Posterior Flap Hemipelvectomy: An Orthopaedic Masterclass in Pelvic Amputation
Key Takeaway
This masterclass guides fellows through posterior flap hemipelvectomy, a complex pelvic amputation. We meticulously cover patient selection, detailed surgical anatomy, preoperative planning, and granular intraoperative execution. Learn to navigate neurovascular structures, perform precise osteotomies, manage potential complications, and optimize postoperative recovery, ensuring comprehensive mastery of this life-saving procedure.
Comprehensive Introduction and Patho-Epidemiology
The posterior flap hemipelvectomy stands as one of the most formidable and anatomically demanding procedures within the armamentarium of orthopaedic oncology and major pelvic trauma surgery. This operation transcends the traditional definition of an amputation; it is a profound, life-altering anatomical extirpation and subsequent reconstruction that demands meticulous preoperative planning, unwavering intraoperative precision, and a comprehensive understanding of three-dimensional pelvic anatomy. While the modern era of orthopaedic oncology has witnessed a paradigm shift toward limb-sparing techniques—facilitated by advanced neoadjuvant chemoradiotherapy and modular endoprosthetics—there remains a critical subset of aggressive, locally advanced tumors of the upper thigh, hip, and pelvis for which a hemipelvectomy is not merely the optimal choice, but the only life-saving surgical intervention available.
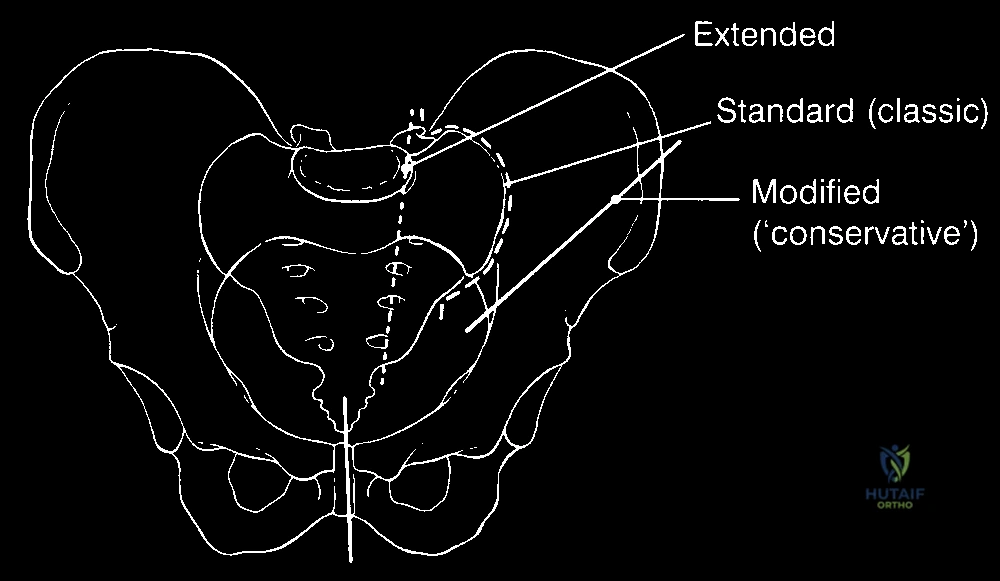
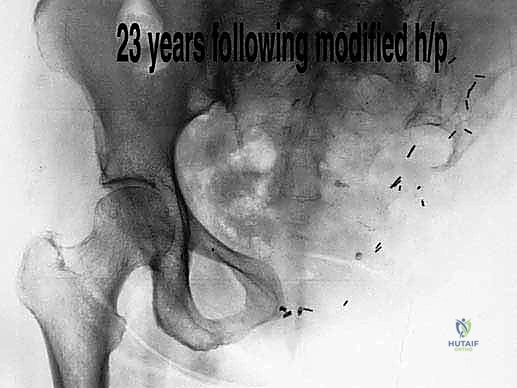
The nomenclature surrounding major pelvic amputations requires precise delineation to avoid catastrophic intraoperative missteps. Historically, terms such as "hindquarter amputation" and "hemipelvectomy" have been utilized interchangeably in the literature. However, modern surgical taxonomy categorizes these procedures based on the specific bony resection and the soft tissue flap utilized for closure. The standard procedure entails creating a robust, vascularized myocutaneous posterior flap, predominantly utilizing the gluteus maximus, to achieve durable wound coverage over the exposed pelvic viscera. The term "hemipelvectomy" itself encapsulates a spectrum of resections: the "classic" disarticulation passes through the sacroiliac joint and pubic symphysis; the "extended" hemipelvectomy involves transection through the sacral ala and neural foramina or the contralateral pubic rami for tumors encroaching upon the midline; and the "modified" hemipelvectomy preserves a portion of the ilium to facilitate seating and prosthetic fitting.
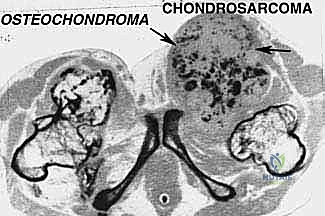
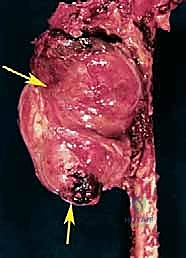
Epidemiologically, the primary indication for a posterior flap hemipelvectomy is a primary bone or soft tissue sarcoma—most frequently chondrosarcoma, osteosarcoma, or Ewing sarcoma—that exhibits extensive involvement of the pelvic ring, neurovascular bundles, or multiple muscular compartments of the proximal thigh. Beyond oncology, this radical procedure may be indicated in the setting of massive, unsalvageable crush injuries to the pelvis, uncontrollable ascending necrotizing fasciitis, or for the palliation of fungating, intractable metastatic lesions that cause severe hemorrhage or sepsis. Regardless of the underlying pathology, the physiological insult of a hemipelvectomy is immense. Surgeons must approach this procedure with a systematic, multidisciplinary strategy to mitigate the profound intraoperative blood loss, the high risk of postoperative wound necrosis, and the significant long-term biomechanical and psychological morbidity associated with the loss of a hindquarter.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Landmarks
Before the scalpel touches the skin, the operating surgeon must possess an intrinsic, three-dimensional visualization of the pelvic labyrinth. The pelvis functions as a rigid, load-bearing ring, transmitting the entire weight of the axial skeleton to the lower extremities. It is composed of the sacrum posteriorly and the two innominate bones (ilium, ischium, and pubis) laterally and anteriorly. The critical articulations that must be navigated or disarticulated during a classic hemipelvectomy are the sacroiliac (SI) joint posteriorly and the pubic symphysis anteriorly. The SI joint is a massive, highly stable amphiarthrodial joint supported by the dense anterior and posterior sacroiliac ligaments, as well as the robust interosseous ligaments, all of which must be systematically divided.
Navigating the bony pelvis relies heavily on identifying and utilizing superficial and deep palpable landmarks. Superficial landmarks—including the iliac crest, the anterior superior iliac spine (ASIS), the posterior superior iliac spine (PSIS), the ischial tuberosity, and the greater trochanter—are indispensable for designing the racquet-shaped skin incision and guiding the initial planes of dissection. Deep to these structures, the anatomy becomes significantly more complex. The true pelvic brim (linea terminalis) separates the false pelvis from the true pelvis and serves as a critical boundary during the retroperitoneal dissection. When performing an extended hemipelvectomy, the surgeon must identify the sacral neural foramina, ensuring that osteotomies through the sacral ala are executed lateral to the central spinal canal while deliberately sacrificing the ipsilateral sacral nerve roots involved in the tumor mass.
Neurovascular Topography
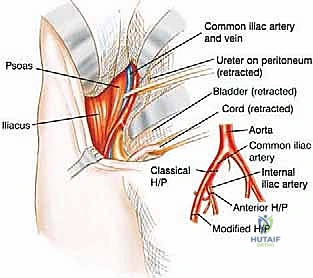
The vascular anatomy of the pelvis dictates the flow of the operation; precise identification and ligation of the major pelvic vessels are arguably the most critical steps in minimizing catastrophic intraoperative hemorrhage. The abdominal aorta typically bifurcates at the level of the L4 vertebral body into the common iliac arteries, while the inferior vena cava forms at the L5 level from the confluence of the common iliac veins. As these vessels descend into the pelvis, the external iliac artery and vein continue anteriorly along the pelvic brim beneath the inguinal ligament to become the femoral vessels. In a standard hemipelvectomy, these external vessels are ligated and divided early in the anterior dissection.
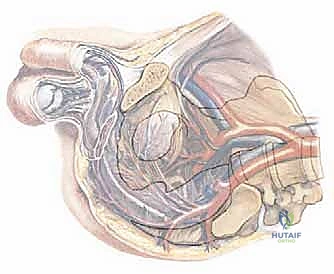
The internal iliac (hypogastric) artery is of paramount importance in the posterior flap hemipelvectomy. Branching from the common iliac artery, it dives deep into the true pelvis, supplying the pelvic viscera and, crucially, giving rise to the superior and inferior gluteal arteries. These gluteal vessels exit the pelvis through the greater sciatic foramen to supply the gluteus maximus muscle. In a "modified" hemipelvectomy, preserving the internal iliac artery and its gluteal branches is essential to maintain the vascularity of the posterior myocutaneous flap. Conversely, in a "classic" hemipelvectomy where the tumor dictates ligation of the common iliac or internal iliac artery at its origin, the gluteus maximus becomes entirely dependent on collateral circulation from the lumbar and circumflex iliac vessels, drastically increasing the risk of postoperative flap necrosis.
Visceral and Soft Tissue Relationships
The pelvis is a densely packed anatomical crossroads, housing terminal portions of the gastrointestinal, urinary, and reproductive tracts. During the retroperitoneal phase of the operation, the peritoneum and its contents must be meticulously swept medially. The sigmoid colon and rectum are particularly vulnerable during left-sided amputations and must be identified and protected when dividing the pelvic floor musculature (levator ani and coccygeus). Preoperative insertion of a rectal tube assists the surgeon in palpating the rectum, preventing inadvertent enterotomies that would catastrophically contaminate the massive surgical wound.
The genitourinary tract presents its own set of hazards. The ureters cross anterior to the bifurcation of the common iliac vessels and must be identified—often aided by their characteristic peristalsis or preoperatively placed lighted stents—and gently retracted medially. The bladder and urethra lie in intimate proximity to the pubic symphysis. When dividing the symphysis, extreme caution must be exercised to avoid lacerating the urethra or the highly vascular periprostatic venous plexus (in males) or perivaginal plexus (in females). The posterior flap itself is primarily composed of the gluteus maximus muscle, overlying subcutaneous fat, and skin. Its elevation requires precise detachment from its femoral and iliotibial band insertions while carefully protecting its deep neurovascular pedicle emerging from the sciatic notch.
Exhaustive Indications and Contraindications
Oncologic and Non-Oncologic Indications
The decision to proceed with a hemipelvectomy is profound and is typically reached only after exhaustive multidisciplinary tumor board discussions. The most frequent indication is a high-grade, non-metastatic primary bone or soft tissue sarcoma of the pelvis or proximal thigh that has failed to respond to neoadjuvant therapies, or one that is anatomically situated such that limb-sparing wide excision is impossible without leaving gross residual tumor. Extremely large sarcomas that invade multiple compartments, encase the sciatic nerve, or involve the major iliofemoral vessels often necessitate immediate radical amputation to achieve clear oncologic margins and prevent tumor fungation.
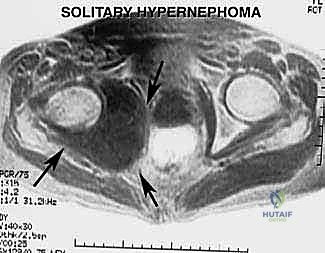
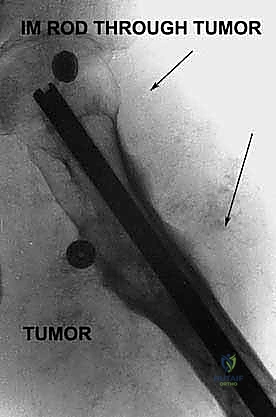
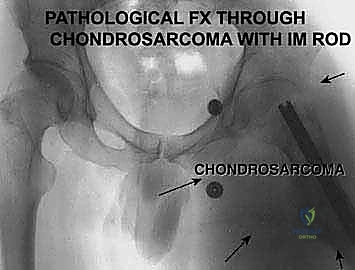
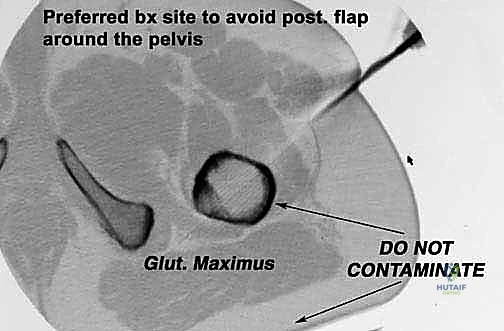
Beyond primary sarcomas, massive contamination of surrounding structures often forces the surgeon's hand toward amputation. Inappropriately placed biopsy tracts, unplanned intralesional excisions ("whoops" surgeries) performed outside of tertiary referral centers, or pathologic fractures through massive tumor burdens can contaminate vast volumes of pelvic and thigh tissue. In these scenarios, the wide margins required for curative intent can only be achieved via hemipelvectomy. Furthermore, solitary, highly destructive metastatic lesions—such as those from renal cell carcinoma or thyroid carcinoma—may be treated with hemipelvectomy for curative intent or durable palliation when the lesion is causing intractable pain, hemorrhage, or loss of pelvic stability.


Absolute and Relative Contraindications
While hemipelvectomy can be life-saving, it is not universally applicable. Absolute contraindications include the presence of widely disseminated metastatic disease, unless the procedure is being performed strictly for the palliation of a fungating, bleeding, or severely infected primary tumor mass. Additionally, patients with severe cardiopulmonary comorbidities who cannot tolerate the massive fluid shifts, profound intraoperative blood loss (often exceeding 3-5 liters), and the extended duration of general anesthesia are not candidates for this radical surgery.
Relative contraindications revolve around local tumor anatomy. If the tumor extends significantly across the midline, invading the contralateral sacral plexus or the contralateral iliac vessels, achieving a negative margin via a unilateral hemipelvectomy becomes anatomically impossible. In such cases, alternative palliative measures or hemicorporectomy (translumbosacral amputation) might be considered, though the latter carries an extraordinarily high mortality rate. Severe malnutrition and profound immunosuppression are also relative contraindications, as the massive posterior flap requires robust host healing capacity to prevent catastrophic necrosis and subsequent pelvic sepsis.
| Category | Indications for Posterior Flap Hemipelvectomy | Contraindications (Absolute & Relative) |
|---|---|---|
| Oncologic | - High-grade pelvic/thigh sarcoma unresponsive to neoadjuvant therapy - Massive tumor encasing major neurovascular bundles - Pathologic fracture with massive compartment contamination - Unplanned intralesional excision of sarcoma - Solitary, destructive metastasis (e.g., RCC) for palliation/cure |
- Widely disseminated metastatic disease (Absolute, unless palliative) - Tumor crossing midline involving contralateral neurovascular structures (Absolute) |
| Infectious/Trauma | - Uncontrollable, ascending necrotizing fasciitis of the lower extremity/pelvis - Massive, unsalvageable crush injury to the hemipelvis - Chronic, intractable osteomyelitis of the pelvis with systemic sepsis |
- Active, untreated systemic bacteremia unrelated to the surgical site (Relative) |
| Physiological | - Intractable pain from fungating mass | - Severe cardiopulmonary disease unable to tolerate massive blood loss (Absolute) - Profound malnutrition/cachexia precluding wound healing (Relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Multidisciplinary Coordination
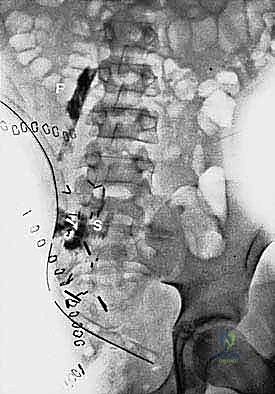
The success of a hemipelvectomy is predicated on exhaustive preoperative planning. Advanced cross-sectional imaging is mandatory. High-resolution MRI of the pelvis with and without intravenous contrast is the gold standard for delineating the soft tissue extent of the tumor, assessing marrow involvement, and mapping the relationship of the mass to the lumbosacral plexus and pelvic viscera. A fine-cut CT scan of the pelvis is essential for evaluating cortical bone destruction and planning the exact trajectory of the osteotomies. Increasingly, 3D printed anatomical models are utilized to conceptualize complex extended resections and to pre-contour any necessary reconstructive meshes or hardware.
This procedure demands a highly coordinated multidisciplinary team. The orthopaedic oncologist must collaborate closely with general surgeons or urologists to manage visceral involvement, particularly if a "compound hemipelvectomy" (involving en bloc resection of the bladder or rectum) is anticipated. Preoperative bowel preparation is absolute, and prophylactic broad-spectrum antibiotics must be administered to mitigate the high risk of infection from accidental visceral injury. In cases of highly vascular tumors (e.g., renal cell carcinoma metastases or certain soft tissue sarcomas), preoperative angioembolization of the internal iliac or specific tumor-feeding vessels performed 24 to 48 hours prior to surgery can dramatically reduce intraoperative blood loss and improve visualization.
Anesthesia, Hemodynamic Monitoring, and Positioning
The anesthetic management for a hemipelvectomy is as complex as the surgery itself. Patients require comprehensive invasive hemodynamic monitoring, including an arterial line, a central venous pressure (CVP) catheter, and large-bore peripheral access. A massive transfusion protocol must be initiated preemptively, with a minimum of 6 to 10 units of packed red blood cells, fresh frozen plasma, and platelets available in the operating room. A Foley catheter with a large, inflated balloon is placed to decompress the bladder and aid in its intraoperative palpation. A rectal tube is similarly placed to decompress the lower GI tract.
Patient positioning is critical for optimal exposure. The patient is typically placed in a "floppy" lateral decubitus position on a radiolucent bean bag. This allows the surgeon to roll the patient anteriorly or posteriorly as the dissection dictates. The entire hemipelvis, lower extremity, abdomen up to the costal margin, and the contralateral thigh are meticulously prepped and draped free. The ipsilateral leg is draped in a sterile fashion to allow the surgical assistant to manipulate the limb, utilizing it as a massive lever arm during the final stages of disarticulation and delivery of the specimen.
Step-by-Step Surgical Approach and Fixation Technique
Incision Design and Anterior Dissection
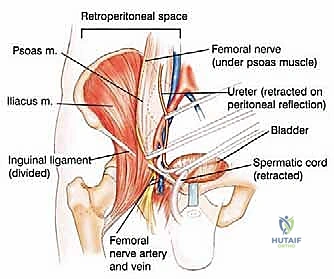
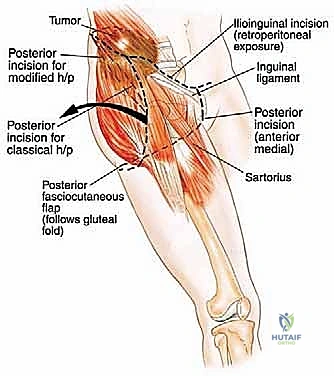
The classic incision for a posterior flap hemipelvectomy is racquet-shaped. The anterior limb begins at the pubic symphysis, courses laterally along the inguinal ligament to the anterior superior iliac spine (ASIS), and extends posteriorly along the iliac crest. The posterior limb drops from the iliac crest, curving distally and medially across the greater trochanter, following the gluteal fold to meet the anterior incision at the perineum. The anterior dissection begins by incising the abdominal musculature (external oblique, internal oblique, and transversus abdominis) directly off the iliac crest.
Once the abdominal wall is detached, the surgeon enters the retroperitoneal space. The peritoneum and its visceral contents are gently swept medially using blunt dissection and laparotomy sponges. The ureter is identified and protected. The external iliac artery and vein are isolated, doubly ligated with heavy silk sutures or vascular staplers, and divided. The femoral nerve is identified and sharply transected high in the pelvis. If oncologically permissible, the internal iliac artery is preserved to maintain blood supply to the gluteus maximus; if not, it is ligated at its origin. The spermatic cord or round ligament is identified and typically divided to facilitate exposure of the pubic symphysis.
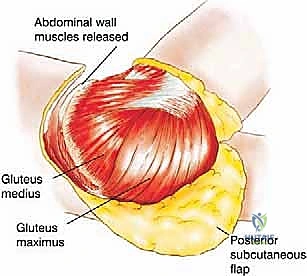
Posterior Dissection and Flap Elevation
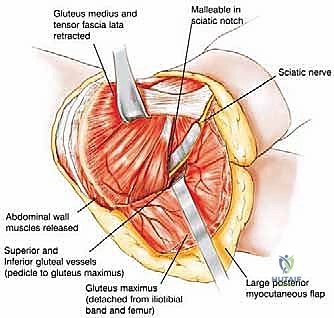
With the anterior structures secured, attention turns to the posterior flap. The skin and subcutaneous tissues of the posterior thigh and buttock are incised. The gluteus maximus is identified and its distal insertion on the gluteal tuberosity of the femur and the iliotibial tract is sharply detached. The muscle is then elevated from distal to proximal, taking extreme care to identify and preserve the superior and inferior gluteal neurovascular bundles as they exit the greater sciatic notch.
Deep to the gluteus maximus, the short external rotators of the hip (piriformis, obturator internus, gemelli, and quadratus femoris) are divided. The massive sciatic nerve is identified, isolated, and sharply transected as high as possible. Prior to transection, the nerve is often injected with a long-acting local anesthetic to mitigate postoperative phantom limb pain, and it is allowed to retract deep into the pelvic musculature to prevent painful neuroma formation near the skin surface. The hamstring muscles are detached from the ischial tuberosity, completely freeing the posterior aspect of the hemipelvis.
Osteotomies and Specimen Delivery
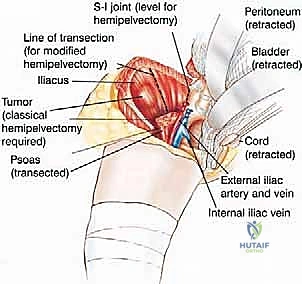
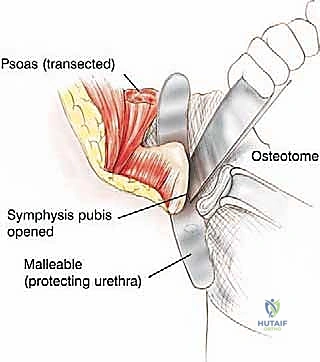
The critical bony disarticulations are now performed. Anteriorly, the pubic symphysis is cleared of soft tissue. A Gigli saw or a broad, sharp osteotome is utilized to divide the symphysis. The surgeon must place a protective retractor (such as a malleable or right-angle retractor) immediately posterior to the symphysis to shield the bladder and urethra from the saw blade. Posteriorly, the sacroiliac joint is addressed. The robust anterior and posterior sacroiliac ligaments are divided.
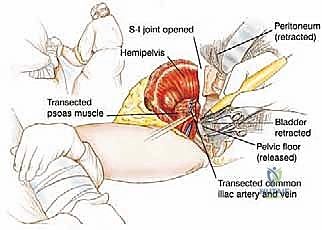
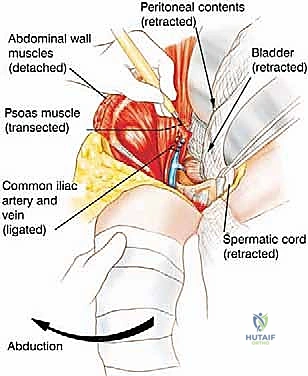
Depending on the preoperative plan, the ilium is either disarticulated directly through the SI joint or an osteotomy is performed through the sacral ala or iliac wing using an oscillating saw or osteotomes. As the bony ring is broken, the assistant uses the leg to externally rotate and abduct the hemipelvis, opening the deep pelvic floor like a book. The final tethering structures—the levator ani, coccygeus muscles, and the sacrotuberous/sacrospinous ligaments—are divided under direct vision, taking care to avoid injuring the adjacent rectum. The entire hemipelvis and lower extremity are then delivered en bloc off the operative field.
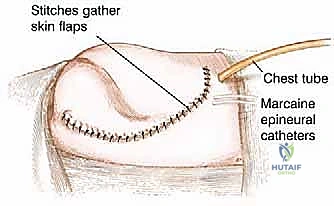
Hemostasis, Drain Placement, and Flap Closure
Following specimen removal, the massive surgical void requires meticulous attention. The presacral venous plexus is a notorious source of persistent, difficult-to-control hemorrhage. Hemostasis is achieved using a combination of electrocautery, bone wax, hemostatic matrix agents (e.g., Floseal, Surgicel), and judicious packing. The wound is copiously irrigated with pulsatile lavage. Given the vast dead space, multiple large-bore closed-suction drains (e.g., 10-mm Jackson-Pratt or Blake drains) are placed strategically: deep in the presacral space, along the retroperitoneum, and immediately beneath the subcutaneous flap.

Closure of the posterior flap is a critical biomechanical reconstruction. The gluteus maximus is rotated anteriorly to cover the pelvic viscera. Its robust fascial edge is sutured securely to the anterior abdominal wall musculature (external oblique and rectus abdominis) and the inguinal ligament using heavy, non-absorbable or slowly absorbable continuous sutures (e.g., #1 or #2 PDS). This fascial repair must be absolutely tension-free to prevent dehiscence and subsequent herniation of abdominal contents.