Calcaneal Osteotomy: Dwyer & Crescentic Techniques
Key Takeaway
Calcaneal osteotomies, including the Dwyer lateral closing wedge and Samilson crescentic techniques, are powerful procedures for correcting complex hindfoot deformities such as cavovarus and calcaneocavus. This comprehensive surgical guide details the biomechanical principles, precise operative steps, and postoperative protocols required to achieve optimal multiplanar correction, restore plantigrade alignment, and mitigate complications in both neurogenic and traumatic foot deformities.
Comprehensive Introduction and Patho-Epidemiology
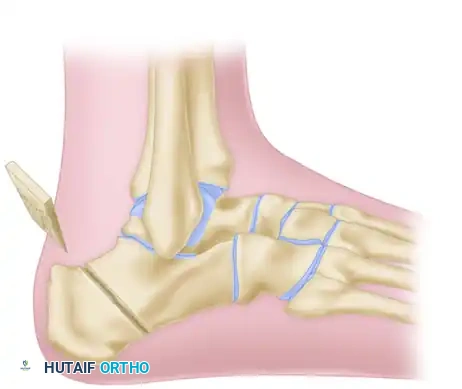
The calcaneus serves as the foundational osseous structure of the hindfoot, dictating the alignment, biomechanics, and force transmission of the entire lower extremity during the gait cycle. It acts as the primary posterior pillar of the foot's longitudinal arch, functioning in concert with the midfoot and forefoot to create a stable tripod for weight-bearing. Malalignment of the calcaneus—whether in varus, valgus, or severe cavus—profoundly alters the biomechanics of the subtalar and transverse tarsal joints. When the calcaneus is locked in a non-physiologic position, the compensatory mechanisms of the foot are exhausted, leading to progressive articular degeneration, ligamentous attenuation, and debilitating pain. Calcaneal osteotomies are powerful, joint-sparing procedures designed to extra-articularly realign the mechanical axis of the hindfoot, thereby preserving subtalar motion while restoring a plantigrade, biomechanically sound foot.
Surgical intervention via calcaneal osteotomy is primarily indicated for complex, multiplanar deformities such as the cavovarus foot and the calcaneocavus foot. The cavovarus deformity is most frequently encountered in the setting of hereditary sensorimotor neuropathies, predominantly Charcot-Marie-Tooth (CMT) disease. In CMT, the pathoanatomy is driven by a predictable sequence of muscle imbalances: the peroneus longus overpowers the weakened tibialis anterior, driving the first metatarsal into rigid plantarflexion. Concurrently, the tibialis posterior overpowers the weakened peroneus brevis, initiating hindfoot varus. Over time, what begins as a flexible, forefoot-driven hindfoot varus rigidifies into a fixed osseous deformity due to contracture of the plantar fascia and capsular structures. The Dwyer lateral closing wedge osteotomy was specifically designed to address this fixed hindfoot varus by extra-articularly realigning the calcaneal tuberosity, moving the ground reaction force lateral to the subtalar joint axis, and restoring the eversion capacity of the hindfoot.
Conversely, the calcaneocavus foot presents a distinctly different patho-epidemiological profile. This deformity is classically a sequela of poliomyelitis, spinal dysraphism, or isolated triceps surae weakness. The loss of Achilles tendon function leads to unopposed dorsiflexion of the calcaneus by the anterior compartment musculature, resulting in a steeply pitched, verticalized calcaneus and a profoundly high longitudinal arch. The posterior lever arm of the calcaneus is effectively shortened, severely compromising push-off power during the terminal stance phase of gait. To address this, the Samilson crescentic osteotomy was developed. Unlike the Dwyer procedure, which primarily corrects coronal plane varus, the Samilson osteotomy is a sagittal plane correction that translates the posterior calcaneal tuberosity superiorly and posteriorly, thereby flattening the calcaneal pitch, lengthening the Achilles lever arm, and restoring the mechanical advantage of the calf musculature.
The evolution of these extra-articular osteotomies represents a paradigm shift in orthopedic foot and ankle surgery, moving away from the historical reliance on triple arthrodesis for deformity correction. While arthrodesis reliably corrects deformity, it does so at the cost of joint mobility, leading to adjacent joint arthrosis, particularly at the ankle and midfoot. By utilizing procedures like the Dwyer and Samilson osteotomies, the modern orthopedic surgeon can achieve profound multiplanar correction, preserve essential subtalar and transverse tarsal kinematics, and significantly enhance the longevity and function of the patient's native foot.
Detailed Surgical Anatomy and Biomechanics
Osseous and Articular Anatomy
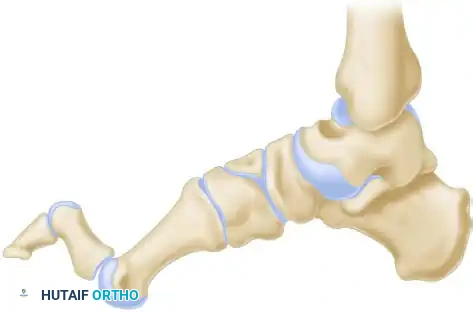
The calcaneus is the largest of the tarsal bones, featuring a complex three-dimensional geometry designed to withstand immense compressive and tensile loads. The bone is structurally divided into the anterior process, the body, and the posterior tuberosity. The superior surface articulates with the talus via three distinct facets—anterior, middle, and posterior. The posterior facet is the largest and most critical for weight-bearing, supported by a dense trabecular network known as the thalamic portion of the calcaneus. Just anterior to the posterior facet lies the calcaneal sulcus, which forms the floor of the sinus tarsi. When planning a Dwyer or Samilson osteotomy, the surgeon must maintain a precise spatial awareness of the posterior facet to avoid iatrogenic intra-articular violation. The osteotomy must be strictly confined to the extra-articular extra-thalamic posterior tuberosity, which consists primarily of highly vascular cancellous bone enclosed in a thin cortical shell. This vascularity ensures rapid osseous union but also predisposes the bone to significant intraoperative bleeding.
Neurovascular and Soft Tissue Considerations
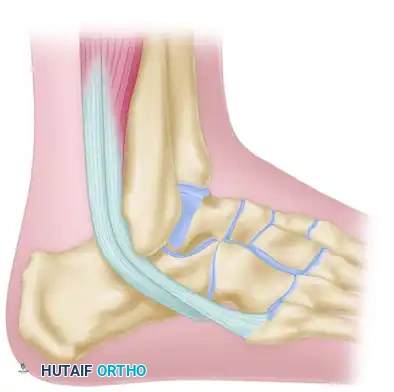
The lateral aspect of the calcaneus, the primary surgical corridor for these osteotomies, is intimately associated with several critical soft tissue structures. The peroneal tubercle separates the peroneus brevis (superior) and peroneus longus (inferior) tendons. These tendons must be meticulously mobilized and protected during lateral exposure. The sural nerve and the lesser saphenous vein course obliquely across the lateral hindfoot. The sural nerve typically divides into the lateral dorsal cutaneous nerve and the lateral calcaneal branches. Injury to the sural nerve or its branches during incision, retraction, or osteotomy execution is a devastating complication, leading to intractable neuroma formation. Medially, the neurovascular bundle (posterior tibial artery and tibial nerve) courses behind the medial malleolus and divides into the medial and lateral plantar branches. During a Dwyer osteotomy, preserving the medial periosteal hinge is not only critical for biomechanical stability but also serves as a vital physical barrier protecting these medial neurovascular structures from the oscillating saw blade.
Biomechanics of the Hindfoot
The biomechanical rationale for calcaneal osteotomies is rooted in the manipulation of the subtalar joint axis and the alteration of ground reaction forces (GRF). The subtalar joint axis runs obliquely from posterolateral-inferior to anteromedial-superior. In a normal plantigrade foot, the GRF passes slightly medial to the center of the calcaneal tuberosity, creating a mild eversion moment that unlocks the transverse tarsal joints, allowing the foot to accommodate uneven terrain. In a severe cavovarus foot, the calcaneal tuberosity is inverted, shifting the GRF lateral to the subtalar axis. This creates a powerful, self-perpetuating inversion moment that locks the transverse tarsal joints, resulting in a rigid, shock-absorbing deficient foot. The Dwyer lateral closing wedge osteotomy physically translates and angulates the tuberosity laterally, shifting the GRF back medial to the subtalar axis, thereby restoring the normal eversion moment.
In the sagittal plane, the calcaneocavus deformity drastically alters the lever arm of the Achilles tendon. The calcaneal pitch angle, normally between 20 and 30 degrees, can exceed 40 to 50 degrees in a calcaneocavus foot. This verticalization moves the insertion of the Achilles tendon closer to the axis of rotation of the ankle joint, exponentially decreasing its mechanical advantage and resulting in a weak, inefficient push-off. The Samilson crescentic osteotomy addresses this by sliding the posterior tuberosity superiorly and posteriorly along a curvilinear path. This maneuver not only decreases the calcaneal pitch angle but also significantly increases the distance from the ankle joint axis of rotation to the Achilles insertion, thereby restoring the moment arm and optimizing the length-tension relationship of the triceps surae complex.
Exhaustive Indications and Contraindications
Patient selection is the most critical determinant of success in extra-articular calcaneal osteotomies. The decision to perform a Dwyer, Samilson, or adjunctive procedure must be based on a comprehensive understanding of the deformity's flexibility, the integrity of the adjacent joints, and the patient's overall functional demands and neurologic status.
Indications for Intervention
The primary indication for a Dwyer lateral closing wedge osteotomy is a rigid, fixed hindfoot varus deformity. This is most commonly seen in the mature cavovarus foot associated with Charcot-Marie-Tooth disease, Friedreich’s ataxia, or as a late complication of neglected or overcorrected clubfoot. It is also indicated in post-traumatic scenarios, such as malunited calcaneal fractures resulting in severe varus malalignment. Crucially, the Dwyer osteotomy is indicated only when the subtalar joint is free of advanced osteoarthritic changes; if significant arthrosis is present, a subtalar or triple arthrodesis is the mandated procedure. The Samilson crescentic osteotomy has a much narrower set of indications. It is reserved almost exclusively for ambulatory patients with symptomatic calcaneocavus deformities, typically secondary to poliomyelitis or isolated triceps surae weakness, where the apex of the cavus is posterior to the midtarsus and the calcaneus is vertically oriented.
Contraindications to Joint-Sparing Osteotomies
Contraindications to extra-articular calcaneal osteotomies can be absolute or relative. Absolute contraindications include advanced subtalar or transverse tarsal arthritis, severe peripheral vascular disease, active deep infection, and Charcot neuroarthropathy of the hindfoot. In these scenarios, arthrodesis or amputation are the only viable reconstructive options. Relative contraindications include profound osteopenia (which compromises hardware fixation), uncontrolled diabetes mellitus (which significantly increases the risk of wound dehiscence and nonunion), and a purely flexible hindfoot varus that corrects entirely with a Coleman block test. In the latter case, the varus is purely compensatory to a plantarflexed first ray, and isolated forefoot or midfoot procedures (e.g., first metatarsal dorsiflexion osteotomy) may suffice without the need to violate the calcaneus.
| Parameter | Indications | Contraindications |
|---|---|---|
| Dwyer Osteotomy | Fixed hindfoot varus; Neurologic cavovarus (CMT); Post-traumatic varus malunion; Clubfoot overcorrection sequelae. | Flexible hindfoot varus (forefoot driven); Subtalar arthritis; Active infection; Severe peripheral neuropathy/Charcot. |
| Samilson Osteotomy | Symptomatic calcaneocavus; Polio sequelae; Isolated triceps surae weakness; Vertical calcaneus with apex posterior to midtarsus. | Anterior cavus deformity (midfoot/forefoot driven); Degenerative joint disease; Non-ambulatory patient status. |
| Reverse Evans | Traumatic cavovarus with lateral column overlength; Preserved midtarsal motion requirement. | Medial column shortening; Arthritic talonavicular or calcaneocuboid joints. |
| Triple Arthrodesis | Severe, rigid, multiplanar equinocavovarus; Concomitant hindfoot/midfoot arthritis; Failed prior osteotomies. | Young, active patients with preserved joint cartilage (relative); Flexible deformities. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and the Coleman Block Test
Thorough preoperative clinical evaluation is mandatory to dissect the components of a complex hindfoot deformity. The examination begins with observing the patient's gait, noting the presence of a lateral thrust, foot drop, or lack of heel push-off. The Silfverskiöld test is performed to assess for gastrocnemius or Achilles contracture, which frequently accompanies cavovarus deformities. The cornerstone of the clinical exam is the Coleman block test. The patient stands with the lateral border of the foot (heel and lateral rays) on a 1-inch wooden block, allowing the first metatarsal to drop freely off the medial edge. If the hindfoot varus corrects to neutral or valgus while on the block, the deformity is forefoot-driven (flexible), and a calcaneal osteotomy may be avoided. If the hindfoot remains in varus, the deformity is fixed, definitively indicating the need for a Dwyer osteotomy or similar hindfoot correction.
Radiographic Evaluation and Templating
Standard weight-bearing radiographs, including anteroposterior (AP), lateral, and axial (Harris) heel views, are non-negotiable. The lateral view is utilized to assess Meary’s angle (talo-first metatarsal angle), the calcaneal pitch, and the presence of a calcaneocavus deformity. In a normal foot, Meary's angle is 0 degrees; in a cavus foot, the angle intersects superiorly. The axial heel view or a Saltzman hindfoot alignment view is critical for quantifying the degree of coronal plane varus. Preoperative digital templating is essential to determine the precise size and angle of the wedge to be resected in a Dwyer osteotomy. Typically, an 8 to 12 mm laterally based wedge is required to correct a standard fixed varus deformity. For the Samilson osteotomy, templating involves mapping the crescentic arc posterior to the subtalar joint to ensure adequate superior and posterior translation of the tuberosity without violating the articular surface.
Patient Positioning and Operating Room Setup
Proper patient positioning is vital for optimal exposure and execution of the osteotomies. For the Dwyer osteotomy, the patient is typically placed in the lateral decubitus position, heavily padded, with the operative leg uppermost. Alternatively, a supine position with a large bump under the ipsilateral hip to internally rotate the leg can be utilized, though this may make access to the posterior heel more challenging. A high-thigh pneumatic tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying and protecting the sural nerve. For the Samilson crescentic osteotomy, the lateral decubitus position is almost exclusively preferred, as it provides unrestricted access to the posterior tuberosity and allows for the precise curvilinear saw cuts required. Intraoperative fluoroscopy (C-arm) must be positioned to allow for unencumbered AP, lateral, and axial views of the hindfoot throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The Dwyer Lateral Closing Wedge Osteotomy
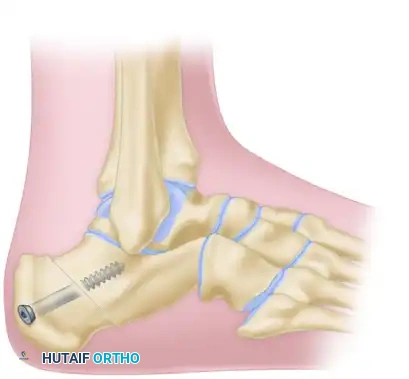
The procedure frequently begins with a release of the plantar fascia, as contracture of this structure acts as a bowstring, maintaining the cavus deformity. The plantar fascia is divided subcutaneously or through a small medial incision to reduce the drop of the forefoot and release the tethering effect on the medial longitudinal arch. Following this, attention is turned to the lateral calcaneus. An oblique or curved incision is made paralleling the peroneus longus tendon, maintaining a distance of approximately 1 cm posterior and inferior to it. Meticulous blunt dissection is required in the subcutaneous tissues to identify, mobilize, and protect the sural nerve. The entire fasciocutaneous flap is turned anteriorly until the tendon of the peroneus longus muscle is fully exposed.
Once the lateral wall of the calcaneus is exposed, the periosteum is stripped from the superior, lateral, and inferior surfaces using a Cobb elevator. Retractors are placed superiorly and inferiorly to protect the peroneal tendons and plantar structures. The osteotomy is then executed. A laterally based wedge of bone is removed from the calcaneus just inferior and posterior to the peroneus longus tendon, keeping the cuts parallel with the tendon's course.

The base of the lateral wedge is typically 8 to 12 mm wide, dictated by preoperative templating. The cuts are tapered medially to, but not through, the medial cortex. Preserving the medial periosteal hinge is critical; it provides inherent stability and acts as a fulcrum for closure, while also protecting the medial neurovascular bundle. The medial cortex is then carefully broken using a greenstick fracture technique. The osteotomy gap is closed by bringing the bony surfaces snugly together, often facilitated by pressing the forefoot into dorsiflexion against the pull of the Achilles tendon.

Failure to obtain complete closure of the lateral gap is almost always caused by a small, retained piece of bone left behind at the medial apex of the wedge. A small curette or rongeur must be used to clear the apex if resistance is met. Once closed, the osteotomy is secured with rigid internal fixation, typically utilizing one or two large-fragment cannulated screws (6.5 mm or 7.3 mm) directed from the posterior-inferior tuberosity into the anterior calcaneal body, or a dedicated titanium calcaneal step-plate.
Management of Combined Deformities
In patients with CMT, a Dwyer osteotomy alone is rarely sufficient. Because the deformity is driven by a plantarflexed first ray, a concomitant dorsal closing wedge osteotomy at the base of the first metatarsal is frequently required to address the forefoot pronation.
Initial small wedge (3 to 4 mm) is resected from the base of the first metatarsal.

The wedge is increased as necessary to bring the first metatarsal to a plantigrade position post-osteotomy.
For severe, rigid, multiplanar equinocavovarus deformities with arthritic changes, a triple arthrodesis is mandated. This involves precise biplanar wedge resections from the midtarsal and subtalar joints to correct adduction, cavus, and varus simultaneously.

A, Wedge with its base lateral (colored area) is resected from the midtarsal region to correct the adduction and cavus deformity of the forefoot.

B, Wedge with its base lateral (colored area) is resected from the subtalar region to correct the varus deformity of the hindfoot.



C and D, Position of the bones after surgery, demonstrating a restored plantigrade alignment and neutral hindfoot.
The Crescentic Calcaneal Osteotomy (Samilson Technique)
For the calcaneocavus deformity, the Samilson technique is employed. The patient is positioned laterally, and an obliquely placed lateral incision is made over the posterior tuberosity of the calcaneus, posterior to the subtalar joint.
A, The oblique lateral incision is planned posterior to the subtalar joint and peroneal tendons.
Deep dissection is carried down to the lateral wall, ensuring the peroneal tendons remain anterior and protected.
B, Exposure of the lateral calcaneal wall, preparing for the crescentic cut.
Using a specialized crescentic saw blade, the osteotomy is initiated posterior to the posterior facet of the subtalar joint. The concavity of the cut must face posteriorly and inferiorly.
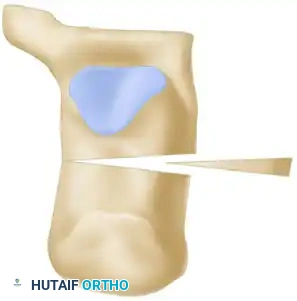
C, The crescentic osteotomy is executed, ensuring the subtalar joint is not violated.
Once the osteotomy is complete through both cortices, the posterior tuberosity fragment is mobilized. It is then translated superiorly and posteriorly along the crescentic arc, decreasing the calcaneal pitch angle and lengthening the posterior lever arm.

D, The posterior tuberosity is displaced superiorly along the crescentic path to correct the calcaneocavus deformity.
Rigid internal fixation is then achieved, typically with two large-fragment cannulated screws directed from the posterior-inferior tuberosity into the anterior body of the calcaneus.
E, Final rigid internal fixation of the Samilson crescentic osteotomy.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, calcaneal osteotomies carry a distinct profile of perioperative and postoperative complications. The surgeon must be acutely aware of these risks, employ preventative strategies, and possess the armamentarium to execute salvage procedures when necessary.
Neurologic and Soft Tissue Complications
Sural nerve injury is the most frequently cited complication following lateral calcaneal approaches, with incidence rates reported between 5% and 15% in the literature. The nerve is highly vulnerable to direct transection, traction neuropraxia from aggressive retraction, or entrapment in the surgical scar. Injury results in painful neuroma formation or debilitating dysesthesias along the lateral border of the foot. Prevention relies on meticulous blunt dissection and the use of atraumatic retraction techniques. Wound dehiscence and skin necrosis are also significant concerns, particularly given the tenuous angiosome of the lateral hindfoot. The skin flap must be handled as a full-thickness fasciocutaneous unit, avoiding excessive undermining. Early weight-bearing or excessive postoperative edema can rapidly compromise flap viability, leading to deep infection.
Osseous and Biomechanical Complications
Undercorrection of the deformity is a common pitfall, particularly in the Dwyer procedure. This typically occurs if the medial cortex is not adequately hinged, if bone debris is left at the apex of the wedge, or if the surgeon fails to address concomitant forefoot pathology (e.g., a plantarflexed first ray). Undercorrection leaves the patient with residual varus, perpetuating lateral column overload and progressive joint degeneration. Conversely, overcorrection into valgus, while less common, can lead to subfibular impingement and acquired flatfoot deformity. Nonunion is relatively rare (less than 3%) due to the highly vascular cancellous bone of the calcaneal tuberosity, but delayed union can occur, particularly in smokers or patients with non-compliant weight-bearing status.
Salvage Management Strategies
When complications arise, definitive salvage management is required. For a painful sural neuroma that fails conservative management (gabapentinoids, targeted injections), surgical excision and proximal burying of the nerve stump into the muscle belly of the peroneus brevis or gastrocnemius is indicated. In cases of severe undercorrection or symptomatic nonunion, revision surgery is mandatory. If the adjacent joints remain pristine, a revision osteotomy with structural bone grafting and robust plate fixation may be attempted. However, if the subtalar joint has developed secondary arthrosis due to chronic malalignment, the definitive salvage procedure is a subtalar arthrodesis or a triple arthrodesis, which reliably corrects the deformity and eliminates arthritic pain at the cost of hindfoot motion.
| Complication | Incidence Rate | Preventative Strategy | Salvage Management |
|---|---|---|---|
| Sural Nerve Injury | 5% - 15% | Meticulous blunt dissection; Atraumatic retraction; Full-thickness flaps. | Neuroma excision and proximal muscle burying. |
| Wound Dehiscence / Necrosis | 3% - 8% | Avoid excessive undermining; Strict elevation post-op; Delayed suture removal (3 weeks). | Local wound care; Vacuum-assisted closure; Sural artery flap (severe). |
| Undercorrection | 10% - 20% | Clear medial apex debris; Ensure greenstick fracture; Address 1st ray pathology. | Revision osteotomy; Subtalar/Triple arthrodesis if arthritic. |
| Nonunion / Delayed Union | < 3% | Rigid internal fixation (screws/plates); Strict non-weight-bearing protocol; Smoking cessation. | Revision internal fixation with autologous bone grafting; Bone stimulator. |
Phased Post-Operative Rehabilitation Protocols
The success of a calcaneal osteotomy is inextricably linked to strict adherence to a phased postoperative rehabilitation protocol. The calcaneus, while highly vascular, is subjected to immense biomechanical forces. Premature weight-bearing can lead to catastrophic failure of fixation, loss of correction, or delayed union. The rehabilitation protocol must balance the need for rigid immobilization to facilitate osseous healing with the necessity of early motion to prevent debilitating joint stiffness.
Phase I: Immediate Postoperative Period (0-2 Weeks)
Immediately following surgery, the foot and ankle are immobilized in a well-padded, short-leg splint in a neutral position (or slight dorsiflexion to relax the Achilles tension on the posterior fragment). The patient is made strictly non-weight-bearing (NWB) on the operative extremity. The paramount goals of this phase are wound healing and edema control. The lateral calcaneal incision is notoriously prone to delayed healing; therefore, strict elevation of the limb above the level of the heart is enforced. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk stratification.
Phase II: Immobilization and Early Healing (2-6 Weeks)
At the two-week postoperative mark, the initial splint is removed, and the surgical wounds are meticulously inspected. Assuming the incision is fully healed and dry, sutures or staples are removed. If there is any question regarding wound integrity, suture removal is delayed until week three. The patient is then transitioned to a short-leg fiberglass cast or a rigid controlled ankle motion (CAM) boot. The patient remains strictly NWB. During this phase, isometric exercises for the proximal musculature (quadriceps, hamstrings, gluteals) are encouraged to prevent profound deconditioning.
Phase III: Progressive Loading and Mobilization (6-10 Weeks)
At six weeks postoperatively, the first set of follow-up radiographs (AP, lateral, and axial views) is obtained. The surgeon evaluates for evidence of bridging trabecular callus and obliteration of the osteotomy line. If radiographic progression of union is satisfactory, the patient is cleared to begin progressive partial weight-bearing (PWB) in the CAM boot, typically advancing by 25% of body weight per week. Formal physical therapy is initiated. The focus of therapy shifts to restoring active and passive range of motion at the ankle, subtalar, and transverse tarsal joints. Gentle intrinsic foot muscle strengthening and proprioceptive training are also introduced.
Phase IV: Return to Function (10+ Weeks)
By 10 to 12 weeks, assuming complete clinical and radiographic union, the patient is transitioned out of the CAM boot and into regular, supportive footwear. Custom orthotics or a slight heel lift may be prescribed to accommodate any residual minor limb length discrepancies or to support the newly reconstructed arch. Physical therapy intensifies, focusing on closed-kinetic-chain exercises, eccentric triceps surae strengthening, and advanced gait retraining. Full return to high-impact athletic activity or heavy manual labor is generally restricted until 4 to 6 months postoperatively, contingent upon the complete restoration of calf strength, pain-free subtalar motion, and uncompromised radiographic union.
Summary of Landmark Literature and Clinical Guidelines
The foundation of extra-articular calcaneal osteotomies rests upon several landmark papers that have
