Mastering Foot & Ankle Interventions: Essential Ankle Surgery Insights
Key Takeaway
Your ultimate guide to Mastering Foot & Ankle Interventions: Essential Ankle Surgery Insights starts here. Ankle arthrodesis is a foot ankle int indicated for severe arthropathy, failed arthroplasty, or avascular necrosis of the talus. This surgical procedure fuses the ankle joint into a specific functional position (e.g., 0° dorsiflexion, 0-5° valgus, 5-10° external rotation). It aims to relieve pain but results in altered walking mechanics and increased energy expenditure.
A 45-year-old high-demand manual laborer presents with end-stage post-traumatic ankle arthritis following a pilon fracture 10 years ago. He reports constant pain and significant functional limitation. You are discussing surgical options. How do you approach the decision between ankle arthrodesis and total ankle arthroplasty (TAA)?

Candidate: I would discuss both options. Arthrodesis is good for young, active patients, but TAA preserves motion. I would examine him and see if he has subtalar arthritis or bad alignment. If he is young and a manual laborer, I would lean towards a fusion because it's more durable.
Failing to structure the answer. Candidates often "chat" without a clear framework. They miss critical factors like BMI, soft tissue quality, and the specific contraindications to TAA (e.g., prior infection, neuro-deficits). They also fail to mention the 100% risk of adjacent joint arthritis over time with fusion.
I would approach this by assessing the "Candidate, Deformity, and Joint" triad. Patient Factors: In a young, high-demand manual laborer, ankle arthrodesis is the gold standard for reliable pain relief and durability. TAA in this cohort has a higher risk of aseptic loosening and revision. Deformity Factors: I would assess coronal and sagittal alignment. Severe uncorrectable deformity is a relative contraindication to TAA. Joint Factors: I would evaluate the subtalar and midfoot joints clinically and via CT. If there is pre-existing arthritis in adjacent joints, an ankle fusion will accelerate their failure, potentially mandating a pantalar fusion or making a case for TAA to spare those joints if the patient meets criteria. I would conclude by explaining that arthrodesis sacrifices motion for stability/durability, while TAA attempts to restore kinematics at the risk of long-term implant failure.
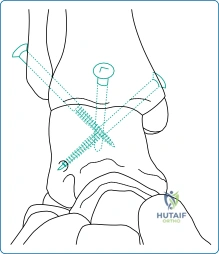
You have decided to proceed with an ankle arthrodesis. Describe the three critical parameters for the position of fusion and explain the biomechanical rationale for each.
Candidate: You need to put the ankle in neutral, a little bit of valgus, and some external rotation. This is to make sure the patient can walk properly and that the other joints in the foot don't get arthritis.
Vague terminology ("a little bit"). The examiner wants specific degrees. Failing to link the malalignment to specific gait abnormalities (e.g., equinus leading to knee recurvatum) shows a lack of depth regarding the biomechanical consequences.
The "Non-negotiable" parameters for ankle arthrodesis are:
1. Sagittal Plane (Neutral 0°): Prevents equinus, which causes a functional limb length discrepancy, knee recurvatum, and heel ulceration; or dorsiflexion, which causes a "peg-leg" gait.
2. Coronal Plane (0°–5° Valgus): Essential to "unlock" the transverse tarsal joints, maintaining midfoot flexibility to accommodate uneven terrain. Varus malunion locks the midfoot, leading to rapid lateral column overload.
3. Transverse Plane (5°–10° External Rotation): Mirrors the transmalleolar axis and tibial torsion, ensuring the foot clears the contralateral limb during the swing phase of gait.
During the anterior approach for an ankle arthrodesis, you notice the patient has a significant equinus contracture. How do you manage this soft tissue pathology, and what are the risks if you ignore it?
Candidate: I would perform an Achilles tendon lengthening. If you don't, the patient won't be able to get their heel down to the ground, and they will walk on their toes.
Only discussing the gait effect. The candidate must address the surgical site complications, specifically the catastrophic risk of wound dehiscence due to tension on the anterior skin closure.
An Achilles tendon lengthening (TAL)—either percutaneous or open—is mandatory. Biomechanical consequences of ignoring it: It forces the ankle into equinus, creating a recurvatum thrust at the knee and massive overload on the midfoot. Surgical consequences: Forcing the ankle into neutral against a tight Achilles creates excessive tension on the anterior surgical flap. This leads to wound ischemia, necrosis, and potentially deep infection. It also puts undue strain on the internal fixation hardware, increasing the risk of nonunion or construct failure.
