Modular Proximal Femoral Replacement: Reconstructing an Above-Knee Stump After Hip Disarticulation
Key Takeaway
Join us in the OR for a masterclass on creating a functional above-knee stump after hip disarticulation using a custom modular prosthesis. This advanced technique significantly improves patient mobility and quality of life compared to traditional disarticulation. We'll meticulously cover preoperative planning, precise surgical steps, critical anatomical considerations, and post-operative management, emphasizing technique and rationale for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of aggressive osseous and soft tissue malignancies of the femur frequently presents a complex reconstructive dilemma. When limb-sparing wide resection is oncologically contraindicated due to the proximal extent of the tumor, skip metastases, or massive soft tissue contamination, surgeons have historically been forced to default to a standard hip disarticulation. While oncologically sound, a traditional hip disarticulation results in a profound functional deficit. Patients are left without a residual femoral lever arm, rendering the suspension and mobilization of a standard lower extremity prosthesis biomechanically inefficient and metabolically exhausting.
Historically, functional outcomes following a standard hip disarticulation have been dismal. The absence of a femoral fulcrum necessitates that the patient initiates the swing phase of gait through exaggerated pelvic tilt and truncal momentum. Biomechanical studies have consistently demonstrated that the energy expenditure required to ambulate with a hip disarticulation prosthesis can be up to 82% greater than that of a non-amputee, and significantly higher than that of a standard transfemoral (above-knee) amputee. This extreme metabolic demand frequently relegates patients—particularly those who are older or deconditioned from adjuvant chemotherapy—to permanent wheelchair reliance, precipitating a cascade of adverse psychological and physiological sequelae, including profound losses in self-esteem, independence, and cardiovascular conditioning.
Building upon the pioneering conceptual work of Marcove and subsequent advancements in orthopaedic oncology, the technique of modular proximal femoral replacement to reconstruct an above-knee stump was developed as a functional salvage operation. The overarching objective is to convert an anatomical hip disarticulation into a functional transfemoral amputation. By preserving an uncontaminated soft tissue envelope and utilizing a custom modular endoprosthesis to replace the resected femur, the surgeon creates a durable, dynamic lever arm. This prosthetic stump articulates with the native acetabulum, dramatically lowering the energy consumption required for ambulation and exponentially increasing the likelihood of successful prosthetic fitting and independent community ambulation.
This procedure represents a pinnacle of reconstructive orthopaedic oncology. It requires meticulous preoperative planning, an advanced understanding of cross-sectional anatomy, and precise execution of soft tissue balancing. While relatively rare, the creation of a functional stump using a modular endoprosthesis is a testament to the evolution of surgical techniques, offering a vastly superior quality of life alternative when traditional limb salvage is precluded by aggressive tumor biology.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the cross-sectional and longitudinal anatomy of the thigh and pelvic girdle is an absolute prerequisite for this procedure. The operation hinges not merely on the extirpation of the tumor, but on the strategic preservation of neurovascular bundles and myocutaneous flaps that will ultimately envelop the endoprosthesis. The vascular anatomy dictates flap viability; the primary blood supply to the anterior and posterior thigh flaps must be meticulously traced and preserved. The superficial femoral artery and the profunda femoris artery must be evaluated preoperatively. Often, the profunda femoris must be ligated if the tumor involves the proximal diaphysis, leaving the superficial femoral artery (ligated as distally as oncologically safe) to provide retrograde collateral flow, or relying on the descending branch of the lateral femoral circumflex artery to supply the vastus lateralis and overlying integument.
Biomechanically, the reconstructed stump must function as a dynamic, suspended pendulum that can interface with a prosthetic socket without pistoning or dislocating. The native hip joint is stabilized by the bony architecture of the acetabulum, the robust iliofemoral ligaments, and the balanced tension of the pelvifemoral musculature. When the native femur is resected, this equilibrium is obliterated. The modular endoprosthesis, typically featuring a bipolar head, must be secured within the acetabulum primarily through meticulous capsulorrhaphy and dynamic muscle tensioning.
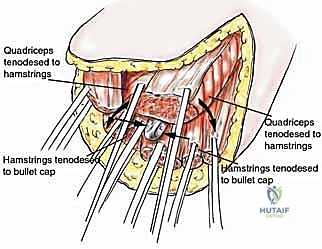
The muscular reconstruction (myodesis) is arguably the most critical biomechanical step. The residual muscles must be reattached to the prosthesis and to each other to provide a functional cushion and to power the stump. The gluteus maximus, medius, and minimus must be anchored to the proximal aspect of the prosthesis or the residual capsule to provide extension and abduction power, preventing the stump from resting in fixed adduction. The distal musculature—the transected quadriceps, hamstrings, and adductors—must be sutured securely through the distal holes of the prosthetic bullet tip. If this myodesis fails, the prosthesis will piston within the soft tissue envelope, leading to distal skin necrosis, hardware exposure, and ultimate failure of the reconstruction.
Furthermore, the surgeon must account for the gravitational pull on the prosthesis. Unlike a standard total hip arthroplasty where the implant is supported by the femur and the ground during weight-bearing, the stump prosthesis hangs freely when the patient is upright. This constant inferior distraction force places immense stress on the reconstructed hip capsule. Therefore, preserving as much native capsule as possible and reinforcing it with synthetic mesh or local fascial flaps is imperative to prevent inferior dislocation of the bipolar head.
Exhaustive Indications and Contraindications
The decision to proceed with a modular proximal femoral replacement for stump reconstruction rather than a standard hip disarticulation requires rigorous oncologic and anatomical assessment. The primary indication is the necessity to completely resect the femur to achieve negative oncologic margins, coupled with the presence of adequate, tumor-free soft tissues to cover a prosthesis.
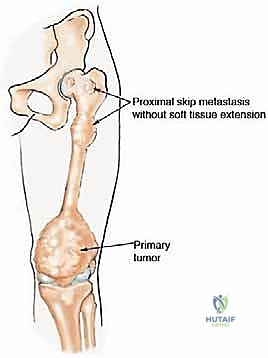


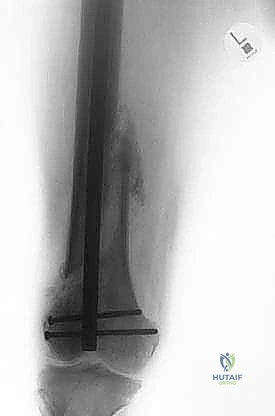
Typical scenarios include osteosarcoma or Ewing sarcoma of the distal or middle third of the femur with proximal transosseous skip metastases. Another frequent indication involves pathologic fractures of the distal femur that have been inadvertently stabilized with intramedullary nailing prior to oncologic diagnosis, thereby contaminating the entire medullary canal up to the greater trochanter. In such cases, the entire bone must be considered contaminated, necessitating total femoral resection.
Contraindications are primarily dictated by the local extent of the tumor. If the malignancy extends into the hip joint, involves the acetabular bone, or massively infiltrates the neurovascular structures of the femoral triangle or the sciatic nerve at the level of the sciatic notch, a functional stump reconstruction is impossible. In these scenarios, a standard hip disarticulation or hemipelvectomy is the only oncologically safe option.
Indications and Contraindications Matrix
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Absolute Indications | Proximal transosseous skip metastases | Standard limb salvage leaves residual tumor; standard HD leaves no functional lever arm. |
| Pathologic fracture with IM nail contamination | Entire femoral canal is seeded with tumor cells; total femoral resection required. | |
| Massive diaphyseal tumor extension | Inability to achieve safe osseous margins with a traditional transfemoral amputation. | |
| Relative Indications | Severe radiation-induced osteonecrosis of the entire femur | Massive bone loss precluding standard arthroplasty, but soft tissues remain viable for coverage. |
| Recurrent periprosthetic joint infection (Total Femur) | Two-stage revision to a stump prosthesis when the patient cannot tolerate a massive reimplantation. | |
| Absolute Contraindications | Acetabular or pelvic bone involvement | Requires hemipelvectomy; no native acetabulum remains to support a bipolar prosthesis. |
| Inadequate tumor-free soft tissue envelope | High risk of wound breakdown, hardware exposure, and catastrophic infection. | |
| Tumor infiltration of the proximal sciatic/femoral nerves | Resection would leave a flail, insensate stump prone to severe neuropathic pain and ulceration. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a modular stump reconstruction is entirely dependent on exhaustive preoperative planning. The surgeon must synthesize data from multiple imaging modalities to map the tumor's exact dimensions and design the custom endoprosthesis.
High-resolution Magnetic Resonance Imaging (MRI) of the entire femur and pelvis is the gold standard for defining the soft tissue extent of the tumor. The MRI must be scrutinized to determine exactly which muscle compartments can be safely retained to form the myocutaneous flaps. A Computed Tomography (CT) scan of the chest, abdomen, and pelvis is required for systemic staging, while a dedicated CT of the pelvis is utilized to confirm the integrity of the acetabulum and to template the size of the bipolar cup. A whole-body technetium-99m bone scan or a Positron Emission Tomography (PET) scan is critical to rule out additional distant osseous metastases that might alter the surgical intent from curative to palliative.

Prosthetic customization is a collaborative effort between the orthopaedic oncologist and the implant manufacturer. The implant typically consists of a proximal bipolar head, a modular diaphyseal segment, and a specialized distal "bullet tip." The length of the modular body is templated to match the length of the planned soft tissue envelope, ensuring that the distal tip sits deep within the muscle bed without placing undue tension on the skin closure. The bullet tip itself is smoothly contoured to prevent pressure necrosis of the distal flap and is heavily fenestrated to allow for the passage of heavy non-absorbable sutures during the myodesis phase. Furthermore, the proximal segment of the prosthesis often features a porous titanium coating or a synthetic mesh sleeve to promote soft tissue ingrowth and enhance the stability of the capsular reconstruction.
Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table. This orientation provides unimpeded access to the anterior abdomen, groin, and the entire circumference of the thigh. A bump may be placed under the ipsilateral hemipelvis to slightly elevate the operative side, facilitating access to the posterior gluteal and hamstring musculature.
The entire lower extremity, from the costal margin down to the toes, is prepped and draped free. This allows for manipulation of the limb during the tumor resection and enables the surgeon to perform trial reductions of the endoprosthesis to assess stability and soft tissue tension across a full range of motion. Intraoperative fluoroscopy (C-arm) must be readily available and draped in the sterile field to confirm the seating of the bipolar head within the acetabulum and to verify the trajectory of any necessary osteotomies. A sterile tourniquet is generally not feasible given the proximal extent of the dissection, necessitating meticulous, proactive hemostasis throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a modular stump reconstruction is a marathon of meticulous dissection, demanding strict adherence to oncologic principles while simultaneously prioritizing reconstructive viability.
1. Incision Design and Flap Elevation

The incision is typically designed as a massive fish-mouth or racquet shape, dictated entirely by the location of the tumor and the necessity for wide margins. Most commonly, a long anterior or posterior myocutaneous flap is utilized. The medial limb of the incision is carried over the adductor compartment, while the lateral limb extends distally from the greater trochanter along the fascia lata.
The skin and subcutaneous tissues are incised down to the deep fascia. Flap elevation must proceed strictly outside the reactive zone of the tumor. The surgeon must identify and ligate multiple perforating vessels during this stage. The viability of the superficial tissues relies heavily on preserving the dermal and subdermal plexuses; therefore, handling the skin edges with atraumatic technique is paramount.
2. Neurovascular Dissection and Management



Attention is then directed to the femoral triangle. The femoral artery and vein are isolated. Depending on the proximal extent of the tumor, the superficial femoral vessels are ligated as distally as oncologically permissible to preserve collateral flow to the flaps. The femoral nerve is identified and transected sharply.
Posteriorly, the sciatic nerve must be managed with extreme care to mitigate the risk of debilitating phantom limb pain and neuroma formation. The nerve is dissected free, placed under gentle traction, and cleanly transected high in the sciatic notch. Contemporary techniques strongly advocate for Targeted Muscle Reinnervation (TMR) or the placement of an epineural catheter infusing local anesthetic, combined with burying the proximal nerve stump deep within the gluteus maximus muscle belly to shield it from mechanical irritation.
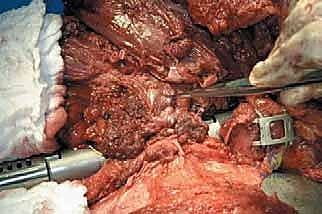
3. Total Femoral Resection
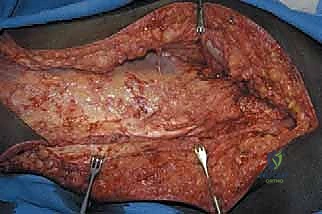
The muscular attachments to the femur are systematically transected at their insertions. The quadriceps, hamstrings, and adductors are divided at a level that ensures negative margins while retaining sufficient length for the subsequent myodesis. The hip joint capsule is exposed. If the tumor does not involve the proximal femur, a standard capsulotomy is performed, and the femoral head is dislocated. If there is concern for proximal contamination, an extracapsular resection is mandated, taking the entire hip capsule en bloc with the specimen. The ligamentum teres is divided, and the entire femur, enveloped in its native musculature containing the tumor, is delivered from the surgical field and sent for pathologic margin assessment.
4. Prosthetic Assembly and Implantation
Once margins are confirmed negative, the field is copiously irrigated. The custom modular endoprosthesis is assembled on the back table according to the preoperative template. A trial reduction is performed. The bipolar head is seated within the native acetabulum. The surgeon must manually assess the length of the prosthetic construct against the residual soft tissue envelope. The distal bullet tip must sit comfortably within the muscle bed; excessive length will cause catastrophic skin tension, while inadequate length compromises the biomechanical lever arm.
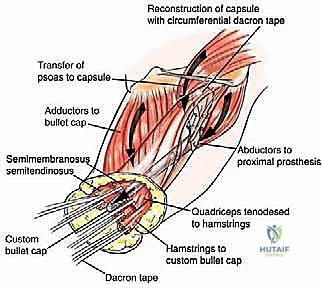
5. Capsulorrhaphy and Myodesis


This is the most critical reconstructive phase. The proximal prosthesis must be secured to prevent inferior subluxation. If native capsule remains, it is tightly imbricated around the prosthetic neck using heavy, non-absorbable (#2 or #5) sutures. If the capsule was resected, an artificial capsule is constructed using synthetic mesh (e.g., Trevira tube) sutured directly to the acetabular rim and the proximal abductor musculature.
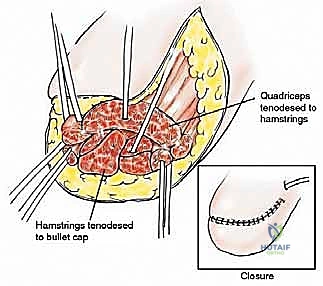
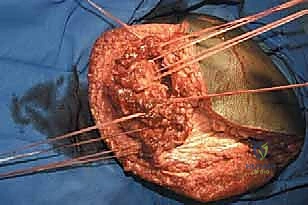
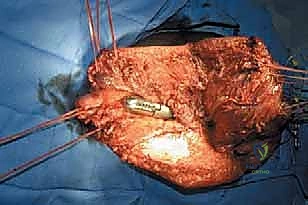
The distal myodesis involves anchoring the retained thigh musculature to the bullet tip of the prosthesis. Heavy non-absorbable sutures are passed through the fenestrations in the bullet tip and woven into the fascial layers of the quadriceps, hamstrings, and adductors using a Krackow or similar locking stitch technique. The muscles are then sutured to one another over the tip of the prosthesis in a multi-layered, "purse-string" fashion. This creates a robust, dynamic soft tissue envelope that grips the prosthesis, preventing pistoning and providing a cushioned distal end for eventual socket weight-bearing. Subfascial closed-suction drains are placed, and the skin is closed meticulously without tension.
Complications, Incidence Rates, and Salvage Management
The creation of a modular proximal femoral stump is an operation of massive magnitude, and the complication profile reflects the radical nature of the resection and reconstruction. The primary challenges arise from the creation of a massive anatomical dead space, the presence of a large foreign body, and the biomechanical stresses placed on the soft tissue envelope.
Infection is the most devastating complication. The extensive soft tissue dissection, combined with the immunocompromised state of many oncology patients undergoing adjuvant chemotherapy, creates an environment ripe for bacterial colonization. Deep periprosthetic joint infection (PJI) in this setting often requires complete removal of the hardware, converting the patient back to a standard, flail hip disarticulation, as the soft tissue envelope is frequently too compromised to support a two-stage revision.
Dislocation of the bipolar head is a unique and frequent complication in stump prostheses. Because the limb lacks distal bony support, the sheer weight of the prosthesis exerts constant inferior traction on the capsular reconstruction when the patient is upright. Failure of the capsulorrhaphy leads to inferior dislocation, which can cause severe pain and render the stump useless for prosthetic fitting.
Complications and Management Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Deep Infection (PJI) | 10% - 25% | Massive dead space, prolonged operative time, chemotherapy-induced neutropenia. | Aggressive I&D, targeted IV antibiotics. Often requires complete explantation and conversion to standard HD. |
| Prosthetic Dislocation | 15% - 30% | Gravitational traction, failure of capsular reconstruction, inadequate abductor tension. | Closed reduction often fails. Requires open revision capsulorrhaphy, use of synthetic mesh, or conversion to a constrained acetabular liner. |
| Distal Flap Necrosis | 10% - 20% | Prosthesis too long (tension), vascular compromise during dissection, failure of distal myodesis (pistoning). | Debridement of necrotic tissue. May require prosthetic shortening or coverage with a pedicled or free myocutaneous flap. |
| Phantom Limb / Neuroma Pain | 30% - 50% | Inadequate sciatic nerve management, mechanical irritation of the nerve stump. | Multimodal pharmacotherapy (Gabapentinoids). Surgical revision for neuroma excision, TMR, or burying the nerve deep in muscle. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a modular stump reconstruction is a protracted, multidisciplinary endeavor requiring close coordination between the orthopaedic surgeon, physiatrist, physical therapist, and prosthetist. The protocol is strictly phased to protect the delicate soft tissue reconstruction while progressively optimizing the biomechanics of the new lever arm.
Phase I: Tissue Healing and Protection (Weeks 0-4)
The immediate postoperative focus is strictly on wound healing, hematoma evacuation (via drains), and pain management. The stump is wrapped in compressive dressings to minimize edema and shape the residual limb. The patient is mobilized out of bed to a chair, but the stump is generally supported to prevent excessive gravitational pull on the capsular reconstruction. Active range of motion of the hip is restricted to allow the myodesis and capsulorrhaphy to scar down and stabilize.
Phase II: Pre-Prosthetic Conditioning (Weeks 4-10)
Once the surgical incisions are fully healed and the drains are removed, the focus shifts to stump conditioning and core strengthening. Aggressive shrinker socks are utilized to mature the stump volume. Physical therapy initiates gentle, progressive active-assisted range of motion, focusing heavily on strengthening the gluteal and core musculature. Preventing flexion and abduction contractures of the stump is critical during this phase, as contractures will severely impede the fitting of a prosthetic socket.
Phase III: Prosthetic Fitting and Gait Training (Weeks 10+)
When the stump volume has stabilized, the prosthetist fabricates a custom socket. Because the stump is essentially an above-knee amputation from a functional standpoint, an ischial containment socket or a sub-ischial vacuum-assisted suspension system is typically employed. The patient begins intensive gait training in parallel bars, learning to utilize the prosthetic lever arm to initiate the swing phase. The ultimate goal is independent community ambulation with minimal assistive devices, capitalizing on the dramatically reduced energy expenditure afforded by the retained femoral fulcrum.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the modular proximal femoral stump reconstruction is well-documented in the orthopaedic oncology literature, transitioning from an experimental salvage technique to a validated, albeit highly specialized, reconstructive option.
The foundational concept was introduced by Marcove and colleagues, who first recognized the profound metabolic and psychological penalties of standard hip disarticulation. Their early attempts utilized custom-cast implants to provide a lever arm. Subsequent retrospective series from major sarcoma centers (such as the Rizzoli Orthopaedic Institute and Memorial Sloan Kettering) validated the biomechanical rationale. These studies consistently demonstrated that patients with a reconstructed stump experienced a statistically significant reduction in oxygen consumption and an increase in self-selected walking velocity compared to matched cohorts with standard hip disarticulations.
Modern clinical guidelines emphasize patient selection as the primary determinant of success. The consensus in the literature dictates that while the functional benefits of a stump prosthesis are undeniable, the procedure should not compromise oncologic margins. Furthermore, recent literature heavily focuses on the techniques of soft tissue reconstruction—specifically the use of synthetic meshes for capsular reinforcement and TMR for neuroma prevention—as the critical variables in reducing the historically high complication rates associated with this massive reconstructive undertaking. Ultimately, in the carefully selected patient, this procedure represents a triumph of limb-salvage philosophy applied to ablative surgery, restoring dignity and mobility in the face of devastating disease.
