
A 42-year-old recreational overhead athlete presents with persistent anterior shoulder pain and deep clicking. An MRI arthrogram demonstrates an isolated Type II SLAP tear. After 6 months of dedicated physical therapy, symptoms remain debilitating. Which of the following surgical interventions is most strongly supported by current literature for a patient of this age?
Options:
- Arthroscopic debridement of the superior labrum only
- Anatomic SLAP repair utilizing suture anchors
- Biceps tenodesis
- Biceps tenotomy without tenodesis
- Coracoid process transfer (Latarjet procedure)
Correct Answer: Biceps tenodesis
Explanation:
In older patients (typically > 35-40 years old), SLAP repairs have a higher rate of stiffness, continued pain, and clinical failure compared to younger patients. Current evidence strongly favors primary biceps tenodesis over SLAP repair for Type II SLAP lesions in patients over 40.
Question 96:
A 50-year-old female presents with a sudden inability to actively flex the interphalangeal joint of her thumb. Three years prior, she underwent volar plate fixation of a distal radius fracture. The spontaneous rupture of the flexor pollicis longus (FPL) tendon in this setting is most commonly associated with which of the following intraoperative technical errors?
Options:
- Excessive dorsal screw prominence
- Volar plate placement distal to the watershed line
- Intra-articular screw penetration into the radiocarpal joint
- Inadequate restoration of radial inclination
- Failure to address ulnar positive variance
Correct Answer: Volar plate placement distal to the watershed line
Explanation:
FPL attrition and spontaneous rupture is a well-recognized complication of volar locking plating for distal radius fractures. It most commonly occurs when the plate is placed too distally, crossing the "watershed line" of the distal radius, creating a mechanical prominence that directly abrades the FPL tendon (Soong Grade 2).
Question 97:
According to Perren's strain theory regarding fracture healing, what mechanical strain condition within a fracture gap is required to achieve primary (direct) bone healing via Haversian remodeling, bypassing cartilaginous callus formation?
Options:
- Strain less than 2%
- Strain between 2% and 10%
- Strain between 10% and 30%
- Strain greater than 30%
- Constant dynamic strain fluctuations
Correct Answer: Strain less than 2%
Explanation:
Perren's strain theory posits that primary (direct) bone healing requires absolute stability, defined as a strain environment of < 2%. This environment prevents the disruption of crossing osteons and avoids callus formation. Strain between 2% and 10% allows for secondary healing (callus formation), while strain > 10% leads to nonunion or fibrous tissue formation.
Question 98:
An 8-week-old infant with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a routine follow-up, the parents note that the child is no longer actively kicking the leg on the affected side. Upon physical examination, there is an absent patellar reflex and decreased active knee extension. Which of the following errors in harness application is the most likely cause of this complication?
Options:
- Excessive flexion of the hip
- Excessive abduction of the hip
- Excessive adduction of the hip
- Placement of the chest strap too high
- Inadequate tension on the posterior straps
Correct Answer: Excessive flexion of the hip
Explanation:
Femoral nerve palsy is a known complication of Pavlik harness treatment, typically resulting from hyperflexion of the hips, which compresses the femoral nerve against the inguinal ligament. Excessive abduction is associated with avascular necrosis (AVN) of the femoral head.
Question 99:
A 52-year-old female presents with medial ankle pain and a progressively flattening arch. Examination shows a flexible pes planovalgus, inability to perform a single-limb heel rise, and a positive "too many toes" sign. Radiographs show significant talonavicular uncoverage (>40%). Which of the following is the most appropriate surgical reconstruction for this specific stage of adult-acquired flatfoot deformity (Stage IIB)?
Options:
- Isolated flexor digitorum longus (FDL) transfer to the navicular
- FDL transfer, medial displacement calcaneal osteotomy, and lateral column lengthening
- Isolated subtalar arthrodesis
- Triple arthrodesis
- Gastrocnemius recession alone
Correct Answer: FDL transfer, medial displacement calcaneal osteotomy, and lateral column lengthening
Explanation:
The patient has Stage IIB Posterior Tibial Tendon Dysfunction (flexible flatfoot with severe forefoot abduction, indicated by >40% talonavicular uncoverage). Stage IIB requires an FDL transfer to reconstruct the posterior tibial tendon, a medial displacement calcaneal osteotomy to correct the hindfoot valgus, and a lateral column lengthening (e.g., Evans osteotomy) to adequately correct the severe forefoot abduction.
Question 100:
A 68-year-old male presents with bilateral lower extremity pain and cramping associated with walking. To differentiate between neurogenic claudication (due to lumbar spinal stenosis) and vascular claudication (due to peripheral arterial disease), which of the following historical features is most specific for neurogenic claudication?
Options:
- Relief of symptoms when stopping and standing completely upright
- Pain exacerbation that occurs promptly when riding a stationary bicycle
- Relief of symptoms when continuing to walk while leaning forward over a shopping cart
- Diminished posterior tibial and dorsalis pedis pulses
- Symptoms consistently begin distally in the calves and radiate proximally
Correct Answer: Relief of symptoms when continuing to walk while leaning forward over a shopping cart
Explanation:
The "shopping cart sign"—relief of claudication symptoms while walking in a flexed posture—is highly specific for neurogenic claudication. Flexion increases the cross-sectional area of the spinal canal, relieving nerve root compression. Vascular claudication is worsened by any leg exercise (including stationary bicycling) due to metabolic demand and is relieved simply by standing rest, unaffected by posture.