Masterclass in Foot Amputations: Surgical Techniques and Biomechanics

Key Takeaway
Amputations of the foot and ankle are critical reconstructive procedures rather than treatment failures. Success depends on meticulous soft tissue handling, preoperative vascular assessment, and optimization of nutritional status. This guide details the biomechanical implications, indications, and step-by-step surgical techniques for toe amputations, ray resections, and metatarsophalangeal disarticulations, providing orthopedic surgeons with evidence-based protocols to maximize functional outcomes and limb salvage.
Comprehensive Introduction and Patho-Epidemiology
Amputations around the foot and ankle are becoming increasingly prevalent, driven largely by the rising global incidence of diabetic neuropathy, peripheral vascular disease (PVD), and end-stage renal disease (ESRD). Historically viewed by both patients and surgeons as a definitive failure of medical management or limb salvage efforts, ablation by amputation or disarticulation must instead be conceptualized as a definitive, life-enhancing reconstructive procedure. The primary goal of any lower extremity amputation is to eradicate fulminant infection, remove ischemic or necrotic tissue, and meticulously create a stable, durable, and biomechanically sound residual limb that maximizes the patient's functional independence and mobility.
The patho-epidemiology of the diabetic foot is a complex triad of neuropathy (sensory, motor, and autonomic), ischemia, and altered immunopathy. Motor neuropathy leads to intrinsic muscle wasting, creating dynamic imbalances that result in characteristic deformities such as claw toes and prominent metatarsal heads. Sensory neuropathy removes the protective feedback mechanism, allowing repetitive microtrauma to evolve into full-thickness ulcerations. Concurrently, autonomic neuropathy causes localized anhidrosis, leading to dry, fissured skin that serves as a portal of entry for polymicrobial infections. When coupled with macrovascular and microvascular arterial insufficiency, the tissue's ability to heal is profoundly compromised, frequently necessitating surgical ablation.
With advanced modalities in vascular perfusion assessment, sophisticated orthotic design, and modern footwear modifications, the success rates of partial foot amputations have improved significantly over the last two decades. However, patients requiring distal amputations frequently present with complex, multi-systemic medical comorbidities, including coronary artery disease, chronic kidney disease, and profound malnutrition. Consequently, the orthopedic surgeon must exercise exceptional clinical judgment regarding the precise level of amputation, meticulous soft tissue handling, and rigorous postoperative wound management to prevent proximal revision.
Clinical Pearl: Avoidance of excessive pressure on the skin edges is paramount. Never use toothed forceps (e.g., Adson forceps) on the skin edges of a dysvascular patient. Utilize skin hooks or stay sutures, employ thick fasciocutaneous flaps, refrain from tourniquet use when possible to avoid ischemic reperfusion injury, and ensure meticulous hemostasis to prevent hematoma formation and subsequent flap necrosis.
Detailed Surgical Anatomy and Biomechanics
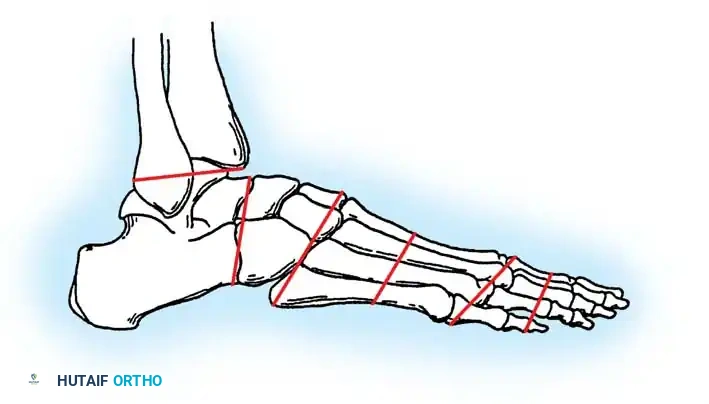
A profound understanding of the surgical anatomy and biomechanics of the foot is non-negotiable when planning partial foot amputations. The vascular supply to the foot is classically described by the angiosome concept, pioneered by Taylor and Palmer. The foot is divided into distinct three-dimensional blocks of tissue supplied by specific source arteries: the posterior tibial artery (calcaneal, medial plantar, and lateral plantar branches), the anterior tibial artery (dorsalis pedis), and the peroneal artery. Recognizing which angiosome is compromised allows the surgeon to design flaps based on the most robust remaining arterial inflow, utilizing collateral "choke" vessels to sustain the soft tissue envelope.

Biomechanically, the foot acts as both a flexible shock absorber during initial heel strike and a rigid lever arm during terminal stance and push-off. This transition is mediated by the windlass mechanism, whereby dorsiflexion of the hallux tightens the plantar fascia, elevating the longitudinal arch and locking the midtarsal joints. Amputation of the great toe (hallux) does not severely impair standing or slow walking; however, because the hallux provides the primary fulcrum for the windlass mechanism and terminal push-off, rapid walking, running, or ascending stairs will result in a noticeable, energy-inefficient limp.
Amputations proximal to the metatarsal heads become increasingly disabling due to the exponential loss of the anterior lever arm. Midfoot amputations (such as Lisfranc and Chopart disarticulations) historically carried unacceptably high failure rates due to severe biomechanical imbalances. Severing the dorsal insertions of the primary dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus) leaves the powerful posterior plantarflexors (triceps surae) entirely unopposed.

This unopposed pull inevitably leads to a severe, rigid equinus deformity. As the talus plantarflexes, the anterior distal stump is driven directly into the ground during the stance phase of gait, resulting in catastrophic distal stump breakdown, recurrent ulceration, and deep space infection. To prevent this, simultaneous percutaneous Tendo-Achilles Lengthening (TAL) or formal heel cord tenotomy is absolutely mandatory during midfoot amputations, neutralizing the deforming forces and preserving the plantigrade alignment of the residual stump.
Exhaustive Indications and Contraindications
The decision to proceed with a specific level of amputation requires a delicate balance between preserving maximal limb length for biomechanical advantage and ensuring the selected level has adequate perfusion to achieve primary wound healing. The indications for partial foot amputation are broad but generally fall into categories of infection, ischemia, trauma, or tumor.
In the diabetic and dysvascular population, the most common indication is a non-healing neuroischemic ulcer complicated by deep space infection or osteomyelitis that has failed aggressive conservative management and targeted antimicrobial therapy. Wet gangrene, characterized by active infection superimposed on ischemic tissue, represents a surgical emergency requiring immediate guillotine amputation or wide debridement to control ascending sepsis, followed by definitive reconstructive amputation once the patient is physiologically stabilized.
Contraindications to partial foot amputation are primarily dictated by inadequate vascular inflow. Attempting a distal amputation in a zone of profound ischemia guarantees wound dehiscence, necrosis, and the need for a higher-level revision, subjecting the patient to unnecessary physiological stress and prolonged hospitalization. Furthermore, severe systemic sepsis, profound malnutrition, or a non-ambulatory baseline status may push the surgeon toward a more proximal, definitive amputation (e.g., Transtibial or Transfemoral) to ensure rapid healing and minimize the risk of recurrent foot complications.
| Clinical Scenario | Primary Indication | Relative Contraindication | Preferred Amputation Level |
|---|---|---|---|
| Localized Osteomyelitis (Distal Phalanx) | Eradication of localized bone infection | Proximal soft tissue cellulitis | Distal Syme or PIP Joint Disarticulation |
| Wet Gangrene of 2nd Digit | Source control of ascending infection | Severe ischemia (tcPO2 < 20 mmHg) | Ray Amputation (with delayed primary closure) |
| Global Forefoot Ischemia / Dry Gangrene | Ablation of non-viable tissue | Uncorrectable iliac/femoral occlusion | Transmetatarsal Amputation (TMA) |
| Charcot Midfoot Collapse with Ulceration | Unbraceable, unstable deformity | Active systemic bacteremia | Midfoot (Chopart) + TAL or Syme Amputation |
| Malignant Melanoma (Subungual) | Oncologic resection (wide margins) | Metastatic disease (palliative care preferred) | MTP Disarticulation or Ray Amputation |

Pre-Operative Planning, Templating, and Patient Positioning
The preoperative assessment is arguably the most critical phase of the amputation process. The decision to proceed with a specific level relies heavily on predicting the healing potential of the residual soft tissue envelope. Clinical examination—including the assessment of palpable pulses, capillary refill, skin temperature, dependent rubor, and absence of hair growth—is essential but wholly insufficient in isolation. Objective non-invasive vascular testing is mandatory for all dysvascular patients.
Vascular assessment must be multi-modal. The Ankle-Brachial Index (ABI) is standard; an ABI > 0.45 generally suggests adequate perfusion for healing. However, diabetic patients and those with ESRD frequently exhibit medial arterial calcinosis (Mönckeberg's sclerosis), resulting in falsely elevated, incompressible vessels (ABI > 1.3). In these scenarios, Toe Pressures become critical; a toe pressure greater than 45 mm Hg strongly correlates with successful wound healing. Furthermore, Transcutaneous Oximetry (tcPO2) provides a direct measure of tissue oxygenation. A tcPO2 > 30 mm Hg indicates a high probability of healing, whereas a tcPO2 < 20 mm Hg indicates severe ischemia, necessitating preoperative vascular bypass or endovascular angioplasty before any elective amputation is attempted.

Nutritional optimization is a critical, yet frequently overlooked, determinant of surgical success. Landmark studies by Dickhaut et al. demonstrated that specific serologic markers are highly predictive of amputation healing. Serum Albumin levels < 3.5 g/dL correlate with poor healing, while a Total Lymphocyte Count (TLC) < 1500/µL indicates severe malnutrition and immunocompromise, drastically increasing failure rates. A healing rate of over 80% can be achieved when TLC > 1500/µL and Albumin ≥ 3.5 g/dL. Patients falling below these thresholds require aggressive dietary supplementation or enteral feeding prior to elective surgery.
Patient positioning is typically supine with a bump placed under the ipsilateral hip to internally rotate the leg to a neutral position, allowing circumferential access to the foot. In dysvascular patients, the use of a pneumatic tourniquet is highly controversial and generally discouraged. Tourniquet inflation can cause severe ischemic reperfusion injury, shear calcified atheromatous plaques, and precipitate acute arterial thrombosis. If a tourniquet is absolutely necessary for visualization during a complex midfoot reconstruction, it should be inflated to the lowest effective pressure for the shortest possible duration, and the limb should be exsanguinated by elevation rather than aggressive Esmarch wrapping.
Step-by-Step Surgical Approach and Fixation Technique
Surgical technique in the dysvascular foot requires a paradigm shift from standard orthopedic trauma principles. The tissue is unforgiving; rough handling, excessive electrocautery, and tension on closure will unequivocally lead to flap necrosis.
Technique 1: Standard Amputation of a Digit
This technique is utilized for definitive ablation of a severely infected, ischemic, or deformed digit where bone preservation is not viable. Flap design is paramount: fashion a long plantar and a short dorsal skin flap. The plantar skin is highly specialized for weight-bearing, containing fibrous septa that stabilize the epidermis against shear forces.

Begin the incision at the intended level of bone resection at the medial midpoint of the toe, curving it dorsally to the lateral midpoint. Create a corresponding plantar flap, ensuring it is slightly longer than the dorsoplantar diameter of the toe to allow tension-free closure over the bone stump. Elevate the skin flaps proximally using a strict "no-touch" technique on the epidermal edges—utilize skin hooks rather than forceps. Divide the flexor and extensor tendons under tension, allowing them to retract deep into the proximal soft tissues to prevent tethering. Isolate the digital nerves, apply gentle distal traction, section them sharply, and allow them to retract proximally into healthy soft tissue to prevent painful neuroma formation at the weight-bearing stump. Section the phalanx at the selected level using an oscillating microsaw, and crucially, smooth the distal bone end with a rasp to remove any sharp prominences.
Technique 2: Amputation at the Base of the Proximal Phalanx
Whenever oncologically and physiologically possible, maintaining the base of the proximal phalanx is biomechanically superior to a complete MTP joint disarticulation. Retaining at least 1 cm of the proximal phalanx preserves the insertion of the plantar fascia and the intrinsic musculature (e.g., flexor hallucis brevis in the great toe).
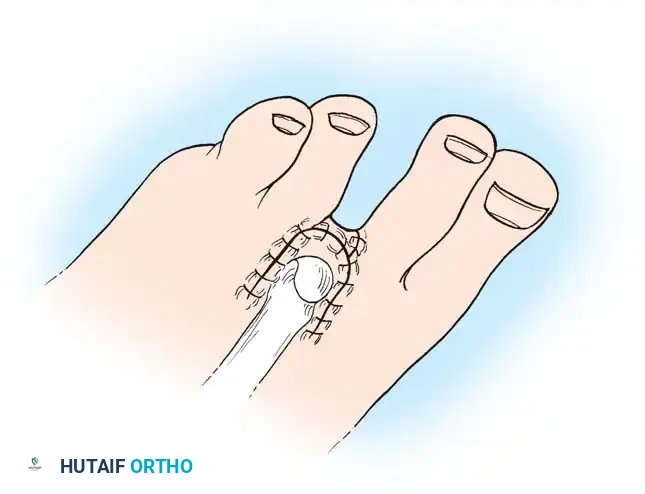
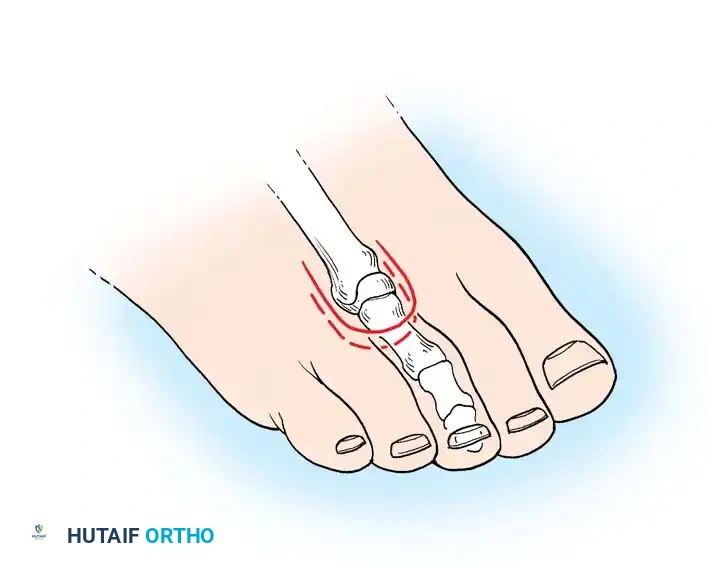
For the great toe, create a long posteromedial flap. For lesser toes, utilize a short dorsal racquet-shaped incision starting 1 cm proximal to the MTP joint. Reflect the flaps proximally, transect tendons, and perform traction neurectomies. Resect the proximal phalanx ensuring the base remains, contour the bone meticulously, and approximate the skin edges with interrupted nonabsorbable sutures (e.g., 3-0 or 4-0 nylon).
Technique 3: Metatarsophalangeal Joint Disarticulation and Ray Amputation
Disarticulation at the MTP joint is indicated in profound ischemia or osteomyelitis extending into the proximal phalanx. The approach mirrors the proximal phalanx amputation but requires a significantly longer plantar flap to cover the bulky metatarsal head.
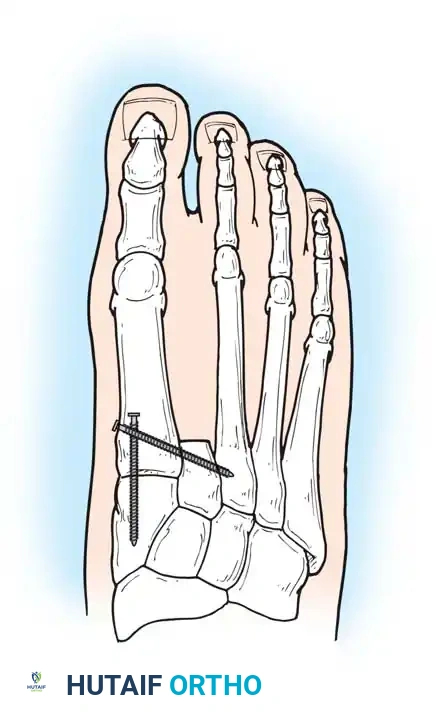
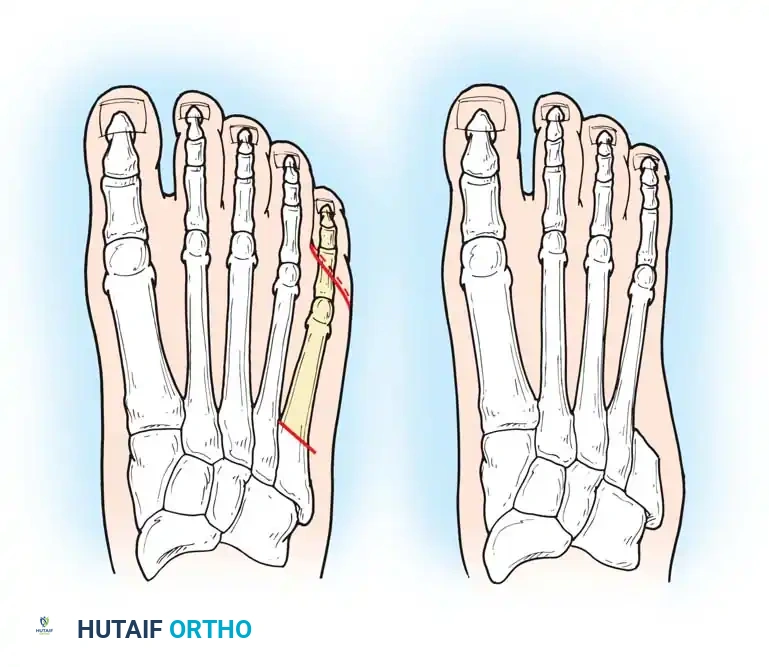
In cases where the metatarsal head is severely prominent, atrophic, or if skin tension is excessive, a ray amputation (resection of the digit and the distal metatarsal) is performed. Amputation of the second toe frequently results in severe hallux valgus, as the great toe naturally drifts laterally into the void left by the resected second ray.


Surgical Warning: To prevent severe hallux valgus following a second ray amputation, Smith recommended a complete second ray resection combined with surgical narrowing of the foot using transverse screw fixation between the first and third metatarsals.
Technique 4: Transmetatarsal Amputation (TMA)
The TMA is a highly functional, durable amputation level that preserves the insertions of the tibialis anterior and peroneus brevis, maintaining active dorsiflexion and a balanced foot. A long, thick plantar flap is designed extending to the metatarsal necks. The dorsal incision is made straight across the mid-shaft of the metatarsals. The metatarsals are osteotomized with a saw, typically with a slight dorsal-to-plantar bevel, and the lateral metatarsals are cut slightly shorter to mirror the natural cascade of the foot. The plantar flap is then rotated dorsally. As previously emphasized, a prophylactic percutaneous Achilles tendon lengthening is routinely performed to eliminate any equinus forces that could compromise the distal dorsal suture line.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and comprehensive preoperative optimization, complications following partial foot amputations in the dysvascular population remain high. The surgeon must be prepared to aggressively manage these complications to prevent proximal limb loss.
Wound dehiscence and flap necrosis are the most common early complications, typically resulting from unrecognized arterial insufficiency, excessive tension on the suture line, or postoperative hematoma formation. Hematomas act as an ideal culture medium for bacteria and increase localized pressure, leading to ischemic necrosis of the overlying skin. If a hematoma is suspected, early evacuation is mandatory.

Deep space infection and recurrent osteomyelitis usually present in the subacute phase. This is frequently due to inadequate initial debridement, leaving behind microscopic foci of infected bone, or failure to denude the avascular articular cartilage during a disarticulation, which prevents vascularized granulation tissue from forming. Salvage requires a return to the operating room for further proximal bone resection, aggressive pulse-lavage irrigation, and potentially the placement of antibiotic-impregnated polymethylmethacrylate (PMMA) beads or spacers.
Biomechanical complications, such as the aforementioned equinus deformity or progressive hallux valgus, lead to new pressure points and recurrent ulceration. A rigid equinus deformity that develops postoperatively due to failure to perform a prophylactic TAL will rapidly cause ulceration at the distal anterior stump.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management / Revision Strategy |
|---|---|---|---|
| Flap Necrosis / Dehiscence | 15% - 30% | Ischemia, tight closure, hematoma | Debridement, negative pressure wound therapy (NPWT), or revision to higher level |
| Recurrent Osteomyelitis | 10% - 20% | Inadequate resection margins | Proximal bone resection, prolonged IV antibiotics, infectious disease consult |
| Equinus Deformity | 25% (if no TAL) | Unopposed triceps surae pull | Formal open Achilles Z-lengthening, total contact casting, orthotic AFO |
| Symptomatic Neuroma | 5% - 10% | Failure to perform traction neurectomy | Targeted steroid injection, surgical excision, and deep muscular implantation |
| Phantom Limb Pain | Variable | Central and peripheral nerve sensitization | Gabapentinoids, SNRIs, mirror box therapy, regional nerve blocks |



Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a partial foot amputation is a highly structured, multiphasic process that requires close collaboration between the orthopedic surgeon, physical therapist, and prosthetist/orthotist. The ultimate goal is to return the patient to a functional, plantigrade, and pain-free ambulatory status while fiercely protecting the contralateral "at-risk" limb.
Phase 1: Immediate Post-Operative Protection (Weeks 0-3)
The primary objective in the immediate postoperative period is wound healing and edema control. The amputation site must be protected with a sterile, non-adherent dressing (e.g., Xeroform or Adaptic) followed by a bulky, well-padded soft dressing. In reliable patients, a rigid wooden-soled postoperative shoe or a specialized offloading boot (e.g., CAM walker) is utilized. The patient is strictly non-weight-bearing on the operative extremity. Edema control is achieved through continuous limb elevation. Premature dependency of the limb will cause severe throbbing pain and venous engorgement, threatening the viability of the marginal flaps.
Phase 2: Subacute Healing and Suture Removal (Weeks 3-6)
In dysvascular or diabetic patients, the standard timeline for suture removal is intentionally delayed. Sutures should remain in place for 21 to 28 days to prevent catastrophic wound dehiscence, as the fibroblastic phase of healing is significantly impaired in this population. Once the wound is clinically stable and sutures are removed, the patient may begin a graduated transition to partial weight-bearing. Desensitization techniques for the residual stump are initiated to prepare the soft tissue for eventual orthotic loading.

Phase 3: Prosthetic/Orthotic Fitting and Gait Training (Weeks 6+)
Once the residual limb has matured and volumetric fluctuations have stabilized, definitive orthotic management begins. Amputation of all toes eliminates the spring and resilience of the foot, interfering significantly with squatting, tiptoeing, and rapid gait; however, it requires no complex prosthesis other than a custom molded shoe filler with a rigid carbon-fiber footplate. Transmetatarsal and midfoot amputations require more substantial support, typically involving a custom-molded Ankle-Foot Orthosis (AFO) to replace the lost anterior lever arm and prevent late equinus drift. The addition of a rocker-bottom sole to the patient'
Clinical & Radiographic Imaging Archive

