Interdigital Neuroma (Morton's Toe): Comprehensive Surgical Management
Key Takeaway
Interdigital neuroma, or Morton's toe, is a degenerative perineural fibrosis of the common digital nerve, most frequently affecting the third web space. Diagnosis is primarily clinical, characterized by forefoot pain and a positive Mulder's click. When conservative measures fail, surgical excision via a dorsal or plantar approach yields high satisfaction rates. This guide details the anatomical biomechanics, histological findings, and step-by-step operative techniques for successful neuroma resection.
Comprehensive Introduction and Patho-Epidemiology
Historical Context and Evolution of Thought
Interdigital neuroma, universally recognized by its eponym Morton's toe or Morton's neuroma, is a common, highly debilitating affliction of the forefoot characterized by entrapment, mechanical irritation, and subsequent profound degeneration of the common digital nerve. The condition was first formally described in the medical literature in 1845 by Durlacher, chiropodist to the Queen of England, who accurately identified it as a "form of neuralgic affection" involving the plantar nerve situated between the third and fourth metatarsal bones. Several decades later, in 1876, Thomas G. Morton expanded upon this initial clinical description, postulating that the underlying pathology resulted directly from the pinching of the common digital branch of the lateral plantar nerve between the mobile fourth and fifth metatarsal heads. Though anatomically slightly inaccurate regarding the most common interspace, his name remains inextricably linked to the pathology.
Historically, the exact etiology of this neuralgic pain has been a subject of intense academic debate, yielding numerous biomechanical and anatomical theories over the past century. Pollosson suggested that an inherent laxity of the transverse metatarsal ligament allowed a break in the anterior arch, leading to plantar displacement of the central metatarsal heads and subsequent nerve traction. Guthrie and Woodruff proposed that instability of the fourth metatarsophalangeal (MTP) joint was the primary mechanical culprit. Jones and Tubby hypothesized a "pressure neuralgia" developing specifically during the weight-bearing phases of the gait cycle. McElvenny theorized the presence of a distinct tumor involving the lateralmost branch of the medial plantar nerve, while Nissen suggested that lumen occlusion in the common digital artery adjacent to the nerve led to ischemic neuropathy.
In 1940, Betts introduced a highly compelling anatomical theory that dominated surgical teaching for decades. He reasoned that the singular anatomy of the fourth digital branch of the medial plantar nerve was the primary culprit. This specific branch frequently receives a communicating branch from the common digital branch of the lateral plantar nerve. Because of this anatomical convergence, Betts argued that the common digital nerve to the third web space is thicker and inherently more susceptible to compression against the unyielding deep transverse intermetatarsal ligament (DTML) located dorsal to it. However, while Betts' theory of the communicating branch is anatomically sound in many patients, a rigorous anatomical review by Levitsky et al. demonstrated that this communicating branch was completely absent in 73.2% of cadaveric feet. Furthermore, neuromas were identified in an almost equal distribution between the second and third web spaces, indicating that while nerve thickness may play a partial role, repetitive microtrauma against the DTML remains the primary mechanical driver across all affected interspaces.
Histopathological Characteristics
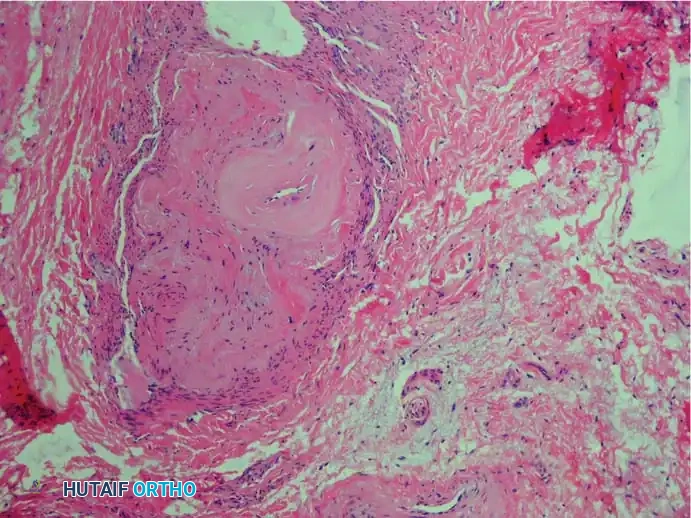
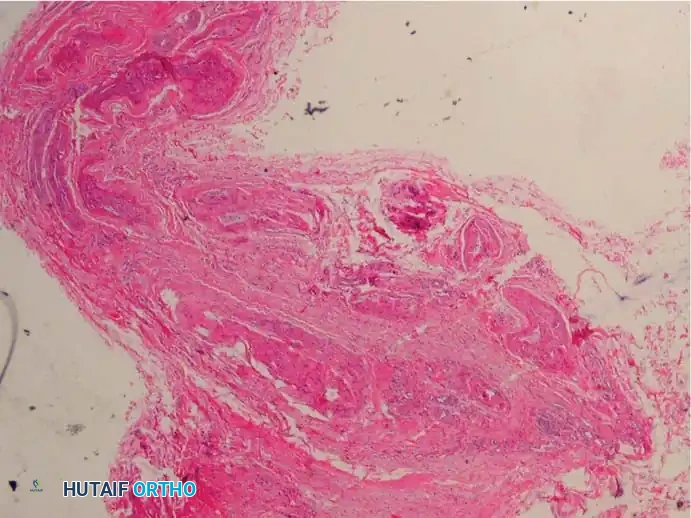
In a strict histopathological sense, the term neuroma is a misnomer. The haphazard, disorganized proliferation of axons attempting to cross a gap—characteristic of a true traumatic stump neuroma—is entirely absent in a primary Morton's neuroma. Instead, the macroscopic enlargement of the nerve is driven by the extensive deposition of hyaline and collagenous material within the nerve sheath. The pathological process is fundamentally degenerative and fibrotic rather than proliferative. Consequently, prominent foot and ankle surgeons such as Weinfeld and Myerson have strongly advocated for the more accurate, descriptive term, interdigital neuritis or perineural fibroma.
The pathogenesis is multifactorial, driven by repetitive mechanical microtrauma, progressive perineural fibrosis, ischemia resulting from vasa nervorum occlusion, and chronic endoneural edema. The essential histological findings, as meticulously described by Bickel, Dockerty, Lassmann, and others, provide a clear picture of this degenerative cascade:
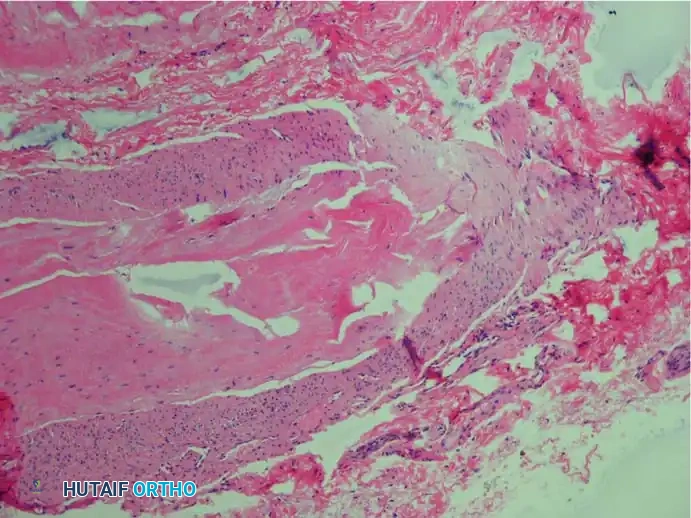
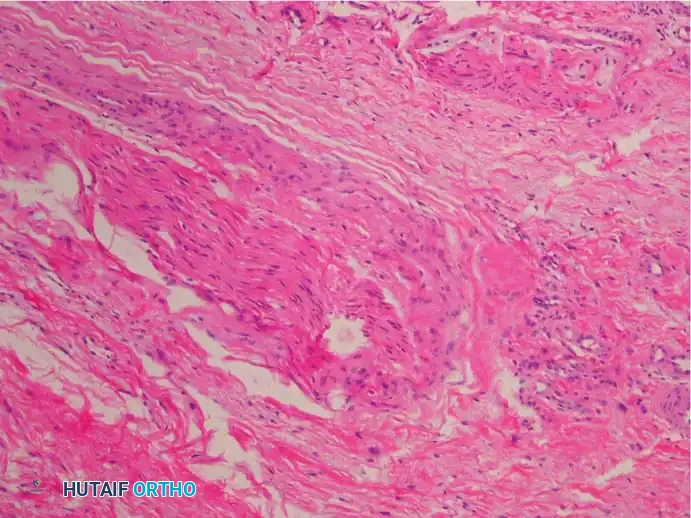
1. Extensive thickening of the perineurium, often with concentric layers of fibrosis.
2. Increased number of intrafascicular arterioles exhibiting thickened, hyalinized walls due to the deposition of multiple layers of basement membranes, leading to localized ischemia.
3. Demyelination and degeneration of nerve fibers, accompanied by a marked decrease in the absolute number of viable axis cylinders.
4. Fluid accumulation within the endoneurium, contributing to the fusiform swelling of the nerve.
5. A distinct and notable lack of acute inflammatory cells (lymphocytes, macrophages), confirming this is a chronic degenerative process rather than an acute inflammatory one.
6. The frequent presence of reactive, hypertrophic intermetatarsal bursal tissue intimately accompanying the nerve specimen.
Epidemiologically, the condition exhibits a striking predilection for the female demographic, with reported female-to-male ratios ranging from 4:1 to as high as 10:1 in some operative series. This disparity is widely attributed to footwear choices, specifically narrow toe boxes and elevated heels, which biomechanically force the forefoot into a confined space while simultaneously hyperextending the MTP joints. The peak incidence occurs in the fourth to sixth decades of life. While usually unilateral, bilateral presentations are not uncommon, though simultaneous bilateral surgical intervention is generally discouraged due to the significant impairment of postoperative ambulation.
Detailed Surgical Anatomy and Biomechanics
Osseous and Ligamentous Architecture
A profound understanding of the forefoot's structural anatomy is non-negotiable for the orthopedic surgeon managing interdigital neuromas. The metatarsal heads form the transverse metatarsal arch, which dynamically flattens during the weight-bearing phase of gait. Connecting the adjacent metatarsal heads is the deep transverse intermetatarsal ligament (DTML), a robust, unyielding band of fibrous tissue. The DTML attaches to the plantar plates of the MTP joints, creating a rigid dorsal roof over the intermetatarsal space.
Directly plantar to the DTML lies the neurovascular bundle, consisting of the common digital nerve and the common digital artery and vein. The lumbrical muscles also traverse this space, typically lying plantar and slightly adjacent to the neurovascular bundle, before inserting onto the extensor expansion. Dorsal to the DTML lies the intermetatarsal bursa, which extends distally between the metatarsal heads. In the pathologic state, chronic irritation leads to bursal hypertrophy, which further decreases the available volume within the intermetatarsal space, exacerbating nerve compression from above while the plantar ground reaction forces compress the nerve from below.
Neurologic Pathways and The Communicating Branch
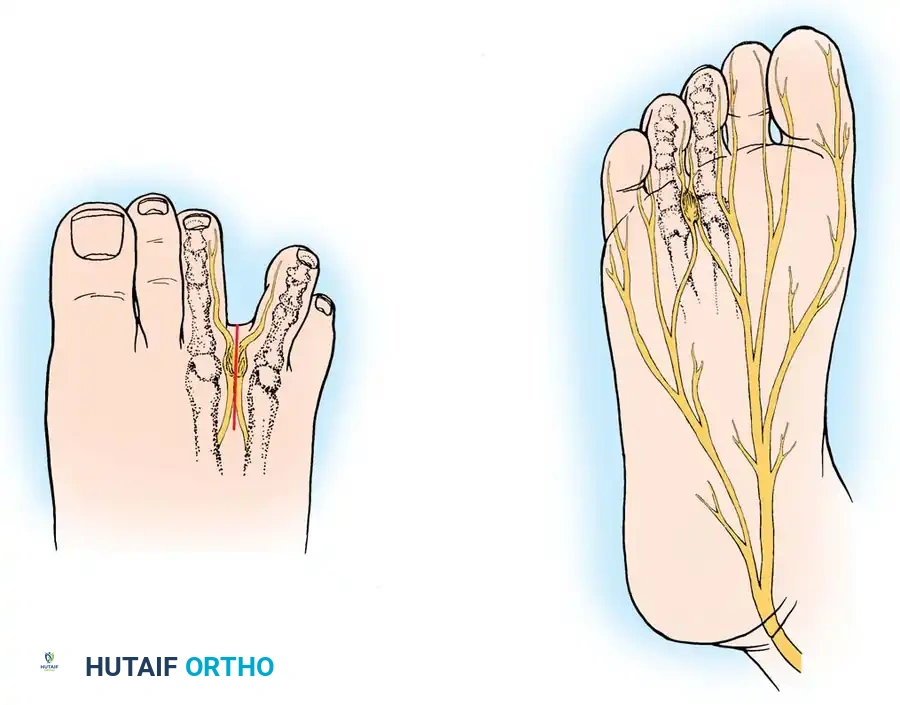
The innervation of the plantar forefoot is derived from the medial and lateral plantar nerves, which are terminal branches of the tibial nerve. The medial plantar nerve typically supplies the first three digits and the medial aspect of the fourth digit via three common digital branches. The lateral plantar nerve supplies the fifth digit and the lateral aspect of the fourth digit.
The third web space (between the third and fourth metatarsals) is the most frequent site of neuroma formation, followed closely by the second web space. Anatomically, the third common digital nerve is often formed by the confluence of the third common digital branch of the medial plantar nerve and a communicating branch from the lateral plantar nerve. This anatomical convergence creates a nerve with a larger cross-sectional area. When the foot is enclosed in a constrictive shoe, the metatarsal heads are squeezed together, and the enlarged nerve is repeatedly driven upward against the sharp, unyielding distal edge of the DTML during the toe-off phase of gait.
Dynamic Forefoot Biomechanics
During the normal gait cycle, as the heel lifts and the foot transitions into the terminal stance and pre-swing phases, the MTP joints undergo significant dorsiflexion. This action engages the windlass mechanism, drawing the plantar aponeurosis taut and elevating the longitudinal arch. Concurrently, the common digital nerve, which is tethered distally by its bifurcation into the proper digital nerves at the base of the toes, is stretched tightly across the distal margin of the DTML.
When a patient wears high-heeled shoes, the MTP joints are held in a state of chronic hyperextension, placing continuous traction on the nerve and pulling it firmly against the ligament. The addition of a narrow toe box physically compresses the metatarsal heads together, reducing the intermetatarsal distance and directly crushing the nerve. This combination of traction, friction, and direct compression initiates the cascade of endoneural edema and perineural fibrosis that ultimately defines the interdigital neuroma.
Exhaustive Indications and Contraindications
Clinical Presentation and Physical Examination
The diagnosis of an interdigital neuroma remains primarily clinical, heavily reliant on a meticulous history and physical examination. Patients characteristically present with severe, episodic pain localized to the plantar aspect of the affected metatarsal heads. The pain is frequently described in neuropathic terms: burning, aching, cramping, or electric shock-like sensations that radiate distally into the adjacent toes. A hallmark historical feature is the patient's urgent need to remove their shoe and massage the forefoot to obtain relief. Subjective numbness or a "pins and needles" sensation in the toes of the involved interspace is common, though objective sensory deficits on examination (e.g., using Semmes-Weinstein monofilaments) are surprisingly rare.
Physical examination reveals exquisite, localized point tenderness in the affected web space, specifically in the soft tissue just distal to the weight-bearing pad of the metatarsal heads. This must be carefully differentiated from tenderness directly over the metatarsal head or the MTP joint line, which would suggest Freiberg's infraction, avascular necrosis, or capsulitis/plantar plate pathology.

The pathognomonic clinical test is Mulder's Sign. The examiner manually compresses the metatarsal heads together with one hand (splaying the web space and pushing the neuroma plantarward), while applying direct dorsal pressure to the plantar aspect of the suspected web space with the thumb of the opposite hand. A palpable, and frequently audible, "click" occurs as the fibrotic, enlarged neuroma is forced to subluxate dorsally across the unyielding transverse ligament.

Advanced Imaging Modalities
While the diagnosis is clinical, imaging plays a role in ruling out competing pathologies. Weight-bearing anteroposterior, lateral, and oblique radiographs of the foot are mandatory to exclude stress fractures, degenerative joint disease, MTP joint subluxation, and Freiberg's infraction.
Ultrasonography (US) and Magnetic Resonance Imaging (MRI) are frequently employed in contemporary practice, particularly in atypical presentations or recurrent cases. High-resolution ultrasound can visualize the hypoechoic, ovoid mass of the neuroma and allows for dynamic assessment (sonographic Mulder's sign). MRI, typically utilizing T1-weighted and fluid-sensitive (STIR or T2 fat-suppressed) sequences, demonstrates a teardrop-shaped mass in the intermetatarsal space that is iso- to hypointense on T1 and T2 sequences. However, extensive studies, including those by Resch et al., have repeatedly concluded that advanced imaging is of limited additive value compared to a rigorous, expert clinical examination, and asymptomatic neuromas are frequently identified incidentally on MRI, leading to potential false-positive surgical indications.
| Parameter | Indications for Surgical Excision | Contraindications for Surgical Excision |
|---|---|---|
| Clinical History | Intractable neuralgic pain failing >3-6 months of conservative care (wide shoes, orthotics, NSAIDs). | Mild, intermittent pain manageable with shoe wear modification alone. |
| Physical Exam | Positive Mulder's click; localized web space tenderness; positive diagnostic injection response. | Tenderness localized primarily to the MTP joint or proximal phalanx base (suggests plantar plate tear). |
| Diagnostic Injections | Temporary, complete ablation of symptoms following a localized lidocaine/corticosteroid web space block. | Failure to achieve even temporary relief from a properly placed diagnostic local anesthetic block. |
| Vascular Status | Palpable pedal pulses; normal Ankle-Brachial Index (ABI > 0.9); brisk capillary refill. | Severe Peripheral Arterial Disease (PAD); ischemic rest pain; ABI < 0.5. |
| Neurologic Status | Isolated interdigital neuralgia without proximal radicular symptoms. | Proximal nerve entrapment (Tarsal Tunnel Syndrome, L5/S1 lumbar radiculopathy) causing the primary symptoms. |
| Systemic Health | Medically optimized for elective outpatient surgery. | Active local or systemic infection; poorly controlled diabetes mellitus (HbA1c > 8.0%) with profound peripheral neuropathy. |
Pre-Operative Planning, Templating, and Patient Positioning
Patient Counseling and Operative Setup
Pre-operative planning for interdigital neuroma excision does not involve traditional osseous templating, but rather relies on meticulous patient counseling and precise localization of the pathology. The most critical aspect of the pre-operative phase is managing patient expectations. Surgeons must explicitly document that while 80% to 95% of patients achieve excellent or complete pain relief, the primary goal of the procedure is the eradication of sharp, neuralgic pain, not the restoration of normal forefoot sensation. Studies by Mann and Reynolds have demonstrated that up to 65% of patients may experience mild, persistent local plantar tenderness, and nearly 70% will note permanent, objective numbness in the opposing aspects of the toes of the involved interspace. Patients must consent to this permanent sensory loss.
Furthermore, the surgeon must confirm the exact interspace involved immediately prior to surgery, ideally marking the foot in the pre-operative holding area while the patient is awake and able to confirm the site of their typical pain. Operating on the wrong web space is a devastating, entirely preventable "never event."
Anesthesia and Patient Positioning
The procedure is typically performed on an outpatient basis. Anesthetic options include a regional ankle block (utilizing a long-acting local anesthetic such as bupivacaine), a popliteal sciatic nerve block, or general anesthesia. If a regional block is utilized, it is highly recommended to supplement the block with local infiltration of lidocaine with epinephrine directly into the dorsal web space to aid in hemostasis.
The patient is positioned supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a perfectly neutral position. A calf or thigh tourniquet is routinely applied to ensure a bloodless surgical field, which is absolutely critical for the precise identification of the delicate proper digital nerve branches and the avoidance of iatrogenic injury to adjacent structures. The foot is prepped and draped in standard sterile orthopedic fashion. Essential instrumentation includes self-retaining Weitlaner retractors, a small lamina spreader, delicate dissecting scissors (tenotomy or Metzenbaum), and loupe magnification (typically 2.5x to 3.5x), which is indispensable for identifying the nerve bifurcation and ensuring complete resection.
Step-by-Step Surgical Approach and Fixation Technique
Note: As interdigital neuroma excision is entirely a soft-tissue procedure involving nerve resection, "fixation" in this context refers to the stabilization of the metatarsals during exposure and the precise handling and positioning of the transected nerve stump to prevent recurrence, rather than osteosynthesis.
The Dorsal Approach: Primary Excision
The dorsal longitudinal approach is the gold standard and the most frequently utilized technique for primary neuroma excision. Its primary advantage is the avoidance of a plantar scar, which can become hypertrophic and result in intractable, mechanically induced pain on the weight-bearing surface of the foot. Furthermore, the dorsal approach provides unparalleled visualization of the DTML.
Step 1: Incision and Superficial Dissection
A 3 to 4 cm longitudinal incision is made centered over the dorsal aspect of the affected web space. The incision begins precisely at the web commissure and extends proximally between the metatarsal shafts. The skin and subcutaneous tissues are sharply divided. The surgeon must remain vigilant to identify and gently retract any superficial dorsal sensory nerve branches (branches of the superficial peroneal or sural nerves) to avoid creating a painful postoperative dorsal neuroma.
Step 2: Deep Exposure and Ligament Release
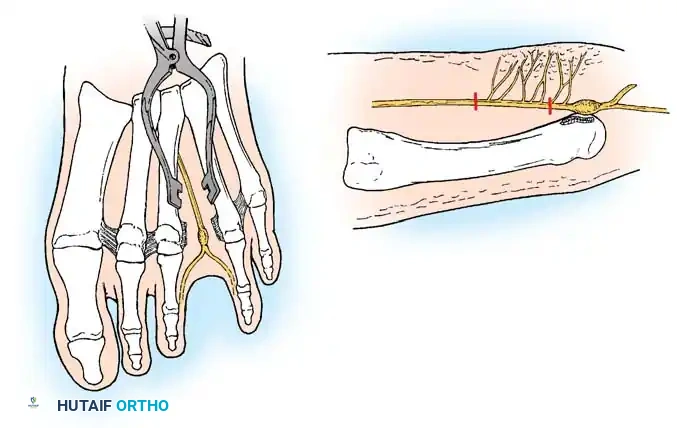
Blunt dissection is carried down between the metatarsal heads. A self-retaining Weitlaner retractor is placed to separate the soft tissues. To adequately expose the DTML, a small lamina spreader is carefully inserted between the metatarsal necks and gently opened. This maneuver distracts the metatarsals and places the DTML under tension, making its transverse fibers clearly visible. Using a #15 scalpel blade or sharp dissecting scissors, the DTML is completely transected from its distal edge to its proximal extent. Care must be taken not to plunge the blade deep to the ligament, which could prematurely transect the underlying nerve or artery.
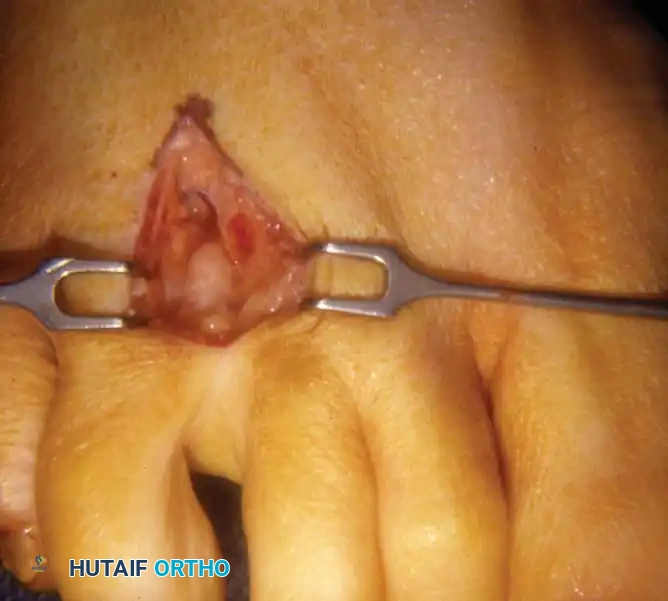
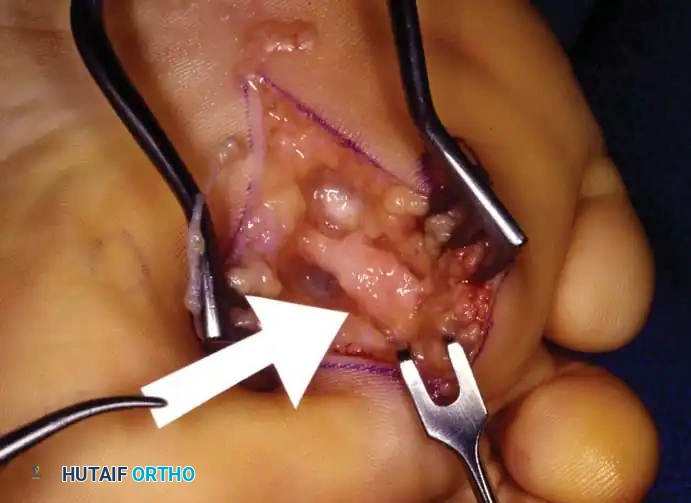
Step 3: Nerve Isolation and Distal Transection
Once the DTML is released, pressure applied to the plantar aspect of the foot by the surgeon's non-dominant hand will frequently cause the enlarged, fibrotic neuroma to bulge dorsally into the operative field. The common digital nerve is carefully isolated from the accompanying common digital artery and vein. The dissection is carried distally to identify the bifurcation of the common digital nerve into the proper digital nerves that supply the adjacent toes. The nerve is sharply transected just distal to this bifurcation, ensuring that the entire pathological specimen is captured.
Step 4: Proximal Transection and Stump Management
This is the most critical step in preventing a recurrent stump neuroma. Gentle distal traction is applied to the isolated nerve. The dissection is carried proximally deep into the intermetatarsal space. The surgeon must trace the nerve at least 1 to 2 cm proximal to the weight-bearing pad of the metatarsal heads. While maintaining tension, the nerve is transected sharply with a fresh scalpel blade. Upon release of tension, the proximal nerve stump must be visualized retracting deep into the intrinsic musculature (specifically the lumbrical muscle belly), ensuring it lies in a protected, non-weight-bearing environment.

Step 5: Closure
The tourniquet is deflated, and meticulous hemostasis is achieved using bipolar electrocautery. Hematoma formation is a significant risk factor for excessive fibrosis and poor outcomes. The DTML is explicitly not repaired; leaving it open prevents recurrent compression. The deep dermal layer is closed with interrupted absorbable sutures, and the skin is approximated with non-absorbable monofilament sutures (e.g., 4-0 nylon) using a vertical mattress or simple interrupted technique.
The Plantar Approach: Revision and Proximal Lesions
The plantar approach is highly effective and is universally considered the preferred approach for revision surgery (addressing recurrent or stump neuromas) or for primary lesions that are located unusually proximal in the foot. The profound advantage of the plantar approach is that it provides direct, unhindered anatomical access to the nerve proximal to the DTML without the necessity of dividing the ligament, thereby preserving the structural integrity of the transverse metatarsal arch.
Step 1: Incision Placement
The placement of the plantar incision is critical to avoid painful scarring. A longitudinal incision is utilized, centered over the affected interspace. Crucially, the distal extent of the incision must begin just proximal to the primary weight-bearing pad of the metatarsal heads and extend proximally into the non-weight-bearing arch of the sole. Transverse incisions are generally avoided due to the risk of widespread sensory denervation distal to the cut.
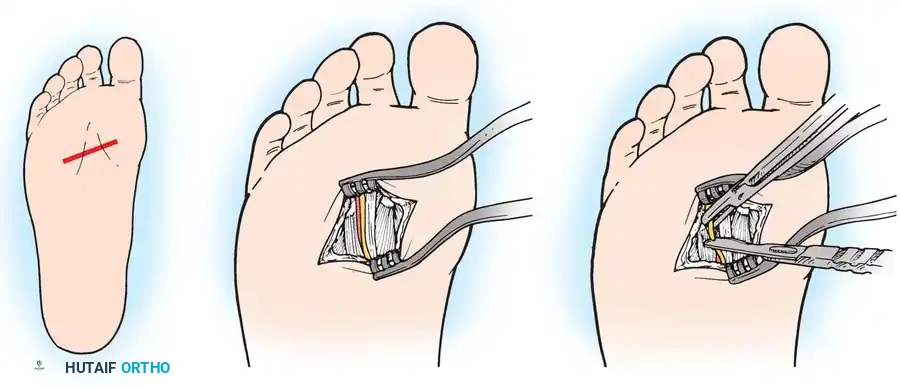
Step 2: Dissection and Exposure
The incision is deepened through the thick plantar skin and the underlying lobulated plantar fat pad. The vertically oriented fibrous septa of the fat pad are divided to expose the glistening white fibers of the plantar aponeurosis. A longitudinal incision is made in the plantar fascia directly in line with the skin incision.
Step 3: Nerve Resection
Directly beneath the plantar fascia, superficial to the lumbrical musculature, the common digital nerve is readily identified. In a revision setting, the bulbous stump neuroma is usually found tethered in scar tissue. The nerve is isolated, dissected distally to the bifurcation (if present), and proximally to healthy, unscarred nerve tissue. The nerve is resected sharply, ensuring the new proximal stump lies deep within the intrinsic muscles, far from the weight-bearing surface.
Step 4: Closure
Meticulous hemostasis is achieved. The plantar fascia is reapproximated if possible using strong absorbable sutures to prevent fat pad herniation. Deep dermal closure is performed, followed by skin closure using robust, non-absorbable vertical mattress sutures (e.g., 3-0 nylon) to ensure perfect eversion of the thick, unforgiving
Clinical & Radiographic Imaging Archive

