Masterclass in Hindfoot and Ankle Amputations

Key Takeaway
Hindfoot and ankle amputations, notably the Syme amputation, provide a highly functional, end-bearing stump when executed with meticulous surgical technique. Success relies on preserving the specialized heel pad, ensuring adequate vascularity, and preventing posterior pad migration. This guide details the indications, biomechanics, and step-by-step surgical techniques for the classic Syme, two-stage Syme, Boyd, and Pirogoff amputations, optimizing outcomes for prosthetic fitting and patient mobility.
Comprehensive Introduction and Patho-Epidemiology
Amputations around the ankle joint represent a critical and highly nuanced intersection of orthopedic biomechanics, vascular surgery, and advanced prosthetic engineering. To be deemed successful, these procedures must flawlessly fulfill two non-negotiable biomechanical requirements: first, they must provide a durable, end-bearing stump capable of withstanding the immense compressive and shear forces of human locomotion; second, they must leave sufficient spatial clearance between the distal end of the bony stump and the ground to accommodate the construction and integration of a functional prosthetic ankle joint mechanism. The mastery of hindfoot amputations distinguishes the meticulous reconstructive surgeon from the mere ablative operator.
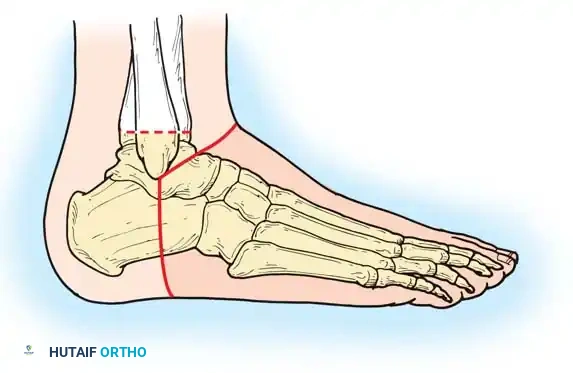
Historically, amputations at this anatomical level were plagued by catastrophic rates of poor wound healing, flap necrosis, and insurmountable prosthetic fitting challenges. However, in 1843, the pioneering Scottish surgeon James Syme described an ankle disarticulation technique that elegantly met these requirements better than any other procedure in the distal lower extremity. The classic Syme amputation involves a precise bone section through the distal tibia and fibula approximately 0.6 cm proximal to the periphery of the ankle joint, passing centrally through the dome of the tibial plafond. Crucially, the tough, highly specialized, and durable skin of the heel flap is meticulously preserved and rotated to provide a near-normal weight-bearing surface.
From an epidemiological standpoint, the landscape of lower extremity amputations has shifted dramatically over the past century. While trauma and infectious gangrene dominated the etiology in Syme’s era, contemporary practice is overwhelmingly driven by the global pandemic of diabetes mellitus and peripheral arterial disease (PAD). Diabetic foot ulcers complicated by deep space infection, osteomyelitis of the midfoot or hindfoot, and ascending necrotizing soft tissue infections constitute the vast majority of indications today. Less common, yet equally challenging, etiologies include severe crush injuries to the forefoot and midfoot, unconstructable congenital deformities (such as severe fibular hemimelia or proximal focal femoral deficiency requiring limb length equalization), and malignant neoplasms of the foot.
The clinical reality of the Syme amputation is binary; there is absolutely no "middle ground" in its execution. When executed perfectly in a properly selected patient, it yields the most satisfactory, energy-efficient functional amputation level in the lower extremity, allowing patients to ambulate short distances without a prosthesis—a massive advantage for nocturnal bathroom visits. Conversely, when executed poorly, or in the face of inadequate vascular perfusion, it is functionally valueless, inevitably necessitating morbid revision to a more proximal level, typically a transtibial (below-knee) amputation.
Detailed Surgical Anatomy and Biomechanics
Vascular Angiosomes and Soft Tissue Envelope
A profound understanding of the vascular anatomy of the hindfoot is the absolute prerequisite for success in ankle-level amputations. The survival of the crucial heel pad relies entirely on the posterior tibial artery and its terminal branches. The heel pad is supplied by the calcaneal branches of the posterior tibial artery, which form a rich anastomotic network with the calcaneal branches of the peroneal artery. This specific vascular territory, or angiosome, must be meticulously protected during the medial and lateral dissection. The concept of "dog ears" at the medial and lateral apices of the surgical incision is paramount; these redundant tissue folds contain the critical microvascular anastomoses that perfuse the heel flap. Aggressive surgical trimming of these dog ears for immediate cosmetic contouring invariably compromises the blood supply to the entire flap, leading to ischemic necrosis and catastrophic failure of the amputation.
The heel pad itself is a marvel of evolutionary bioengineering. It consists of highly specialized, pressure-tolerant adipose tissue compartmentalized by dense, U-shaped fibrous septa that anchor the thick plantar dermis directly to the periosteum of the calcaneus.
These septa create a hydraulic shock-absorbing mechanism capable of dissipating the massive kinetic energy generated during the heel-strike phase of the gait cycle. During the subperiosteal dissection of the calcaneus, the surgeon must stay strictly on the bone; violating the subcutaneous fat and severing these fibrous septa destroys the structural integrity of the heel pad, rendering it a highly mobile, shear-prone mass of fat that will rapidly ulcerate under the loads of prosthetic weight-bearing.
Neuroanatomy and Neuroma Prevention
The neuroanatomy of the hindfoot amputation dictates the postoperative comfort of the patient. The primary sensory nerves encountered are the medial and lateral plantar nerves (terminal branches of the tibial nerve), the sural nerve laterally, the saphenous nerve medially, and the deep and superficial peroneal nerves anteriorly. Failure to properly manage these nerves results in symptomatic terminal neuromas, which are particularly devastating in an end-bearing stump. The surgical imperative is to dissect each nerve proximally, apply gentle distal traction, and transect the nerve sharply with a fresh scalpel blade, allowing the proximal stump to retract deep into the well-vascularized muscular compartments of the distal leg, far away from the distal weight-bearing interface and the rigid socket of the prosthesis.
Biomechanics of the End-Bearing Stump
Unlike a transtibial amputation, which relies on a total-contact, pressure-distributing socket (such as the Patellar Tendon Bearing or PTB socket) to transfer loads through the proximal tibia and soft tissues, the Syme and Boyd amputations are true end-bearing constructs. The distal end of the stump directly accepts the axial load of the body. This significantly reduces the complexity of prosthetic suspension and allows for a more proprioceptively intuitive gait. However, because the distal tibial metaphysis flares outward and is covered by thick, heavy plantar skin, the resulting classic Syme stump is inherently large and bulbous. While this bulbous nature aids in prosthetic suspension (the "stovepipe" effect), it severely limits the cosmetic appeal of the prosthesis, as the ankle region must be manufactured significantly wider than the contralateral sound limb to accommodate the stump.
Exhaustive Indications and Contraindications
The decision to proceed with a hindfoot amputation requires a rigorous evaluation of the patient's systemic health, local tissue perfusion, and rehabilitation potential. The paradigm has shifted from viewing amputation as a failure of limb salvage to recognizing it as the definitive first step in functional rehabilitation.
| Parameter | Indications for Hindfoot Amputation | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Vascular / Perfusion | ABI > 0.45; TcPO2 > 30 mm Hg; palpable posterior tibial pulse. | Ischemic limb with ABI < 0.3; TcPO2 < 20 mm Hg; absent Doppler signals in the posterior tibial artery. | Non-compressible vessels (ABI > 1.3) requiring toe pressures; severe venous stasis. |
| Infection | Unsalvageable midfoot/forefoot osteomyelitis; localized gangrene distal to the Chopart joint. | Ascending necrotizing fasciitis; active infection extending into the heel pad or proximal to the ankle joint. | Poorly controlled systemic sepsis (requires open guillotine amputation first). |
| Trauma | Severe crush injury to the forefoot/midfoot with intact heel pad; traumatic forefoot amputation. | Extensive degloving of the heel pad; severe comminution of the distal tibial plafond. | Concomitant severe ipsilateral proximal fractures delaying weight-bearing. |
| Oncology | Malignant tumors of the forefoot/midfoot requiring wide margins. | Tumors involving the distal tibia, calcaneus, or posterior compartment. | Extensive metastatic disease with life expectancy < 3 months. |
| Neuropathy / Deformity | End-stage Charcot neuroarthropathy of the midfoot with recurrent ulceration. | Complete insensate heel pad with a history of prior posterior heel ulceration. | Severe, uncorrectable equinovarus deformity of the proximal tibia/knee. |
Never proceed with a Syme amputation in a vasculopathic or diabetic patient without objective, non-invasive vascular testing. Clinical palpation of pulses is dangerously insufficient. Success rates have dramatically increased by utilizing Transcutaneous Oxygen Measurements (TcPO2), where a value greater than 30 mm Hg at the proposed level of amputation is a strong, validated predictor of successful primary wound healing. In highly specialized centers, radioactive Xenon clearance tests and Skin Perfusion Pressure (SPP) mapping are utilized to delineate the exact ischemic penumbra.
Pre-Operative Planning, Templating, and Patient Positioning
Imaging and Templating
Pre-operative planning begins with high-quality orthogonal radiographs of the ankle and foot to assess the integrity of the distal tibia, fibula, and calcaneus. In cases of diabetic foot infection, Advanced imaging, specifically contrast-enhanced Magnetic Resonance Imaging (MRI), is mandatory to definitively rule out proximal tracking of deep space abscesses or osteomyelitis extending into the calcaneus, which would strictly contraindicate a Syme or Boyd procedure. Angiography (CT or invasive) is reviewed in conjunction with the vascular surgery team; if the posterior tibial artery is occluded but reconstructable, a preliminary endovascular or open bypass should be performed to optimize inflow prior to amputation.
Templating is critical for determining the level of bone transection. For the classic Syme, the osteotomy is templated 0.6 cm proximal to the joint line, parallel to the ground. For the Sarmiento modification, the cut is planned 1.3 cm proximal to the joint line. For the Boyd amputation, precise templating of the calcaneal osteotomy and the distal tibial cut is required to ensure optimal limb length and a congruent arthrodesis surface.

Patient Positioning and Operating Room Setup
The patient is placed in the supine position on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, counteracting the natural external rotation of the hip and allowing unrestricted access to both the medial and lateral malleoli. A pneumatic tourniquet is applied to the proximal thigh.
Surgical Warning: In patients with severe peripheral arterial disease or heavily calcified vessels, the use of a tourniquet is highly controversial and often contraindicated. Tourniquet inflation can cause plaque rupture, acute thrombosis, or severe ischemic reperfusion injury to the marginal flaps. In these patients, the procedure must be performed under careful hemostatic control without a tourniquet.
Prophylactic intravenous antibiotics targeting skin flora and, in diabetic patients, deep anaerobic and gram-negative pathogens, are administered 30 minutes prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
Meticulous soft tissue handling, strict adherence to anatomic planes, and precise osteotomies are required to construct a durable hindfoot stump. The following details the exhaustive steps for the Classic Syme, the Sarmiento Modification, and the alternative Boyd and Pirogoff procedures.
The Classic Syme Amputation
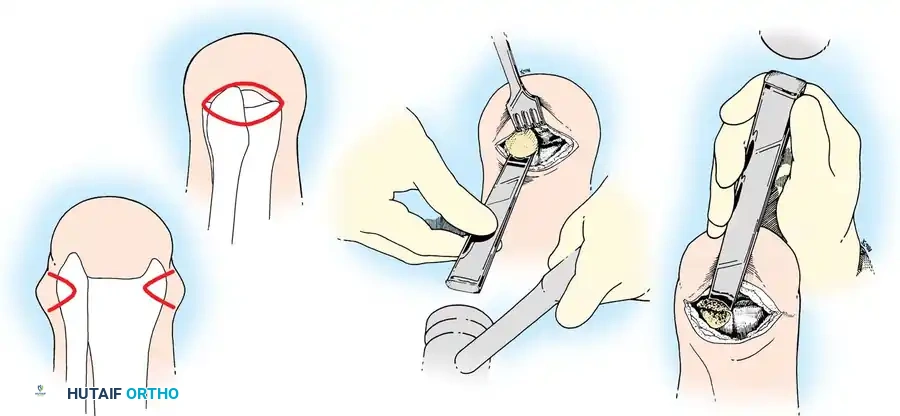
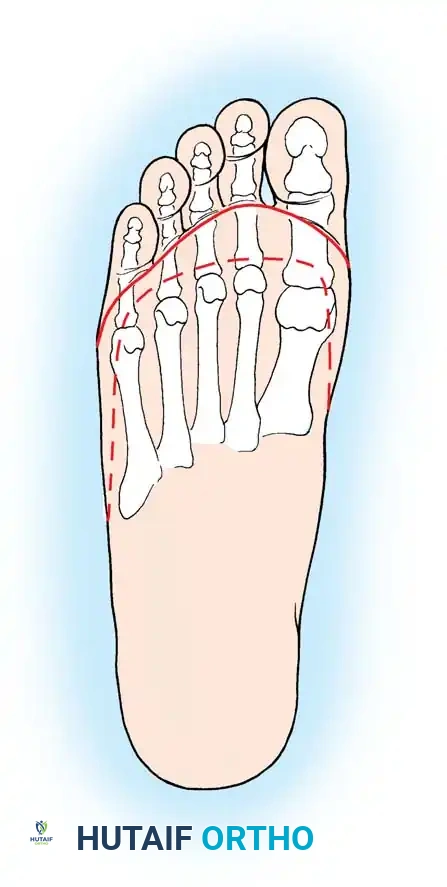
Step 1: Incision and Exposure
The design of the flap is the most critical step. A single, long posterior heel flap is utilized. Begin the incision exactly at the distal tip of the lateral malleolus. Pass the scalpel across the anterior aspect of the ankle joint at the level of the distal tibia to a point exactly one fingerbreadth inferior to the tip of the medial malleolus. This precise asymmetry accounts for the differing distal extents of the malleoli.
Extend the incision directly plantarward, cutting perpendicularly through the thick skin and plantar fascia across the sole of the foot to the lateral aspect, ending precisely at the starting point.

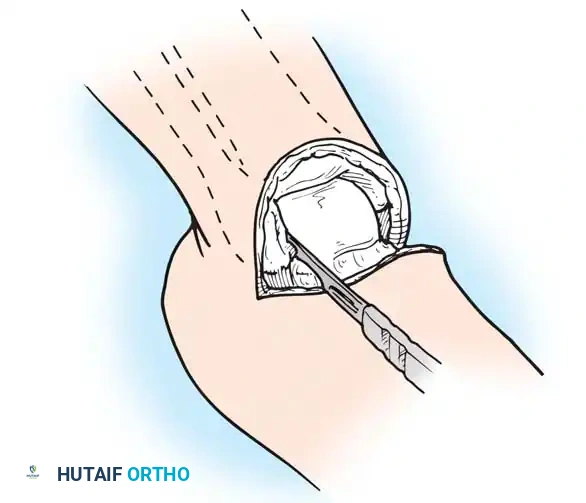
Step 2: Joint Disarticulation
Divide all anterior structures straight down to the bone. Identify the anterior tibial artery as it lies in the anterior flap, clamp, and securely ligate it with a non-absorbable suture. Identify and sharply transect the deep peroneal nerve, allowing it to retract proximally.
Place the foot in marked equinus to place the anterior capsule of the ankle joint under tension. Divide the capsule transversely to expose the talar dome.
Insert a scalpel into the joint space between the medial malleolus and the talus. Draw it inferiorly to section the deltoid ligament.
Crucial Pitfall: The posterior tibial artery lies immediately posterior to the medial malleolus. The scalpel blade must be kept strictly within the joint space and directed laterally against the talus to avoid catastrophic transection of the primary blood supply to the heel flap.
Repeat this maneuver on the lateral side to section the calcaneofibular and anterior talofibular ligaments.
Step 3: Posterior Dissection and Calcanectomy
Place a heavy bone hook into the posterior aspect of the talus to provide forceful, continuous equinus traction. This opens the posterior aspect of the joint. Proceed with posterior dissection, dividing the posterior capsule of the ankle joint.

Identify the Achilles tendon as it inserts into the calcaneal tuberosity. Divide it directly at its insertion.
Pitfall: Do not damage the overlying posterior skin during the Achilles tenotomy. The skin here is exceedingly thin. Buttonholing the skin or deeply scoring the subdermal plexus will lead to inevitable necrosis of the entire posterior heel flap.

Using a sharp periosteal elevator, dissect the soft tissues from the lateral and medial surfaces of the calcaneus. Keep the instrument firmly pressed against the bone. Pull the bone into extreme equinus.
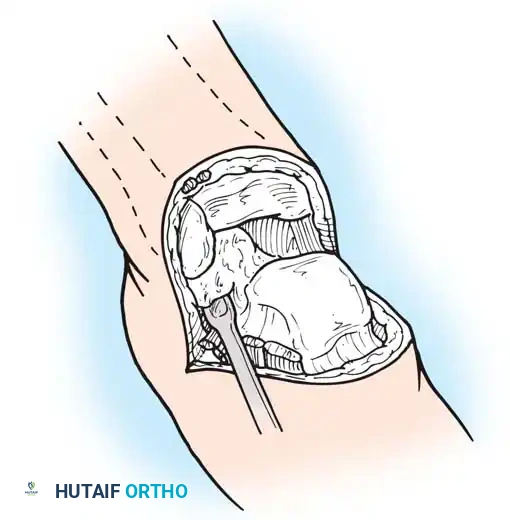
Continue this strict subperiosteal dissection on the inferior surface of the calcaneus until the distal end of the plantar skin flap is reached. Remove the entire foot, leaving only the robust heel flap.
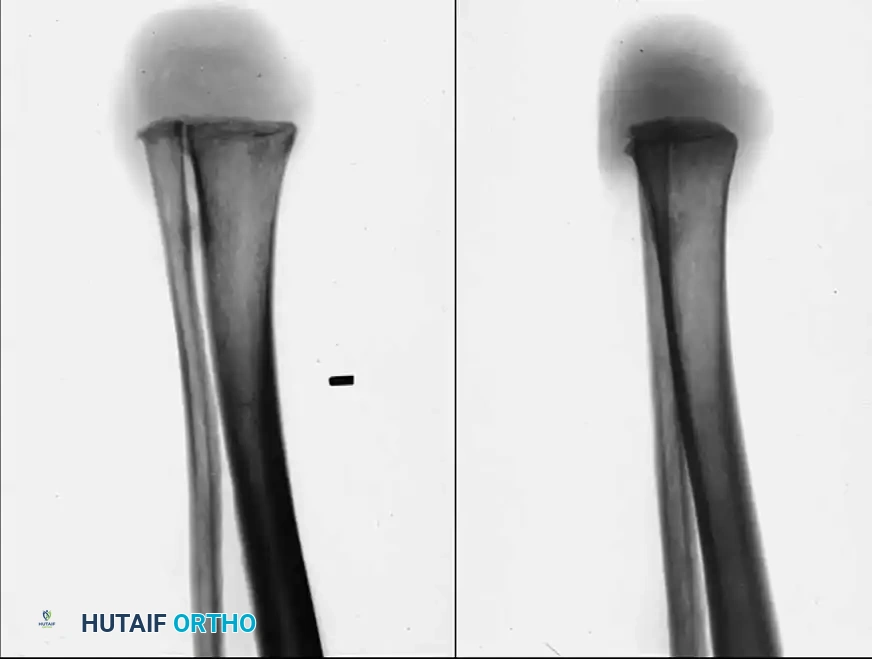
Step 4: Bone Transection
Retract the heel flap posteriorly using a moist laparotomy sponge to protect the tissue. Dissect the soft tissue circumferentially from the distal tibia and malleoli. Incise the periosteum circumferentially exactly 0.6 cm proximal to the joint line.
Using a wide oscillating saw, divide the tibia and fibula at this level. The line of transection must pass just through the dome of the ankle joint centrally, removing the articular cartilage but preserving the broad metaphyseal flare.
Alignment: The plane of the transection must be perfectly parallel to the ground when the patient is standing. This usually requires a cut that is perpendicular to the mechanical axis of the tibia in both the coronal and sagittal planes. Round and smooth all sharp cortical edges, particularly the anterior tibial crest and the lateral fibular border, with a bone rasp.
Step 5: Soft Tissue and Nerve Management
Identify the medial and lateral plantar nerves in the medial aspect of the flap. Dissect them proximally into the tarsal tunnel, apply tension, and divide them sharply so they retract well proximal to the bone end.
Pull all visible tendons (tibialis posterior, FDL, FHL, peroneals) inferiorly, section them under tension, and allow them to retract proximally into the muscular compartments of the leg.
Isolate the posterior tibial artery and vein. Ligate them securely just proximal to the cut distal edge of the heel flap to preserve the maximum length of the calcaneal branches.
Perform minimal debridement of any soft-tissue tags of plantar muscle (abductor hallucis, flexor digitorum brevis) lining the inner surface of the heel flap. Preserve the subcutaneous fat and its fibrous septa entirely intact.
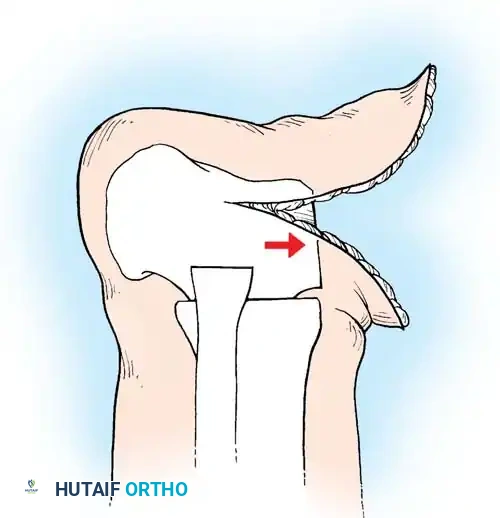
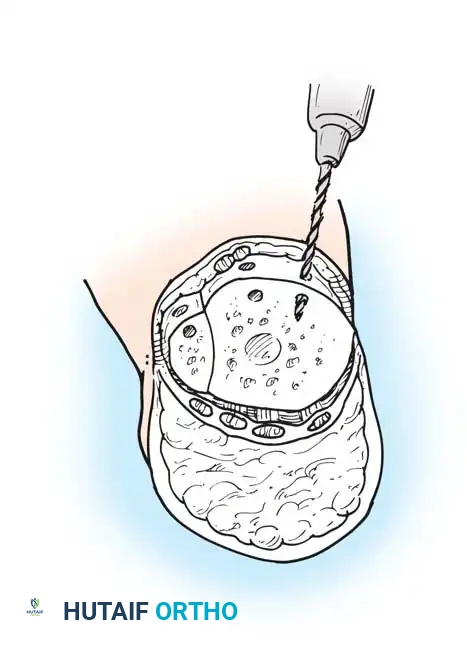
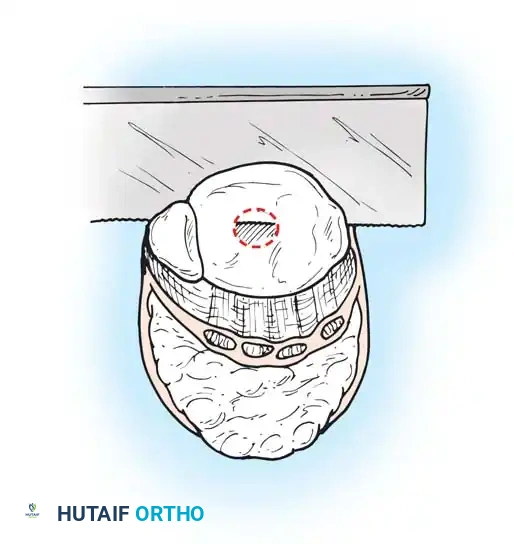
Step 6: Anchoring the Heel Pad (Wagner Technique)
To prevent the disastrous complication of posterior heel pad migration under the shear forces of ambulation, the pad must be rigidly fixed to the distal tibia. Drill several small transverse holes through the anterior edge of the distal tibia and fibula.
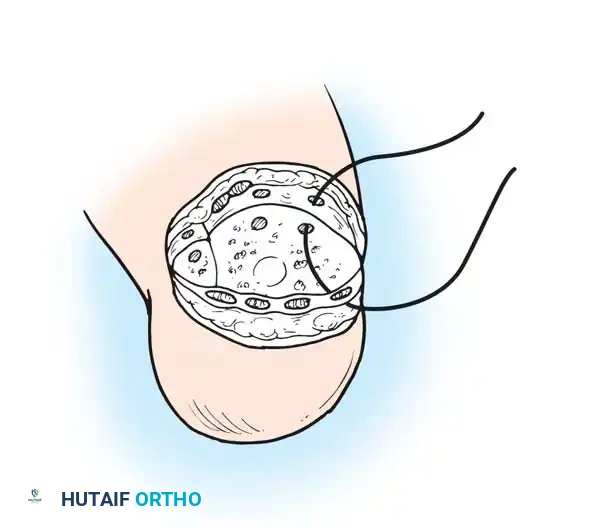
Pass heavy, nonabsorbable sutures (e.g., #2 FiberWire or Ethibond) through these drill holes and anchor them securely to the robust deep fascia lining the anterior edge of the heel flap. Tie these sutures with the heel pad held in a perfectly centralized position over the distal tibia.

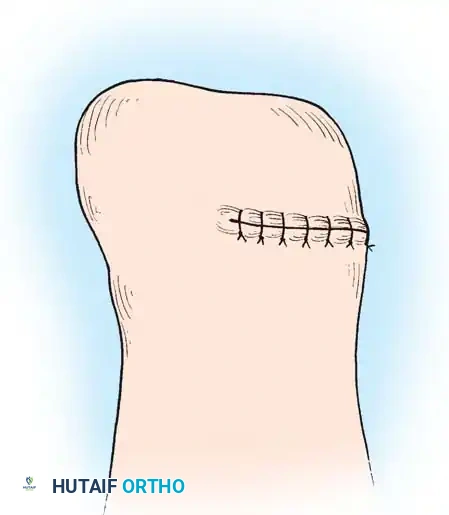
Step 7: Closure
Approximate the skin edge of the heel flap to the anterior flap using interrupted nonabsorbable vertical mattress sutures (e.g., 3-0 nylon). Ensure there is absolutely zero tension on the closure.
Crucial Step: Large, protruding tags of skin ("dog ears") will inevitably form at the medial and lateral ends of the suture line. Never excise these. They carry the primary microvascular blood supply to the heel flap and will naturally remodel and shrink over 6 to 8 weeks under postoperative compressive bandaging.

Place a closed suction drain deep into the flap and exit it laterally, proximal to the incision. Apply a rigid cast extending above the knee. Remove the drain at 24 to 48 hours via a window in the cast.
The Sarmiento Modification
To address the cosmetic shortcomings of the classic bulbous technique, Sarmiento described a modification that produces a more cylindrical stump.
* Technique: The surgical approach is identical, but the tibia and fibula are transected approximately 1.3 cm proximal to the ankle joint, and the medial and lateral malleoli are completely excised along with the metaphyseal flare.
* Advantage: This produces a stump only slightly larger in circumference than the diaphyseal portion of the leg. It allows the patient to be fitted with a highly cosmetic prosthesis incorporating an expandable inner socket rather than a bulky removable medial window.
The Two-Stage Syme Amputation (Wagner Protocol)
Developed specifically to salvage limbs in diabetic patients presenting with gross infection or gangrene of the forefoot, this technique boasts a 95% success rate in properly selected patients.
- Stage 1 (Debridement and Disarticulation): Perform a standard ankle disarticulation. Key Difference: Preserve the tibial articular cartilage and the medial/lateral malleoli entirely. The avascular cartilage acts as a biologic barrier to proximal bacterial seeding into the cancellous bone. Perform a loose, Syme-type closure over a robust suction-irrigation system, allowing for continuous instillation of targeted antibiotic solutions directly into the wound bed.
- Stage 2 (Definitive Closure): Once the infection is eradicated (typically 4 to 6 weeks later, confirmed by negative tissue cultures and normalized inflammatory markers), the patient returns to the OR. The malleoli are excised, the tibial plafond is prepared, and the heel pad is definitively anchored and closed as described in the classic technique.
Alternative Hindfoot Amputations: Boyd and Pirogoff
While the Syme amputation is the gold standard, the Boyd and Pirogoff amputations offer alternative methods of achieving an end-bearing stump, primarily by retaining a portion of the calcaneus to permanently prevent heel pad migration.
The Boyd Amputation:
The Boyd amputation produces an excellent end-bearing stump and completely eliminates the risk of posterior heel pad migration because the heel pad remains naturally attached to the retained calcaneus.
- Technique: The procedure involves a complete talectomy. The anterior process of the calcaneus is excised just proximal to the calcaneocuboid joint. The remaining calcaneus is then shifted forward into the ankle mortise. The distal tibia and the superior surface of the calcaneus are denuded of cartilage, and a formal calcaneotibial arthrodesis is performed. Fixation is typically achieved with large threaded Steinmann pins or cannulated screws driven from the plantar aspect of the calcaneus up into the tibia.
- Disadvantages: The required arthrodesis makes this procedure technically much more demanding than a Syme amputation. Nonunion of the calcaneotibial fusion is a significant risk, particularly in diabetic patients. Furthermore, it produces an even more bulbous stump than the Syme, exacerbating prosthetic fitting issues.
The Pirogoff Amputation:
The Pirogoff amputation is a historical variant that is rarely performed today but remains conceptually important.
* Technique: Following a talectomy, the calcaneus is osteotomized vertically. The posterior half of the calcaneus (with the heel pad attached) is rotated 90 degrees forward so that the cut vertical surface of the calcaneus is opposed to the cut horizontal surface of the distal tibia for arthrodesis.
* Disadvantages: It creates a limb length discrepancy that is extremely difficult to manage prosthetically, as the stump is often too long to accommodate a functional prosthetic ankle mechanism, yet too short for normal shoe wear.
Complications, Incidence Rates, and Salvage Management
The complication profile of hindfoot amputations is heavily skewed by the patient's underlying vascular status and the surgeon's meticulousness.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management |
|---|---|---|---|
| Posterior Heel Pad Migration | 10% - 15% | Failure to anchor the pad to the tibia; premature weight-bearing; loss of fixation. | Early: Revision anchoring. Late/Chronic: Revision to transtibial amputation due to anterior tibial ulceration. |
| Skin Slough / Flap Necrosis | 5% - 20% | Ischemia; overly vigorous trimming of "dog ears"; excessive tourniquet time; tight closure. | Small eschar: Local wound care, allow to demarcate. Full-thickness necrosis: Urgent revision to transtibial amputation. |
| Symptomatic Neuroma | 5% - 10% | Inadequate proximal resection of medial/lateral plantar nerves or sural nerve. | Conservative: Socket modification, steroid injections. Surgical: Excision of neuroma and deeper proximal burying. |
| Nonunion (Boyd/Pirogoff) | 10% - 25% | Inadequate bone preparation; poor fixation; infection; severe neuropathy (Charcot). | Prolonged immobilization; bone grafting with rigid internal fixation; revision to Syme or transtibial amputation. |
| Stump Osteomyelitis | 2% - 8% | Contiguous spread from primary infection; hematogenous seeding; exposed bone from flap necrosis. | Aggressive surgical debridement; targeted IV antibiotics; often requires proximal revision amputation. |
The most devastating complication is the posterior migration of the heel pad. If the heel pad is not securely anchored, the shear forces of walking will drive the pad posteriorly, exposing the distal tibia to non-weight-bearing, fragile anterior skin. This inevitably leads to intractable ulceration and osteomyelitis.
Skin slough is equally disastrous. The vascular supply is tenuous, and any tension on the suture line or damage to the subdermal plexus during the calcanectomy will result in marginal necrosis. If the necrosis is superficial, it may heal by secondary intention. However, full-thickness necrosis exposing the distal tibia is an absolute indication for revision to a transtibial amputation.
Phased Post-Operative Rehabilitation Protocols
Optimal postoperative care dictates the application of a properly padded rigid dressing in the operating room immediately following closure. This controls edema, protects the wound from trauma, and prevents equinus contracture of the soft tissues.
Phase 1: Immediate Postoperative Care (Days 0 - 14)
- Immediate Postoperative Cast: Apply a light sterile dressing and a sterile stump sock. The prosthetist or surgeon should fashion and skive sterile felt pads to relieve pressure over the anterior tibial crest and the edges of the transected bones. These are glued to the stump sock.
- Plaster Application: Use elastic plaster of Paris for the initial wrap to control tension, reinforced with conventional plaster or fiberglass. Compression should be maximal over the distal end of the stump, decreasing proximally to promote venous return.
- Positioning: The limb is elevated. The cast usually extends above the knee initially to prevent rotational forces on the healing flap. Strict non-weight-bearing is enforced.
Phase 2: Intermediate Care and Early Mobilization (Weeks 2 - 6)
- Cast Changes: The initial cast is removed at 10 to 14 days to inspect the wound and remove sutures (if healed). A new, intimately fitting below-knee total contact cast is applied.
- Weight Bearing: Flatten the end of the rigid dressing with a board while the plaster is wet to simulate the weight-bearing surface. Mold the proximal cast to create a patellar bar and popliteal bulge (similar to a PTB prosthesis) to allow partial
Clinical & Radiographic Imaging Archive