Masterclass in Digital Amputations: Principles and Flap Coverage
Key Takeaway
Finger amputations require meticulous soft-tissue handling, nerve management, and bone contouring to ensure a painless, functional stump. Treatment of fingertip amputations depends on defect size, exposed bone, and patient age. Techniques range from secondary intention healing to complex local advancements like Kutler and Atasoy V-Y flaps, or regional adipofascial turnover flaps, prioritizing length preservation, durable volar padding, and optimal sensory recovery.
Comprehensive Introduction and Patho-Epidemiology
The primary objective of any digital amputation—whether performed in the acute trauma setting or as a secondary reconstructive procedure—is to provide a painless, sensate, and highly functional stump. The human hand is an exquisitely specialized organ of interaction, serving as both a mechanical tool for powerful grasp and a highly refined sensory receptor for environmental exploration. Consequently, the surgical preservation of functional length must always be meticulously balanced against the absolute necessity of durable, well-padded, and sensate soft-tissue coverage. A poorly executed amputation that leaves a painful, dysesthetic, or mechanically unstable stump is a profound failure that can permanently disable the patient, leading to severe socioeconomic and psychological consequences.
Epidemiologically, digital amputations and severe fingertip injuries constitute a massive proportion of emergency orthopedic and plastic surgery consultations. Industrial accidents, particularly those involving heavy machinery, saws, and crush mechanisms, account for the majority of these injuries in the adult population, predominantly affecting young to middle-aged males. In the domestic setting, crush injuries from doors are notoriously common in the pediatric demographic, often presenting with complex nail bed lacerations and distal phalangeal tuft fractures. The mechanism of injury dictates not only the zone of trauma but also the viability of local tissues for reconstruction. Sharp, guillotine-type amputations present a distinct clinical entity compared to avulsion or severe crush injuries, where the zone of vascular intimal damage may extend far proximal to the obvious soft-tissue defect.
The modern orthopedic surgeon must approach digital amputation not merely as an ablative procedure, but as a definitive reconstructive operation. Historically, the prevailing dogma often prioritized the absolute preservation of length at all costs, frequently resulting in functionally useless, stiff, and painful digits. Contemporary surgical philosophy has shifted toward optimizing the global function of the hand. This paradigm shift requires a nuanced understanding of when to attempt complex flap coverage to preserve a critical functional unit (such as the thumb or the index finger in a manual laborer) and when a primary shortening and primary closure (reamputation) will yield a faster, more reliable return to work and daily activities.
Furthermore, the psychological impact of digital loss cannot be overstated. The hand is a highly visible anatomical structure, intimately tied to a patient's body image and non-verbal communication. Surgeons must engage in comprehensive preoperative counseling, managing patient expectations regarding aesthetic outcomes, sensory recovery, and the inevitable period of functional adaptation. The decision-making algorithm must incorporate the patient's age, hand dominance, occupation, avocation, and systemic comorbidities, such as diabetes mellitus or peripheral vascular disease, which profoundly influence wound healing and flap survival.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of digital anatomy is the absolute prerequisite for successful digital amputation and flap coverage. The integument of the digit is highly specialized and regionally distinct. The volar skin is glabrous (hairless), highly innervated, and uniquely tethered to the underlying distal phalanx by a complex network of dense fibrous septa. These septa compartmentalize the volar pulp fat, creating a specialized hydraulic cushion that resists shear forces during pinch and grasp. This volar pad is densely populated with mechanoreceptors, including Pacinian corpuscles (mediating high-frequency vibration and deep pressure) and Meissner's corpuscles (mediating light touch and low-frequency vibration), making it an irreplaceable sensory organ.

The vascular architecture of the digit is predicated on the proper digital arteries, which travel volar to the proper digital nerves within the neurovascular bundle. These arteries arborize extensively as they proceed distally, forming a robust cruciate anastomosis in the distal pulp and contributing to the subungual arcade. Understanding the spatial relationship of the neurovascular bundle is critical during flap elevation; the bundle is stabilized by Cleland’s ligaments (which are dorsal to the bundle and remain taut during flexion and extension) and Grayson’s ligaments (which are volar to the bundle and become lax during flexion). When mobilizing local advancement flaps, such as the Atasoy or Kutler flaps, selective release of these precise fibrous constraints is mandatory to achieve distal advancement without inducing devastating traction on the delicate vascular pedicle.
Tendon and Joint Biomechanics
The biomechanical interplay of the flexor and extensor mechanisms dictates the functional outcome of any amputation proximal to the distal interphalangeal (DIP) joint. The flexor digitorum profundus (FDP) inserts onto the volar base of the distal phalanx, while the terminal tendon of the extensor mechanism inserts onto the dorsal base. In amputations traversing the DIP joint or the middle phalanx, the management of these tendons is fraught with potential pitfalls. As a strict surgical rule, the flexor and extensor tendons must never be sutured together over the exposed bone end. This historical, deeply flawed practice tethers the deep flexor mechanism to the extensor apparatus. Because the FDP tendons to the ulnar three digits share a common muscle belly, tethering one tendon restricts the proximal excursion of the entire muscle unit. This phenomenon, known as the "Quadriga Effect," severely limits the active flexion of the adjacent, uninjured digits, effectively crippling the entire hand.
When an amputation occurs through an interphalangeal joint (either DIP or PIP), the intrinsic osseous anatomy presents a significant reconstructive challenge. The prominent flares of the phalangeal condyles are covered only by a thin layer of skin and subcutaneous tissue. If these condyles are not aggressively contoured with a rongeur and rasp, the resulting stump will be bulbous, "clubbed," and highly susceptible to skin breakdown and ulceration due to internal pressure against the surgical closure. The articular cartilage must also be meticulously excised to prevent the formation of painful synovial cysts and to encourage stable soft-tissue adherence to the cancellous bone bed.
Exhaustive Indications and Contraindications
The selection of the optimal surgical intervention for a digital amputation requires a sophisticated algorithmic approach, synthesizing the geometry of the defect, the level of amputation, the presence of exposed bone or tendon, and the patient's physiological profile. The following table delineates the precise indications and absolute or relative contraindications for the most frequently employed reconstructive strategies.
| Reconstructive Technique | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Secondary Intention | Pediatric fingertip injuries; Adult defects < 1 cm² without exposed bone/tendon; High surgical risk patients. | Exposed bone, joint, or tendon in adults; Defects > 1.5 cm²; Volar oblique amputations with significant pulp loss. |
| Primary Closure (Reamputation) | Severe crush injuries with non-viable local tissue; Elderly patients; Rheumatoid arthritis (where immobilization causes severe stiffness); Multiple severe hand injuries requiring rapid mobilization. | Thumb amputations (where length is paramount); Index finger in manual laborers; Clean, sharp amputations amenable to replantation. |
| Split-Thickness Skin Graft (STSG) | Large dorsal defects; Volar defects without exposed deep structures; Used to pull sensate pulp distally via graft contraction. | Exposed avascular bone (without periosteum); Exposed bare tendon; Weight-bearing or heavy pinch areas where durability is required. |
| Full-Thickness Skin Graft (FTSG) | Volar defects requiring durable coverage; Minimal contraction desired; Adequate vascular bed present. | Exposed bone or tendon; Heavily contaminated wounds; Active smokers (relative, due to poor inosculation risk). |
| V-Y Advancement Flaps (Atasoy/Kutler) | Transverse or dorsal oblique amputations with exposed bone; Need for sensate, durable distal padding. | Volar oblique amputations (insufficient volar tissue to advance); Extensive crush injuries to the remaining pulp; Severe peripheral vascular disease. |
| Cross-Finger Flap | Volar oblique amputations with exposed bone/tendon; Extensive volar pulp loss requiring durable, padded coverage. | Advanced age (risk of stiffness); Rheumatoid arthritis; Injury to the proposed donor digit; Unwillingness to tolerate a second stage division. |
Nuances in Decision Making
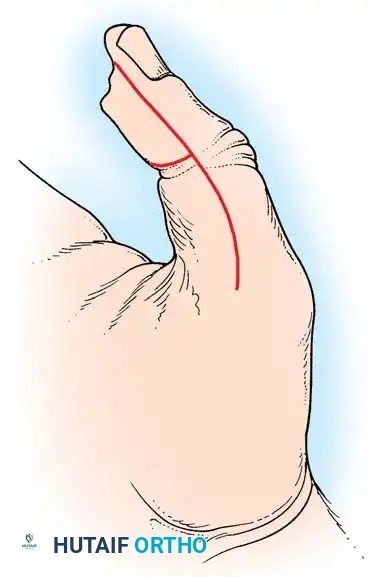
Amputations of the thumb represent a distinct reconstructive category. The thumb provides approximately 40-50% of total hand function, serving as the essential opposition post for all other digits. Therefore, the preservation of thumb length is an absolute priority. Reamputation and bone shortening should be vigorously avoided in the thumb unless absolutely dictated by massive tissue necrosis. Techniques such as the Moberg volar advancement flap, which can advance the entire volar skin of the thumb up to 1.5 cm due to its robust independent dorsal blood supply, are heavily favored.
Conversely, the index finger presents a different functional paradigm. An amputation proximal to the proximal interphalangeal (PIP) joint often results in a "bypassed" digit. The patient will subconsciously transfer pinch functions to the middle finger, rendering the shortened index stump an obstructive nuisance that gets in the way of power grip. In such scenarios, particularly for manual laborers, a ray amputation (excision of the digit and the corresponding metacarpal) may provide a vastly superior functional and aesthetic outcome compared to a short, stiff index stump.
Pre-Operative Planning, Templating, and Patient Positioning
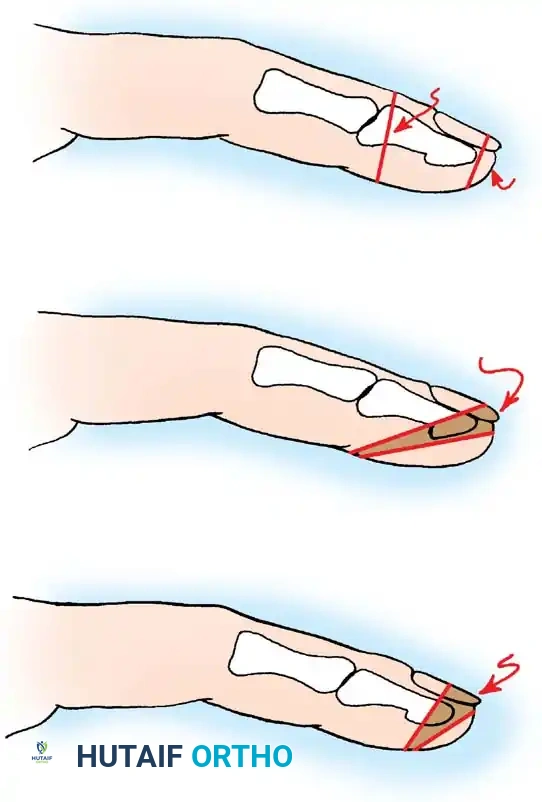
Meticulous preoperative planning is the cornerstone of successful digital reconstruction. The initial evaluation must take place in a well-lit environment, utilizing loupe magnification if necessary, to accurately assess the geometry of the defect. Fingertip amputations are classically categorized into transverse, dorsal oblique, and volar oblique patterns. This geometric classification directly dictates the reconstructive options. For example, a dorsal oblique defect leaves abundant volar pulp, making it the ideal candidate for an Atasoy volar V-Y advancement flap. In contrast, a volar oblique defect sacrifices the critical volar pad, necessitating regional coverage such as a cross-finger flap or a thenar flap to restore durable pinch mechanics.



Standard two-view radiographs (anteroposterior and true lateral) of the injured digit are mandatory. These images allow the surgeon to assess the exact level of osseous transection, the presence of associated fractures extending proximally into the shaft or articular surfaces, and the presence of radiopaque foreign bodies. Templating the anticipated bone resection is crucial; the surgeon must calculate exactly how much distal phalanx must be excised to allow tension-free soft-tissue closure, balancing this against the functional necessity of the remaining bone.
Anesthesia and Hemostatic Control
The choice of anesthesia profoundly impacts the surgical workflow and patient comfort. For isolated digital amputations, a comprehensive digital block utilizing a long-acting local anesthetic (e.g., 0.5% Bupivacaine mixed with 1% Lidocaine) provides excellent intraoperative anesthesia and prolonged postoperative pain relief. The block should be administered at the level of the metacarpal neck or the proximal web space to avoid volume compartment syndrome within the tight confines of the proximal phalanx. In cases requiring complex regional flaps (e.g., cross-finger flaps) or when the patient is highly anxious, a regional axillary or supraclavicular brachial plexus block is preferred.

A bloodless surgical field is an absolute requirement for the meticulous identification of neurovascular structures. A digital tourniquet (such as a sterile Penrose drain securely clamped at the base of the finger) is highly effective for short procedures lasting less than 30 minutes. However, for more complex flap mobilizations or when the amputation is proximal, a pneumatic forearm or upper arm tourniquet inflated to 250 mmHg is mandatory. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. The surgeon must be seated comfortably, with the operative field resting at the level of the surgeon's lower sternum to facilitate precise, microsurgical tissue handling.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a digital amputation or flap coverage demands rigorous adherence to atraumatic tissue handling principles. The use of fine-toothed forceps (e.g., Adson or Bishop-Harmon) should be restricted to the subdermal tissues; the delicate epidermal edges must be manipulated entirely with skin hooks to prevent crush necrosis.
General Principles of Terminal Amputation
Regardless of the specific flap utilized, several immutable steps apply to all digital amputations. First, the bone end must be addressed. Using a micro-sagittal saw or a sharp Luer rongeur, the bone is shortened just enough to allow the soft tissues to coapt without tension. The sharp cortical edges are then meticulously smoothed with a diamond rasp. If the amputation traverses the nail bed, the remaining germinal matrix must be completely ablated. Failure to aggressively curette or surgically excise the germinal matrix from the proximal eponychial fold will result in the growth of a painful, disfiguring "horn nail" or nail spicule.
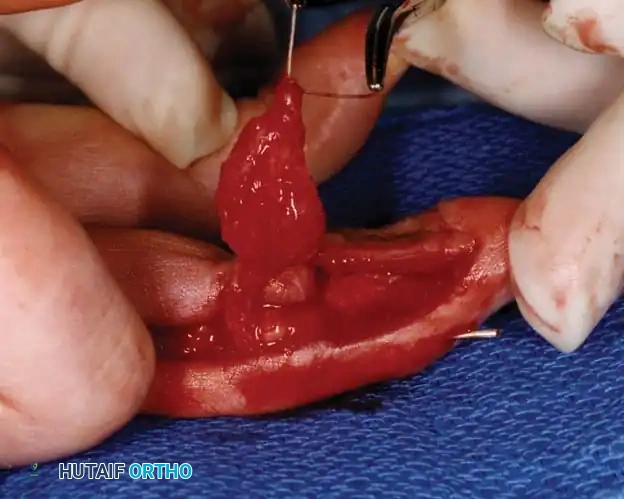
Nerve management is perhaps the most critical step in ensuring a painless stump. Neuromas at the transected nerve ends are physiologically inevitable as regenerating axons form a disorganized tangle of neural tissue. The surgical objective is to dictate where this neuroma forms. The digital nerves are identified, carefully dissected from the surrounding volar fat, and placed under gentle distal traction. The nerve is then sharply transected with a #15 blade or iris scissors at least 6 to 10 mm proximal to the bone end. Upon release of traction, the nerve retracts deep into the proximal soft tissues, ensuring the inevitable neuroma is shielded from the mechanical trauma of daily pinch and grasp.
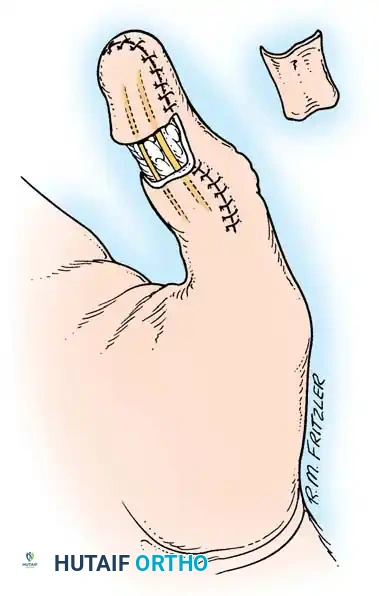
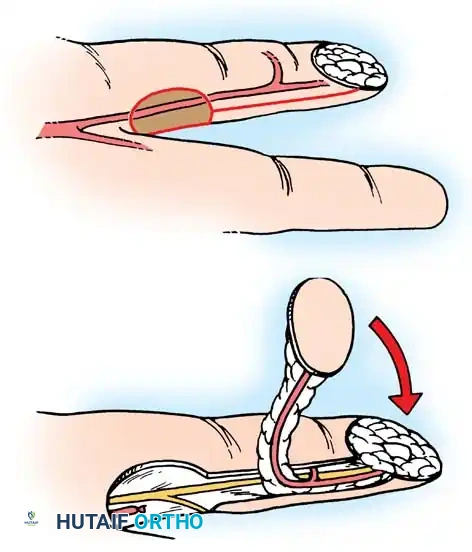
The Atasoy Volar V-Y Advancement Flap
The Atasoy technique is the undisputed workhorse for dorsal oblique fingertip amputations where the volar pulp remains largely intact.
- Design: Under tourniquet control, a distally based V-shaped incision is marked on the volar pulp. The distal base of the triangle must perfectly match the width of the defect (often the cut edge of the nail bed). The apex of the V extends proximally to the distal interphalangeal joint crease.
- Incision and Elevation: The skin is incised through the dermis only. The critical step is the mobilization of the flap. Using tenotomy scissors, the surgeon carefully spreads and selectively divides the vertical fibrous septa that tether the volar fat pad to the underlying flexor tendon sheath and distal phalangeal periosteum.
- Preservation of Neurovascular Supply: The blood supply to this flap is entirely dependent on the arborizing branches of the proper digital arteries entering the flap from the lateral aspects. Deep dissection must remain central, meticulously avoiding the lateral neurovascular bundles.
- Advancement and Closure: Once adequately released, the flap will passively slide distally like a visor. The distal edge is sutured to the sterile matrix or the dorsal skin edge using 5-0 chromic gut or nylon. The proximal V-shaped defect is then closed primarily in a Y-configuration, effectively pushing the flap distally.
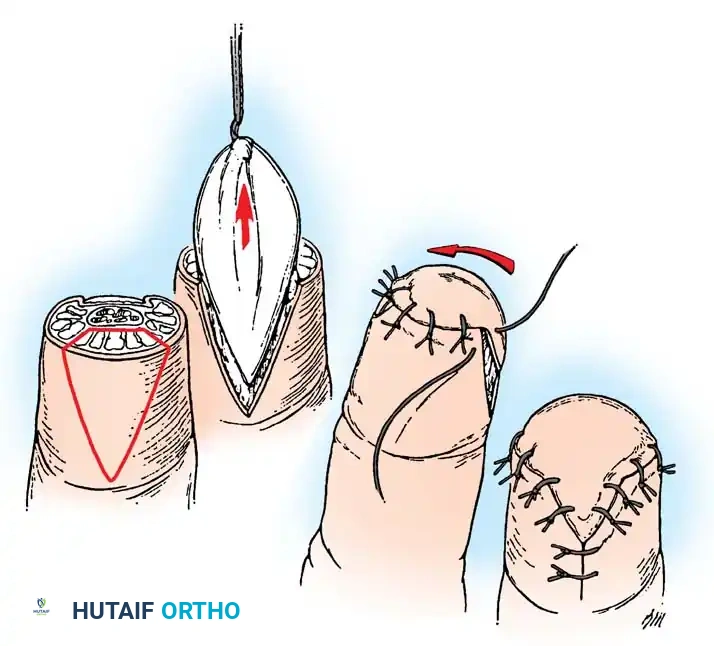
The Kutler Bilateral V-Y Advancement Flap
The Kutler flap is reserved for transverse or slightly volar-oblique amputations where a single volar flap provides insufficient coverage.
- Design: Two distinct triangular flaps are designed on the mid-lateral aspects of the injured digit. The apices point proximally, and the bases are located at the distal wound margin.
- Mobilization: The incisions are carried down through the dermis. A skin hook is placed at the apex of each triangle, applying gentle distal traction. The fibrous septa tethering the deep surface of the flap to the phalangeal periosteum are delicately snipped.
- Advancement: As the septa are released, the lateral flaps mobilize distally. Extreme caution is required to avoid strangulating the microscopic vascular pedicles entering the deep surface of the flaps.
- Closure: The two flaps are advanced over the bone end and sutured to each other in the midline. The dorsal and volar aspects are sutured to the remaining nail bed and volar skin, respectively. The proximal donor defects are closed in a Y-configuration.
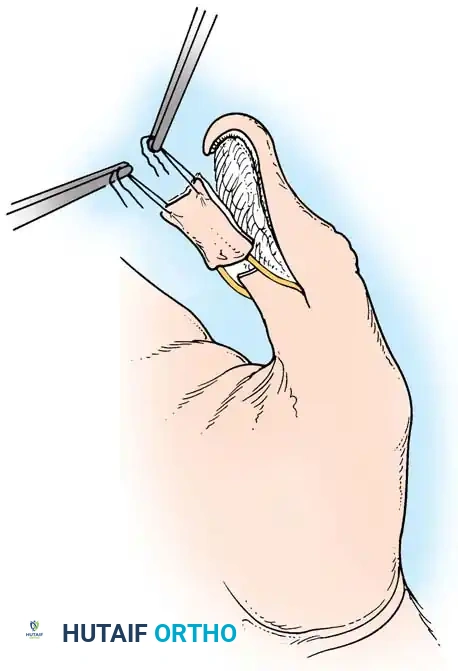

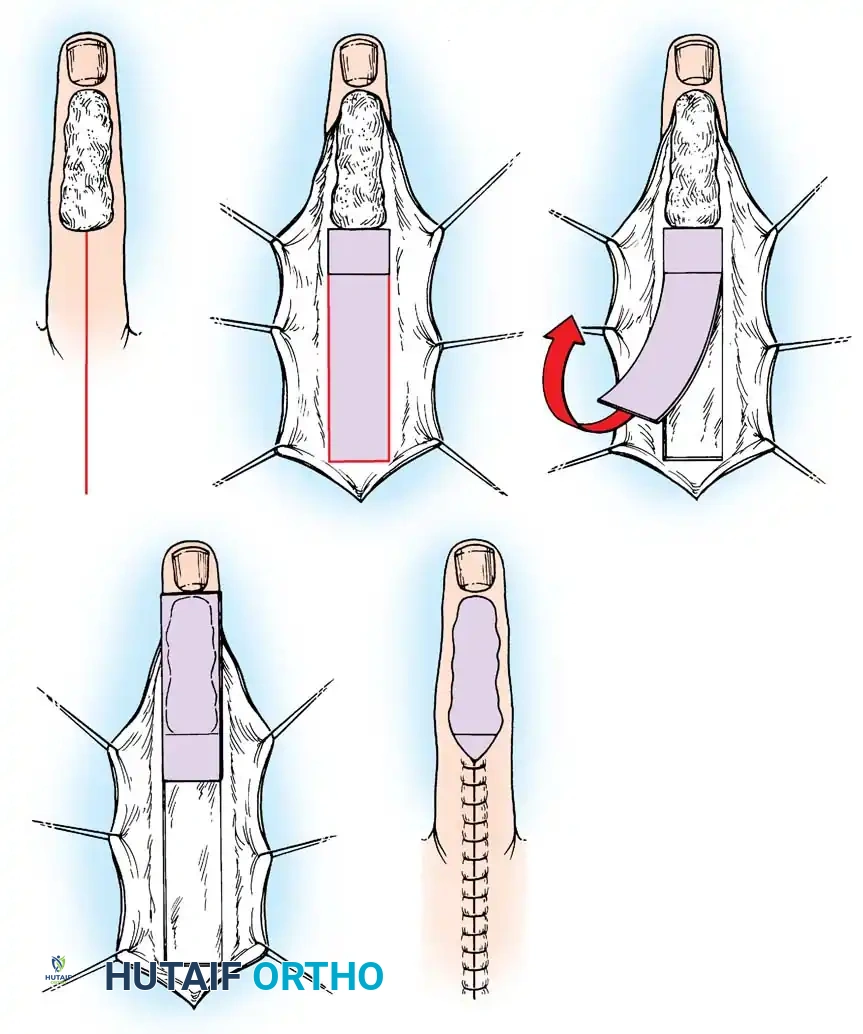
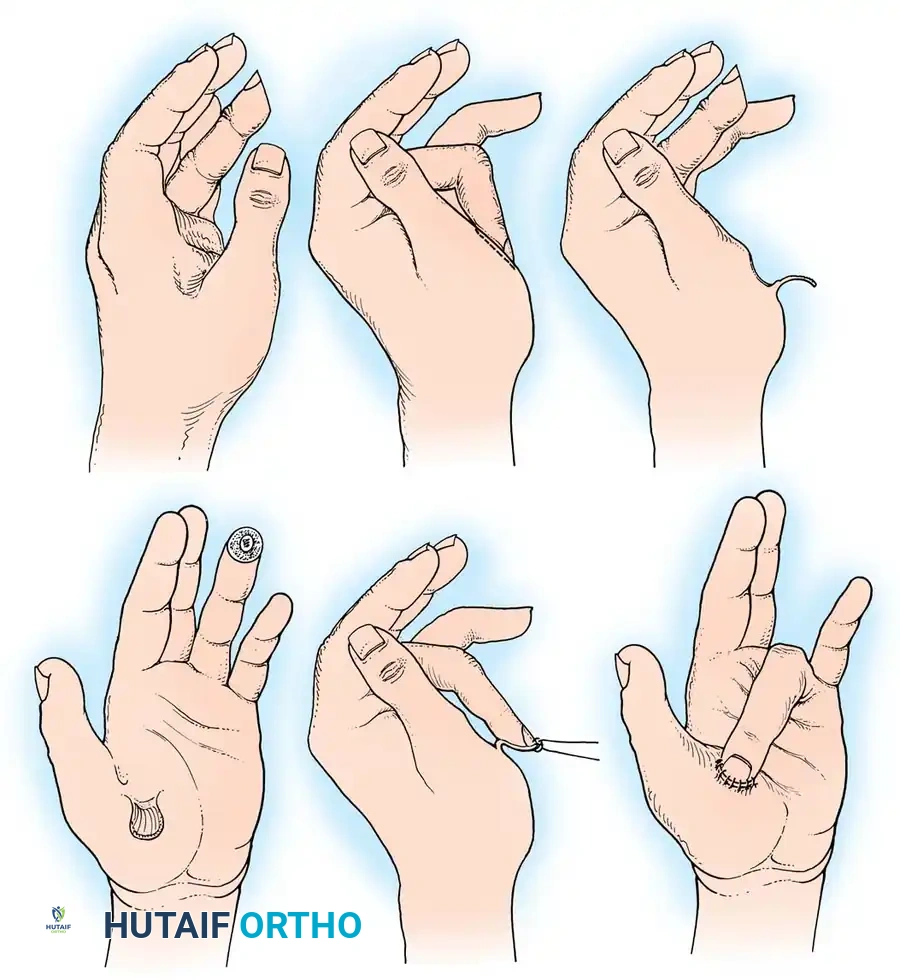
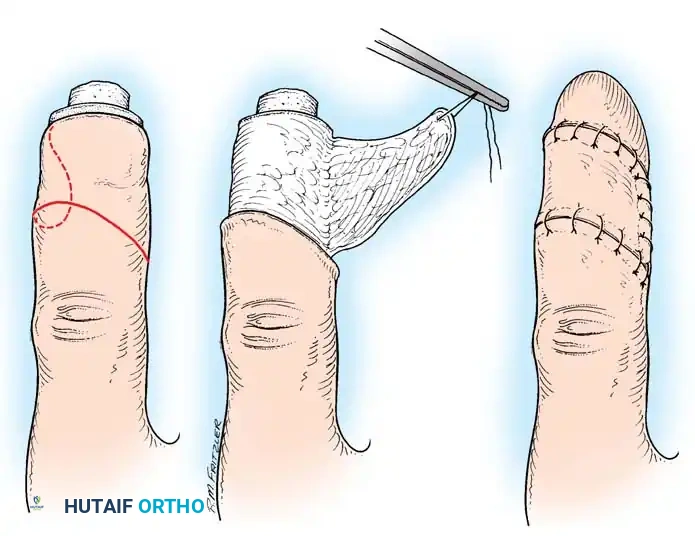
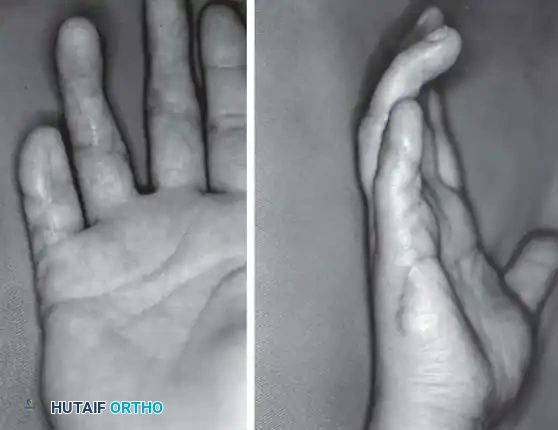
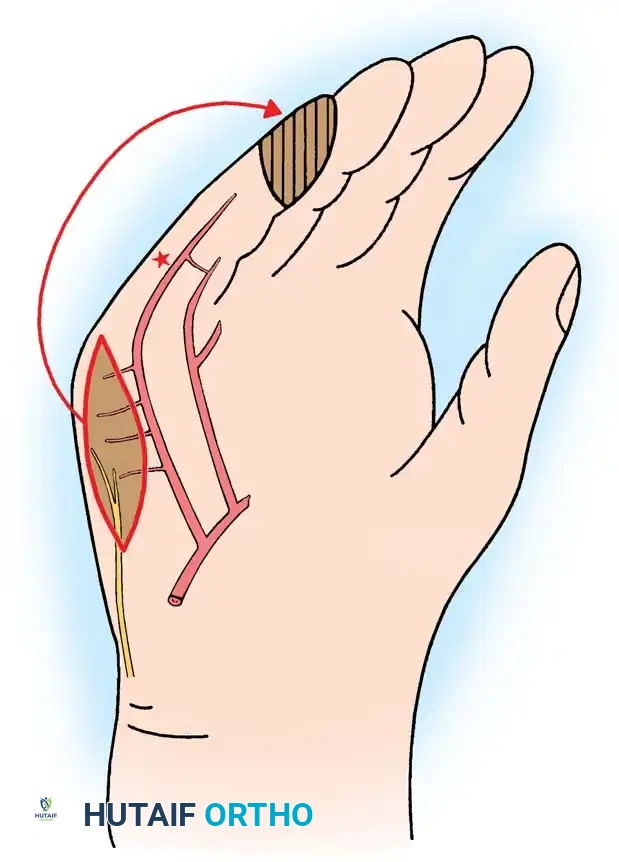
Regional Flap Coverage: The Cross-Finger Flap
When local advancement flaps are insufficient, particularly in severe volar oblique amputations exposing the flexor tendon or extensive bone, the cross-finger flap provides robust, durable coverage. This is a two-stage procedure utilizing the dorsal skin and subcutaneous tissue of an adjacent, uninjured digit.
- Stage 1 (Elevation): A laterally based rectangular flap is designed on the dorsum of the middle phalanx of the adjacent donor digit. The flap is elevated in the plane between the subcutaneous fat and the paratenon of the extensor mechanism. It is imperative that the paratenon remains intact to accept a skin graft.
- Transfer: The flap is flipped over like the page of a book and sutured into the volar defect of the injured digit.
- Donor Site Coverage: A full-thickness skin graft (often harvested from the volar wrist crease) is placed over the intact paratenon of the donor digit.
- Stage 2 (Division): The digits are immobilized together for 14 to 21 days to allow neovascularization. At 3 weeks, the pedicle is sharply divided, and the margins are inset.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, digital amputations carry a significant risk of postoperative complications. The hand is highly sensitive to edema, immobilization, and altered biomechanics. Early recognition and aggressive management of these complications are essential to salvage a functional outcome and prevent chronic disability.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage & Management Strategy |
|---|---|---|---|
| Symptomatic Neuroma | 10% - 20% | Failure to perform adequate traction neurectomy; neuroma forms in a superficial, contact-bearing area. | Conservative: Desensitization therapy, gabapentin. Surgical: Excision and proximal burying into muscle/bone, or Targeted Muscle Reinnervation (TMR). |
| Hook Nail Deformity | 15% - 25% | Inadequate bony support for the nail bed; the nail curves volarly over the amputated stump. | Ablation of the entire nail matrix; Reamputation with further bone shortening; Microvascular free tissue transfer for severe cases. |
| Flap Necrosis | 5% - 10% | Excessive tension on closure; strangulation of pedicle during V-Y advancement; systemic factors (smoking, diabetes). | Early: Release sutures, apply nitroglycerin paste, optimize hemodynamics. Late: Debridement and healing by secondary intention or revision flap. |
| Joint Stiffness | 30% - 50% | Prolonged immobilization; edema-induced fibrosis of collateral ligaments; "Quadriga Effect" from tethered tendons. | Aggressive hand therapy, dynamic splinting. Surgical tenolysis or capsulotomy for refractory cases > 6 months post-op. |
| Cold Intolerance | 40% - 60% | Disruption of normal thermoregulatory vascular shunts; sympathetic nervous system hypersensitivity. | Usually self-limiting over 1-2 years. Management includes warm clothing, biofeedback, and avoidance of cold exposure. Calcium channel blockers in severe cases. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 5% | Abnormal autonomic nervous system response to trauma/surgery; severe pain out of proportion to injury. | Multidisciplinary approach: Aggressive physical therapy, neuropathic pain modulators, sympathetic nerve blocks, Vitamin C prophylaxis. |

Deep Dive: Managing the Symptomatic Neuroma
The symptomatic neuroma remains the most debilitating complication following digital amputation. When a patient presents with exquisite, localized point tenderness and a positive Tinel's sign at the stump, a neuroma must be suspected. Initial management is always non-operative, relying heavily on specialized hand therapy. Desensitization protocols—utilizing fluidotherapy, varied texture massage, and percussion—aim to increase the patient's pain threshold through central nervous system habituation.
If conservative measures fail after 3 to 6 months, surgical intervention is warranted. The revision surgery involves exploring the stump, identifying the bulbous neuroma, and sharply excising it. The critical step is the subsequent management of the fresh nerve end. Modern techniques advocate for transposing the nerve end proximally into a deep, well-vascularized, non-contact environment. This can be achieved by burying the nerve deep into the lumbrical muscle belly or drilling a small cortical window into the proximal phalanx and burying the nerve end directly into the medullary canal. More recently, Targeted Muscle Reinnervation (TMR), where the cut nerve is coapted to a nearby expendable motor branch, has shown immense promise in preventing neuroma recurrence by providing the regenerating axons with "somewhere to go and something to do."

Phased Post-Operative Rehabilitation Protocols
The surgical procedure represents only the first half of the reconstructive journey; rigorous, phased postoperative rehabilitation is paramount to achieving an optimal functional outcome. The hand is notoriously unforgiving of prolonged immobilization, rapidly developing dense capsular contractures and tendon adhesions. A close, collaborative relationship between the orthopedic surgeon and a certified hand therapist (CHT) is essential.
Phase I: Protection and Edema Control (Weeks 0-2)
Immediately postoperatively, the digit is dressed with non-adherent gauze (e.g., Adaptic or Xeroform) and a bulky, compressive soft dressing to minimize hematoma formation. The hand is elevated continuously above the level of the heart. For simple amputations or local V-Y flaps, the initial dressing is removed at 3 to 5 days. Early, gentle active range of motion (AROM) of all uninvolved joints (shoulder, elbow, wrist, and adjacent digits) is initiated immediately to prevent proximal stiffness and facilitate venous and lymphatic return. The operative digit is protected with a custom-molded thermoplastic splint, typically in an intrinsic-plus position (MCP joints flexed 70 degrees, IP joints fully extended) if proximal immobilization is required.
Phase II: Wound Healing and Desensitization (Weeks 2-6)
Sutures are typically removed between 10 and 14 days, provided the flap margins demonstrate robust healing. Once the wound is completely epithelialized, aggressive desensitization protocols commence. Patients are instructed to massage the stump with varying textures (cotton, silk, Velcro) and immerse the digit in a fluidotherapy unit or contrast baths. Active and active-assisted range of motion of the involved digit is aggressively pursued. Tendon gliding exercises are emphasized to prevent adhesions between the flexor mechanism and the amputation stump. If the patient develops early signs of CRPS (erythema, hyperhidrosis, disproportionate pain), mirror visual feedback therapy is initiated immediately to reorganize the cortical somatosensory mapping.
Phase III: Strengthening and Work Hardening (Weeks 6+)
By six weeks, the soft tissues should be stable, and the bony architecture healed (if fractures were present). Therapy transitions toward functional restoration. Progressive resistance exercises utilizing therapy putty, grip strengtheners, and functional task simulation are introduced. For manual laborers, a specialized work-hardening program is essential to simulate the specific mechanical demands of their occupation. Scar management continues with silicone gel sheeting and deep friction massage to ensure the volar pad remains pliable and mobile over the underlying distal phalanx. Maximum medical improvement (MMI) is typically not reached until 6 to 12 months post-injury, particularly concerning sensory re-education and the resolution of cold intolerance.
Summary of Landmark Literature and Clinical Guidelines
The evolution of digital amputation and flap coverage is deeply rooted in several landmark anatomical and clinical studies that continue to dictate modern surgical practice. A thorough understanding of this literature is essential for any reconstructive surgeon.
The foundational principles of local advancement flaps were established by Kutler in 1947, who first described the bilateral V-Y advancement for transverse fingertip amput
