Mastering Ray Resections: An Intraoperative Guide to Foot Amputations for Oncologic Conditions

Key Takeaway
This masterclass guides fellows through ray resections for foot tumors, emphasizing precise surgical anatomy, comprehensive preoperative planning, and meticulous intraoperative execution. We cover techniques for first, lesser, and fifth ray resections, including fibular strut grafting, ensuring optimal functional outcomes. Learn critical pearls, pitfalls, and postoperative management, focusing on preserving foot biomechanics and preventing complications.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of primary and metastatic neoplasms of the foot presents a unique and formidable challenge to the orthopaedic oncologist. Unlike other anatomical regions of the musculoskeletal system where wide resections can be compensated for by robust soft tissue envelopes or massive endoprosthetic reconstructions, the foot is characterized by its intricate biomechanics, dense compartmentalization, and critical, irreplaceable role in bipedal locomotion. Any surgical intervention in this region, particularly an oncologic resection that mandates the sacrifice of osseous and soft tissue structures to achieve negative margins, demands meticulous preoperative planning and flawless intraoperative execution to preserve a functional, plantigrade, and painless extremity.
The foot functions fundamentally as a dynamic tripod during the stance phase of gait. The first ray, the fifth ray, and the calcaneus form its primary weight-bearing pillars. This architectural configuration, coupled with the inherent structural stability of the midfoot's Roman arch, facilitates the efficient absorption, translation, and distribution of ground reaction forces. When a surgeon performs a ray resection—defined as the amputation of a toe along with all or a portion of its corresponding metatarsal—this delicate biomechanical equilibrium is profoundly disrupted.
Resections of the border rays (first and fifth) induce the most significant functional alterations. A first ray resection, for instance, eliminates the primary medial column strut, which normally bears up to 50% of the body's weight during the terminal stance (toe-off) phase of gait. The loss of the first ray inevitably results in an abrupt transfer of mechanical forces to the lesser metatarsals. Because these smaller, more slender metatarsals are structurally unequipped to bear the body's full weight, patients frequently develop chronic, debilitating transverse metatarsalgia, and are at a high risk for lesser metatarsal stress fractures postoperatively. Conversely, a fifth ray resection is generally better tolerated from a weight-bearing perspective, though it compromises lateral column stability. Compensation is often successfully achieved through custom orthotics featuring lateral posts and medial arch supports that shift forces medially. Resection of the central rays (second, third, or fourth), surprisingly, often results in the least profound global functional deficit. The primary consequence is a narrowing of the forefoot (a surgically induced cleft foot deformity) and potential splaying of the remaining digits, which can typically be managed with appropriate shoe modifications and custom toe fillers.
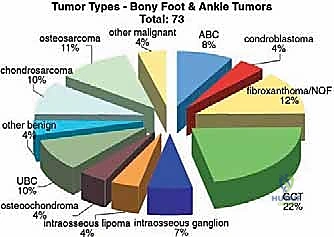
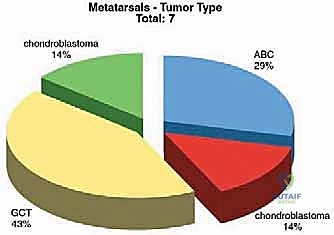
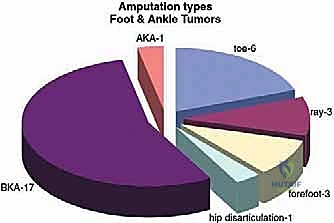
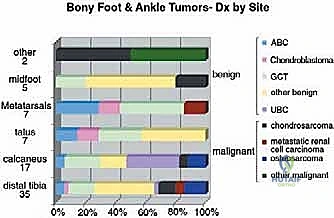
Malignant tumors of the foot are exceedingly rare, accounting for less than 5% of all primary musculoskeletal sarcomas, and are even rarer distal to the metatarsophalangeal (MTP) joints. Synovial sarcoma, clear cell sarcoma, and epithelioid sarcoma are among the most frequently encountered soft tissue malignancies in this region, while chondrosarcoma and Ewing sarcoma represent the more common primary bone malignancies. Benign lesions, such as plantar fibromatosis, giant cell tumor of tendon sheath, and enchondromas, are encountered with much greater frequency. However, regardless of whether a lesion is benign and locally aggressive or frankly malignant, the fundamental oncologic principles of achieving adequate surgical margins remain paramount. The compact nature of the foot often precludes the ability to obtain wide margins without sacrificing critical neurovascular structures or joint complexes, frequently forcing the surgeon to choose between a functionally compromising ray resection and a more proximal amputation, such as a Syme or below-knee amputation (BKA).
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical incision, a profound mastery of pedal anatomy is non-negotiable. The foot is a marvel of evolutionary engineering, comprising 26 bones, 33 complex articulations, over 100 muscles, tendons, and ligaments, and a dense, highly arborized neurovascular network, all constrained within a remarkably small and unforgiving anatomical volume.
Osteology and Arch Mechanics
The osseous framework is divided into the hindfoot, midfoot, and forefoot. For the context of ray resections, our focus is primarily on the forefoot and midfoot articulations. Each "ray" consists of a metatarsal and its associated phalanges. The first ray, comprising the robust first metatarsal, the medial cuneiform, and the hallux (with its associated sesamoid complex), is the biomechanical anchor of the medial column. The lesser rays (second through fourth) are more slender and articulate with the intermediate and lateral cuneiforms and the cuboid. The second metatarsal base is recessed proximally between the medial and lateral cuneiforms, acting as the "keystone" of the Lisfranc (tarsometatarsal) joint complex, providing immense structural rigidity to the transverse arch.
The longitudinal and transverse arches are maintained not only by the osseous configuration but also by formidable ligamentous and tendinous support. The plantar fascia, the spring ligament (calcaneonavicular ligament), and the dynamic tendinous slings of the tibialis posterior and peroneus longus are crucial for shock absorption and propulsion. Resecting a metatarsal, particularly at its base, can irrevocably compromise this stability, leading to midfoot collapse and progressive flatfoot deformity.
Neurovascular Topography
The compact nature of the foot ensures that critical neurovascular structures are in perilous proximity to the osseous and soft tissue boundaries of any oncologic resection.
On the dorsal aspect, the dorsalis pedis artery, a direct continuation of the anterior tibial artery, courses distally over the talus and navicular, giving rise to the arcuate artery and dorsal metatarsal arteries. It is superficial and vulnerable during dorsal dissections. The deep peroneal nerve accompanies the dorsalis pedis artery, providing motor innervation to the extensor digitorum brevis and critical sensory innervation to the first web space. The superficial peroneal nerve arborizes into the medial and intermediate dorsal cutaneous nerves, supplying the majority of dorsal pedal sensation.
The plantar neurovascular anatomy is significantly more complex and clinically critical. The posterior tibial artery bifurcates beneath the flexor retinaculum into the medial and lateral plantar arteries. The lateral plantar artery forms the deep plantar arch, anastomosing with the deep plantar branch of the dorsalis pedis. These vessels are vital for distal perfusion and the viability of the plantar flaps required for closure. The medial and lateral plantar nerves, branches of the tibial nerve, provide motor innervation to the intrinsic pedal musculature and sensation to the plantar skin. The common digital nerves and their terminal proper digital nerves are particularly vulnerable during web space dissection. In oncologic cases, these nerves are frequently directly involved with, or closely adherent to, the tumor pseudocapsule, mandating en bloc resection and proximal traction neurectomy to prevent debilitating postoperative neuromas.
Muscular Compartments and Intervals
The foot is divided into nine distinct anatomical compartments. Understanding these boundaries is critical for achieving compartmental resections for sarcomas. The extensor tendons (extensor digitorum longus and brevis, extensor hallucis longus) run dorsally. Plantarly, the intrinsic muscles (lumbricals, interossei, quadratus plantae, abductor hallucis, abductor digiti minimi) are layered intricately. The interossei, located between the metatarsals, are critical for toe stability and must frequently be transected proximally during a ray resection.
When harvesting a free fibular graft from the ipsilateral limb to reconstruct massive osseous defects, the surgeon utilizes the interval between the peroneus longus and soleus muscles. The common peroneal nerve courses perilously around the fibular neck, and the peroneal artery and veins are intimately associated with the posterior aspect of the fibula. Meticulous, bloodless dissection is paramount to avoid catastrophic neurovascular injury during graft harvest.
Exhaustive Indications and Contraindications
The decision to proceed with a ray resection versus a local soft tissue excision or a more proximal amputation requires a nuanced synthesis of oncologic imperatives and functional considerations. The primary directive is the preservation of life through adequate oncologic margins; functional preservation is strictly a secondary, albeit highly important, goal.
| Parameter | Indications for Ray Resection | Contraindications for Ray Resection |
|---|---|---|
| Oncologic | Primary bone sarcomas of the phalanges or distal/mid-metatarsals. | Tumors extending proximally into the tarsometatarsal (Lisfranc) joint or midfoot compartments. |
| Soft Tissue | Soft tissue sarcomas of the forefoot web spaces or individual digits where negative margins can be achieved by sacrificing the adjacent ray. | Extensive soft tissue involvement precluding primary closure or requiring massive free tissue transfer that would result in an insensate, non-durable plantar weight-bearing surface. |
| Vascular | Adequate distal perfusion (palpable pulses, biphasic/triphasic Doppler signals, ABI > 0.8) to ensure flap healing. | Severe peripheral arterial disease (PAD), non-reconstructable vascular compromise, or microvascular disease (e.g., severe diabetic angiopathy) precluding wound healing. |
| Neurologic | Intact protective sensation in the remaining plantar foot. | Severe peripheral neuropathy (e.g., Charcot arthropathy) where the altered biomechanics of a ray resection will inevitably lead to rapid, massive ulceration of the remaining foot. |
| Infection | Localized osteomyelitis or tumor-associated fungation limited to a single ray. | Spreading necrotizing fasciitis, uncontrolled deep space plantar abscesses extending into the hindfoot. |
A critical consideration is the "margin vs. function" paradigm. If achieving a wide margin necessitates the resection of the medial and lateral plantar neurovascular bundles, the resulting foot will be insensate and highly prone to ulceration, rendering a below-knee amputation a functionally superior and more durable option.
Pre-Operative Planning, Templating, and Patient Positioning
Effective preoperative planning is the blueprint for oncologic success. It is not merely a recommendation; it is an absolute mandate. The compact anatomy of the foot leaves zero margin for intraoperative improvisation regarding tumor boundaries.
Clinical Evaluation
Patients typically present with localized pain, a palpable mass, or a non-healing ulceration (in the case of fungating soft tissue sarcomas). A meticulous physical examination must document the precise anatomical location, size, mobility (fixed to bone vs. mobile within subcutaneous tissues), and consistency of the mass. The vascular examination is critical; the dorsalis pedis and posterior tibial pulses must be graded, and capillary refill assessed. Neurologic evaluation must map any sensory deficits, as tumor infiltration into the digital or plantar nerves will dictate the necessity of nerve sacrifice.
Imaging and Staging Modalities
Preoperative imaging provides the three-dimensional roadmap for the resection.
Plain radiographs (weight-bearing AP, lateral, and oblique views) are the first line of investigation. They assess osseous involvement, cortical destruction, periosteal reaction, and the presence of matrix mineralization (e.g., chondroid rings and arcs, or osteoid cloudiness).

Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard and absolutely indispensable. T1-weighted images delineate intramedullary osseous extent and marrow replacement. T2-weighted and STIR (Short Tau Inversion Recovery) sequences highlight peritumoral edema and the precise soft tissue boundaries of the mass. Axial and coronal sequences are critical for evaluating the tumor's relationship to the plantar aponeurosis, the interosseous muscular compartments, and the neurovascular bundles. The MRI dictates the exact level of the planned osteotomy and the required soft tissue margins.


Computed Tomography (CT) scans are utilized for evaluating complex cortical breaches and planning precise osteotomies, particularly when the tumor approaches the complex articulations of the midfoot. For malignant lesions, a comprehensive staging workup (CT of the chest, abdomen, and pelvis, and potentially a whole-body PET-CT or bone scan) is mandatory to rule out metastatic disease prior to definitive local control surgery.
The Biopsy Principle
A core needle biopsy or incisional biopsy is required for definitive histopathologic diagnosis and grading. The golden rule of orthopedic oncology applies strictly here: The biopsy tract must be meticulously planned so that it can be excised en bloc with the tumor specimen during the definitive resection. In the foot, this usually means placing the biopsy incision longitudinally over the involved ray, directly within the planned surgical ellipse.
Patient Positioning and OR Setup
The patient is positioned supine on a radiolucent operating table. A pneumatic thigh tourniquet is applied over generous cast padding on the ipsilateral limb. Exsanguination with an Esmarch bandage is strictly contraindicated in oncologic cases to prevent the theoretical risk of proximal tumor embolization; instead, the limb is elevated for 3-5 minutes prior to tourniquet inflation.
A small bump is placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral, perfectly vertical alignment. The C-arm fluoroscopy unit must be positioned to enter from the contralateral side, allowing for unimpeded AP, lateral, and oblique imaging to confirm osteotomy levels and hardware placement. The limb is prepped with a standard chlorhexidine or povidone-iodine solution from the mid-thigh to the toes, ensuring the entire foot and ankle are freely mobile within the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a ray resection demands meticulous soft tissue handling, precise osteotomies, and a profound respect for the remaining neurovascular structures. The following details the approach for a central ray resection, which serves as the foundational technique, with specific modifications noted for the border rays.
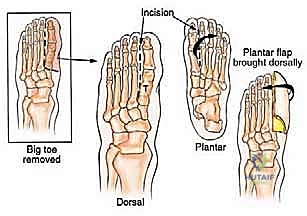
Incision Planning and Flap Elevation
The incision is typically a racket-shaped or elliptical design. A dorsal longitudinal incision is marked directly over the involved metatarsal, extending from the planned level of the proximal osteotomy distally to the MTP joint. At the level of the web spaces, the incision bifurcates and curves plantarly to encompass the base of the involved digit.
Crucially, the plantar incision must be designed to preserve a robust, full-thickness plantar flap. The plantar skin is uniquely adapted for weight-bearing, characterized by thick stratum corneum and specialized septated fat pads. Dorsal skin cannot tolerate plantar pressures; therefore, the closure line must be positioned dorsally, pulling the plantar flap upwards.
Using a #10 scalpel, the skin and subcutaneous tissues are incised sharply down to the deep fascia. Electrocautery is used judiciously to maintain a bloodless field, but thermal necrosis of the skin edges must be strictly avoided. The dorsal veins are ligated and divided. The extensor tendons to the involved ray (extensor digitorum longus and brevis) are identified, tagged, and transected proximally, allowing them to retract out of the surgical field.
Deep Dissection and Neurovascular Management
The dissection proceeds into the intermetatarsal spaces adjacent to the involved ray. The dorsal and plantar interosseous muscles are elevated off the adjacent, healthy metatarsals using a periosteal elevator or electrocautery, taking care to leave the muscle bellies attached to the tumor-bearing metatarsal to serve as a soft tissue margin.
At the level of the web spaces, the deep transverse metatarsal ligament must be identified and sharply divided on both sides of the involved ray. This is a critical step that mobilizes the metatarsal head.
Neurovascular management is paramount. The common digital arteries and nerves supplying the involved web spaces are identified. The vessels are meticulously ligated with non-absorbable suture or surgical clips. The nerves require special attention to prevent postoperative neuroma formation. The involved digital nerves are isolated, placed under gentle distal traction, and transected sharply with a fresh scalpel blade as far proximally as possible. The proximal stump is allowed to retract deep into the intrinsic muscle bellies, away from the weight-bearing surface and the surgical scar.
The Osteotomy and Specimen Extraction
Once the soft tissue attachments are released, attention is turned to the bone cut. Based on preoperative MRI templating, the exact level of the metatarsal osteotomy is identified. In oncologic resections, a margin of at least 1-2 cm of normal marrow is typically desired.
The periosteum is incised circumferentially at the osteotomy site. A sagittal saw is used to perform the osteotomy. The cut should be beveled from dorsal-proximal to plantar-distal. This critical technical nuance ensures that the remaining plantar cortex is shorter than the dorsal cortex, preventing a sharp, prominent bony spike from impinging on the plantar skin during weight-bearing, which would inevitably lead to ulceration.
If the entire ray must be resected, the osteotomy is replaced by a disarticulation at the tarsometatarsal (Lisfranc) joint. The capsule and supporting ligaments are sharply incised, and the metatarsal base is levered out of its articulation.
Once the osteotomy or disarticulation is complete, the entire ray—comprising the digit, the metatarsal, the attached intrinsic musculature, and the biopsy tract—is removed en bloc. The specimen is immediately oriented with sutures for the pathologist to evaluate the margins.
Soft Tissue Reconstruction and Closure
Following copious irrigation of the tumor bed with normal saline, hemostasis is meticulously achieved. The tourniquet is deflated to identify and control any bleeding vessels.
Reconstruction focuses on obliterating the dead space and restoring forefoot stability. For central ray resections, the remaining adjacent metatarsals are approximated. Heavy, absorbable sutures (e.g., #1 or #0 Vicryl) are placed through the capsules of the adjacent MTP joints and the remnants of the deep transverse metatarsal ligament. Tying these sutures effectively closes the surgically created cleft, narrowing the forefoot and preventing splaying of the remaining digits.
Myodesis is performed by suturing the remaining intrinsic muscle bellies and the transected extensor/flexor tendons over the beveled end of the metatarsal stump. This provides a dynamic soft tissue cushion over the bone.
Closure is performed in multiple layers. The deep subcutaneous layer is closed with interrupted absorbable sutures, ensuring no tension is placed on the skin edges. The skin is closed with non-absorbable monofilament sutures (e.g., 3-0 or 4-0 Nylon) using a vertical mattress technique to evert the edges and maximize the healing surface area. A closed suction drain may be placed if significant dead space remains, though it is often avoided in the foot if hemostasis is excellent.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, foot amputations for oncologic conditions carry a significant risk of complications due to the tenuous vascularity, lack of redundant soft tissue, and the immense biomechanical demands placed on the extremity postoperatively.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage Management and Mitigation |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 15% - 25% | Tension on closure, inadequate plantar flap, peripheral vascular disease, smoking, prior radiation therapy. | Aggressive local wound care, judicious debridement of necrotic edges. Utilization of incisional Negative Pressure Wound Therapy (iNPWT) immediately post-op. May require split-thickness skin grafting or local rotational flaps if deep structures are exposed. |
| Symptomatic Neuroma | 10% - 20% | Inadequate proximal retraction of transected digital or plantar nerves; entrapment of nerve stump in scar tissue. | Prevention via traction neurectomy is key. Management includes targeted corticosteroid injections, custom orthotics with offloading pads. Surgical excision and implantation of the nerve stump into deep muscle or bone is indicated for refractory cases. |
| Transfer Metatarsalgia | 30% - 50% (High in 1st/5th ray resections) | Altered biomechanics; loss of primary weight-bearing struts forces lesser metatarsals to bear excessive loads. | Custom orthotics with metatarsal bars or pads to redistribute pressure. Rocker-bottom shoe modifications. In severe, recalcitrant cases, prophylactic osteotomies of the overloaded lesser metatarsals may be required. |
| Deep Infection / Osteomyelitis | 5% - 10% | Contiguous spread from superficial wound breakdown, hematoma formation, immunocompromised state (chemotherapy). | Broad-spectrum intravenous antibiotics tailored to intraoperative cultures. Aggressive surgical debridement of infected bone and soft tissue. Hardware removal if applicable. May necessitate revision to a more proximal amputation level. |
| Local Oncologic Recurrence | 5% - 15% (Depends on tumor histology and margins) | Inadequate surgical margins, microscopic satellite lesions, highly aggressive tumor biology (e.g., synovial sarcoma). | Requires comprehensive restaging. Treatment usually mandates a radical proximal amputation (e.g., Below-Knee Amputation) to achieve definitive local control, often combined with adjuvant radiotherapy or chemotherapy. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a ray resection is a protracted process that requires a multidisciplinary approach involving the orthopaedic surgeon, physical therapist, and orthotist. The protocol is strictly phased to protect the surgical repair while progressively restoring function.
Phase I: Maximum Protection and Tissue Healing (Weeks 0-3)
Immediately postoperatively, the foot is placed in a bulky, well-padded, non-weight-bearing splint. The primary goals in this phase are edema control, wound healing, and pain management. Strict non-weight-bearing (NWB) status is enforced using crutches or a knee scooter. The limb must be elevated above the level of the heart whenever the patient is resting. Sutures are typically left in place longer in the foot than in other areas, usually removed between 14 and 21 days, contingent upon complete epithelialization of the incision line.
Phase II: Progressive Mobilization and Early Weight-Bearing (Weeks 3-6)
Once the incision is fully healed and sutures are removed, the patient is transitioned into a rigid Controlled Ankle Motion (CAM) walker boot. Weight-bearing is initiated gradually, starting with touch-down weight-bearing (TDWB) and advancing to weight-bearing as tolerated (WBAT) over the course of several weeks. Physical therapy focuses on active and passive range of motion of the ankle and the remaining unoperated digits to prevent stiffness and tendon adhesions. Desensitization techniques for the stump are initiated to prepare the skin for custom footwear.
Phase III: Orthotic Integration and Functional Restoration (Weeks 6-12+)
This phase marks the transition out of the CAM boot and into definitive footwear. An orthotist evaluates the patient for a custom-molded total contact insert. For central ray resections, a custom toe filler is fabricated to prevent the adjacent digits from drifting into the surgical void. For first ray resections, a rigid carbon fiber footplate with a Morton's extension is often utilized to substitute for the lost medial column lever arm and to protect the lesser metatarsals from excessive bending moments. Gait training is paramount to correct compensatory antalgic patterns and ensure a fluid, energy-efficient stride.
Summary of Landmark Literature and Clinical Guidelines
The surgical philosophy surrounding pedal amputations for oncologic conditions has evolved significantly, driven by advancements in imaging and a deeper understanding of foot biomechanics.
Historically, the paradigm favored radical proximal amputations (e.g., Syme or BKA) for almost all malignant foot lesions to guarantee oncologic clearance. However, landmark studies in the late 20th and early 21st centuries demonstrated that limb-sparing ray resections, when combined with
