Advanced Surgical Techniques in Upper Extremity Limb Salvage: Shoulder Girdle and Humerus
Key Takeaway
Upper extremity limb salvage prioritizes functional preservation over amputation, even when major nerves are sacrificed. This guide details advanced oncologic resections, including the Tikhoff-Linberg procedure, scapulectomy, and proximal humerus resections. Utilizing the Malawer classification, surgeons can achieve precise oncologic margins while optimizing biomechanical reconstruction using modular megaprostheses, allograft-prosthetic composites, or noninvasive expandable implants for pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
In contrast to the lower extremity, where modern prosthetics can closely mimic the biomechanics of the native limb through advanced microprocessor-controlled joints and energy-storing carbon fiber components, even the most advanced artificial limb fails to provide comparable function in the upper extremity. The upper extremity is uniquely adapted for prehension, fine motor dexterity, and positioning the hand in three-dimensional space. The lack of sensory feedback, fine motor control, and spatial proprioception makes upper extremity amputation a profoundly disabling procedure that severely impacts a patient's independence and psychological well-being. Consequently, modern imaging, neoadjuvant chemoradiation protocols, and advanced surgical techniques prioritize limb salvage in almost all oncologic circumstances involving the shoulder girdle and humerus. The evolution from routine forequarter amputation to sophisticated limb-sparing resections represents one of the most significant triumphs in modern orthopedic oncology.
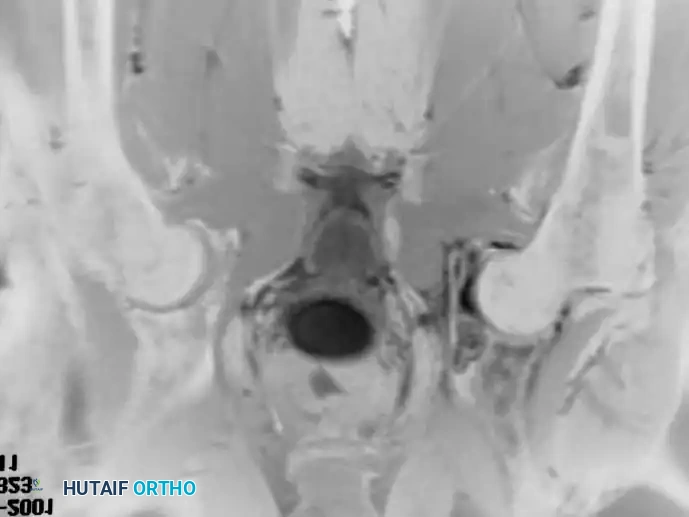
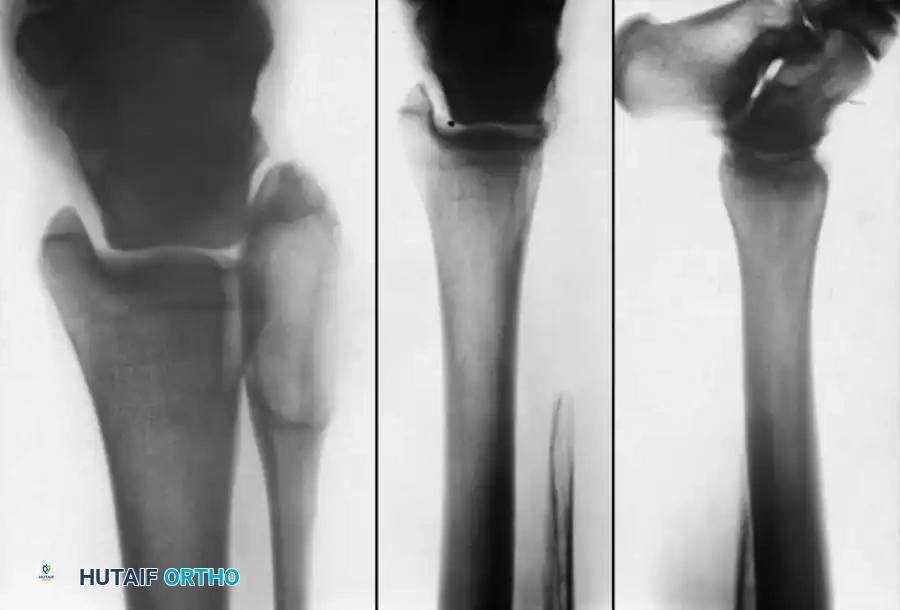
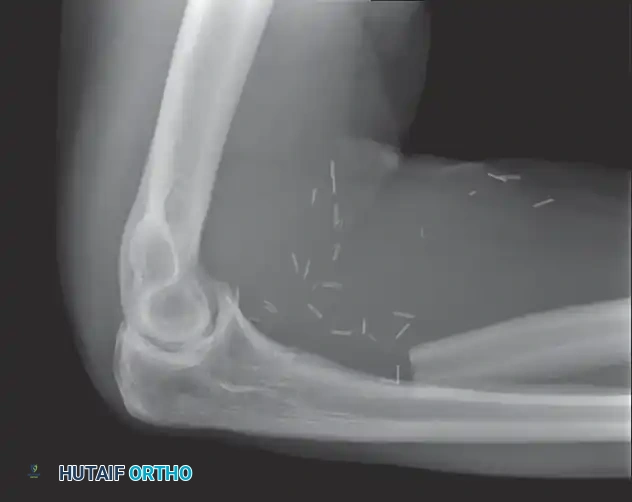
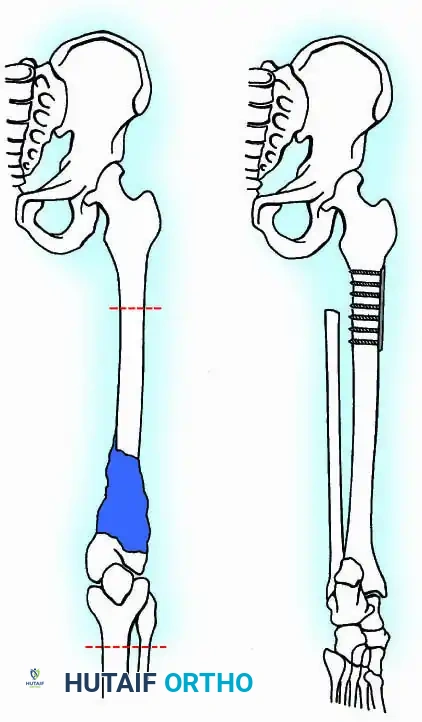
Primary bone and soft tissue sarcomas of the upper extremity, while less common than their lower extremity counterparts, present formidable reconstructive challenges due to the dense concentration of critical neurovascular structures within a confined anatomical space. The proximal humerus is the third most common site for primary osteosarcoma and Ewing sarcoma, and it is a frequent site for metastatic deposition from renal, thyroid, breast, and lung carcinomas. Patho-epidemiologically, these lesions often expand rapidly, breaching the thin cortical bone of the proximal humerus and infiltrating the surrounding muscular compartments. Resections of the proximal humerus frequently require the sacrifice of the axillary nerve, and resections of the humeral shaft frequently necessitate the sacrifice of the radial nerve. Remarkably, even with the sacrifice of up to three major nerves, limb salvage usually provides superior functional outcomes compared to an artificial limb. If the median or ulnar nerve must be sacrificed, limb salvage may still be highly worthwhile provided that functioning muscles are available for tendon transfers to restore grip and pinch.
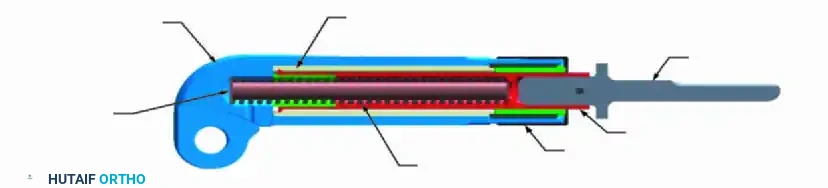


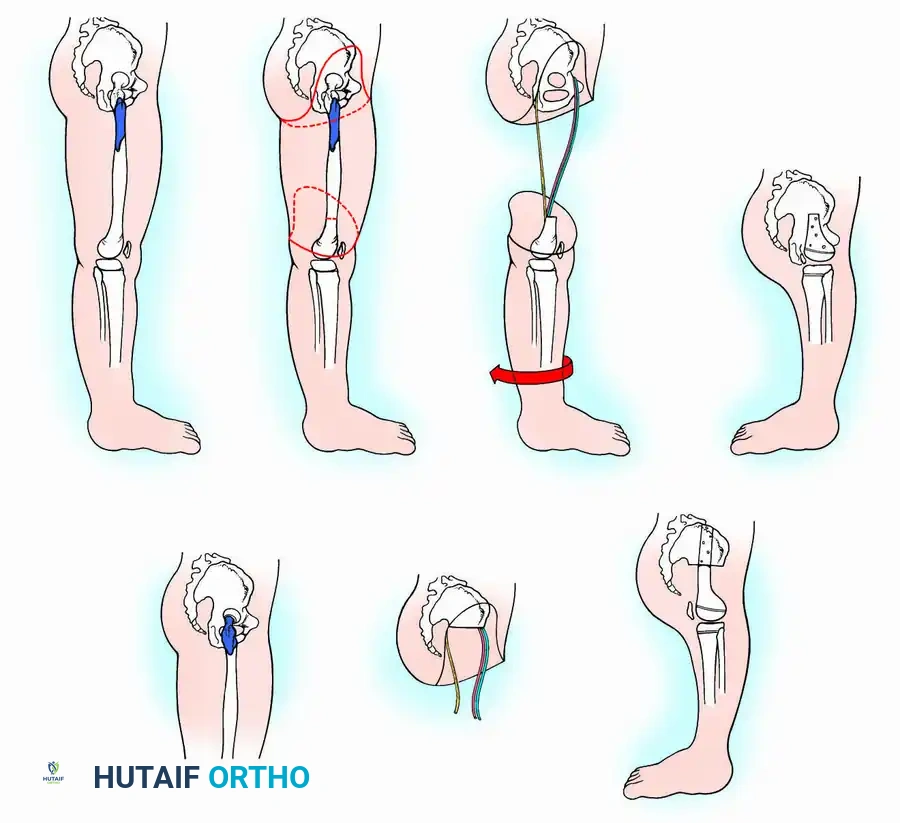
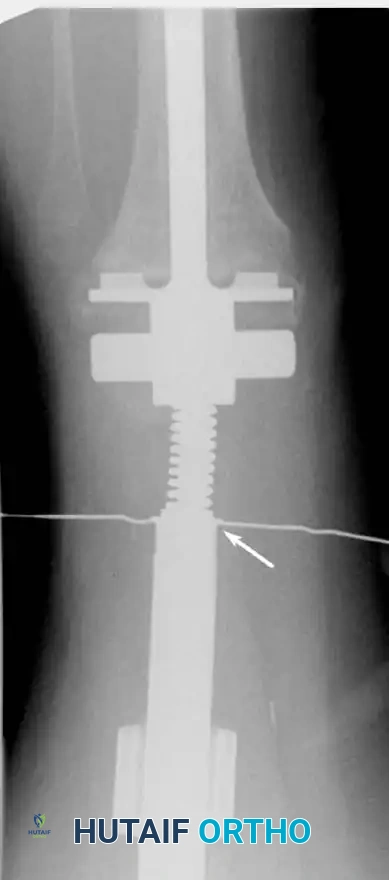
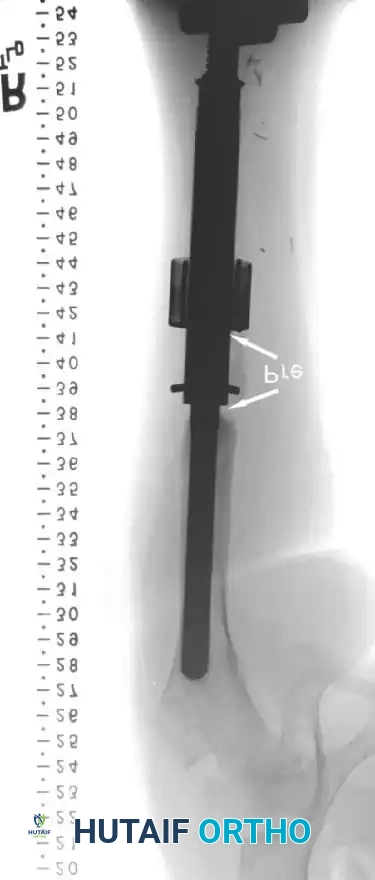
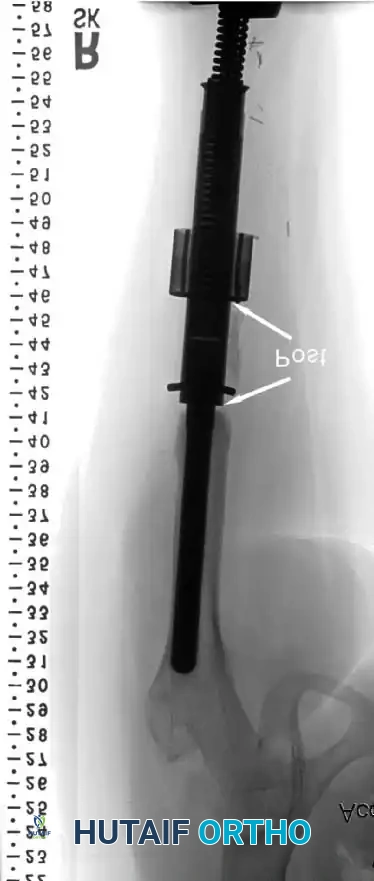
In skeletally immature patients requiring massive bone resection for osteosarcoma or Ewing sarcoma, limb length discrepancy is a major postoperative complication that historically necessitated multiple morbid open lengthening procedures or resulted in severe functional asymmetry. The development of noninvasive expandable prostheses, such as the Repiphysis system, has revolutionized pediatric limb salvage. These devices utilize an electromagnetic field to release a locking mechanism within the prosthesis, allowing a compressed spring to expand the tubular housing. This permits incremental lengthening in the outpatient clinic without the need for repeated surgical interventions. The lengthening process is meticulously controlled: the locking mechanism is located via palpation or fluoroscopy, the patient’s limb is marked at the exact site of the internal mechanism, and an electromagnetic coil is placed circumferentially around the limb. The device is activated, generating a field that releases the internal spring, and pre-expansion and post-expansion radiographs are obtained to quantify the exact lengthening achieved.



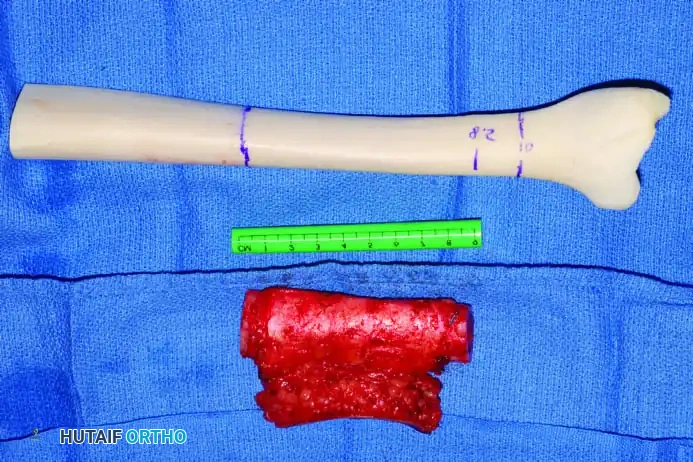
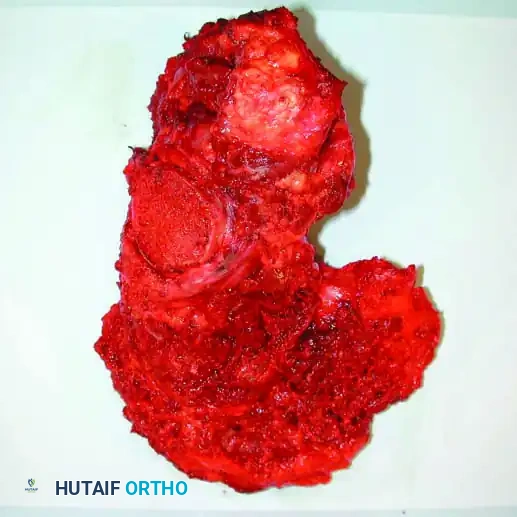
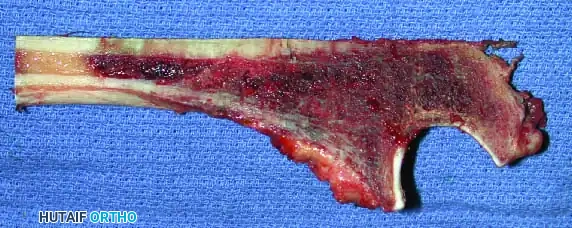
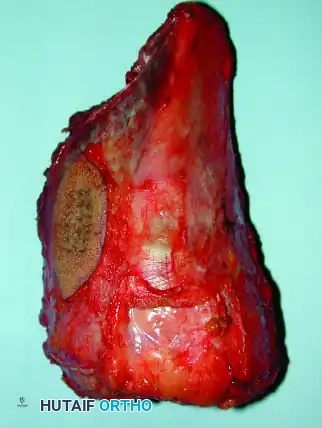
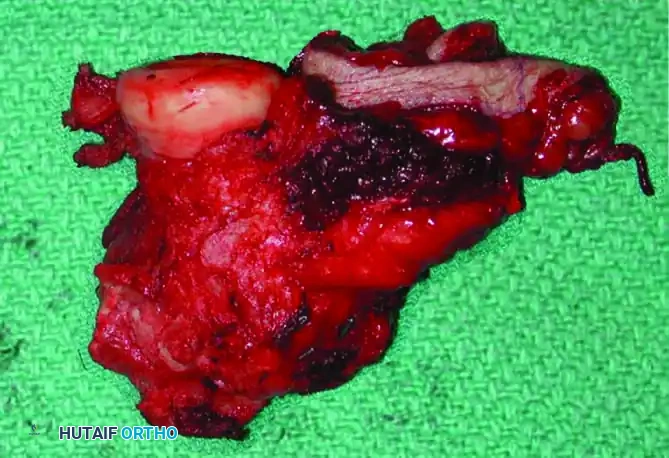
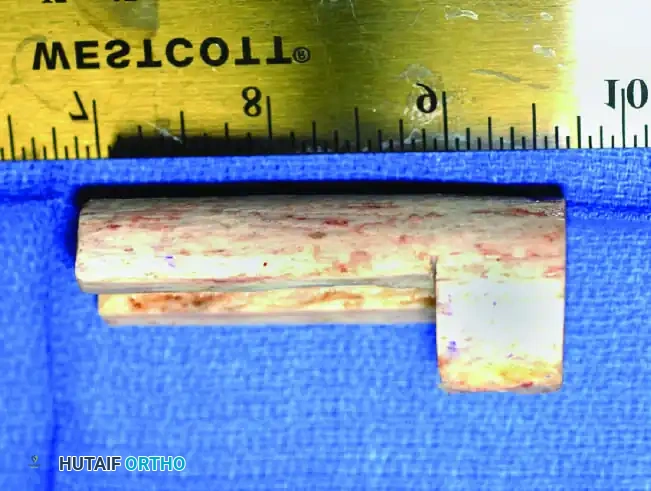
The patho-epidemiology of these tumors dictates that surgical margins must be meticulously planned. High-grade sarcomas exhibit a pseudocapsule composed of compressed tumor cells and reactive tissue, surrounded by a reactive zone containing microscopic satellite lesions. Inadequate resection through this reactive zone inevitably leads to local recurrence, which in the upper extremity often precludes further salvage attempts and necessitates morbid amputations. Therefore, an exhaustive understanding of tumor biology, compartmental anatomy, and advanced reconstructive options is mandatory for the orthopedic oncologist undertaking these complex procedures.


Detailed Surgical Anatomy and Biomechanics
The shoulder girdle is a complex functional syncytium comprising the sternoclavicular, acromioclavicular, glenohumeral, and scapulothoracic articulations. The biomechanical stability of the upper extremity relies heavily on the dynamic suspension provided by the periscapular musculature rather than intrinsic bony congruity. Tumors of the scapula are frequently complicated by extension into the glenohumeral joint, necessitating extra-articular resection of the humeral head en bloc with the scapula. The subscapularis muscle often provides a robust anatomical barrier, protecting tumors of the anterior scapula from direct chest wall invasion until late in the disease process. Conversely, the long head of the biceps tendon provides a direct anatomical passageway for tumors of the proximal humerus to extend into the joint, often requiring an extra-articular partial scapulectomy to achieve wide oncologic margins.


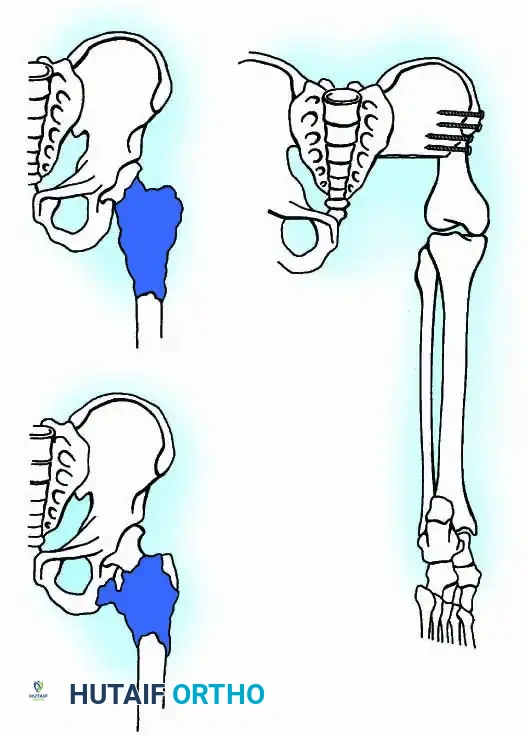
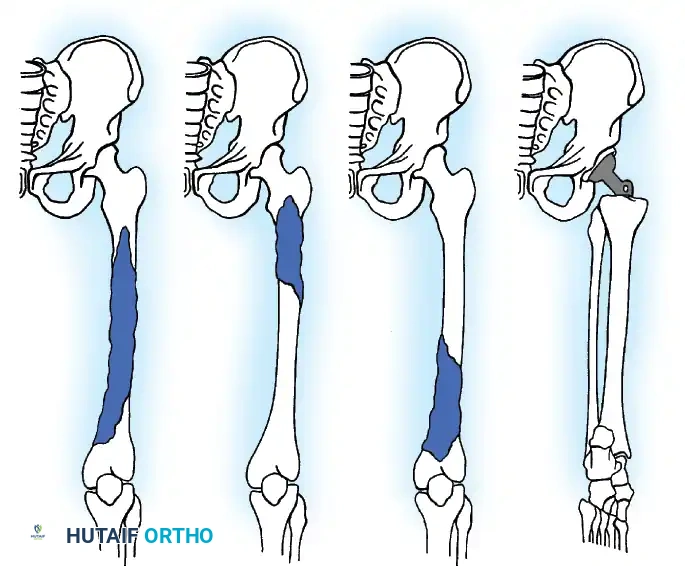
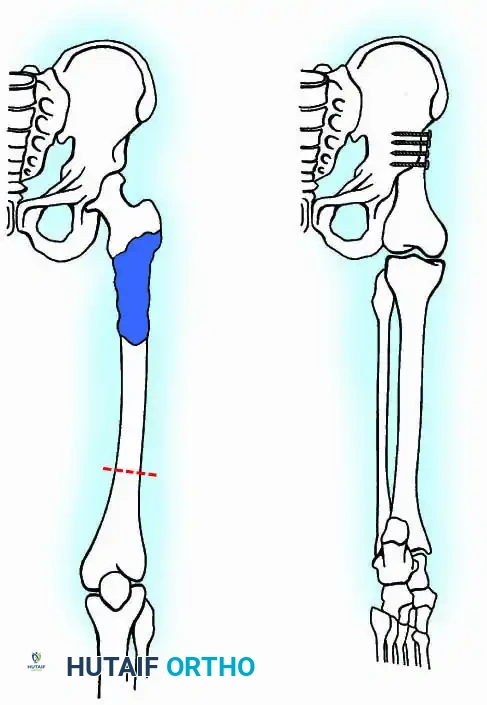
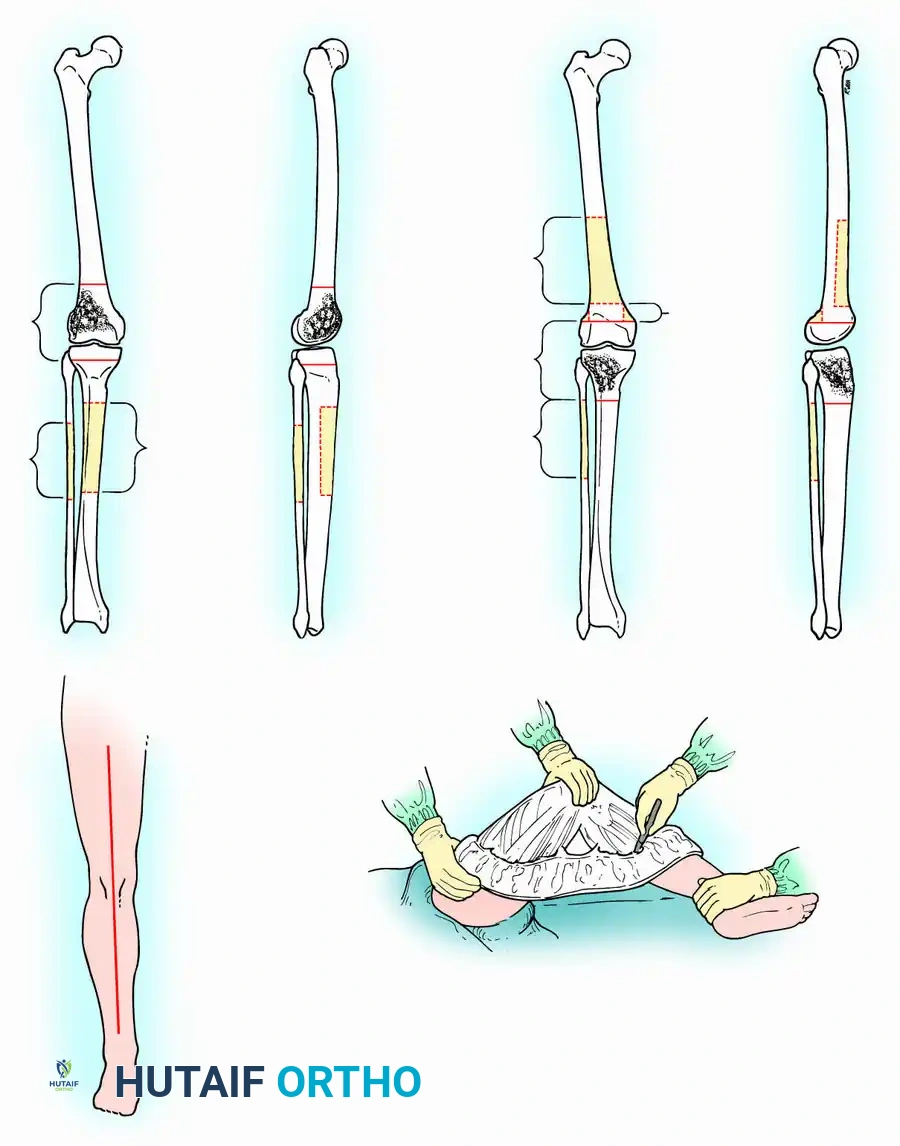
To standardize terminology and allow for meaningful comparison of oncologic and functional results, Malawer et al. proposed a comprehensive classification system for shoulder girdle resections. This system is based strictly on the anatomical structures removed, reflecting the relationship to the glenohumeral joint and the status of the abductor mechanism. The Malawer Classification System categorizes resections into six distinct types: Type I is an intra-articular proximal humeral resection; Type II is a partial scapular resection; Type III is an intra-articular total scapulectomy; Type IV is an extra-articular total scapulectomy and humeral head resection; Type V is an extra-articular humeral head resection; and Type VI is an extra-articular humeral and total scapular resection. Each type is further subdivided based on the status of the abductor mechanism (deltoid and rotator cuff): 'A' denotes an intact abductor mechanism, whereas 'B' indicates partial or complete resection of the abductor mechanism.

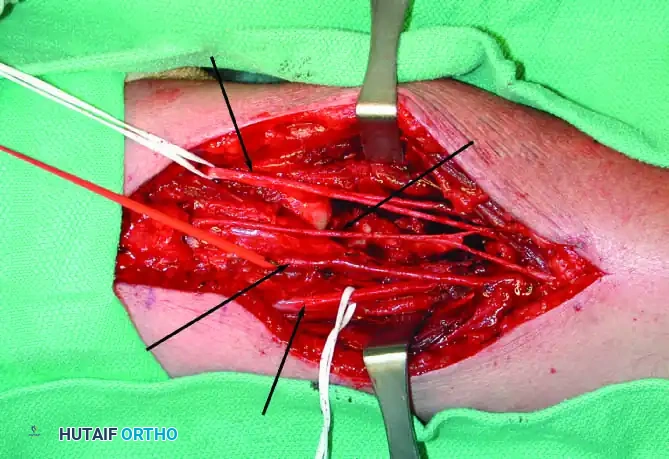
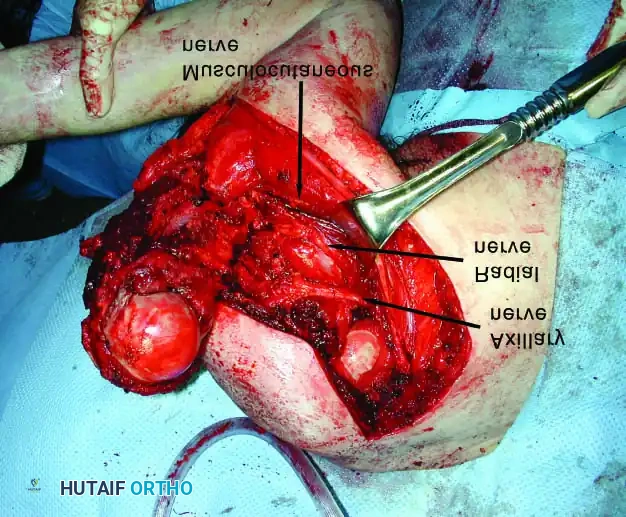
A profound understanding of the neurovascular topography is non-negotiable. The brachial plexus and axillary vessels exit the thoracic outlet and traverse the axilla in intimate proximity to the coracoid process, subscapularis, and proximal humerus. The axillary nerve, a terminal branch of the posterior cord, traverses the quadrangular space accompanied by the posterior circumflex humeral artery, wrapping around the surgical neck of the humerus. This perilous anatomical course makes the axillary nerve highly susceptible to involvement by proximal humeral sarcomas, frequently mandating its en bloc resection. Similarly, the radial nerve courses obliquely across the posterior aspect of the humeral shaft within the spiral groove, placing it at extreme risk during intercalary resections of the humeral diaphysis. Biomechanically, the loss of the deltoid (via axillary nerve sacrifice) drastically reduces active forward elevation and abduction, shifting the reconstructive goal from dynamic motion restoration to static stability and distal limb function preservation.
Following massive resection, the biomechanical paradigm shifts entirely. If an endoprosthetic arthroplasty or Allograft-Prosthetic Composite (APC) is utilized without a functional rotator cuff and deltoid, the construct relies entirely on capsular repair and static suspension to the acromion or clavicle to prevent inferior subluxation. The advent of reverse total shoulder arthroplasty (RTSA) megaprostheses has offered a biomechanical advantage by medializing the center of rotation and increasing the deltoid lever arm, provided the axillary nerve and a sufficient portion of the deltoid can be preserved. When the entire shoulder girdle is resected (Tikhoff-Linberg procedure), the arm becomes a "flail shoulder," suspended merely by scar tissue and dynamic transfers of the biceps and triceps to the remaining axial musculature. Despite this profound proximal biomechanical deficit, hand and elbow function can remain remarkably robust, justifying the procedure over forequarter amputation.
Exhaustive Indications and Contraindications
The decision to pursue limb salvage versus amputation in the upper extremity requires a multidisciplinary approach, weighing oncologic safety against functional outcomes, patient expectations, and the anatomical feasibility of reconstruction. The primary objective is absolute tumor eradication with negative margins; functional restoration, while critical, is strictly secondary. Advanced imaging modalities and neoadjuvant therapies have significantly expanded the indications for limb salvage, reducing the historical reliance on forequarter amputations. However, the surgeon must remain vigilant, as inappropriate attempts at limb salvage in the face of massive local disease can lead to catastrophic local recurrence, fungating tumor masses, and ultimately, a painful, non-functional limb that serves only as a detriment to the patient's quality of life.
One absolute indication for amputation in the upper extremity is extensive, un-reconstructible neurovascular involvement that precludes a functional, sensate hand. Specifically, if the tumor encases the brachial plexus cords or the major vascular trunks in a manner that requires their complete sacrifice without the possibility of nerve grafting or vascular bypass, a forequarter amputation is mandated. A displaced pathological fracture with massive soft-tissue contamination may also serve as a relative indication for amputation, depending on the tumor grade, the extent of the hematoma compartment breach, and the response to neoadjuvant chemotherapy. If the hematoma tracking extends proximally into the axilla and distally into the forearm, the required resection volume may leave the limb entirely flail and insensate.


Age, systemic health, and patient compliance also play pivotal roles in the decision-making process. Massive endoprosthetic reconstructions require rigorous, prolonged rehabilitation and carry a high lifetime risk of revision surgery for aseptic loosening, mechanical failure, or infection. In a highly non-compliant patient, or a patient with severe medical comorbidities precluding multiple major surgeries, a primary amputation or a more durable, low-demand procedure such as a flail shoulder or arthrodesis may be indicated over a complex Allograft-Prosthetic Composite.
| Indication/Contraindication Category | Specific Clinical Scenarios | Rationale and Surgical Implications |
|---|---|---|
| Absolute Indications for Limb Salvage | Primary bone sarcomas (Stage IA-IIB) confined to the bone or single compartment; clear neurovascular planes on MRI; sensate hand achievable. | Standard of care; allows for wide local excision with functional reconstruction using megaprosthesis or APC. |
| Relative Indications for Limb Salvage | Pathologic fracture with contained hematoma; encasement of a single major nerve (e.g., radial or axillary) that can be sacrificed; metastatic disease with reasonable life expectancy. | Requires extensive soft tissue resection and potential tendon transfers to restore lost nerve function; functional outcome is diminished but superior to amputation. |
| Absolute Contraindications for Limb Salvage | Complete encasement of the brachial plexus and axillary vessels precluding a sensate hand; massive fungating tumor with superinfection; inability to achieve negative margins. | Limb salvage will result in a painful, useless appendage and high risk of local recurrence; forequarter or high above-elbow amputation is strictly required. |
| Relative Contraindications for Limb Salvage | Extensive radiation-induced tissue necrosis; severe patient non-compliance; profound medical comorbidities; massive multi-compartmental contamination from poorly placed biopsy. | High risk of catastrophic failure, deep infection, and wound breakdown; requires complex free tissue transfer (e.g., latissimus or rectus free flap) if salvage is attempted. |
Pre-Operative Planning, Templating, and Patient Positioning
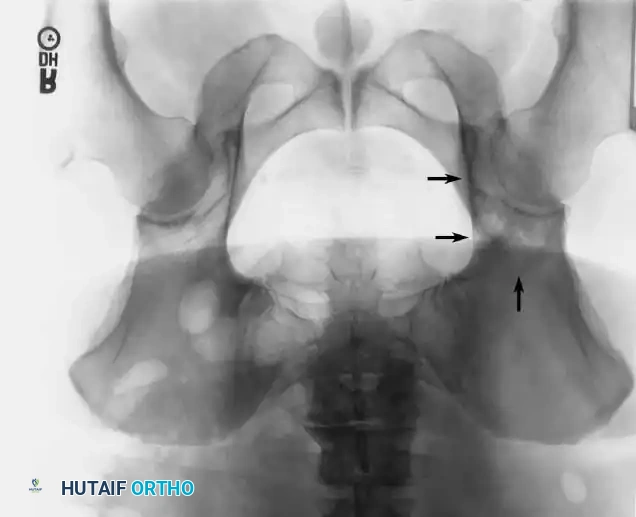
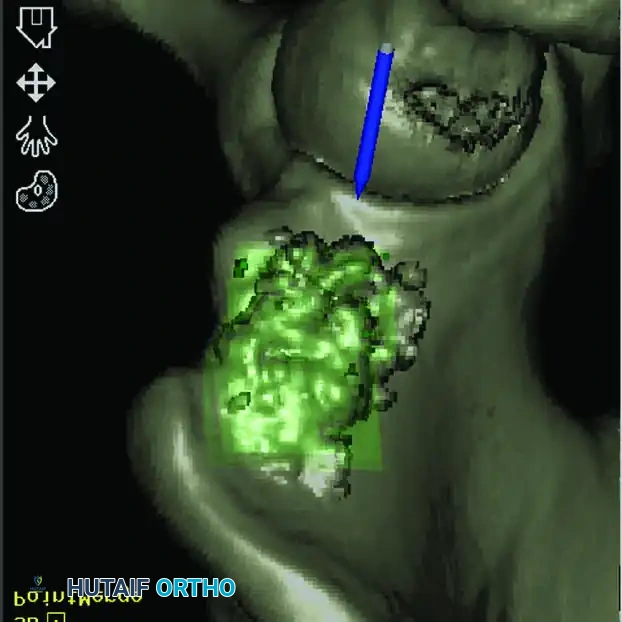
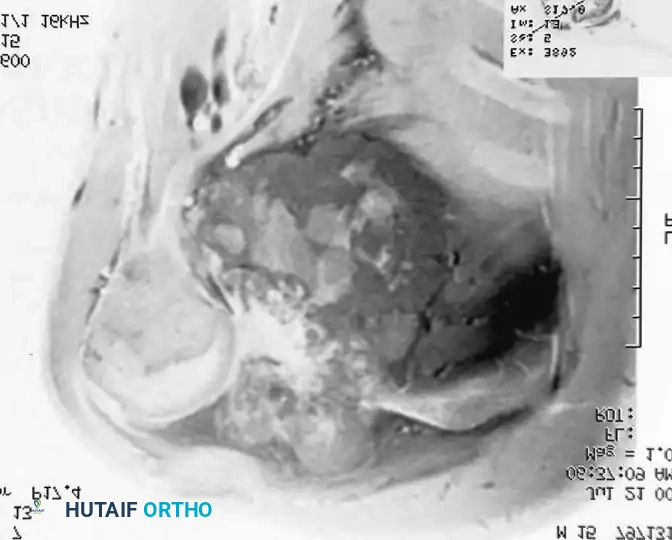
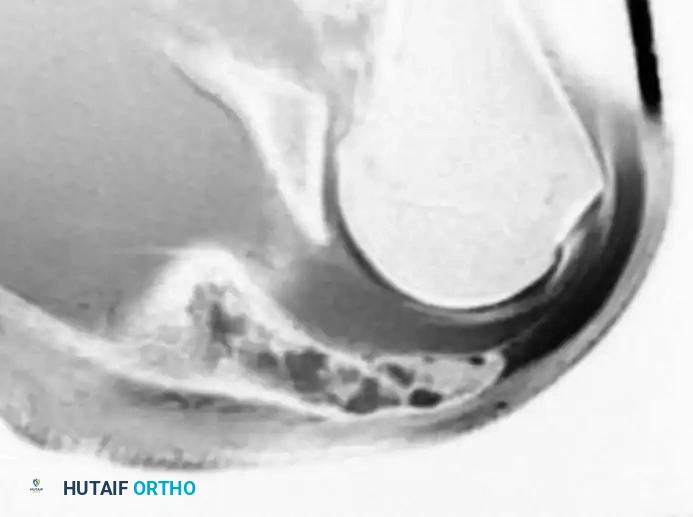
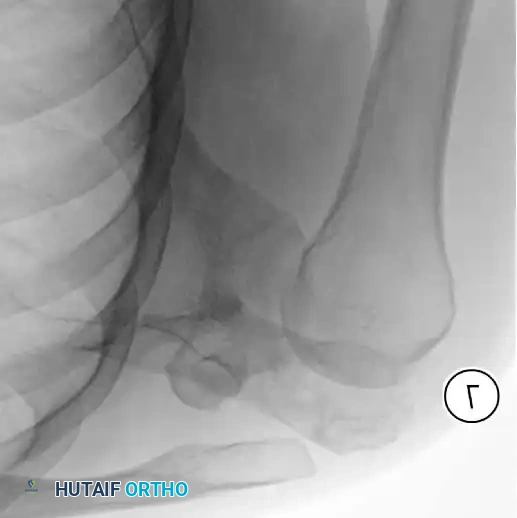
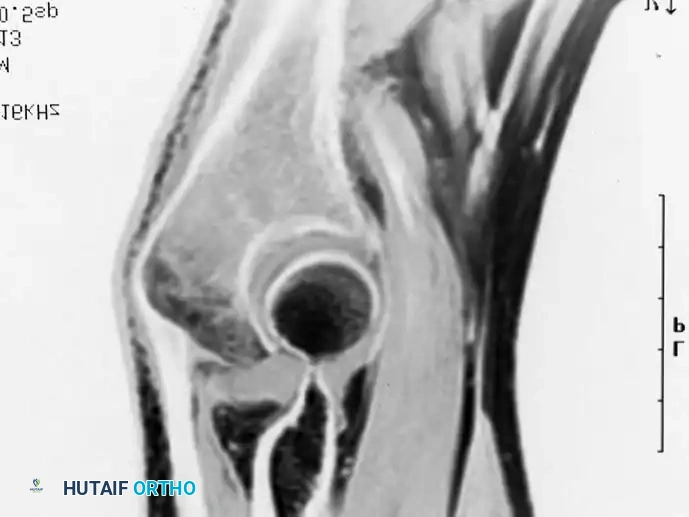
Meticulous preoperative planning is the cornerstone of successful upper extremity limb salvage. The process begins with exhaustive staging, including a high-resolution MRI of the entire affected bone with and without gadolinium contrast to delineate intraosseous skip metastases, soft tissue extension, and the critical relationship of the tumor pseudocapsule to the neurovascular bundle. A CT scan of the chest is mandatory to rule out pulmonary metastases, while a whole-body PET-CT or bone scan assesses for distant skeletal disease. Biopsy of a proximal humeral lesion must be performed through the anterior third of the deltoid, taking absolute care not to contaminate the deltopectoral interval. Contamination of this interval allows tumor cells to spread along the neurovascular bundle, making a successful limb-sparing resection exponentially more difficult and increasing the risk of local recurrence. The biopsy tract must be longitudinally oriented, meticulously hemostatic, and placed in line with the definitive surgical incision so it can be excised en bloc with the specimen.


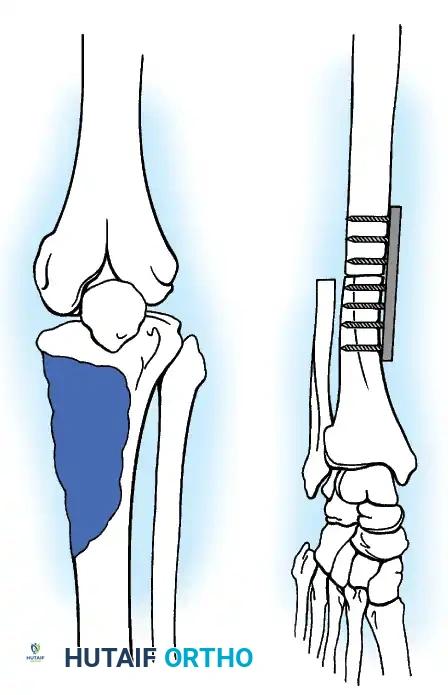
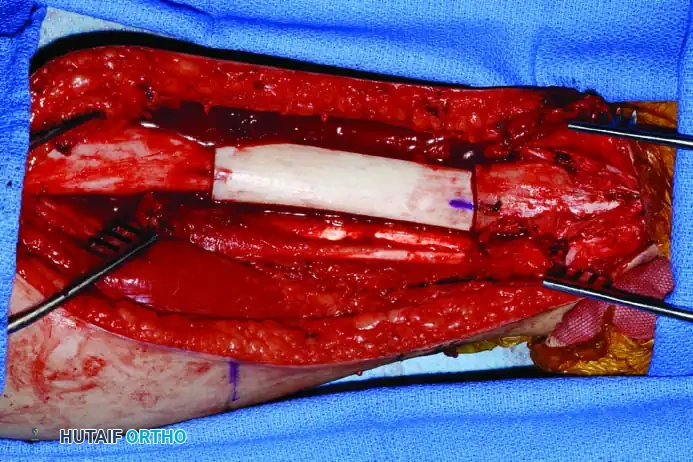
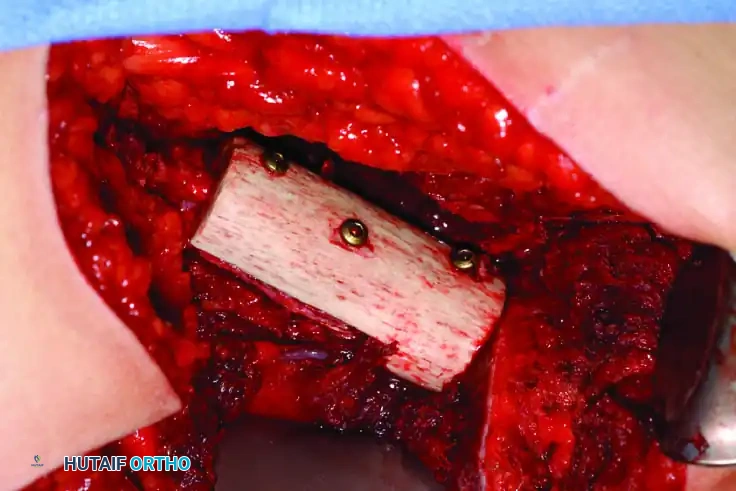
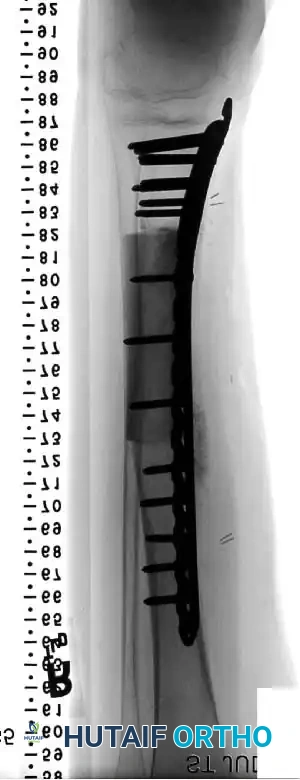
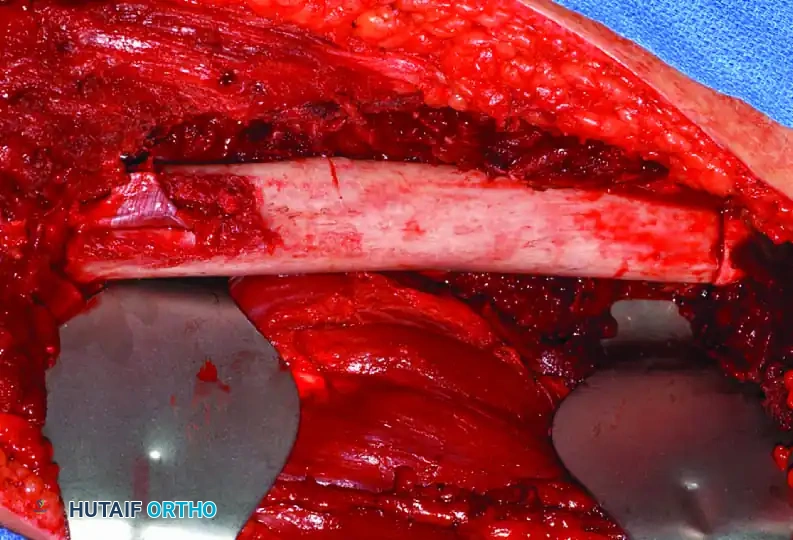
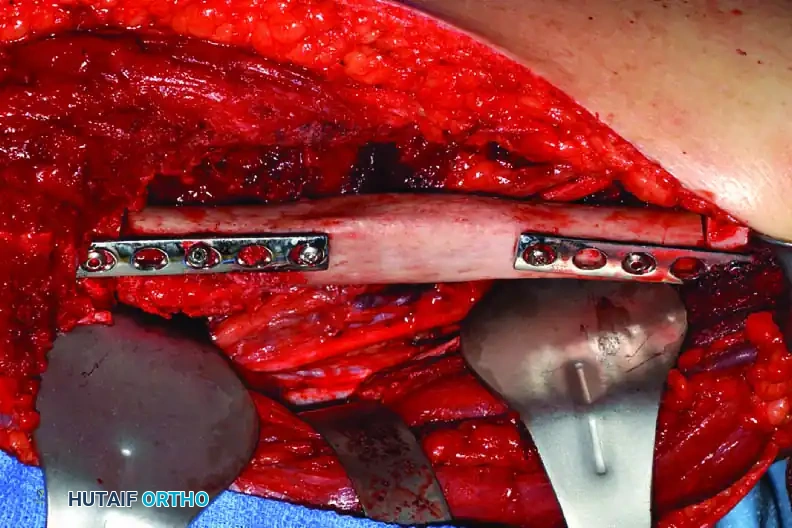
Advanced 3D templating has become standard practice for complex shoulder girdle resections. High-resolution CT data is utilized to create patient-specific 3D printed models and cutting guides. This allows the surgeon to precisely plan the osteotomy sites to ensure wide oncologic margins while maximizing the preservation of host bone for prosthetic fixation. When utilizing an Allograft-Prosthetic Composite (APC), preoperative templating is critical to match the dimensions of the allograft to the host bone and to select an implant with the appropriate stem diameter and length to span the host-allograft junction. Step-cut osteotomies at the host-allograft junction combined with rigid plate fixation significantly increase rotational stability and union rates compared to transverse osteotomies.
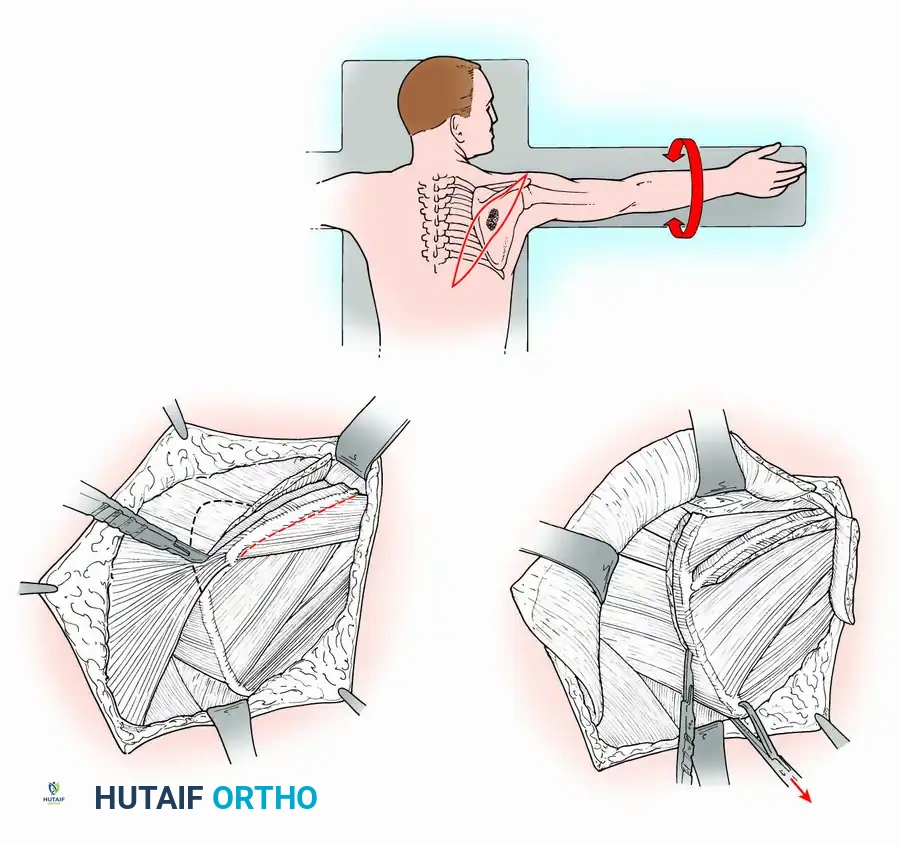
Patient positioning is dictated by the specific anatomical requirements of the planned resection. For isolated proximal humeral resections, the patient is typically placed in the beach-chair position, which allows excellent visualization of the anterior shoulder structures and facilitates gravity-assisted retraction of the arm. However, for total or partial scapulectomies, or the Tikhoff-Linberg procedure, the patient must be placed in the lateral decubitus or prone position. The arm is rested on a sterile arm board or suspended using a sterile traction device, allowing it to be draped free. This free-draping is absolutely critical, as it permits dynamic manipulation of the limb during the procedure—abducting and rotating the arm allows the axillary contents to fall away from the scapular neck, protecting the neurovascular bundle during deep osteotomies and soft tissue dissection.


The surgical team must also prepare for extensive blood loss and the potential need for vascular reconstruction. Arterial lines, central venous access, and rapid infusion systems should be established by the anesthesia team. A vascular surgeon and a microsurgical plastic surgeon should be available on standby, particularly if tumor proximity to the axillary vessels suggests the need for segmental resection and vein grafting, or if massive soft tissue defects will require immediate free flap coverage to protect the endoprosthesis.
Step-by-Step Surgical Approach and Fixation Technique
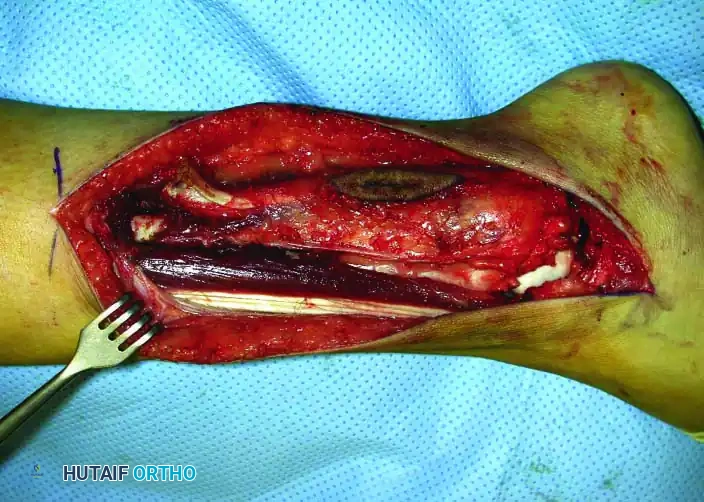
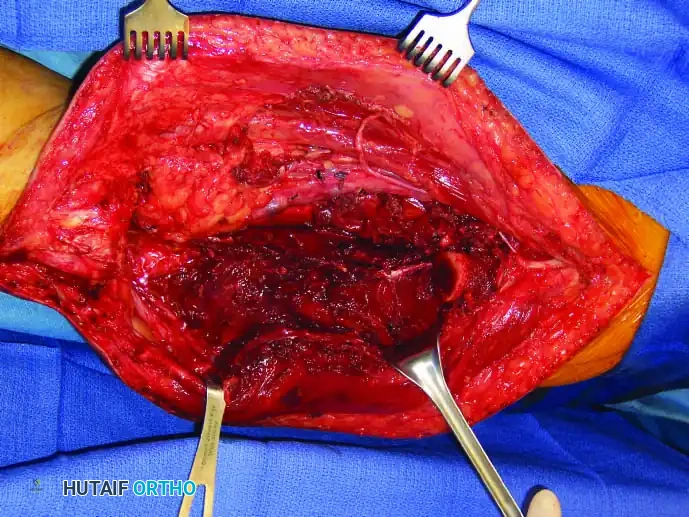
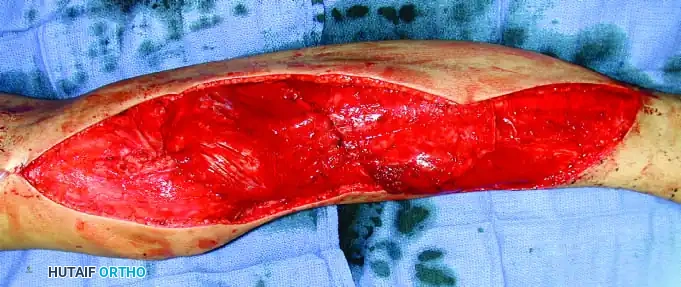
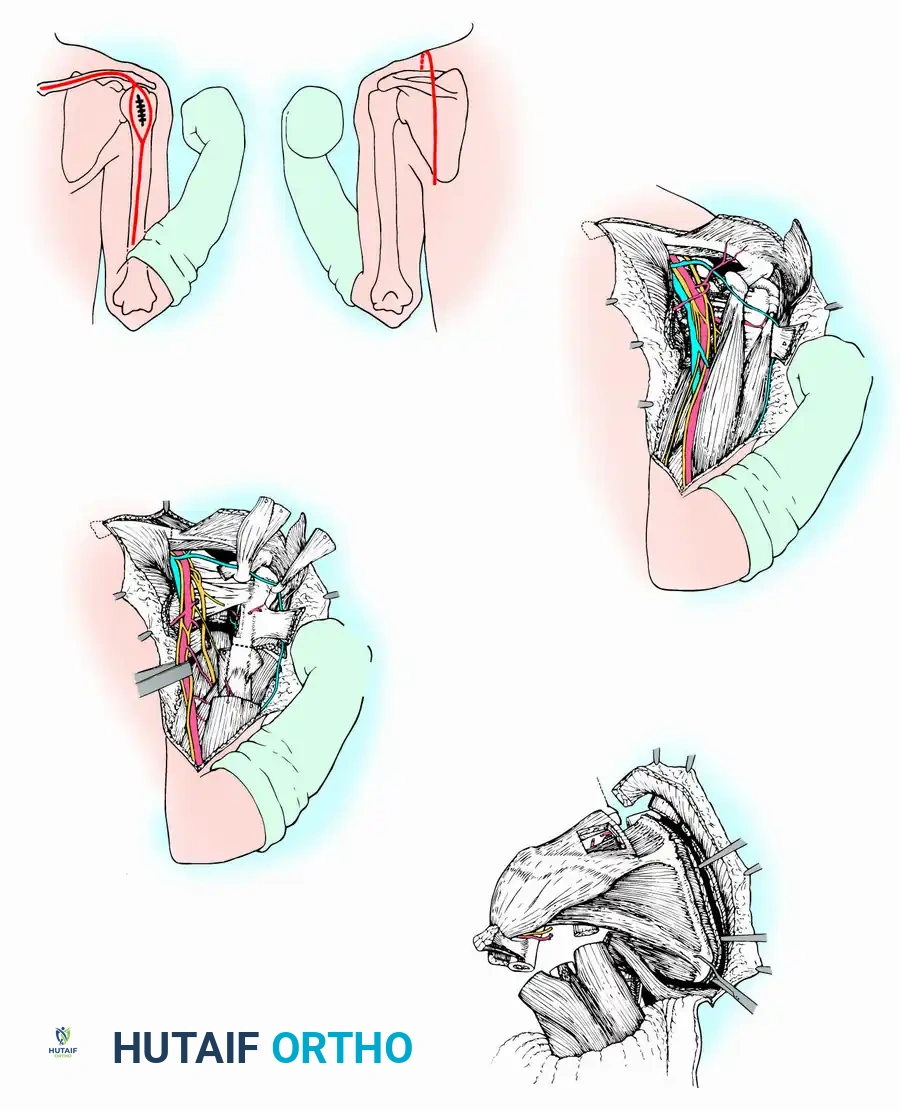
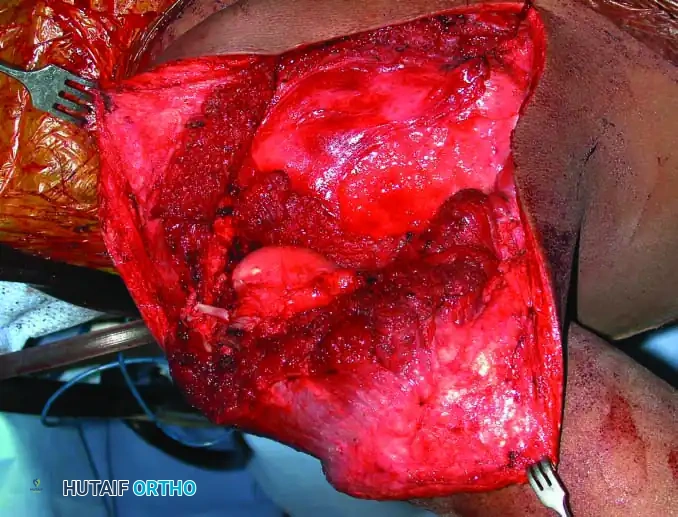
The Tikhoff-Linberg procedure is a massive resection of the shoulder girdle consisting of total scapulectomy, partial or complete excision of the clavicle, and excision of the proximal humerus. It is indicated for high-grade malignant tumors around the shoulder where a sufficient margin of normal tissue exists to clear the neurovascular bundle. The Marcove, Lewis, and Huvos Approach begins with an extensive incision extending from the medial end of the clavicle along the medial two-thirds of the bone, curving inferiorly over the coracoid process, and continuing along the medial aspect of the arm. From the midpoint of this anterior incision, a posterior longitudinal extension is made along the middle of the scapula down to its inferior angle. The deltoid and pectoralis major and minor are incised inferior to the clavicle and medial to the coracoid.
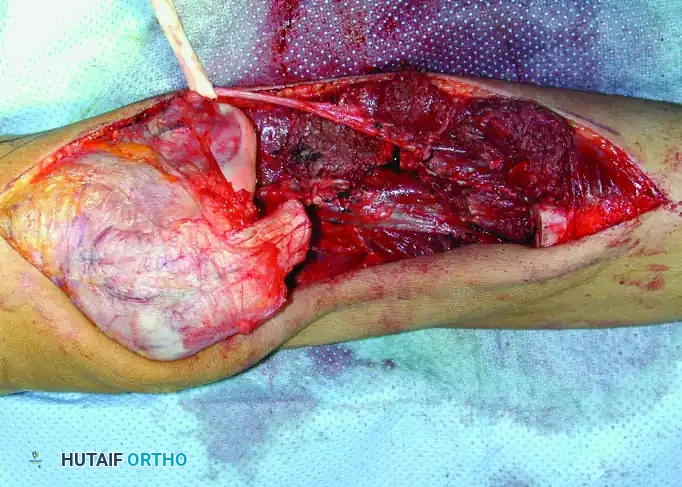
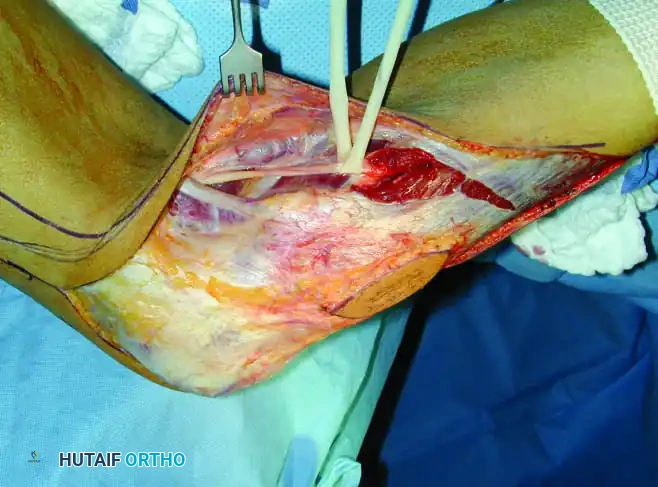
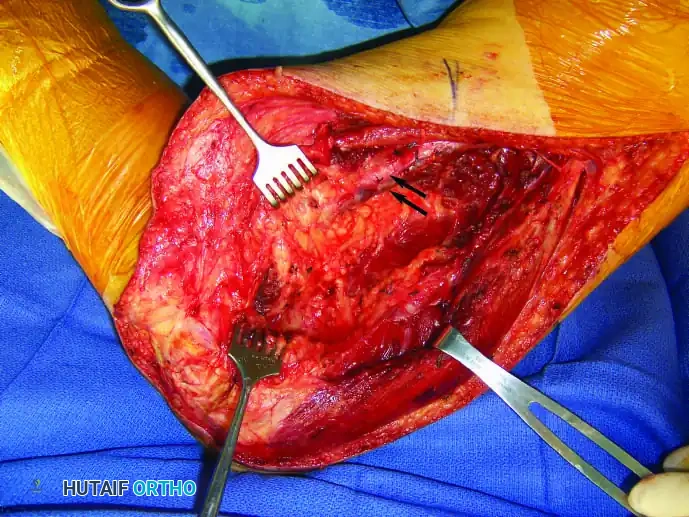
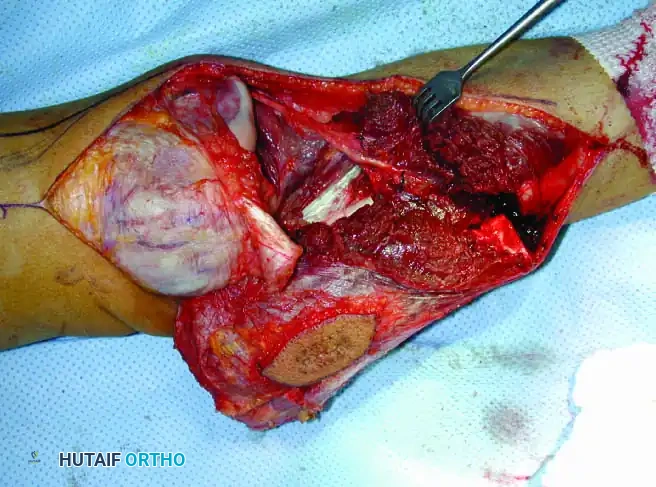
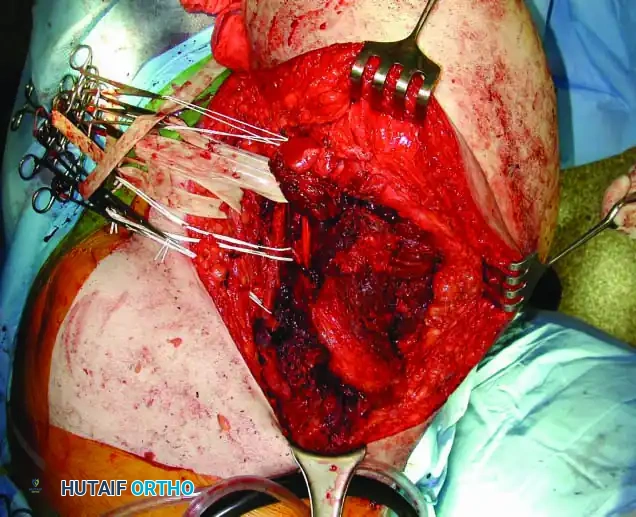
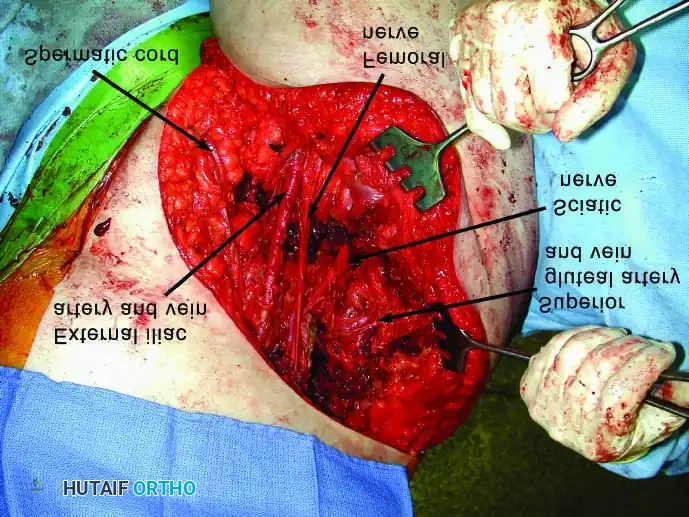
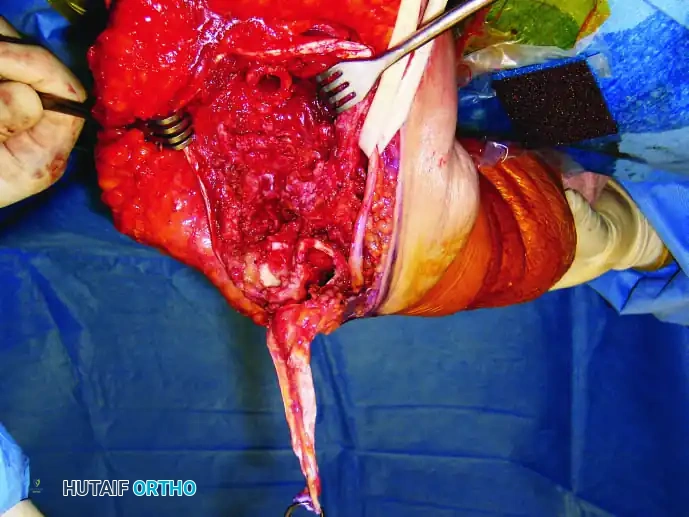
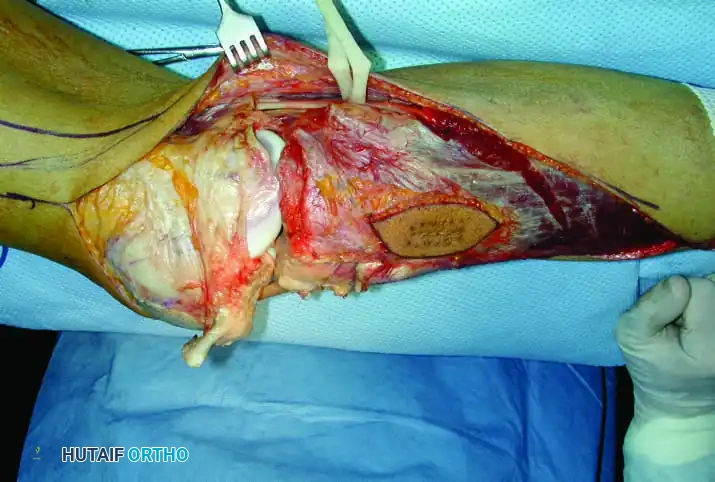
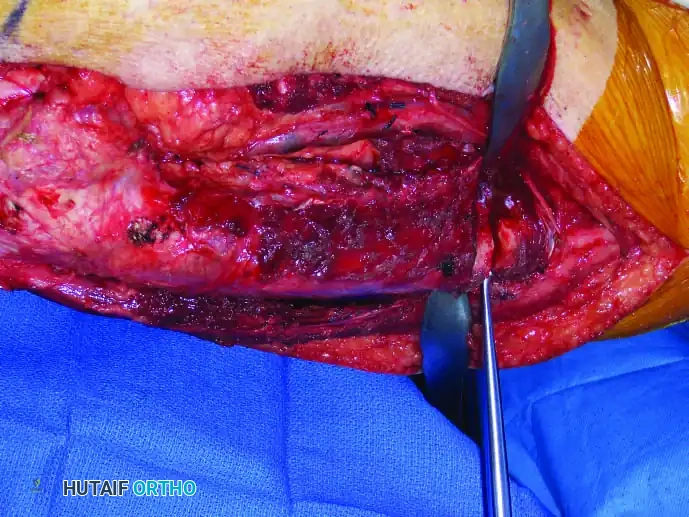
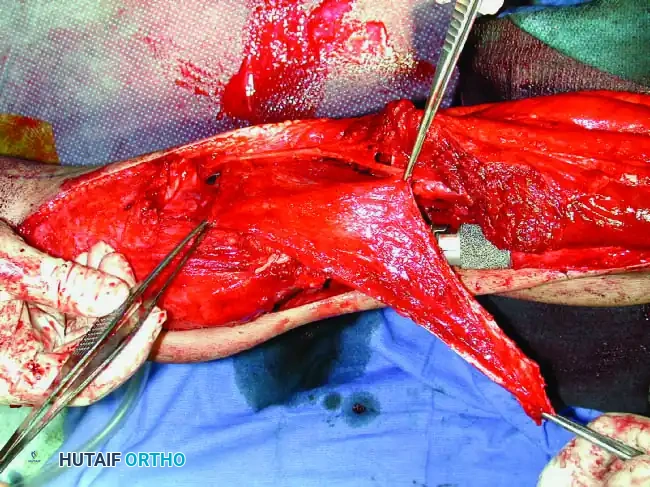
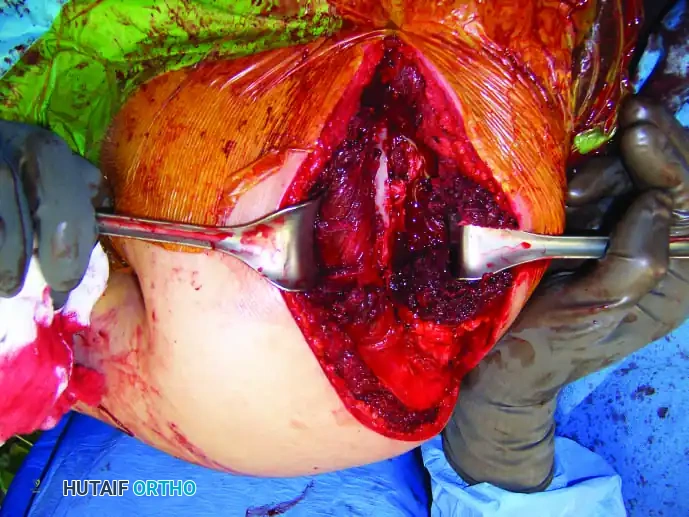
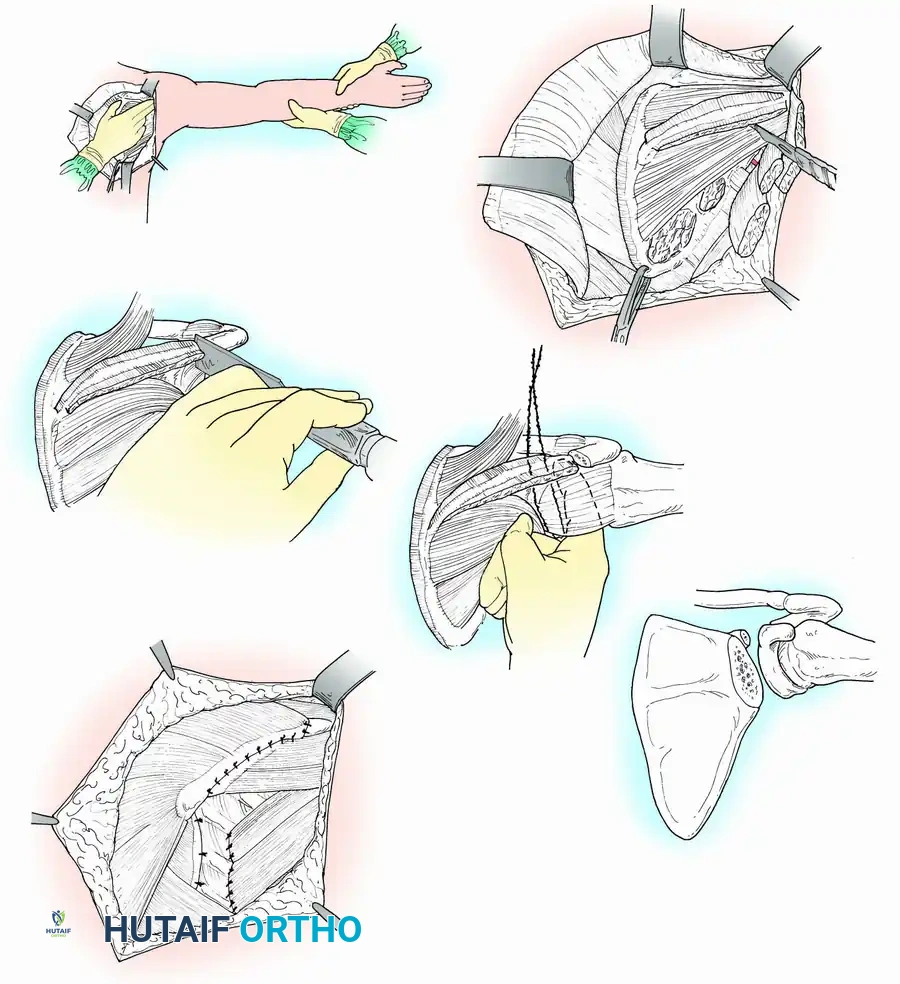
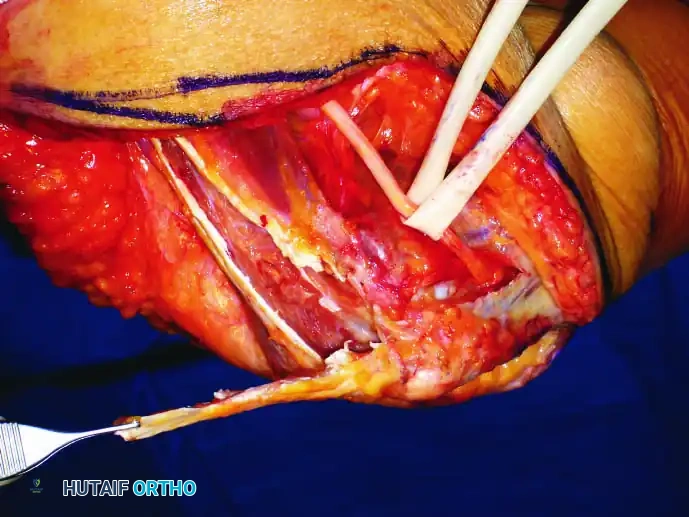
Neurovascular dissection is the most critical and perilous phase of the procedure. The cephalic vein is ligated to expose the axillary vessels and the brachial plexus. The surgeon must meticulously determine that the neurovascular bundle is not involved by the tumor pseudocapsule. The anterior and posterior humeral circumflex vessels are ligated, and the axillary vessels are gently retracted medially. If oncologic margins dictate, the radial and musculocutaneous nerves must be sacrificed without hesitation. The muscular division follows, dividing the coracobrachialis, short head of the biceps, triceps, teres major, and latissimus dorsi muscles well away from the tumor pseudocapsule. The medial end of the clavicle is osteotomized using a Gigli saw or an oscillating saw, protecting the underlying subclavian vessels with a malleable retractor.

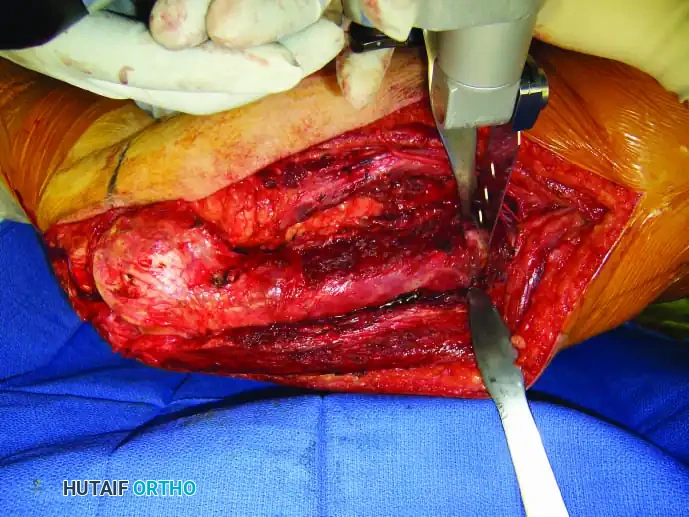
For Scapulectomy (Total or Partial), the approach shifts posteriorly. With the patient in the lateral decubitus position, medial and lateral skin flaps are raised full-thickness down to the investing fascia. The attachment of the trapezius muscle to the scapular spine is divided, and the muscle is retracted superomedially. The latissimus dorsi is divided at the inferior angle. Traction is applied to the inferior angle with a heavy towel clip, allowing the surgeon to divide the rhomboids and levator scapulae at the vertebral border. By rotating the scapula and abducting the arm, the axillary contents fall away anteriorly. The teres major, teres minor, long head of the triceps, and rotator cuff tendons are systematically divided. A Gigli saw is passed around the neck of the scapula, taking extreme care to avoid breaching the glenohumeral joint capsule, and the osteotomy is completed to remove the specimen en bloc.
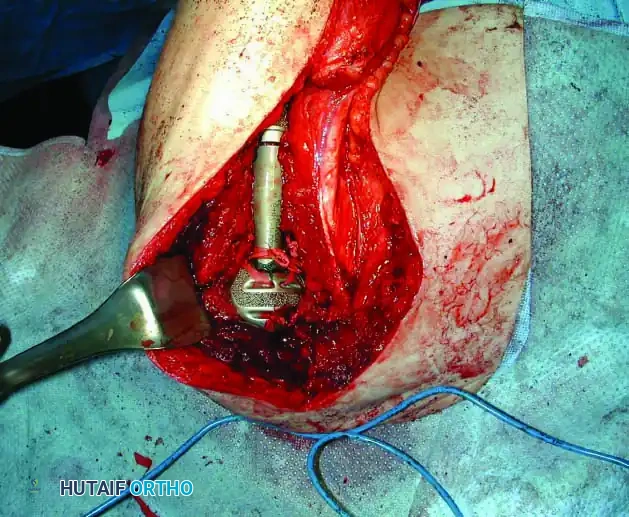

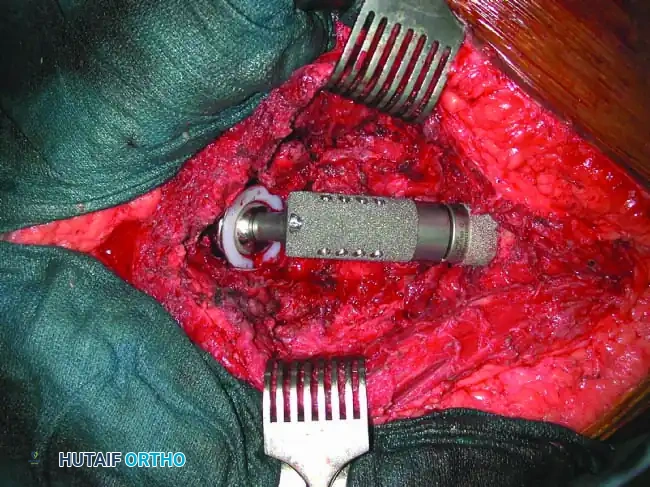
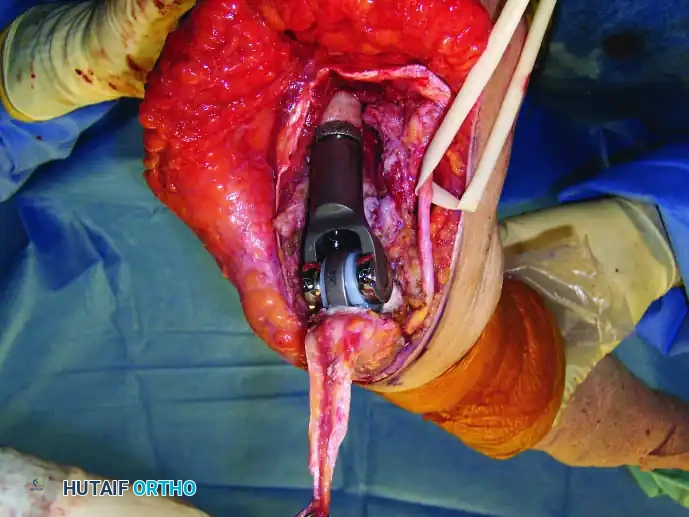
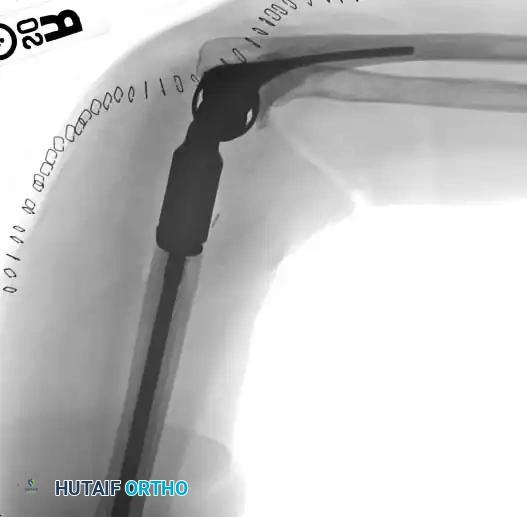
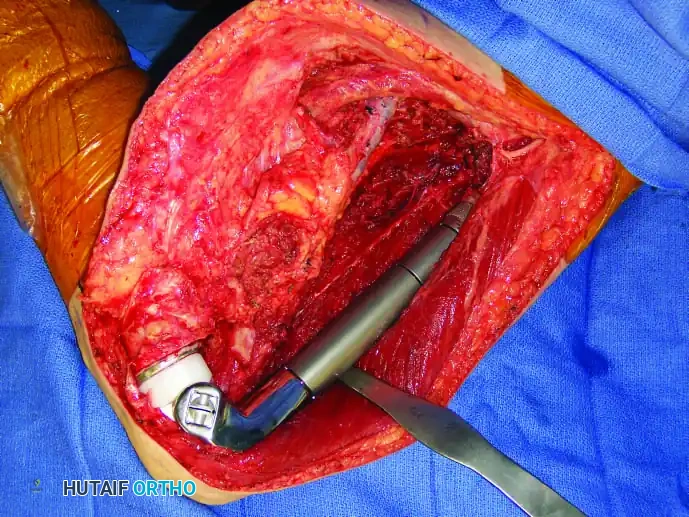
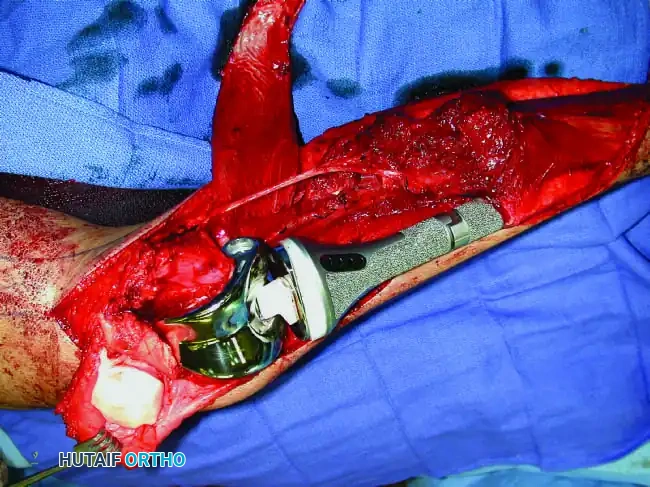
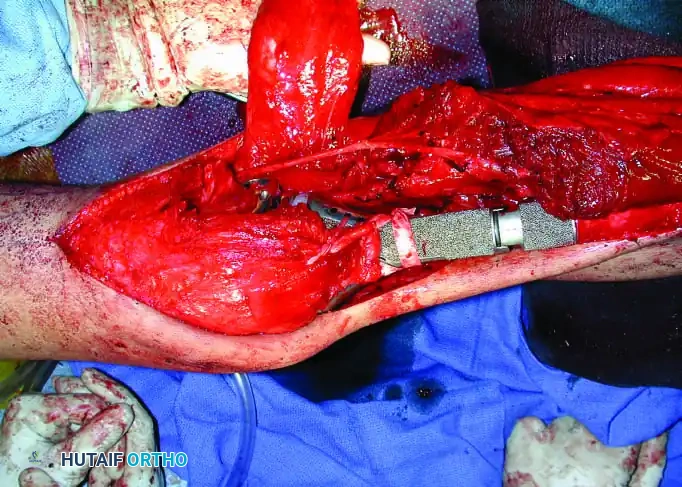
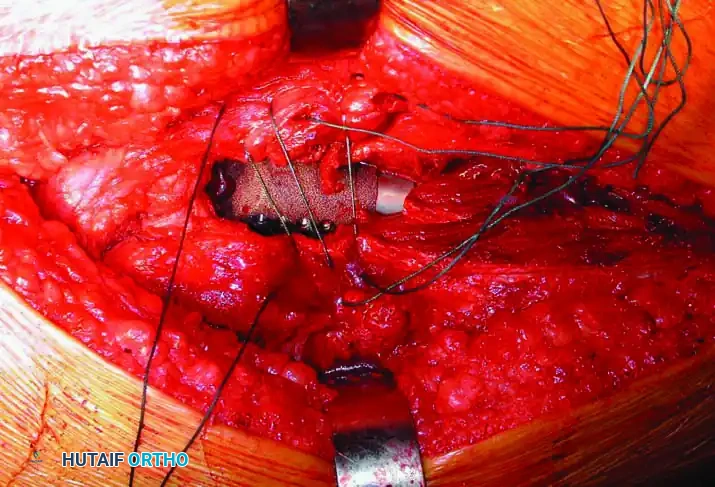
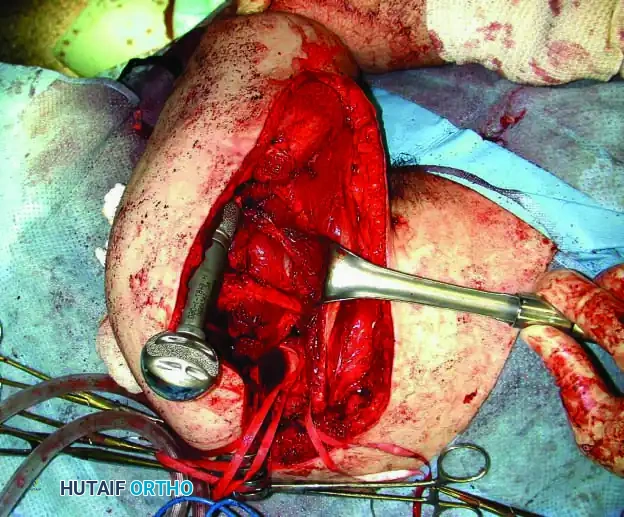
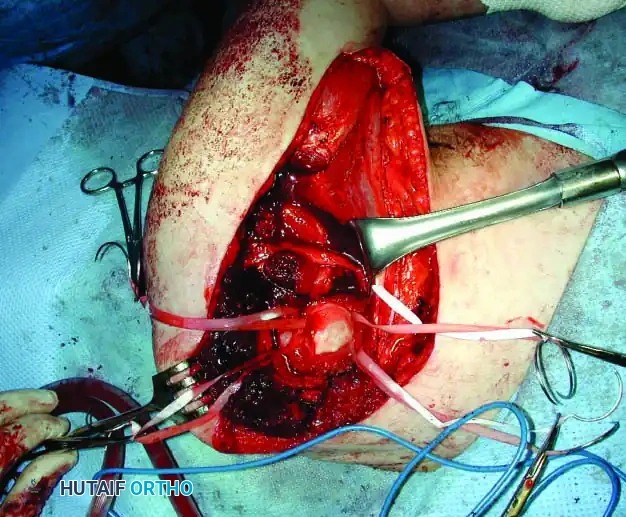
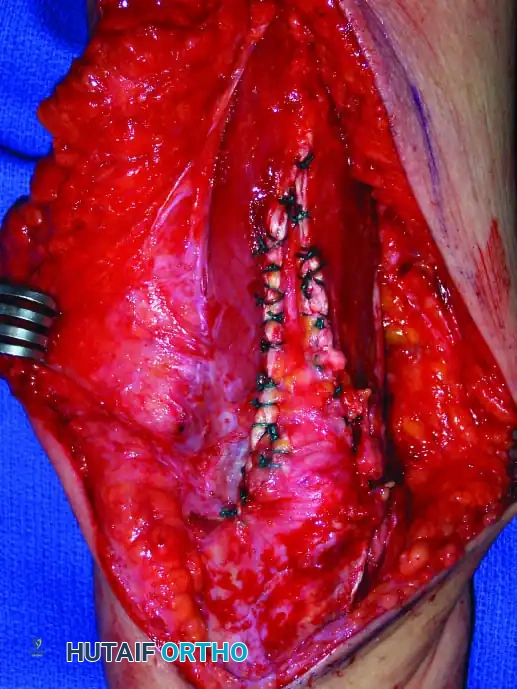
Reconstruction following these massive resections is highly complex. For proximal humerus resections, endoprosthetic arthroplasty using a modular megaprosthesis offers immediate stability. The prosthesis is inserted into the remaining humeral shaft and secured via cemented or press-fit stems. Soft tissue suspension is the Achilles heel of this reconstruction; the proximal end of the prosthesis must be suspended to the acromion, the remaining clavicular stump, or the second rib using heavy non-absorbable sutures, synthetic mesh (e.g., Trevira tube), or an Achilles tendon allograft. The remaining biceps and triceps are reattached to the trapezius, pectoralis major, and latissimus dorsi to provide a dynamic muscular sling. If a flail shoulder is chosen, the humerus is suspended directly to the clavicle or ribs using heavy suture, relying entirely on scar tissue for eventual stability.


Complications, Incidence Rates, and Salvage Management
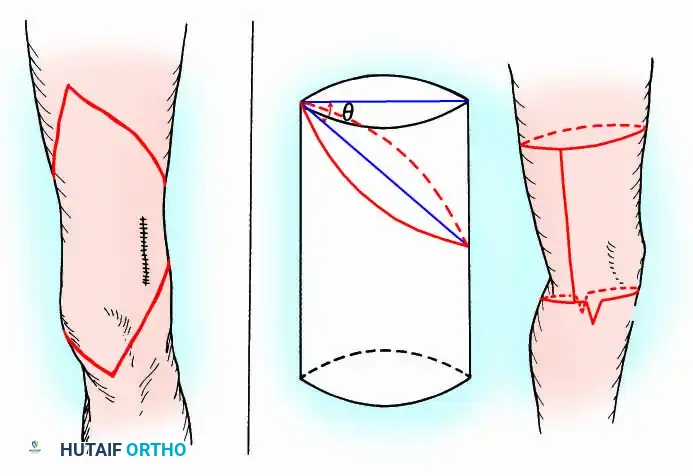
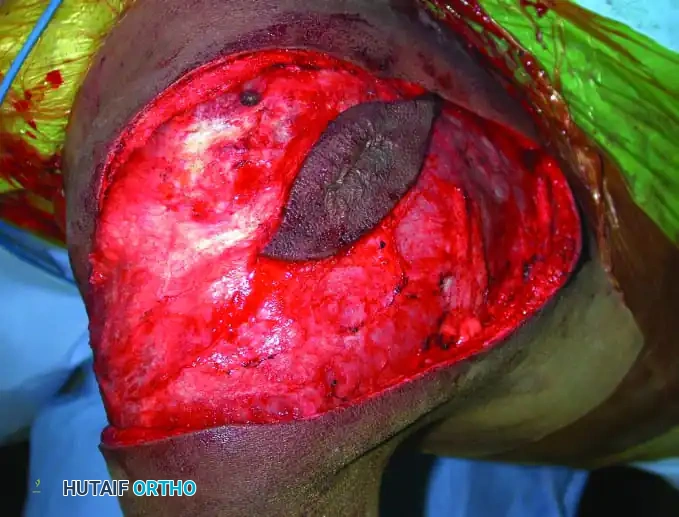
Massive limb salvage surgery of the upper extremity is fraught with early and late complications. The extensive soft tissue dissection, prolonged operative times, creation of massive dead space, and the immunocompromised state of patients receiving neoadjuvant chemotherapy create a perfect storm for surgical site infections and wound breakdown. Deep periprosthetic joint infection (PJI) is one of the most devastating complications, often necessitating multiple debridements, prolonged intravenous antibiotics, and potentially the removal of the megaprosthesis. The lack of robust soft tissue coverage, particularly over the anterior aspect of the proximal humerus, frequently requires the use of rotational or free muscle flaps (e.g., latissimus dorsi or rectus abdominis) to achieve stable wound closure and obliterate dead space.
Mechanical complications are equally prevalent. Aseptic loosening of the humeral stem, particularly in young, active patients, remains a significant cause of late failure. The bending moments and torsional forces applied to the stem-bone interface, combined with stress shielding from rigid metallic stems, can lead to progressive osteolysis. Instability and dislocation of the proximal humeral prosthesis are exceedingly common, occurring in up to 30% of cases due to the complete loss of the rotator cuff and capsular restraints. To mitigate this, surgeons utilize constrained liners, dual-mobility articulations, or synthetic mesh tubes (Trevira) to tightly imbricate the joint and promote dense scar tissue formation.



Local recurrence of the tumor is the ultimate oncologic failure, carrying a grim prognosis for both limb survival and overall patient survival. Recurrence is typically managed with radical re-resection, which almost universally mandates a forequarter amputation if the recurrence involves the neurovascular bundle or the chest wall. The risk of local recurrence is directly correlated with the adequacy of surgical margins, underscoring the absolute necessity of precise preoperative planning and uncompromised intraoperative execution.
| Complication | Estimated Incidence Rate | Etiology and Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Periprosthetic Infection | 10% - 25% | Massive dead space, prolonged surgery, chemotherapy-induced immunosuppression, poor soft tissue envelope. | Irrigation and debridement, targeted IV antibiotics. Two-stage revision with antibiotic spacer for chronic infections. Flap coverage if soft tissue is deficient. |
| Prosthetic Instability / Dislocation | 15% - 30% | Loss of rotator cuff, inadequate capsular reconstruction, failure of suspensory mesh, deltoid sacrifice. | Closed reduction and prolonged immobilization. Revision to constrained liner, dual-mobility construct, or reinforcement with allograft/synthetic mesh. |
| Aseptic Loosening | 10% - 20% (at 10 years) | Stress shielding, high torsional forces, inadequate initial stem fixation, poor bone stock. | Revision arthroplasty with longer, thicker stem. Impaction bone grafting. Transition to total humeral replacement if bone stock is critically depleted. |
| Local Tumor Recurrence | 5% - 15% | Marginal or intralesional resection, highly aggressive tumor biology, tumor spill during biopsy. | Radical re-resection. Often requires forequarter amputation. Adjuvant radiation therapy if margins cannot be cleared. |
| Nerve Palsy (Axillary/Radial) | 5% - 10% (Iatrogenic) | Traction injury during retraction, direct contusion, ischemia. | Observation and EMG at 3 months. Tendon transfers (e.g., modified Eden-Lange or wrist extensor transfers) if recovery fails after 12 months. |



Phased Post-
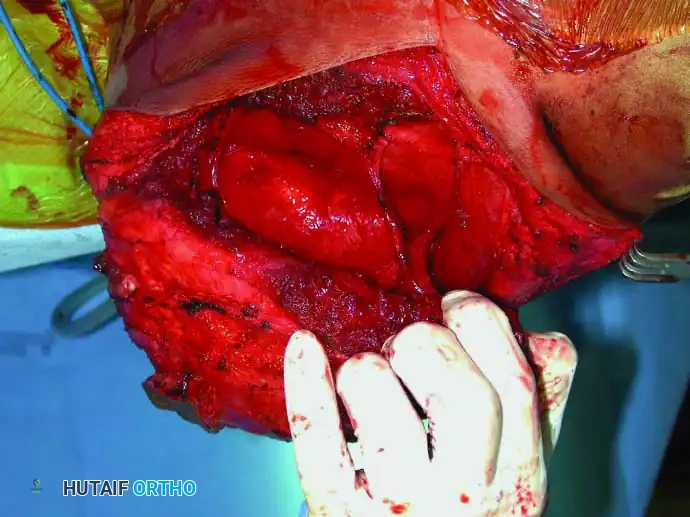
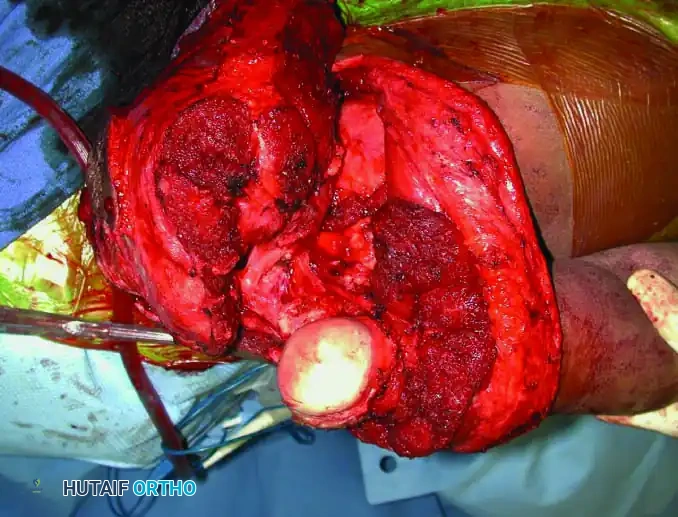
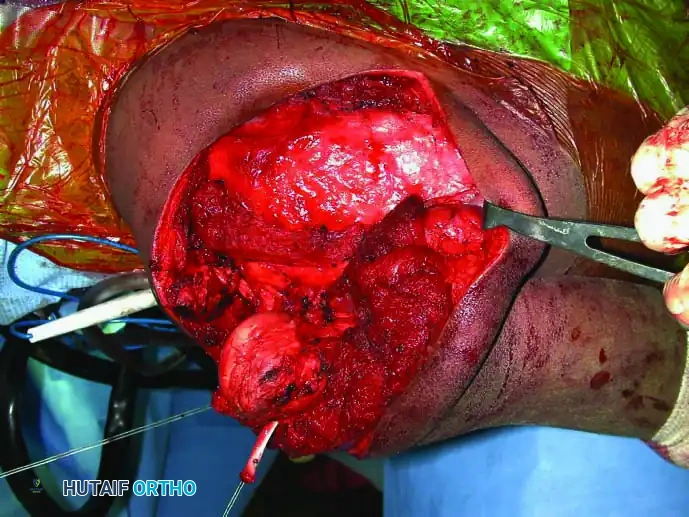
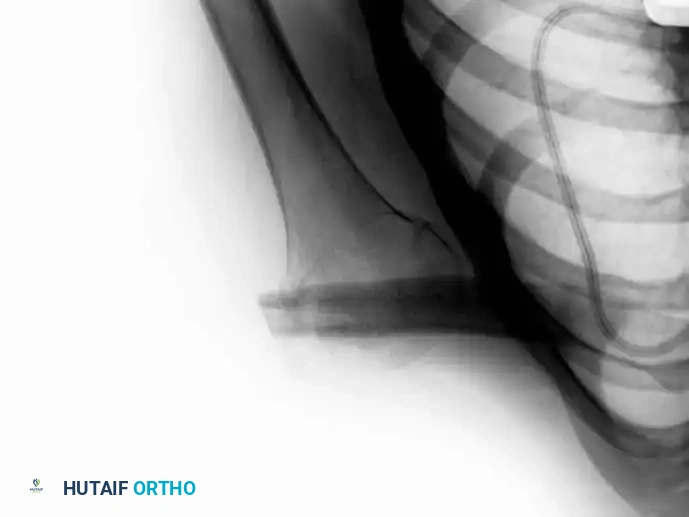
Clinical & Radiographic Imaging Archive