First Metatarsophalangeal Joint Arthrodesis: A Masterclass in Hallux Rigidus Reconstruction

Key Takeaway
This masterclass guides fellows through first MTP joint arthrodesis for advanced hallux rigidus. We cover critical preoperative assessment, exact patient positioning, detailed surgical anatomy to mitigate neurovascular risks, and a step-by-step intraoperative execution using the ball-and-socket technique with dorsal plate and compression screw fixation. Emphasis is placed on achieving optimal toe position for functional gait and avoiding common pitfalls, ensuring successful patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The first metatarsophalangeal (MTP) joint arthrodesis stands as one of the most reliable, durable, and functionally restorative procedures in the armamentarium of the modern orthopedic foot and ankle surgeon. When executed with meticulous attention to biomechanical alignment and rigid internal fixation, this procedure offers profound pain relief and functional improvement for patients suffering from advanced first MTP joint arthrosis. While novice surgeons may view arthrodesis simply as the elimination of a joint, the master surgeon understands that it is, in fact, a complex reconstruction aimed at restoring a functional, pain-free forefoot capable of bearing the immense loads of the terminal stance phase of gait.
Arthrosis of the first MTP joint is a highly prevalent condition, primarily manifesting as hallux rigidus, but it is also frequently encountered in the context of advanced rheumatoid disease, crystalline arthropathies such as gout, and post-traumatic joint incongruity. Hallux rigidus is characterized by progressive degeneration of the articular cartilage, accompanied by the formation of periarticular osteophytes, particularly along the dorsal and dorsolateral margins (the dorsal cheilus). The patho-epidemiology suggests a multifactorial etiology, including repetitive microtrauma, an elevated first ray (metatarsus primus elevatus), an excessively long first metatarsal, or underlying biomechanical instability of the first ray complex. As the cartilage degrades, the joint space narrows, and the dorsal osteophytes mechanically impinge upon the proximal phalanx during dorsiflexion, leading to the hallmark symptom of restricted and exquisitely painful motion.
The natural history of hallux rigidus is one of relentless progression. While the joint itself may deteriorate radiographically over time, a patient's clinical symptoms may not always mirror this progression linearly until they reach an advanced stage where pain becomes constant, activity-limiting, and refractory to conservative measures. Patients frequently present with an altered gait pattern, characterized by supination of the foot to avoid loading the medial column, which subsequently leads to transfer metatarsalgia and lateral column overload. When comprehensive conservative management—encompassing activity modification, targeted non-steroidal anti-inflammatory regimens, intra-articular corticosteroid injections, and specialized orthoses with rigid Morton’s extensions or rocker-bottom soles—fails to provide durable relief, surgical intervention becomes unequivocally indicated. For advanced disease, arthrodesis remains the undisputed gold standard, offering superior long-term outcomes compared to excisional arthroplasty or implant arthroplasty.
Detailed Surgical Anatomy and Biomechanics
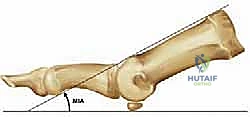
Before initiating any surgical approach, a profound understanding of the complex osteology, ligamentous restraints, and dynamic muscular stabilizers of the first MTP joint is absolutely paramount. The first MTP joint is inherently a specialized condylar articulation, permitting motion in multiple planes, though its primary functional arc during human locomotion is in the sagittal plane (dorsiflexion and plantarflexion). The first metatarsal head forms the convex articular surface, which is unique due to its variable inclination angle relative to the weight-bearing surface—typically ranging from 25 to 30 degrees, though this is heavily influenced by the patient's underlying foot morphotype (e.g., increased in cavus feet, decreased in planus feet). The base of the proximal phalanx forms the corresponding concave articulation.
The sesamoid complex is integral to the biomechanical integrity of the first ray. The tibial and fibular sesamoids are embedded within the medial and lateral slips of the flexor hallucis brevis (FHB) tendon, respectively, articulating with the plantar aspect of the metatarsal head. This complex functions as a vital fulcrum, increasing the mechanical advantage of the FHB and the flexor hallucis longus (FHL), while simultaneously absorbing weight-bearing forces during toe-off. The plantar plate, a robust fibrocartilaginous structure, connects the sesamoids to the base of the proximal phalanx, providing critical stability against hyperextension. During an arthrodesis, while the sesamoids are not directly fused, their position and the integrity of the plantar plate must be respected to prevent iatrogenic elevation of the metatarsal head.
The neurovascular and tendinous anatomy dictates our surgical approach and demands meticulous dissection. The extensor hallucis longus (EHL) tendon runs centrally over the dorsal aspect of the joint and serves as our primary superficial landmark. The medial dorsal cutaneous nerve of the hallux—a terminal branch of the superficial peroneal nerve—courses superficially and medial to the EHL tendon. This nerve is highly susceptible to iatrogenic transection or traction injury during the dorsal approach. Injury here can precipitate a debilitating neuroma or persistent paresthesias, which can overshadow an otherwise technically perfect arthrodesis. The vascular supply is primarily derived from the first dorsal metatarsal artery and the first plantar metatarsal artery, emphasizing the need for careful soft tissue handling to preserve the viability of the surrounding skin flaps and capsular tissues.
Biomechanics of the First Ray
The biomechanical role of the first MTP joint cannot be overstated; it is the linchpin of the windlass mechanism described by Hicks. As the hallux dorsiflexes during the terminal stance phase of gait, the plantar fascia is wound around the metatarsal head, drawing the calcaneus and metatarsal closer together, thereby elevating the longitudinal arch and converting the foot into a rigid lever for forward propulsion. An arthrodesis must be positioned to replicate the functional position of the hallux during this phase. If the toe is fused in excessive plantarflexion, the windlass mechanism is prematurely engaged, leading to massive overload of the interphalangeal (IP) joint and the first ray. Conversely, excessive dorsiflexion renders the hallux incompetent for weight-bearing, transferring the load to the lesser metatarsal heads and causing intractable transfer metatarsalgia.
Exhaustive Indications and Contraindications
The decision to proceed with a first MTP joint arthrodesis must be predicated on a rigorous evaluation of the patient's clinical presentation, radiographic findings, and functional demands. The primary indication is advanced, symptomatic hallux rigidus (Coughlin and Shurnas Grades 3 and 4) that has proven recalcitrant to exhaustive conservative management. In these advanced stages, the articular cartilage is virtually absent, and the joint is characterized by global osteophytosis and severe restriction of motion. Arthrodesis is also the procedure of choice for severe, inflammatory arthritides affecting the forefoot, most notably rheumatoid arthritis, where it is often combined with lesser MTP joint resections or arthroplasties to reconstruct a severely deformed rheumatoid forefoot.
Furthermore, arthrodesis serves as a highly reliable salvage procedure for failed previous forefoot surgeries. This includes the management of recurrent or severe hallux valgus deformities, particularly in the setting of hypermobility of the first tarsometatarsal (TMT) joint, where an isolated distal soft tissue or bony procedure would be doomed to fail. It is also the definitive salvage operation for failed Keller excisional arthroplasties or failed first MTP joint implant arthroplasties (silicone or metallic), where bone loss and biomechanical instability necessitate rigid stabilization to restore function.
Despite its high success rate, the procedure is not without its limitations, and careful patient selection is critical. The presence of absolute contraindications must preclude surgical intervention. Active local or systemic infection is an absolute barrier to any elective arthrodesis. Severe peripheral vascular disease (PVD) is another absolute contraindication; the compromised vascular envelope will inevitably lead to wound dehiscence, nonunion, or catastrophic amputation. Furthermore, pre-existing, advanced arthrosis of the hallux interphalangeal (IP) joint is a strict contraindication. Fusing the MTP joint transfers immense biomechanical stress to the adjacent IP joint; if the IP joint is already degenerative, arthrodesis will rapidly accelerate its destruction and exacerbate the patient's pain.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | Advanced Hallux Rigidus (Grades 3 & 4) | Global cartilage loss and osteophytosis causing intractable pain and mechanical block. |
| Primary Indications | Rheumatoid Arthritis / Inflammatory Arthropathy | Severe joint destruction, deformity, and instability requiring rigid realignment. |
| Salvage Indications | Failed Implant Arthroplasty / Keller Procedure | Loss of bone stock and biomechanical integrity necessitating structural fusion. |
| Salvage Indications | Severe Recurrent Hallux Valgus | Often associated with first ray hypermobility; fusion provides definitive medial column stability. |
| Absolute Contraindications | Active Infection (Local or Systemic) | High risk of hardware seeding, osteomyelitis, and catastrophic failure. |
| Absolute Contraindications | Severe Peripheral Vascular Disease (PVD) | Inadequate perfusion guarantees wound healing failure and high risk of amputation. |
| Absolute Contraindications | Advanced Interphalangeal (IP) Joint Arthrosis | MTP fusion transfers massive stress to the IP joint; pre-existing disease will become highly symptomatic. |
| Relative Contraindications | Severe Peripheral Neuropathy | Loss of protective sensation increases risk of Charcot arthropathy or neuropathic ulceration post-operatively. |
| Relative Contraindications | First Tarsometatarsal (TMT) Joint Arthrosis | Fusing the MTP joint may unmask or exacerbate pain at a degenerative TMT joint (consider pantalar or extended fusions). |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical success in first MTP arthrodesis is engineered before the patient ever enters the operating theater. A comprehensive preoperative physical examination is non-negotiable. The surgeon must assess the exact location of pain, the presence of palpable dorsal cheilus, and the precise arc of motion. The "grind test"—applying axial compression while rotating the proximal phalanx against the metatarsal head—is highly specific for advanced articular degeneration. Crucially, the surgeon must evaluate the adjacent joints. The IP joint must be assessed for mobility and pain, as its health is a prerequisite for MTP fusion. Similarly, the first TMT joint should be evaluated for hypermobility or arthrosis. A thorough vascular assessment, including palpation of the dorsalis pedis and posterior tibial pulses, is mandatory. Any suspicion of vascular compromise mandates a formal non-invasive vascular study prior to scheduling surgery.
Radiographic evaluation requires high-quality, weight-bearing anteroposterior (AP) and lateral radiographs of the foot. The AP view allows for the assessment of the hallux valgus angle, intermetatarsal angle, and the degree of joint space narrowing. The lateral view is critical for identifying the extent of dorsal osteophytosis and measuring the metatarsal inclination angle. This angle is vital for preoperative templating, as it directly influences the required angle of the bone cuts or reaming to achieve the desired final functional position of the hallux. Preoperative templating using digital software allows the surgeon to anticipate the size of the required plate, the trajectory of the interfragmentary lag screw, and the lengths of the locking and non-locking screws, thereby streamlining the intraoperative workflow.
Patient positioning in the operating room is a critical, yet often overlooked, aspect of the procedure. The patient is positioned supine on the operating table. The key ergonomic adjustment is placing the patient's heels at the absolute distal edge of the table, and then dropping the foot of the table by 20 to 30 degrees. This specific configuration allows the surgeon to sit comfortably at the end of the table and provides unimpeded access to the plantar aspect of the foot. This access is essential for performing the intraoperative "flat surface test," utilizing a sterile firm board against the plantar foot to simulate weight-bearing and perfectly gauge the sagittal and coronal alignment of the hallux prior to final fixation. A thigh tourniquet is applied to ensure a bloodless field, which is indispensable for identifying delicate neurovascular structures and confirming complete cartilage removal.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands precision, respect for soft tissues, and an uncompromising approach to biomechanical alignment. The procedure begins with a dorsal, slightly curved longitudinal incision, typically 5 to 7 centimeters in length, centered over the first MTP joint. The incision is meticulously placed just medial to the extensor hallucis longus (EHL) tendon. This trajectory is deliberately chosen to avoid the medial dorsal cutaneous nerve, which typically courses further medially, and to prevent the incision from lying directly over the EHL tendon, which could lead to restrictive tenodesis and extensor lag. Subcutaneous dissection is performed bluntly to identify and protect the nerve, retracting it medially with a small Senn retractor, while the EHL tendon is retracted laterally.

Following exposure, a longitudinal capsulotomy is performed in line with the skin incision. The capsule is reflected sharply off the base of the proximal phalanx and the metatarsal head. A thorough synovectomy is performed to remove inflammatory tissue and clearly delineate the articular margins. The collateral ligaments must be released from the metatarsal head to allow for severe plantarflexion of the proximal phalanx, which "books open" the joint and provides 360-degree visualization of both articular surfaces. At this stage, aggressive dorsal and medial osteophytes (cheilectomy) are excised using a sagittal saw or rongeur to define the true anatomical architecture of the joint and prevent dorsal impingement post-operatively.
Joint Preparation: The Ball-and-Socket Technique
While flat-cut techniques exist, the ball-and-socket (cup-and-cone) technique is widely considered the gold standard due to its ability to maximize cancellous bone contact, minimize metatarsal shortening, and allow for infinite multiplanar adjustment of the toe position prior to fixation.
The preparation begins on the proximal phalanx. A 1.6-mm Kirschner wire is driven centrally into the base of the proximal phalanx, parallel to its longitudinal axis. A cannulated convex reamer, appropriately sized to match the diameter of the phalanx, is passed over the K-wire. Reaming is performed judiciously—the goal is exclusively to remove the eburnated subchondral bone and expose healthy, bleeding, punctate cancellous bone. Over-reaming must be strictly avoided to prevent devastating bone loss and shortening of the hallux.

Attention is then turned to the first metatarsal head. A K-wire is placed centrally in the metatarsal head, aligned with the anatomical axis of the metatarsal. A matching concave reamer is utilized to denude the cartilage. Copious cold saline irrigation is mandatory during all reaming steps to prevent thermal necrosis of the delicate subchondral bone, which is a primary culprit in delayed union or nonunion. Once both surfaces are prepared, they are manually compressed, and the surgeon assesses the fit. The ball-and-socket geometry should provide intrinsic stability and allow the surgeon to smoothly dial in the perfect position.

Positioning and Rigid Internal Fixation
Positioning the hallux is the most critical step of the entire operation; malposition is poorly tolerated and leads to severe functional deficits. The universally accepted optimal position is: 10 to 15 degrees of valgus (to parallel the lesser toes and fit into standard footwear), 15 to 20 degrees of dorsiflexion relative to the first metatarsal anatomical axis (which equates to approximately 5 to 10 degrees of dorsiflexion relative to the floor during simulated weight-bearing), and absolute neutral rotation (the nail plate must face directly dorsal). The "flat surface test" is performed by pressing a sterile board against the plantar aspect of the foot. The hallux pulp should rest lightly on the board, simulating normal weight-bearing without placing excessive pressure on the IP joint.
Once the optimal position is achieved, it is provisionally held with crossed K-wires. Fixation is typically achieved using a combination of an interfragmentary lag screw and a dorsal neutralization plate. A solid core or cannulated lag screw (typically 3.5mm or 4.0mm) is passed from the medial-plantar aspect of the metatarsal head into the dorsal-lateral aspect of the proximal phalanx, compressing the arthrodesis site. Following this, a pre-contoured, low-profile dorsal titanium locking plate is applied.

The plate functions to neutralize dorsal bending moments during the toe-off phase of gait. Locking screws are placed proximally and distally to secure the construct. Intraoperative fluoroscopy is utilized to confirm hardware placement, ensure no screws violate the IP joint, and verify the final alignment of the arthrodesis.

Complications, Incidence Rates, and Salvage Management
While first MTP arthrodesis is highly successful, complications can and do occur, necessitating astute clinical vigilance. The most common complications relate to nonunion, malunion, hardware irritation, and iatrogenic nerve injury.
Nonunion rates in the modern era of rigid plate and lag screw fixation have plummeted to less than 5-10%. Risk factors include smoking, diabetes, non-compliance with weight-bearing restrictions, and technical errors such as thermal necrosis during reaming or inadequate compression. Asymptomatic nonunions (fibrous unions) may not require intervention if the clinical alignment is maintained and the patient is pain-free. However, symptomatic nonunions require revision surgery, typically involving hardware removal, aggressive debridement of the nonunion site down to bleeding bone, application of autologous bone graft (often from the proximal tibia or calcaneus), and revision internal fixation with a larger plate or crossed screws.
Malunion is arguably the most poorly tolerated complication. Fusing the toe in excessive dorsiflexion leads to a "cocked-up" toe, rendering the hallux useless for weight-bearing and resulting in severe transfer metatarsalgia to the lesser metatarsal heads. Conversely, fusion in excessive plantarflexion drives the hallux into the ground, causing intractable pain at the IP joint and tip of the toe, often leading to dorsal ulcerations over the IP joint. Rotational malunions cause the toe to rub against adjacent digits or footwear. Correction of a malunion requires a complex closing or opening wedge osteotomy through the fusion mass, realigning the digit, and reapplying rigid fixation.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion | 2% - 10% | Smoking, diabetes, thermal necrosis, inadequate fixation, non-compliance. | Asymptomatic: Observe. Symptomatic: Revision arthrodesis with autogenous bone grafting and robust internal fixation. |
| Malunion (Dorsiflexion) | 1% - 5% | Technical error during positioning; failure to perform flat-surface test. | Causes transfer metatarsalgia. Requires plantarflexion closing wedge osteotomy through fusion mass. |
| Malunion (Plantarflexion) | 1% - 5% | Technical error; ignoring metatarsal inclination angle. | Causes severe IP joint overload/ulceration. Requires dorsiflexion opening/closing wedge osteotomy. |
| Hardware Irritation | 10% - 15% | Prominent dorsal plate, thin soft tissue envelope, prominent screw heads. | Conservative: Shoe modification. Surgical: Hardware removal after radiographic confirmation of solid union (typically >6 months). |
| Nerve Injury (Neuroma) | 1% - 3% | Iatrogenic transection or traction of medial dorsal cutaneous nerve. | Conservative: Gabapentinoids, desensitization. Surgical: Neuroma excision and burying the proximal stump into muscle/bone. |
| IP Joint Degeneration | Long-term (Variable) | Natural progression of altered biomechanics; accelerated by malposition. | Conservative: Stiff-soled shoes, rocker bottoms. Surgical: IP joint arthrodesis (rarely required if MTP position is optimal). |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to protect the delicate early phases of bone healing while preventing profound disuse osteopenia and adjacent joint stiffness. The protocol is strictly phased based on biological healing timelines.
Phase 1: Immediate Post-Operative Period (Weeks 0-2)
Following surgery, the foot is placed in a bulky, sterile compressive dressing to minimize edema. The patient is placed in a rigid, flat-bottomed postoperative shoe or a controlled ankle motion (CAM) boot. During the first two weeks, the patient is instructed to remain strictly non-weight-bearing or heel-weight-bearing only, utilizing crutches or a knee scooter. Elevation of the limb above the level of the heart is critical to control swelling and promote wound healing. At the two-week mark, sutures are removed, and clinical alignment is assessed.
Phase 2: Protected Weight-Bearing (Weeks 2-6)
If the soft tissue envelope is healing appropriately, the patient is transitioned to progressive weight-bearing as tolerated in the rigid postoperative shoe or CAM boot. The rigid sole is imperative; it acts as an external splint, preventing any dorsiflexion forces from transmitting across the MTP joint, thereby protecting the internal fixation construct from cyclical bending fatigue. Patients are encouraged to perform active and passive range of motion exercises of the ankle and the hallux IP joint to prevent stiffness. Radiographs are typically obtained at the 6-week mark to assess for early trabecular bridging across the arthrodesis site.
Phase 3: Transition to Normal Function (Weeks 6-12)
Upon radiographic confirmation of progressive union (typically between 6 and 8 weeks), the patient is gradually transitioned out of the rigid boot and into a stiff-soled athletic shoe. A carbon fiber insert may be prescribed to provide additional rigidity during the transition phase. Physical therapy may be initiated to focus on gait retraining, restoration of ankle and IP joint kinematics, and strengthening of the intrinsic foot musculature and extrinsic stabilizers. High-impact activities and running are strictly avoided until complete radiographic consolidation is achieved, which often takes 3 to 4 months.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the first MTP joint arthrodesis has been heavily guided by rigorous clinical research and landmark outcome studies. The seminal work by Coughlin and Shurnas established the definitive clinical and radiographic grading system for hallux rigidus, which remains the universal standard for determining surgical indications. Their long-term outcome studies conclusively demonstrated that arthrodesis provides superior, more predictable, and more durable pain relief and functional restoration compared to cheilectomy or implant arthroplasty in advanced disease (Grades 3 and 4).
Furthermore, biomechanical studies by Brodsky et al. have elucidated the critical importance of exact sagittal and coronal plane positioning. Their research highlighted how even minor deviations (greater than 5 degrees) from the optimal functional position exponentially increase the contact pressures on the adjacent IP joint and lesser metatarsal heads.
Comparative literature evaluating fixation constructs has consistently shown that the combination of an interfragmentary lag screw and a dorsal neutralization plate provides the most biomechanically robust construct. This construct offers superior resistance to cyclical loading and torsional forces compared to crossed K-wires or isolated dorsal plates, directly correlating with the significantly decreased nonunion rates observed in modern clinical practice. Consequently, clinical guidelines from major orthopedic foot and ankle societies universally endorse the plate-and-screw construct as the preferred method for achieving rigid stabilization in first MTP joint arthrodesis.
