Anterior Flap Hemipelvectomy: A Masterclass in Oncologic Reconstruction
Key Takeaway
Welcome to an advanced surgical masterclass on anterior flap hemipelvectomy. We'll meticulously navigate this complex oncologic procedure, designed for extensive posterior pelvic and buttock sarcomas. This guide covers detailed anatomy, precise intraoperative execution, critical pearls to avoid pitfalls, and comprehensive postoperative management, ensuring optimal patient outcomes and reconstructive success using the robust anterior myocutaneous thigh flap.
Comprehensive Introduction and Patho-Epidemiology
The anterior flap hemipelvectomy represents one of the most formidable, challenging, and ultimately rewarding surgical endeavors within the domain of oncologic orthopaedics. This procedure is a radical, life-saving hindquarter amputation reserved for clinical scenarios where precision, exhaustive anatomical mastery, and meticulous multidisciplinary planning are absolutely paramount. We are typically intervening in patients presenting with massive, locally aggressive soft tissue sarcomas of the gluteal region or primary bone sarcomas of the pelvis that exhibit extensive posterior extension. Historically, many of these extensive tumors were deemed unresectable or incurable by traditional posterior flap hemipelvectomy techniques due to the high risk of intralesional margins or catastrophic flap failure. The primary surgical objective extends far beyond mere tumor extirpation; it necessitates the creation of a robust, functional, and durable reconstruction utilizing a massive vascularized myocutaneous flap harvested from the anterior thigh.
The patho-epidemiology of tumors necessitating this radical approach is predominantly characterized by high-grade sarcomas, including chondrosarcoma, osteosarcoma, Ewing sarcoma, and massive pleomorphic soft tissue sarcomas. These malignancies often arise insidiously within the capacious gluteal compartment or the deep pelvic basin, allowing them to achieve significant volume before clinical detection. By the time of diagnosis, the tumor has frequently invaded or severely contaminated the posterior buttock skin, the sacrum, or the critical neurovascular structures traversing the greater sciatic notch. In such advanced presentations, the classic posterior flap—which relies heavily on the gluteal musculature and overlying integument for closure—is oncologically compromised and anatomically unavailable. Attempting to utilize a posterior flap in the presence of posterior tumor extension invariably leads to positive margins, rapid local recurrence, and dismal patient survival.
Understanding the philosophy behind the anterior flap modification is critical for the operating surgeon. When the tumor dictates that the posterior tissues must be sacrificed en bloc with the hemipelvis, we must look anteriorly for our reconstructive tissue bank. We engineer a massive, full-thickness myocutaneous flap derived from the anterior thigh, pedicled reliably on the superficial femoral artery (SFA) and its accompanying venous system. This anteriorly based flap provides a voluminous, exceptionally well-vascularized tissue mass capable of rotating superiorly and posteriorly. It is uniquely suited for obliterating massive posterior pelvic defects, providing a durable biological barrier over the exposed peritoneal sac, enhancing postoperative cosmesis, and crucially, creating a robust soft-tissue envelope that facilitates eventual prosthetic fitting.
Furthermore, the anterior flap hemipelvectomy offers profound oncologic advantages in the era of multimodal therapy. Because the flap is harvested from a region anatomically distant from the primary posterior tumor bed, it permits a much more aggressive and extensive posterior resection, ensuring wide, negative (R0) margins. Postoperatively, this well-vascularized anterior tissue demonstrates superior tolerance to adjuvant or neoadjuvant radiation therapy. Unlike irradiated posterior flaps, which are notoriously prone to ischemic necrosis, dehiscence, and chronic wound complications, the SFA-pedicled anterior flap maintains its integrity, allowing oncologists to deliver tumoricidal radiation doses without catastrophic soft-tissue failure.
Detailed Surgical Anatomy and Biomechanics
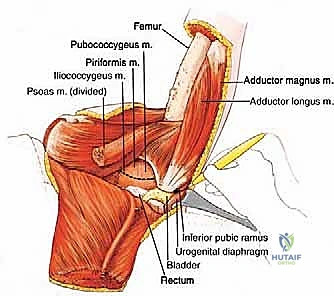
Before a scalpel is even considered, a profound, three-dimensional understanding of pelvic and lower extremity anatomy is your greatest asset. The osteology of the region dictates the boundaries of our resection. We are manipulating the entire hemipelvic ring, encompassing the iliac crest, the sacrum, the pubic symphysis, the sacroiliac (SI) joint, and the greater and lesser sciatic notches. The amputation inherently destabilizes the pelvic ring, proceeding typically through the sacroiliac joint (or adjacent sacral ala) posteriorly and the pubic symphysis anteriorly. Understanding the biomechanical implications of this osseous disruption is vital, not for skeletal reconstruction—as the limb is amputated—but for understanding the subsequent forces on the remaining core musculature and the requirements for sitting balance post-resection.
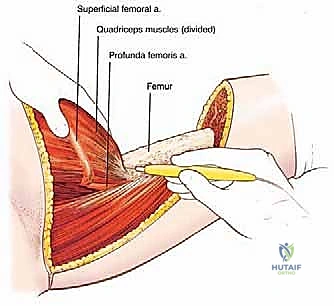
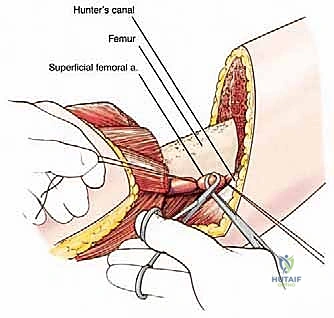
The neurovascular anatomy of the femoral triangle is the absolute crux of flap survival. As the external iliac vessels pass deep to the inguinal ligament, they transition into the common femoral vessels. Surgeons must be acutely aware of a variable, single arterial branch supplying the iliac crest that often arises from the medial aspect of the external iliac artery just proximal to the ligament; inadvertent avulsion of this branch can lead to brisk, challenging retroperitoneal hemorrhage. Distally, the superficial femoral vessels travel deep to the sartorius muscle, coursing through the adductor canal to eventually become the popliteal vessels. Our primary objective is the meticulous preservation of the common and superficial femoral vessels, as they constitute the indispensable vascular pedicle for the entire anterior myocutaneous flap.

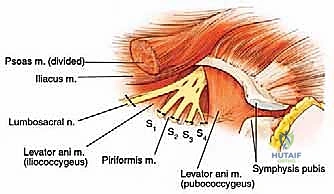
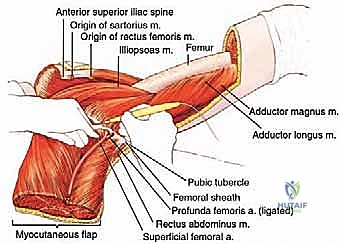
The most critical vascular maneuver in this procedure involves the profunda femoris artery. Arising from the posterolateral aspect of the common femoral or proximal superficial femoral artery, the profunda dives deep to supply the posterior thigh. Ligation and division of the profunda femoris are absolutely mandatory to mobilize and elevate the anterior flap. Failure to adequately secure this vessel will tether the flap and result in catastrophic hemorrhage during elevation. Neurovascularly, the femoral nerve, lying lateral to the artery, must be identified and protected during the initial flap elevation, while the sciatic nerve posteriorly will be a primary resection target if encased by tumor, or meticulously preserved if oncologically safe—though preservation is exceedingly rare in the context of a classic hemipelvectomy.
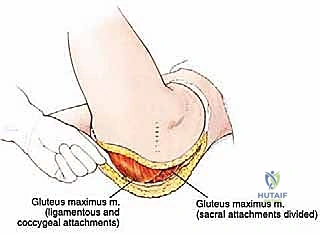
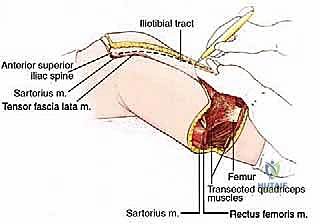
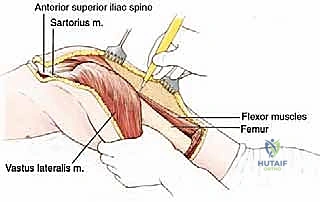
The muscular anatomy defines both our reconstructive assets and our resection targets. The anterior flap is composed of the robust quadriceps femoris group (rectus femoris, vastus lateralis, vastus medialis, vastus intermedius) and the sartorius muscle. These muscles receive their primary perfusion via direct branches and perforators from the SFA. Meticulous dissection is required when elevating the vastus lateralis, as substantial perforating branches from the ligated profunda femoris will be encountered and must be individually ligated to ensure absolute hemostasis. Conversely, the resection targets include the entire gluteal complex (maximus, medius, minimus), the tensor fascia lata (which is separated from its investing fascia and left with the specimen), and the insertions of the core musculature. The erector spinae, latissimus dorsi, quadratus lumborum, and the abdominal obliques must be sharply incised directly at their osseous attachments to the sacrum and iliac crest to mobilize the hemipelvis.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in radical pelvic oncology. The anterior flap hemipelvectomy is a procedure of sheer magnitude, and its application must be governed by strict, evidence-based indications. Primarily, it is indicated for patients harboring massive primary bone or soft tissue sarcomas involving the buttock, posterior ilium, or sciatic notch that are entirely unamenable to limb-sparing resections. These are tumors where achieving a negative margin necessitates the en bloc sacrifice of the hemipelvis and the entirety of the posterior soft tissue envelope. Additionally, patients who have experienced catastrophic local recurrences following previous failed attempts at limb-salvage surgery—often compounded by the fibrotic and ischemic effects of prior high-dose radiation therapy—are prime candidates for this definitive, albeit radical, surgical salvage.
Beyond primary oncologic diagnoses, there exists a narrow but critical subset of non-oncologic indications. Selected paraplegic or tetraplegic patients suffering from intractable, recalcitrant chronic osteomyelitis of the hemipelvis or proximal femur may require this procedure. In cases of uncontrollable, life-threatening pelvic sepsis originating from massive, deep-seated sacral or trochanteric decubitus ulcers that have destroyed the hip joint and pelvic bone, an anterior flap hemipelvectomy can be a life-saving, source-control intervention. By removing the infected bone and utilizing the pristine, vascularized anterior thigh tissue to obliterate the massive dead space, surgeons can cure otherwise fatal pelvic sepsis.
However, the contraindications are equally, if not more, important to respect. Absolute contraindications include the presence of uncontrolled, widely disseminated systemic metastasis where the surgical morbidity would far outweigh any palliative benefit. Anatomically, tumor extension into the spinal canal, gross invasion of the central sacral canal, or bilateral sacral involvement precludes this procedure, as achieving an R0 margin would require destabilizing the spinopelvic junction to an incompatible degree. Furthermore, severe, uncorrectable peripheral vascular disease is a strict contraindication. If preoperative angiography reveals critical stenosis or complete occlusion of the common or superficial femoral arteries, the anterior flap will inevitably undergo ischemic necrosis, rendering the procedure a catastrophic failure.
| Clinical Parameter | Indications for Anterior Flap Hemipelvectomy | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Oncologic Status | Massive gluteal/posterior pelvic sarcomas; Failed limb salvage; Fungating posterior tumors. | Uncontrolled systemic metastasis; Tumor invading spinal cord/dura. | Advanced age with significant frailty; Poor expected overall survival. |
| Anatomical Extent | Tumor involvement of sciatic notch, sacrum (unilateral), or extensive posterior skin. | Bilateral sacral invasion; Central spinal canal involvement. | Tumor approaching the anterior thigh flap donor site. |
| Vascular Health | Patent Common and Superficial Femoral Arteries confirmed on angiography. | Occlusion/severe stenosis of the SFA or Common Femoral Artery. | Heavy smoking history (requires strict cessation and vascular mapping). |
| Non-Oncologic | Intractable pelvic osteomyelitis in paraplegia; Massive infected decubitus ulcers. | Active, uncorrected coagulopathy; Severe cardiopulmonary instability. | Severe malnutrition (must be optimized preoperatively). |
Pre-Operative Planning, Templating, and Patient Positioning
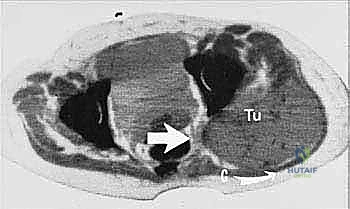
The battle of an anterior flap hemipelvectomy is frequently won or lost in the preoperative planning phase. Non-negotiable, high-resolution imaging is the foundation of this preparation. Beyond standard orthogonal radiographs, multi-planar, contrast-enhanced Magnetic Resonance Imaging (MRI) is essential to precisely delineate the soft tissue extent of the sarcoma, particularly assessing intrapelvic extension, involvement of the neurovascular bundle at the sciatic notch, and the exact margins of the gluteal musculature. Computed Tomography (CT) mapping is equally critical for defining the extent of cortical bone destruction and planning the precise trajectory of the sacral and pubic osteotomies.
Crucially, angiography of the femoral vessels is an absolute, uncompromising requirement for any patient slated for an anterior flap hemipelvectomy. We must definitively assess the patency, caliber, and health of the superficial femoral artery. In elderly patients, diabetics, or individuals with a history of tobacco use, silent atherosclerotic disease can compromise the SFA. If the primary pedicle is diseased, the massive anterior flap will fail, leading to devastating necrotic complications. Angiography also assists in visualizing the internal iliac and pelvic collateral vessels, ensuring they are not pathologically engorged or directly encased by the tumor, which could alter the approach to hemostasis during the intrapelvic dissection.
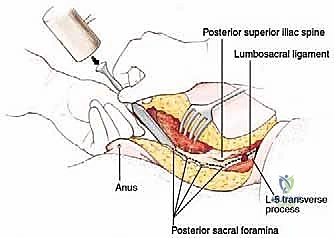
Preoperative physiological optimization and specific protocols are rigorous. We anticipate massive, rapid blood loss; therefore, a massive transfusion protocol must be activated, with adequate units of packed red blood cells, fresh frozen plasma, and platelets cross-matched and physically present in the operating room. A complete mechanical and antibiotic bowel preparation is mandatory to minimize the catastrophic risk of fecal contamination during the deep posterior and perineal dissection phases. In female patients, a thorough vaginal preparation is also performed. On the morning of surgery, a critical, often-overlooked step is the physical closure of the anus. The anus must be sutured shut with a heavy purse-string suture to absolutely prevent intraoperative fecal spillage—a simple maneuver that profoundly reduces postoperative deep pelvic sepsis.

Patient positioning requires meticulous attention to detail and is a dynamic process. While initial central line placement and potential anterior vascular control may begin supine, the primary operative position is the lateral decubitus position. The patient is carefully rolled, ensuring the iliac crest of the affected, operative side is positioned exactly over the mechanical flexion point (the "break") of the operating table. This strategic alignment allows the surgeon to flex the table mid-procedure, effectively opening the angle between the iliac wing and the lumbar vertebrae, dramatically improving access to the deep pelvic basin and the sacroiliac junction.
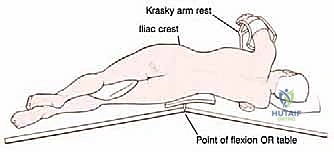
Extensive padding is utilized to prevent pressure neuropraxias and decubitus ulcers during this prolonged case. A gel pad or cushion is placed beneath the contralateral down-side iliac crest and greater trochanter. An axillary roll is mandatory beneath the dependent axilla to allow unhindered chest wall excursion for ventilation and to protect the brachial plexus from traction injury. The dependent arm is secured on a well-padded Krasky armrest. To mitigate the high risk of deep vein thrombosis (DVT) during the lengthy procedure, sequential compression devices and elastic support stockings are applied to the contralateral lower extremity. The operative limb is prepped and draped entirely free, circumferentially from the toes up to the costal margin, allowing the surgical team uninhibited manipulation of the leg to facilitate dissection and optimize tension during flap elevation.
Step-by-Step Surgical Approach and Flap Elevation
Incision Design and Initial Exposure
The execution of the anterior flap hemipelvectomy begins with the meticulous geometric mapping of the incisions. The viability of the reconstruction depends entirely on designing an anterior myocutaneous flap of sufficient length and width to comfortably obliterate the massive posterior and lateral defect without placing the vascular pedicle under tension. Using a sterile marking pen, the anterior flap is drawn, encompassing a vast territory of anterior thigh skin, the thick subcutaneous adipose layer, and the underlying quadriceps muscle complex.
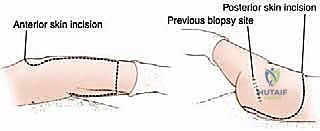
The distal boundary is defined by a transverse incision positioned several inches proximal to the superior pole of the patella. The exact level is determined by measuring the anticipated defect; the tip of this flap must ultimately reach the posterior iliac crest and sacrum after rotation. The medial limb of the incision begins 2 to 3 cm lateral to the surgically closed anus, coursing anteriorly through the gluteal crease toward the pubic tubercle, and then extending distally along the medial aspect of the thigh. It is critical to place this medial incision lateral to the sartorius muscle initially, facilitating direct access to the femoral triangle and the superficial femoral vessels.
The lateral limb of the incision mirrors the medial, starting posteriorly, paralleling the superior border of the iliac crest, passing over the anterior superior iliac spine (ASIS), and continuing distally down the lateral midline of the thigh to intersect the transverse incision. Once the skin and subcutaneous tissues are incised, the immediate priority is securing the vascular pedicle. The medial dissection is deepened to expose the femoral triangle. The common femoral artery and vein are identified, looped with vessel loops, and traced distally. The critical maneuver here is the positive identification, double-ligation, and transection of the profunda femoris artery and vein. This releases the deep tethering of the anterior thigh tissues, allowing the superficial femoral vessels to remain in continuity with the elevating flap.
Pelvic Dissection and Osteotomies
With the anterior flap mobilized distally and its vascular pedicle secured, the focus shifts to the abdominal and pelvic dissection. The abdominal wall musculature—comprising the external oblique, internal oblique, and transversus abdominis—must be sharply detached from the superior lip of the iliac crest. This dissection is carried down to the bone, carefully sweeping the peritoneum medially to avoid enterotomy.
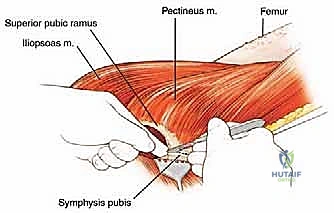
As the retroperitoneal space is entered, the ureter is identified and gently retracted medially with the peritoneal sac. The dissection proceeds anteriorly toward the pubic symphysis. The spermatic cord in males, or the round ligament in females, is identified and preserved if oncologically feasible, or sacrificed if necessary for margins. The bladder is carefully mobilized off the posterior aspect of the pubis. A Gigli saw or an osteotome is then utilized to divide the pubic symphysis precisely at the midline, or slightly contralateral to the midline if required for wider anterior margins.
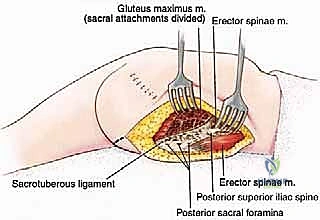
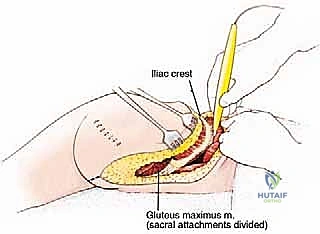
Attention is then directed posteriorly. The patient's position on the flexed operating table is maximized to expose the posterior ilium and sacrum. The massive paraspinal muscles—the erector spinae, multifidus, and quadratus lumborum—are sharply transected at their attachments to the iliac crest and sacrum. The plane of dissection here must remain strictly extra-lesional, ensuring a thick cuff of normal tissue remains over any posterior tumor extension.
The sacroiliac joint is identified. Depending on the preoperative templating, the posterior osteotomy is performed either straight through the SI joint using osteotomes, or more commonly, through the sacral ala using a combination of a Gigli saw and osteotomes to ensure a wider margin. During this phase, the massive sacrotuberous and sacrospinous ligaments are identified and sharply divided. The sciatic nerve is visualized as it exits the greater sciatic foramen; if the tumor involves the notch, the nerve is sharply transected as high as possible.
Specimen Delivery and Flap Inset
With the anterior and posterior osteotomies complete, the hemipelvis is highly mobile. The remaining soft tissue attachments, primarily the pelvic floor musculature (levator ani, coccygeus) and the internal iliac vessels (which must be securely ligated), are systematically divided. The entire lower extremity, hemipelvis, and the encompassing tumor mass are delivered en bloc from the surgical field.
The resultant defect is an immense, cavernous void exposing the retroperitoneum, the bladder, and the raw surfaces of the sacral osteotomy. Meticulous, exhaustive hemostasis is performed using electrocautery, argon beam coagulation, and hemostatic agents. The massive raw surface area is prone to significant postoperative oozing, making this step critical for preventing expanding hematomas.
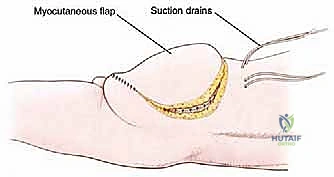
The previously elevated anterior myocutaneous flap is now rotated superiorly and posteriorly to fill the defect. The perfusion of the
Clinical & Radiographic Imaging Archive