Lower Extremity Amputations: Operative Principles and Techniques
Key Takeaway
Lower extremity amputations are critical reconstructive procedures primarily indicated for dysvascular limbs, trauma, and oncologic resections. Successful outcomes depend on meticulous preoperative physiological optimization, precise surgical technique, and the preservation of maximal functional limb length. This guide details the biomechanical considerations, step-by-step surgical approaches, and postoperative rehabilitation protocols essential for transforming the residual limb into a highly functional sensory-motor end organ for prosthetic weight-bearing.
Comprehensive Introduction and Patho-Epidemiology
Lower limb amputations represent a profound intersection of surgical reconstruction, biomechanical engineering, and complex medical management. Accounting for 76% to 80% of all amputations performed globally, these procedures are most frequently dictated by the devastating progression of dysvascular disease. The vast majority of these surgical interventions are necessitated by end-stage manifestations of advanced diabetes mellitus or primary peripheral vascular disease (PVD), which together account for an overwhelming 82% of all hospital discharges attributed to major limb amputations. Strikingly, 97% of all dysvascular amputations occur in the lower extremities, reflecting the unique vulnerability of the distal appendicular skeleton to microvascular and macrovascular ischemic insults.
Despite significant modern advancements in endovascular interventions, atherectomy devices, and open distal revascularization bypass techniques, the overall population-adjusted rates of lower extremity amputations have remained stubbornly constant. This epidemiological persistence is largely driven by the exponential global increase in the prevalence of type 2 diabetes mellitus, coupled with an aging demographic characterized by profound metabolic syndrome and chronic kidney disease. Historically, amputation was viewed through a nihilistic lens—as a definitive failure of limb salvage. However, the modern orthopedic paradigm mandates that the decision to amputate must be conceptualized as a primary, definitive reconstructive procedure. The ultimate surgical objective is to radically excise non-viable, infected, or painful tissue and reconstruct the residual limb into a highly functional, durable "sensory-motor end organ." This reconstructed residuum must be capable of seamlessly interfacing with advanced prosthetic technology to restore bipedal locomotion and maximize the patient's independence.
The systemic comorbidities invariably associated with dysvascular amputations heavily dictate both the immediate surgical success and the long-term overall patient survival. The epidemiological data surrounding lower extremity amputations in the dysvascular population is remarkably sobering and must be communicated clearly to the patient and their family. The 5-year mortality rate following the major amputation of a dysvascular lower limb ranges from 40% to 60%, a survival curve that is worse than many advanced-stage malignancies. Patients suffering from primary peripheral vascular disease without diabetes carry an even higher morbidity and mortality rate than those with diabetes mellitus alone, reflecting widespread systemic atherosclerosis, concomitant coronary artery disease, and cerebrovascular disease. Long-term longitudinal studies indicate a mere 39% patient survival rate at 7 years post-amputation.
Furthermore, the disease process is rarely confined to a single extremity. The risk to the contralateral limb is exceptionally high, with amputation of the contralateral leg required within 5 years in 30% to 50% of dysvascular patients. Revision rates also remain a significant clinical challenge; approximately 20% of transtibial (below-knee) amputations ultimately require proximal conversion to transfemoral (above-knee) amputations due to progressive ischemia, intractable infection, or catastrophic wound failure. Age demographics further stratify risk: statistics from the Centers for Disease Control and Prevention (CDC) demonstrate that transfemoral amputations occur at a rate of 0.5 per 1,000 in diabetic patients younger than 65 years, compared to a staggering 4 per 1,000 in diabetic patients aged 75 years or older. Conversely, younger patients undergoing amputation for high-energy trauma or oncologic resection demonstrate significantly higher physiological reserves and achieve vastly superior success rates with prosthetic rehabilitation.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of lower extremity cross-sectional anatomy, vascular angiosomes, and muscular compartments is the foundational prerequisite for successful amputation surgery. In the dysvascular patient, the surgeon cannot rely on standard anatomical textbook vascularity; rather, they must understand the collateral pathways that sustain the ischemic limb. In the leg, the anterior and lateral compartments are primarily supplied by the anterior tibial artery, which is frequently the first vessel to occlude in diabetic infrapopliteal disease. Conversely, the posterior compartment, housing the bulky gastrocnemius and soleus muscles, receives a robust, redundant blood supply via the sural arteries (branches of the popliteal artery) and the posterior tibial artery. This anatomical reality is the physiological basis for the Burgess long posterior myocutaneous flap in transtibial amputations, which utilizes the well-vascularized posterior tissues to cover the distal tibia where anterior skin is reliably ischemic.
The biomechanics of amputation and the subsequent energy expenditure required for prosthetic ambulation dictate the functional destiny of the patient. The level of amputation has a profound, inverse relationship with the patient’s postoperative quality of life and ambulatory efficiency. This relationship is primarily dictated by the loss of anatomical joints, the shortening of the osseous lever arm, and the exponential increase in metabolic energy expenditure required to propel the body forward. Preserving the anatomical knee joint is universally recognized as the single most critical factor in maintaining ambulatory independence, particularly in the elderly or cardiopulmonary-compromised dysvascular patient. The anatomical knee provides unparalleled proprioception, swing-phase control, and stance-phase stability that even the most advanced microprocessor prosthetic knees cannot fully replicate.
The metabolic penalty of limb loss is staggering and must be factored into preoperative decision-making. For unilateral transtibial amputees, the increased energy consumption of bipedal locomotion ranges from 40% to 50% above their pre-morbid baseline. However, once the knee joint is sacrificed in a transfemoral amputation, the energy requirement skyrockets to 90% to 100% above baseline. Furthermore, the preferred walking speed of a transfemoral amputee decreases by nearly 45% to compensate for this massive metabolic demand. Because of this extreme physiological burden, many elderly transfemoral amputees lack the cardiac reserve to ambulate and ultimately become permanently wheelchair-bound.
In addition to energy expenditure, the biomechanics of the residual limb within the prosthetic socket rely heavily on optimal surgical muscle balancing (myodesis). In the transfemoral amputation, the adductor magnus is the most powerful adductor and hip extensor. If the adductor magnus is simply transected and allowed to retract, the unopposed hip abductors (gluteus medius and minimus) will pull the short femoral remnant into severe, fixed abduction. A laterally drifted, abducted femur destroys the mechanical axis of the limb, rendering the abductor mechanism functionally incompetent (a positive Trendelenburg gait) and making efficient prosthetic ambulation nearly impossible due to massive lateral trunk shift. Therefore, meticulous surgical restoration of the adductor tension via myodesis is a non-negotiable biomechanical requirement.
Exhaustive Indications and Contraindications
The decision to proceed with a major lower extremity amputation requires a multidisciplinary synthesis of the patient's vascular status, infectious burden, systemic physiological reserve, and functional potential. The indications for amputation span a broad spectrum of pathology, from acute, life-threatening sepsis to chronic, intractable pain. The timing of the amputation is equally critical; delaying a necessary amputation in a septic patient can lead to multi-organ failure and death, while premature amputation in a salvageable traumatized limb deprives the patient of their native anatomy.
In the setting of trauma, the decision between limb salvage and primary amputation remains one of the most challenging dilemmas in orthopedic surgery. Scoring systems such as the Mangled Extremity Severity Score (MESS) or the Limb Salvage Index (LSI) provide objective data based on skeletal/soft-tissue injury, limb ischemia, shock, and patient age. A MESS score of 7 or greater is highly predictive of eventual amputation. However, these scores are adjuncts, not absolutes; the ultimate decision rests on the surgeon's assessment of the feasibility of obtaining a sensate, functional limb versus the risk of subjecting the patient to years of reconstructive surgeries, chronic osteomyelitis, and opioid dependence.
Malignant bone and soft-tissue sarcomas of the lower extremity also represent a distinct category of indications. While limb-salvage surgery utilizing mega-prostheses or massive allografts has become the gold standard in orthopedic oncology, amputation remains indicated when the tumor encases major neurovascular bundles (e.g., the sciatic nerve or superficial femoral artery), when clear surgical margins cannot be obtained without rendering the limb completely functionless, or in cases of massive local recurrence following previous limb-sparing resections and radiation therapy.
| Category | Specific Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Dysvascular / Diabetic | Dry gangrene with intractable rest pain; Wet gangrene with ascending infection; Non-healing ulcers with chronic osteomyelitis failing revascularization. | Medically unstable patient in extremis (requires resuscitation prior to definitive surgery). | Inadequate proximal vascular perfusion to heal the selected amputation level (TcPO2 < 20 mmHg). |
| Trauma | Complete anatomic transection; Warm ischemia time > 6 hours with massive muscle necrosis; Unsalvageable sciatic/tibial nerve disruption with massive soft tissue loss. | Salvageable limb with isolated skeletal injury and intact plantar sensation in a hemodynamically stable patient. | Severe concomitant traumatic brain injury (may delay decision-making for functional assessment). |
| Infection | Gas gangrene (Clostridium perfringens); Rapidly progressive necrotizing fasciitis threatening systemic survival; Intractable chronic osteomyelitis. | None in the setting of life-threatening, ascending sepsis. | Mild, localized soft-tissue infection amenable to targeted debridement and intravenous antibiotics. |
| Oncology | High-grade sarcoma encasing the major neurovascular bundle; Massive local recurrence post-radiation; Fungating tumors with intractable bleeding/pain. | Metastatic disease where amputation will not improve quality of life or palliate symptoms. | Tumors completely resectable with negative margins while preserving a functional, sensate extremity. |
Pre-Operative Planning, Templating, and Patient Positioning
Because peripheral vascular disease is the primary driver of lower limb amputations, accurately determining the lowest anatomical level at which an amputation will reliably heal is paramount. Historically, this decision relied almost entirely on the surgeon's subjective clinical judgment of tissue bleeding, skin edge viability, and muscle contractility at the time of the initial incision. Today, while intraoperative judgment remains vital, it must be augmented by objective preoperative physiological testing to minimize the devastating complication of wound dehiscence and the need for revision to a higher level.
The cornerstone of preoperative vascular evaluation is the transcutaneous measurement of oxygen tension (TcPO2). While arteriography and CT angiography are the gold standards for mapping arterial anatomy for vascular bypass or endovascular intervention, they are notoriously poor at predicting actual capillary-level wound healing in the skin flaps. TcPO2 provides a direct, non-invasive assessment of local tissue microvascular perfusion. A TcPO2 threshold greater than 30 mm Hg generally predicts successful wound healing with over 90% accuracy, whereas values below 20 mm Hg are associated with a high rate of flap necrosis and failure. The predictive value of this test is significantly enhanced by utilizing an oxygen challenge: comparing baseline measurements with those obtained while the patient inhales 100% oxygen. A robust increase in local oxygen tension during inhalation indicates functional, recruitable microvascular perfusion and a high likelihood of primary healing.
Beyond vascularity, wound healing in the dysvascular, chronically infected, or catabolic patient is heavily dependent on systemic nutritional status and immunological reserve. Preoperative laboratory markers must be rigorously evaluated and, if time permits, optimized. Serum albumin is a critical marker of visceral protein status; levels greater than 3.0 g/dL are strongly predictive of successful healing, whereas levels below 2.5 g/dL correlate with a high incidence of wound breakdown. Similarly, the Total Lymphocyte Count (TLC) serves as a surrogate for both nutritional and immunological competence; a count greater than 1,500/µL indicates adequate reserve. If a patient presents with profound malnutrition, preoperative enteral or parenteral nutritional supplementation should be instituted, provided the clinical situation (e.g., active sepsis) allows for a delay in surgery.
Patient positioning and intraoperative setup require meticulous attention to detail. The patient is typically positioned supine on a radiolucent operating table. In cases of dysvascular amputation, the use of a pneumatic tourniquet is highly controversial and generally avoided. Inflating a tourniquet on a severely calcified, atherosclerotic vessel can cause intimal plaque rupture, leading to acute thrombosis of the remaining collateral vessels. Furthermore, the mechanical compression can cause irreversible ischemic injury to the marginal soft tissues required for flap closure. If a tourniquet is deemed absolutely necessary (e.g., in a trauma setting with massive hemorrhage), it should be applied as proximally as possible and inflated to the lowest effective pressure for the shortest possible duration.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a lower extremity amputation demands the same meticulous soft-tissue handling, precise osseous contouring, and rigorous hemostasis as a complex joint arthroplasty. Rough handling of ischemic tissues, aggressive use of self-retaining retractors, or failure to properly manage peripheral nerves will inevitably lead to wound failure, intractable phantom limb pain, and the inability to tolerate a prosthetic socket.
Foot and Ankle Amputations (Syme Ankle Disarticulation)
The Syme amputation is a technically demanding ankle disarticulation that involves the en bloc removal of the medial and lateral malleoli, preserving the articular surface of the distal tibial plafond, and repositioning the robust, specialized glabrous skin of the heel pad directly under the distal tibia. This creates an excellent, durable, end-bearing stump that allows the patient to ambulate short distances (e.g., to the bathroom at night) without a prosthesis.
However, the survival of the heel pad is entirely dependent on the pristine vascularity of the posterior tibial artery and its calcaneal branches. The incision is made from the tip of the lateral malleolus, across the anterior ankle joint to a point 1 cm below the tip of the medial malleolus, and then vertically straight down across the plantar aspect of the foot. The anterior structures are divided, the talus is plantarflexed, and the collateral ligaments are sharply released from the inside out to avoid damaging the posterior tibial neurovascular bundle. The calcaneus is meticulously shelled out of the heel pad subperiosteally. The malleoli are then resected flush with the tibial plafond. The heel pad is secured to the anterior tibial cortex via drill holes to prevent catastrophic posterior migration during weight-bearing.
Transtibial (Below-Knee) Amputations
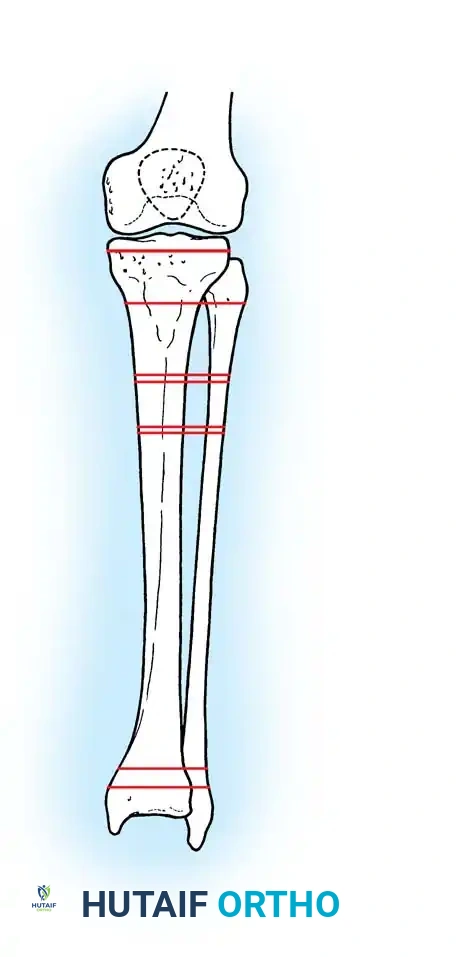
The transtibial amputation is the undisputed workhorse of lower extremity amputations. The ideal bone length is typically 12 to 15 cm distal to the medial joint line, which provides an optimal lever arm while allowing sufficient room distally for modern prosthetic componentry.
For ischemic limbs, the Burgess long posterior myocutaneous flap is the gold standard. The anterior incision is made transversely across the leg at the level of the planned tibial bone cut. The incision is carried laterally and medially to the mid-axial lines, and then extended distally to create a posterior flap that is 12 to 15 cm longer than the anterior incision. The anterior and lateral compartment muscles are transected flush with the bone cut.
The tibia is transected using an oscillating saw. Crucially, the anterior cortex of the tibia must be meticulously beveled at a 45-degree angle and smoothed with a rasp. Failure to bevel the tibia will result in a sharp cortical edge that will inevitably cause pressure necrosis through the overlying anterior skin flap when the patient is fitted with a prosthesis. The fibula is transected 1.0 to 1.5 cm proximal to the tibial cut to create a conical stump and prevent lateral prosthetic impingement.
Nerve management is paramount. The tibial, deep peroneal, superficial peroneal, and sural nerves must be systematically identified. They are dissected proximally, placed under gentle distal traction, sharply transected with a fresh scalpel blade, and allowed to retract deep into healthy, well-vascularized muscle beds. This prevents the formation of painful terminal neuromas at the weight-bearing interface. Finally, the posterior muscle mass (gastrocnemius and soleus) is thinned by excising the avascular soleus muscle. The robust gastrocnemius fascia is brought anteriorly and sutured directly to the anterior tibial periosteum via drill holes (myodesis) or to the anterior compartment fascia (myoplasty), providing a dynamic muscular cushion over the distal bone.
Disarticulation of the Knee
Knee disarticulation offers the advantage of a long, powerful lever arm and a broad, end-bearing surface provided by the distal femoral condyles. The surgical technique involves equal anterior and posterior flaps, or a long anterior flap if the patellar tendon is to be preserved. The patellar tendon is detached from the tibial tubercle, the collateral and cruciate ligaments are divided, and the knee is disarticulated. The patella is typically preserved and the patellar tendon is sutured to the remnant of the cruciate ligaments in the intercondylar notch, providing a robust distal soft-tissue envelope. While highly advantageous in non-ambulatory patients (providing a stable platform for sitting and a long lever arm for transfers), in ambulatory patients, the bulky femoral condyles make prosthetic fitting cosmetically challenging.
Transfemoral (Above-Knee) Amputations
When tissue viability precludes a transtibial amputation, a transfemoral amputation is required. The goal is to preserve as much femoral length as possible. Equal anterior and posterior fish-mouth flaps are typically utilized. The femur is transected, and the cortical edges are carefully smoothed.
The critical step in a transfemoral amputation is the adductor myodesis. The adductor magnus tendon must be isolated and securely anchored to the distal lateral femur via transosseous drill holes. This restores the mechanical tension of the adductor complex, countering the pull of the hip abductors and preventing the femur from drifting into severe abduction.
The sciatic nerve is isolated, and because of its large size and accompanying vasa nervorum, it must be securely ligated prior to sharp division to prevent massive postoperative hematoma. It is then allowed to retract deep beneath the hamstring muscles. The quadriceps and hamstring muscles are then grouped and sutured over the distal end of the femur (myoplasty) to complete the soft-tissue envelope.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, lower extremity amputations in the dysvascular population are associated with a high rate of postoperative complications. The intersection of severe peripheral ischemia, systemic immunocompromise, and the mechanical demands of the residual limb creates an environment ripe for wound failure and infection. Early recognition and aggressive salvage management are critical to preventing proximal revision.
Wound dehiscence and marginal flap necrosis are the most common early complications, occurring in up to 15% to 30% of dysvascular transtibial amputations. This is typically the result of inadequate preoperative vascular assessment, excessive tourniquet use, or suturing the skin under undue tension. If the necrosis is superficial, it can often be managed with advanced local wound care, negative pressure wound therapy (NPWT), and delayed secondary healing. However, if full-thickness necrosis exposes the underlying bone or myodesis, prompt return to the operating room for wedge resection, bone shortening, and primary closure is mandatory.
Phantom limb pain (PLP) and symptomatic neuromas represent the most debilitating long-term complications, severely limiting prosthetic wear and degrading the patient's quality of life. PLP, characterized by neuropathic burning, shooting, or crushing pain in the missing limb, occurs to some degree in up to 80% of amputees. While the etiology is a complex mix of peripheral nerve injury and central cortical reorganization, surgical prevention via meticulous nerve handling is the first line of defense. Modern salvage management for intractable neuromas involves Targeted Muscle Reinnervation (TMR), a microsurgical technique where the amputated nerve stumps are transferred and coapted to redundant motor branches of nearby intact muscles, giving the cut nerves "somewhere to go and something to do," thereby preventing neuroma formation and significantly reducing PLP.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Wound Dehiscence / Flap Necrosis | 15% - 30% | Ischemia, tight closure, hematoma, poor nutrition (Albumin < 3.0). | NPWT for superficial necrosis; Operative debridement and bone shortening for deep/exposed bone. |
| Surgical Site Infection | 10% - 20% | Contamination from distal gangrene, hematoma formation, diabetes. | Aggressive I&D, deep tissue cultures, targeted IV antibiotics, delayed primary closure. |
| Joint Flexion Contracture | 20% - 40% | Prolonged wheelchair use, failure to utilize RRD, poor positioning (pillows under knee). | Aggressive PT, dynamic splinting. Severe cases may require surgical release or proximal revision. |
| Symptomatic Neuroma / PLP | Up to 80% (PLP) | Inadequate nerve retraction, nerve tethering in scar tissue. | Pharmacologic (Gabapentinoids, SNRIs); Surgical excision and Targeted Muscle Reinnervation (TMR). |
| Bone Overgrowth | 10% - 15% (Pediatric) | Appositional bone growth at the transected diaphysis in children (most common in fibula). | Distal epiphyseal arrest; Stump capping (epiphyseal transplant); Surgical revision of the bone spike. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of the lower extremity amputee is a complex, multidisciplinary endeavor that begins immediately in the recovery room and continues for the remainder of the patient's life. The protocol is generally divided into three distinct phases: acute postoperative management, pre-prosthetic training, and definitive prosthetic rehabilitation. The ultimate goal is to return the patient to their maximal level of functional independence while protecting the fragile surgical reconstruction.
Phase 1 focuses on edema control, wound healing, and the absolute prevention of joint contractures. Transtibial amputees are at an exceptionally high risk for developing knee flexion contractures, as the hamstring muscles overpower the weakened quadriceps, especially when the patient is seated in a wheelchair. Transfemoral amputees are at risk for hip flexion and abduction contractures. Prevention mandates strict protocols: pillows must never be placed under the residual limb, and patients must engage in prone lying for at least 30 minutes, three times a day, to stretch the hip flexors.
For wound protection and edema control, Rigid Removable Dressings (RRDs) or Immediate Postoperative Prostheses (IPOP) are highly recommended and represent the standard of care in advanced centers. An RRD is a custom-molded plaster or fiberglass cast that protects the wound from direct trauma (e.g., falls), controls edema significantly more effectively than elastic soft bandages, and prevents knee flexion contractures. IPOPs take this a step further by attaching a pylon and foot to the rigid cast, allowing for immediate, touch-down weight-bearing, which dramatically accelerates the psychological adaptation to limb loss.
Phase 2, the pre-prosthetic phase, begins once the surgical incision has achieved primary healing and the sutures are removed (typically 3 to 4 weeks postoperatively). The focus shifts to aggressive residual limb desensitization, soft-tissue shaping, and core/upper extremity strengthening. Patients are instructed in deep friction massage of the healed incision to prevent tethering of the skin to the underlying bone. Shrinker socks are utilized 24 hours a day to compress the limb into a conical shape, driving out interstitial edema and preparing the limb for its first prosthetic socket.
Phase 3, prosthetic training, is initiated when the residual limb volume has stabilized. The modern prosthetic field has revolutionized amputee rehabilitation, transitioning from rudimentary wood and leather devices to advanced aerospace materials and robotics. Initial fittings utilize a "preparatory" or "check" socket made of clear plastic, allowing the prosthetist to visualize areas of blanching or excessive pressure. Modern definitive prostheses feature computer-assisted stump contour scanning for perfect socket fit, silicone or polyurethane gel liners that reduce shear forces and protect the skin, and carbon-fiber energy-storing ankle-foot systems (e.g., SACH or dynamic response feet). For transfemoral amputees, microprocessor-controlled knee units (e.g., the C-Leg) utilize onboard sensors and hydraulic dampening to dynamically adjust to the patient's gait speed, terrain, and stumble recovery, drastically reducing the metabolic cost of walking and the incidence of catastrophic falls.
Summary of Landmark Literature and Clinical Guidelines
The evolution of lower extremity amputation surgery is deeply rooted in landmark clinical literature that has continuously refined surgical technique and patient selection. Historically, amputations were performed as rapid guillotine procedures to save lives in the pre-antibiotic era. The transition to meticulous, reconstructive flap surgery was championed by Ernest Burgess in the late 1960s. Burgess's seminal work on the long posterior myocutaneous flap for transtibial amputations fundamentally changed the approach to the dysvascular patient, proving that utilizing the robust collateral blood supply of the sural artery to the gastrocnemius could reliably heal incisions over the poorly vascularized anterior tibia. This remains the gold standard technique globally.
In the realm of transfemoral amputations, the biomechanical necessity of the adductor myodesis was solidified by the extensive research of Gottschalk et al. in the 1990s. Their electromyographic and gait analysis studies conclusively demonstrated that failure to secure the adductor magnus to the distal femur results in a 70% loss of adductor power, leading to an uncompensated abductor lurch, massive increases in energy expenditure, and profound prosthetic instability. This literature established adductor myodesis not as an optional adjunct, but as a mandatory, non-negotiable step in transfemoral amputation technique.
More recently, the validation of trauma scoring systems like the MESS score by Johansen et al. provided trauma surgeons with the first objective, reproducible framework for deciding between limb salvage and primary amputation in the severely mangled extremity. Currently, clinical guidelines set forth by the American Academy of Orthopaedic Surgeons (AAOS) and the Department of Veterans Affairs (VA) strongly emphasize a multidisciplinary approach. Modern guidelines dictate that amputation surgery must be integrated with preoperative vascular optimization, immediate postoperative rigid dressings, and early involvement of physiatry and prosthetics to ensure the highest probability of returning the patient to functional bipedal ambulation. The integration of modern microsurgical techniques, such as Targeted Muscle Reinnervation (TMR) for neuroma management, represents the latest frontier in the literature, shifting the focus from mere survival to the optimization of the human-machine interface.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide