Partial Nail Fold and Nail Matrix Removal: Advanced Surgical Techniques

Key Takeaway
Partial nail fold and nail matrix removal aims to eradicate pathological tissue causing onychocryptosis or dystrophy while preserving normal perionychial structures. The critical step in preventing recurrence, particularly nail spicules, is the complete excision of the germinal matrix. This comprehensive surgical guide details the biomechanics, wedge resection principles, and the Quenu technique for total germinal matrix excision, ensuring optimal outcomes for complex nail pathologies.
Comprehensive Introduction and Patho-Epidemiology
The rationale for partial nail fold and nail matrix removal, along with its various surgical modifications, is to definitively eliminate all pathological components causing clinical symptoms while meticulously preserving the normal nail plate and surrounding soft tissue architecture. Conditions such as chronic onychocryptosis (ingrown toenails), severe onychomycosis, and post-traumatic nail dystrophies frequently require surgical intervention when conservative measures—such as orthonyxia, taping, and targeted antimicrobial therapies—fail to provide lasting relief. The epidemiological burden of perionychial pathology is substantial, disproportionately affecting adolescents, young adults, and the geriatric population, often leading to significant functional impairment, chronic pain, and an elevated risk of secondary soft tissue infections.
Onychocryptosis, the most ubiquitous indication for partial nail fold excision, is fundamentally a disease of the surrounding soft tissue rather than an intrinsic abnormality of the nail plate itself. The pathophysiology is driven by a profound mismatch between the width of the nail plate and the accommodating capacity of the nail bed and lateral paronychium. Extrinsic factors, including the chronic use of constricting footwear, improper nail trimming techniques, and repetitive microtrauma during athletic activities, exacerbate this anatomical incongruity. As the lateral edge of the nail plate breaches the epidermal barrier of the paronychial fold, it incites a robust foreign-body inflammatory response, characterized by the proliferation of highly vascularized, friable granulation tissue, exudate formation, and intense localized erythema.
In contrast, chronic onychomycosis and severe nail dystrophies (such as those secondary to psoriasis, lichen planus, or traumatic crush injuries) present a distinct patho-epidemiological profile. In these advanced disease states, the entire nail unit becomes a source of intractable pain and acts as a persistent nidus for fungal or bacterial pathogens. The nail plate often undergoes dramatic morphological changes, culminating in onychogryphosis (the classic "ram's horn" deformity), which mechanically impinges on adjacent digits and renders normal ambulation nearly impossible. When systemic antifungal agents fail due to poor peripheral perfusion or hepatic contraindications, surgical eradication of the entire germinal matrix becomes the definitive standard of care.
The cornerstone of successful perionychial surgery lies in a profound, three-dimensional understanding of the nail unit's anatomy and its dynamic response to surgical alteration. The procedure typically involves a precise wedge resection of the offending nail plate, the underlying nail bed, and the hypertrophic nail fold. However, the most notorious and frequent complication of any matrixectomy—whether partial or total—is the postoperative recurrence of nail spicules. The crucial factor in preventing the formation of recurrent nail spicules is the absolute and complete removal of the germinal matrix at the lateral horns. Because the apex of the surgical wedge—and consequently the narrowest area of resection—is located at the most critical tissue requiring excision, meticulous surgical technique, optimal illumination, and magnification are paramount.
Detailed Surgical Anatomy and Biomechanics
To master nail matrix removal, the orthopedic surgeon must first master the intricate microanatomy and biomechanical function of the perionychium. The nail unit is not merely a static protective shield; it is a highly specialized, complex appendage composed of several distinct, interdependent structures that act in concert to facilitate tactile sensation, protect the distal phalanx, and regulate digital hemodynamics. The nail plate itself is a hard, resilient, keratinized structure produced primarily by the germinal matrix. It lacks intrinsic vascularity and innervation, relying entirely on the underlying vascular bed for its structural integrity and adherence.

The germinal matrix is the biological engine of the nail unit. Located proximally beneath the eponychium and extending distally to the margin of the lunula (the visible white crescent at the base of the nail), the germinal matrix is responsible for approximately 90% of nail plate generation. Its cells undergo rapid proliferation and subsequent keratinization, pushing the nail plate distally. The sterile matrix, conversely, extends from the distal border of the lunula to the hyponychium. While it contributes minimally to the overall thickness of the nail plate, its primary biomechanical function is to provide an exceptionally strong, rigid adherence to the overlying nail plate via a complex system of longitudinal epidermal ridges that interdigitate with the dermal papillae.
Surrounding the nail plate are the specialized soft tissue folds that guide its directional growth and protect the sterile environment of the nail bed from external pathogens. The eponychium (cuticle) is the proximal skin fold that overlies the germinal matrix, creating a watertight seal. The paronychium comprises the lateral soft tissue folds that act as anatomical buttresses, preventing lateral deviation of the growing nail. The hyponychium is the specialized, thickened epidermis located beneath the free edge of the distal nail plate, serving as the terminal waterproof barrier against subungual bacterial and fungal ingress.
From a biomechanical perspective, the nail unit plays a critical role during the toe-off phase of the gait cycle. As ground reaction forces are transmitted through the plantar aspect of the distal phalanx, the soft tissues of the toe pulp are compressed upwards against the rigid counter-pressure of the nail plate. This dynamic interaction maximizes the surface area of the toe pulp, enhancing proprioception and optimizing the propulsive force of the hallux. Surgical alteration of the nail unit, particularly total matrixectomy, inherently modifies this biomechanical relationship. Furthermore, the vascular supply to the nail unit is robust, derived from the paired plantar digital arteries that form extensive anastomotic arcades within the distal pulp and subungual dermal layers. Understanding this vascular network is essential for achieving adequate hemostasis during surgery without compromising the viability of the eponychial flap.
Pathophysiology of Recurrence
When performing a partial nail fold removal, the surgeon creates a complex three-dimensional wedge excision. The base of this wedge is distal, and the apex is proximal, extending deep beneath the eponychium. The anatomical lateral horns of the germinal matrix curve proximally, laterally, and deeply, often extending much further toward the interphalangeal joint than is visually apparent on superficial inspection. These lateral horns reside in a tightly confined proximal cul-de-sac adjacent to the periosteum of the distal phalanx base.
If the apex of the surgical wedge fails to capture the entirety of this lateral horn, the retained germinal matrix cells will continue their physiological mandate to produce keratinized tissue. Because the normal directional guidance of the lateral nail fold has been surgically altered, this new keratin growth typically manifests as a sharp, highly symptomatic nail spicule that pierces the healing paronychium. This leads to a rapid recurrence of pain, foreign-body reaction, and infection, ultimately necessitating a more extensive revision surgery.
Exhaustive Indications and Contraindications
Surgical management of the nail unit is indicated in a wide array of clinical scenarios, ranging from acute, localized infections to chronic, systemic dystrophies that have proven refractory to conservative care. The decision to proceed with surgical intervention must be carefully weighed against the patient's vascular status, functional demands, and the specific pathology affecting the nail unit. A thorough preoperative assessment is mandatory to differentiate between conditions that require a simple partial wedge resection and those that necessitate total eradication of the germinal matrix.
Partial nail fold and matrix removal (frequently referred to as the Winograd procedure or partial wedge resection) is the workhorse procedure for localized pathology. The primary indication is recurrent onychocryptosis that has failed conservative management, such as proper nail trimming education, orthonyxia (nail bracing), and oral antibiotic therapy. It is also highly effective for the excision of hypertrophic granulation tissue resulting from chronic lateral fold irritation. Furthermore, partial resection is often utilized as an access approach for the excision of focal, benign subungual tumors, including glomus tumors, subungual exostoses, and pyogenic granulomas, allowing the surgeon to address the underlying lesion while preserving the majority of the functional nail plate.
Total germinal matrix excision (employing the Quenu, Zadik, or Fowler techniques) is reserved for more severe, global nail pathology. Chronic symptomatic onychomycosis that is entirely resistant to prolonged systemic and topical antifungal therapies is a primary indication, particularly when accompanied by painful onychogryphosis that interferes with shoe wear and ambulation. Severe global nail dystrophy secondary to advanced psoriatic nail disease, lichen planus, or catastrophic post-traumatic crush injuries also warrants total matrixectomy to alleviate intractable pain. Additionally, recurrent global onychocryptosis, where bilateral partial resections have repeatedly failed and the remaining nail plate is excessively narrow and deformed, is best managed with complete removal.
Contraindications to perionychial surgery are primarily related to the patient's vascular and immunological status. Severe peripheral arterial disease (PAD) is an absolute contraindication, as the surgical trauma and subsequent demand for healing can precipitate ischemic necrosis and gangrene of the digit. Uncontrolled diabetes mellitus with profound peripheral neuropathy and microvascular disease is a strong relative contraindication, requiring careful optimization before any elective intervention. Active, spreading cellulitis that extends beyond the immediate paronychial folds should ideally be managed with systemic antibiotics and localized drainage before definitive matrixectomy is attempted, to prevent the proximal spread of infection along the fascial planes of the digit.
| Clinical Condition | Recommended Surgical Procedure | Rationale / Objective | Contraindications / Caveats |
|---|---|---|---|
| Recurrent Onychocryptosis | Partial Wedge Resection (Winograd) | Eradicate offending nail border and hypertrophic tissue; preserve central nail. | Active spreading cellulitis (treat medically first); Severe PAD. |
| Hypertrophic Granulation | Partial Excision with Chemical Cautery | Remove inflammatory nidus and ablate lateral matrix horn. | Avoid excessive chemical application to prevent collateral burn. |
| Subungual Glomus Tumor | Partial Nail Plate Avulsion + Excision | Provide direct access to the subungual space for complete tumor enucleation. | Inadequate imaging pre-op; failure to repair sterile matrix post-excision. |
| Severe Onychomycosis | Total Matrixectomy (Quenu/Zadik) | Complete removal of infected nail unit and generation source. | Uncontrolled diabetes; lack of palpable pedal pulses. |
| Onychogryphosis | Total Matrixectomy (Quenu/Zadik) | Eliminate painful, deformed keratin mass and prevent recurrence. | Patient non-compliance with post-op footwear restrictions. |
| Post-Traumatic Dystrophy | Total Matrixectomy / Terminal Syme | Remove non-functional, painful remnant nail and contour distal phalanx. | Acute trauma with compromised digital viability. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is essential for achieving optimal outcomes in perionychial surgery. The initial step involves a comprehensive vascular assessment of the affected extremity. The surgeon must document the presence and quality of the dorsalis pedis and posterior tibial pulses. In patients with a history of diabetes, smoking, or advanced age, non-invasive vascular studies, including Ankle-Brachial Indices (ABI) and toe pressures, should be obtained. A toe pressure of less than 30 mmHg generally indicates severe microvascular compromise, precluding elective nail surgery due to the unacceptably high risk of postoperative ischemia and non-healing ulceration.
Anesthesia for perionychial surgery requires profound, reliable regional blockade, as the nail unit is exquisitely innervated and highly sensitive to surgical manipulation. A standard digital ring block or a Mayo block utilizing 1% to 2% Lidocaine without epinephrine is the technique of choice. This is frequently combined with 0.5% Bupivacaine in a 50:50 mixture to provide rapid onset and prolonged postoperative analgesia, significantly reducing the patient's requirement for oral narcotics in the immediate postoperative period. The injection should be performed slowly, using a small-gauge needle (e.g., 25G or 27G), targeting the proper digital nerves at the base of the proximal phalanx.
Surgical Warning: The use of epinephrine in digital blocks is a subject of historical debate, but in the context of patients with known peripheral vascular disease, Raynaud's phenomenon, or severe microvascular compromise, it remains absolutely contraindicated. Epinephrine-induced vasospasm in a compromised digit can precipitate irreversible digital ischemia and subsequent necrosis.
Achieving a completely bloodless surgical field is mandatory. The germinal matrix is a translucent, highly vascularized tissue that is nearly impossible to distinguish from the surrounding sterile matrix and capsular tissues in a bloody field. Exsanguination of the digit is typically achieved using a sterile Esmarch bandage or a sterile glove finger with the tip excised, rolled proximally to the base of the digit to serve as a digital tourniquet. The tourniquet must be secured carefully to avoid excessive pressure on the neurovascular bundles. The surgeon must strictly adhere to a maximum tourniquet time of 30 to 45 minutes to prevent ischemic neuropraxia. Patient positioning is generally supine, with the foot positioned at the very edge of the operating table. High-intensity overhead lighting and the use of surgical loupe magnification (2.5x to 3.5x) are strongly recommended to ensure precise identification and complete excision of the microscopic lateral horns of the germinal matrix.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a total germinal matrix excision (the Quenu technique, with modifications by Fowler and Zadik) represents the gold standard for eradicating chronic, symptomatic onychomycosis or severe global dystrophy. The primary objective is to permanently remove the entire nail plate and the underlying germinal matrix while meticulously preserving the sterile matrix and the eponychial fold to ensure an acceptable cosmetic and functional outcome.
Step 1: Skin Incisions and Exposure
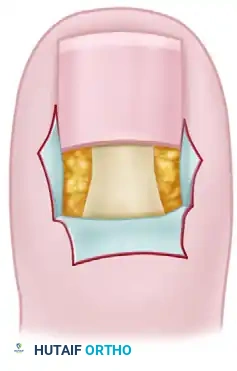
Following the confirmation of profound anesthesia and the establishment of a bloodless field via digital exsanguination, the surgical approach commences with precise incisions designed to mobilize the proximal nail fold. Two oblique incisions are made, extending proximally and slightly laterally from the proximal-lateral corners of the nail fold.

These incisions must be directed outward at approximately a 45-degree angle to avoid creating a narrow, ischemic flap. The depth of the incision is critical; it must be deep enough to completely release the eponychium from its lateral attachments, yet the surgeon must exercise extreme caution to avoid inadvertently transecting or damaging the underlying insertion of the extensor hallucis longus (EHL) tendon, which inserts into the dorsal base of the distal phalanx just proximal to the germinal matrix.

Step 2: Nail Plate Elevation and Extraction
Once the eponychial flap is mobilized, the entire nail plate must be atraumatically removed. A Freer elevator, or a specialized heavy nail elevator, is introduced beneath the free distal edge of the nail plate, gently separating the keratinized plate from the underlying, highly adherent sterile matrix.

The elevator is methodically advanced proximally in a sweeping motion until the entire nail plate is freed from its attachments to both the germinal matrix and the eponychial fold. Once completely mobilized, the nail plate is firmly grasped with a sturdy, straight hemostat and extracted using a rolling, rotational motion toward the midline. This rotational extraction minimizes trauma to the underlying matrix and ensures the plate is removed intact.
Step 3: Elevation of the Eponychial Flap and Matrix Identification
Using delicate skin hooks or fine-toothed forceps (e.g., Adson-Brown), the eponychial flap is carefully reflected proximally and held in retraction. This crucial maneuver exposes the entire proximal cul-de-sac and the underlying germinal matrix.
At this juncture, the surgeon must accurately differentiate the germinal matrix from the adjacent sterile (dormant) matrix. The germinal matrix typically presents as a thicker, slightly more opaque, and often protruding layer of tissue situated immediately beneath the reflected eponychium. In contrast, the sterile matrix is noticeably thinner, more translucent, and is firmly, immovably adherent to the periosteum of the distal phalanx. In cases of chronic, severe onychomycosis or long-standing dystrophy, the normal visual cues may be obscured, as the dormant matrix may appear grossly abnormal, hypertrophic, or deeply scarred by the chronic inflammatory process.
Step 4: Excision and Ablation of the Germinal Matrix
This step dictates the ultimate success or failure of the operation. A precise transverse incision is made with a #15 blade exactly at the junction of the germinal and sterile matrices, which corresponds anatomically to the distal border of the lunula. The germinal matrix is then sharply dissected off the underlying periosteum of the distal phalanx, working in a distal-to-proximal direction.
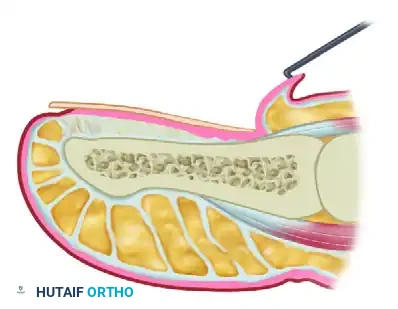
Surgical Pitfall: The lateral horns of the germinal matrix curve deeply and unpredictably into the proximal-lateral corners of the distal phalanx base. Failure to aggressively curette, sharply excise, or chemically ablate these hidden recesses will absolutely guarantee the formation of highly symptomatic postoperative spicules.
All germinal matrix tissue must be meticulously, completely removed down to bare periosteum. While sharp excision alone is theoretically sufficient if performed flawlessly, many experienced surgeons advocate for the adjunctive use of chemical cautery to ensure the absolute destruction of any microscopic cellular remnants.

If chemical matrixectomy is employed, an applicator soaked in 89% phenol or 10% sodium hydroxide is applied strictly to the proximal cul-de-sac for 2 to 3 minutes. Surrounding tissues must be protected with petroleum jelly, and the area must be profusely irrigated with alcohol (for phenol) or weak acetic acid (for sodium hydroxide) immediately following application to neutralize the chemical and prevent collateral tissue necrosis.

Step 5: Tissue Fixation and Closure Technique
Once complete excision is confirmed and absolute hemostasis is verified (often by temporarily releasing the digital tourniquet and applying targeted bipolar electrocautery to any bleeding vessels), the surgical site is prepared for closure. The eponychial flap is repositioned distally over the defect. The eponychium is fixed adjacent to the remaining dormant (sterile) matrix, essentially advancing it to cover the exposed periosteum left by the germinal matrix excision.

The oblique skin incisions are meticulously closed using fine, non-absorbable monofilament sutures (e.g., 4-0 or 5-0 nylon or prolene). The fixation of the eponychial flap must approximate the skin edges accurately but without excessive tension. Strangulation of the flap via overly tight sutures will inevitably lead to ischemic necrosis of the eponychium, resulting in severe scarring and a cosmetically unacceptable outcome.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following partial or total nail matrix removal can and do occur. The incidence of complications is directly correlated with the surgeon's experience, the thoroughness of the preoperative vascular assessment, and the patient's adherence to postoperative protocols. Anticipating these complications and understanding their salvage management is critical for any orthopedic surgeon performing perionychial procedures.
The most frequent and frustrating complication is the postoperative recurrence of nail spicules. This occurs when fragments of the germinal matrix, particularly within the deep lateral horns, are inadvertently retained during the primary excision. These cells continue to proliferate, forming a rigid, sharp shard of keratin that pierces the lateral nail fold or the eponychium. Spicule formation typically presents 3 to 6 months postoperatively as localized pain, swelling, and recurrent foreign-body granuloma formation. Salvage management requires a formal revision surgery; the spicule must be traced proximally to its source, and the offending matrix remnant must be aggressively excised or chemically ablated under direct visualization.
Surgical site infections (SSIs) represent another significant complication, ranging in severity from superficial cellulitis to deep space infections and osteomyelitis of the distal phalanx. Superficial infections are relatively common due to the inherently contaminated nature of the foot and the frequent presence of preexisting paronychia. These are typically managed successfully with oral antibiotics targeting common skin flora (e.g., Staphylococcus aureus) and warm saline soaks to promote local drainage. However, deep infections presenting with extreme throbbing pain, fluctuance, and systemic signs require immediate intervention, including partial or complete suture removal, deep wound culture, aggressive irrigation, and potentially intravenous antibiotic therapy.
Epidermal inclusion cysts are a rare but well-documented complication of perionychial surgery. They occur when viable epidermal cells are inadvertently driven deep into the dermal or subcutaneous layers during the surgical approach or suturing process. Over time, these cells proliferate and produce keratin, forming a slowly expanding, painful, fluctuant nodule beneath the eponychium or within the lateral fold. The definitive salvage management for an epidermal inclusion cyst is meticulous surgical enucleation, ensuring the complete removal of the cyst wall to prevent recurrence.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Nail Spicule Recurrence | 3% - 10% | Incomplete excision of germinal matrix lateral horns. | Revision surgery; targeted sharp excision and chemical ablation of the remnant matrix. |
| Superficial Infection | 2% - 5% | Poor post-op hygiene; premature return to closed footwear. | Oral antibiotics (e.g., Cephalexin, Clindamycin); warm saline soaks; topical antimicrobials. |
| Deep Infection / Osteomyelitis | < 1% | Unrecognized pre-op infection; compromised host immunity. | Suture removal for drainage; deep cultures; IV antibiotics; rarely, terminal amputation. |
| Eponychial Flap Necrosis | 1% - 2% | Excessive suture tension; tourniquet ischemia; severe PAD. | Allow to demarcate; local wound care; secondary intention healing; avoid premature debridement. |
| Epidermal Inclusion Cyst | < 1% | Epidermal cells buried during incision or tight suturing. | Surgical enucleation of the entire cyst capsule under local anesthesia. |
| Prolonged Hyperesthesia | 2% - 4% | Iatrogenic injury to proper digital nerve branches. | Desensitization therapy; gabapentinoids; topical lidocaine patches; time. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management following nail matrix removal is arguably as critical as the surgical execution itself. A structured, phased rehabilitation protocol ensures optimal wound healing, minimizes the risk of complications, and maximizes long-term patient satisfaction. The protocol must be clearly communicated to the patient preoperatively to set realistic expectations regarding the recovery timeline and functional limitations.
Phase 1: Immediate Postoperative Care (Days 0 to 3)
The immediate postoperative phase is focused on pain control, edema management, and protecting the fragile surgical site. In the operating room, a non-adherent, heavily lubricated dressing (such as Adaptic, Xeroform, or a petrolatum-impregnated gauze) is applied directly over the exposed sterile matrix and the sutured eponychial incisions. This prevents the secondary dressing from adhering to the raw wound bed, which would cause severe pain and disrupt early epithelialization during the first dressing change. This primary layer is followed by sterile fluffed gauze and a mildly compressive cohesive bandage (e.g., Coban) to provide gentle hemostatic pressure.
The patient must be instructed to keep the foot strictly elevated above heart level for the first 48 to 72 hours. This strict elevation is the most effective method for minimizing throbbing pain, reducing digital edema, and preventing the formation of a postoperative hematoma beneath the eponychial flap. Analgesia is typically achieved with a multimodal approach; scheduled oral NSAIDs and acetaminophen are usually sufficient, though a short course of stronger breakthrough analgesics may be required for the first 24 hours.
Phase 2: Intermediate Healing and Suture Removal (Days 4 to 14)
The first dressing change is typically performed between postoperative days 3 and 5. The patient is instructed to soak the foot in warm water or a dilute Epsom salt solution to gently loosen the dressing before removal. Following the dressing change, daily soaks followed by the application of a topical antibiotic ointment and a simple adhesive bandage are initiated.
Patient education regarding footwear during this phase is paramount and non-negotiable. The patient must be explicitly instructed not to wear any closed-toe shoe—even if the toe box is exceptionally wide or the shoe is oversized—for a minimum of 10 to 14 days. Premature use of closed footwear causes direct micro-trauma and shear forces on the healing eponychial flap, drastically increasing the risk of wound dehiscence and surgical site infection. Sutures are typically removed between days 10 and 14, once the eponychial incisions demonstrate
Clinical & Radiographic Imaging Archive

