Operative Management of Talar Fractures: A Comprehensive Surgical Guide
Key Takeaway
Talar fractures present complex challenges due to the tenuous retrograde blood supply of the talus, predisposing patients to osteonecrosis and post-traumatic arthritis. Successful management requires precise anatomical reduction, rigid internal fixation, and careful handling of soft tissues. This guide details the biomechanics, surgical indications, step-by-step operative approaches, and postoperative protocols for talar neck, body, and osteochondral fractures, ensuring optimal outcomes in both pediatric and adult populations.
Comprehensive Introduction and Patho-Epidemiology
Fractures of the talus represent a formidable challenge in orthopedic traumatology, demanding an exacting understanding of complex three-dimensional anatomy and joint mechanics. As the primary mechanical link between the leg and the foot, the talus is responsible for transmitting the entire weight of the body across the ankle and subtalar joints. The patho-epidemiology of these injuries is inextricably linked to high-energy trauma, most frequently observed in motor vehicle collisions, motorcycle accidents, and falls from significant heights. The classic "aviator's astragalus," originally described in early aviation crashes, perfectly illustrates the mechanism of high-energy hyperdorsiflexion. In this scenario, the talar neck is violently driven against the anterior lip of the tibial plafond, acting as a fulcrum that leads to transverse fracture and subsequent dorsal displacement or dislocation of the talar body.
Talar fractures are broadly categorized into three basic anatomical types: fractures of the neck, fractures of the body and dome, and fractures of the lateral, medial, or posterior processes. Talar neck fractures remain the most common presentation, accounting for approximately 50% of all talar fractures. Fractures of the lateral process, often dubbed the "snowboarder's fracture," have seen a dramatic epidemiological increase over the past three decades due to the rising popularity of the sport. The mechanism typically involves profound axial loading combined with dorsiflexion and eversion. These process fractures are notoriously difficult to visualize on standard plain radiographs, necessitating a high index of suspicion when a patient presents with persistent lateral subtalar pain mimicking a severe ankle sprain.
Pediatric talar fractures present a distinct pathophysiological entity. Talar neck fractures in children behave differently than in adults due to the presence of open physes, a thicker cartilaginous envelope, and a highly reactive vascular bed. While osteonecrosis can still occur in the pediatric population following severe displacement, the pediatric talus demonstrates a remarkable capacity for spontaneous revascularization and remodeling. In our institutional evaluation of pediatric patients, those who developed osteonecrosis presented with a sclerotic lesion in the dome and body of the talus that subsequently evolved into a cystic lesion on radiographs. Over a 2- to 3-year period, the area typically resolved, and the vast majority remained completely asymptomatic at long-term follow-up.
Most children with osteonecrosis do not require aggressive surgical intervention. A prolonged period of non-weight-bearing or the use of a patellar tendon-bearing, weight-relieving brace should be strictly trialed before any surgical intervention is considered. The natural history of pediatric talar avascular necrosis favors conservative management, provided that articular congruity has been maintained or anatomically restored following the initial injury.

Detailed Surgical Anatomy and Biomechanics
The talus is an anatomical anomaly within the human skeleton, uniquely designed to facilitate multi-planar motion while bearing immense axial loads. Approximately 60% of the talar surface is covered by hyaline articular cartilage, articulating with the tibia, fibula, calcaneus, and navicular. This extensive cartilaginous coverage leaves a severely limited vascular footprint for nutrient arterial inflow. Furthermore, the complete absence of muscular or tendinous attachments means the talus is devoid of a reliable secondary soft-tissue blood supply, relying entirely on a tenuous, retrograde extraosseous vascular network.
The extraosseous blood supply is derived from three primary sources: the artery of the tarsal canal (a branch of the posterior tibial artery), the artery of the sinus tarsi (an anastomotic sling formed by branches of the perforating peroneal and dorsalis pedis arteries), and the superior neck vessels from the anterior tibial artery. The artery of the tarsal canal is the most critical, supplying the vast majority of the talar body. Because the intraosseous blood flow proceeds in a retrograde fashion—from the distal neck proximally into the body—any fracture through the talar neck inherently disrupts this primary vascular conduit. Disruption of this network during high-energy trauma frequently leads to osteonecrosis (avascular necrosis), subsequent structural collapse, malunion, and debilitating post-traumatic arthritis.

Biomechanically, the talus acts as a dynamic intercalated segment. During the gait cycle, it converts the transverse plane rotation of the lower extremity into sagittal and coronal plane motion of the foot. The subtalar joint, functioning as a complex mitered hinge, allows for inversion and eversion, which is crucial for accommodating uneven terrain. Any malalignment of the talar neck, particularly varus malunion, profoundly alters these biomechanics. A varus deformity of the talar neck locks the transverse tarsal joint, effectively eliminating the foot's ability to act as a supple shock absorber during heel strike, and rapidly leads to lateral column overload and progressive peritalar arthritis.
Osteochondral lesions of the talus (OLT), historically termed osteochondritis dissecans, further highlight the intricate biomechanical vulnerabilities of the talar dome. Morphologically and etiologically, medial and lateral lesions differ significantly due to distinct biomechanical forces. Lateral lesions are almost exclusively caused by trauma, typically shear forces during inversion and dorsiflexion. They are typically thin, wafer-shaped, and resemble acute osteochondral shear fractures. Conversely, medial lesions often have an insidious onset with no distinct history of trauma, suggesting an ischemic or repetitive micro-traumatic etiology. Medial lesions are typically deep, cup-shaped, and located on the posterior aspect of the medial talar dome.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in talar fractures hinges on precise anatomical classification, the degree of displacement, and the physiological status of the patient. The overarching goal of surgical management is the absolute anatomical restoration of articular surfaces and the realignment of the talar neck to prevent varus malunion and subsequent biomechanical failure. Non-operative management is strictly reserved for truly non-displaced fractures, which are exceedingly rare and must be confirmed with advanced computed tomography (CT) imaging.
For talar neck fractures, the Hawkins classification dictates operative indications. Hawkins Type I fractures (non-displaced) may be treated in a non-weight-bearing cast, but any displacement greater than 2 millimeters, or any evidence of varus angulation, immediately elevates the injury to a Type II (subtalar subluxation) or Type III (subtalar and tibiotalar dislocation) fracture, mandating open reduction and internal fixation (ORIF). Type IV fractures, which include talonavicular subluxation or dislocation, represent catastrophic energy transfer and require emergent reduction and rigid fixation.
Fractures of the lateral process follow a similar paradigm. Nondisplaced fragments can be treated successfully with closed cast immobilization. However, large displaced fragments (>1 cm or >2 mm of displacement) require ORIF to restore the subtalar joint surface and prevent lateral impingement. Small, highly comminuted displaced fragments that are not amenable to screw fixation should be excised primarily to prevent the development of painful subtalar arthritis and mechanical block to eversion.
| Clinical Scenario | Primary Indications for Operative Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Talar Neck Fractures | Displacement > 2mm, Varus malalignment, Hawkins Type II, III, IV, Open fractures | Active profound systemic infection, Medically unstable for anesthesia | Severe peripheral vascular disease, Severe baseline neuropathy (Charcot) |
| Talar Body Fractures | Intra-articular step-off > 1-2mm, Comminution leading to widening of the mortise | Non-ambulatory patient status, Overlying compromised soft tissue envelope (until healed) | Osteopenia precluding hardware purchase, Heavy smoking history |
| Lateral Process Fractures | Large fragment (>1cm), Displacement > 2mm, Subtalar joint incongruity | Truly non-displaced fractures verifiable on CT | Minimal displacement in a low-demand patient |
| Osteochondral Lesions (OLT) | Stage III lateral lesions, Stage IV loose bodies, "Inverted" floating fragments | Asymptomatic incidental findings | Stage I/II lesions without a trial of conservative bracing |
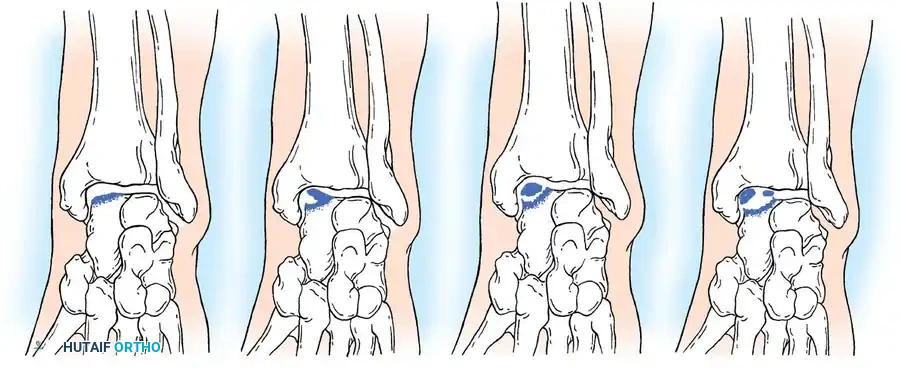
In the context of Osteochondral Lesions of the Talus (OLT), the widely accepted classification system by Berndt and Harty categorizes these lesions into four stages based on radiographic appearance. Operative management is strongly recommended for Stage III lateral lesions (which have notoriously poor healing rates with conservative care) and all Stage IV lesions (displaced fragments loose within the joint). Furthermore, any fragment identified on imaging as "inverted" requires immediate surgical excision, as spontaneous healing is biologically impossible when the subchondral bone faces the joint space.

Pre-Operative Planning, Templating, and Patient Positioning
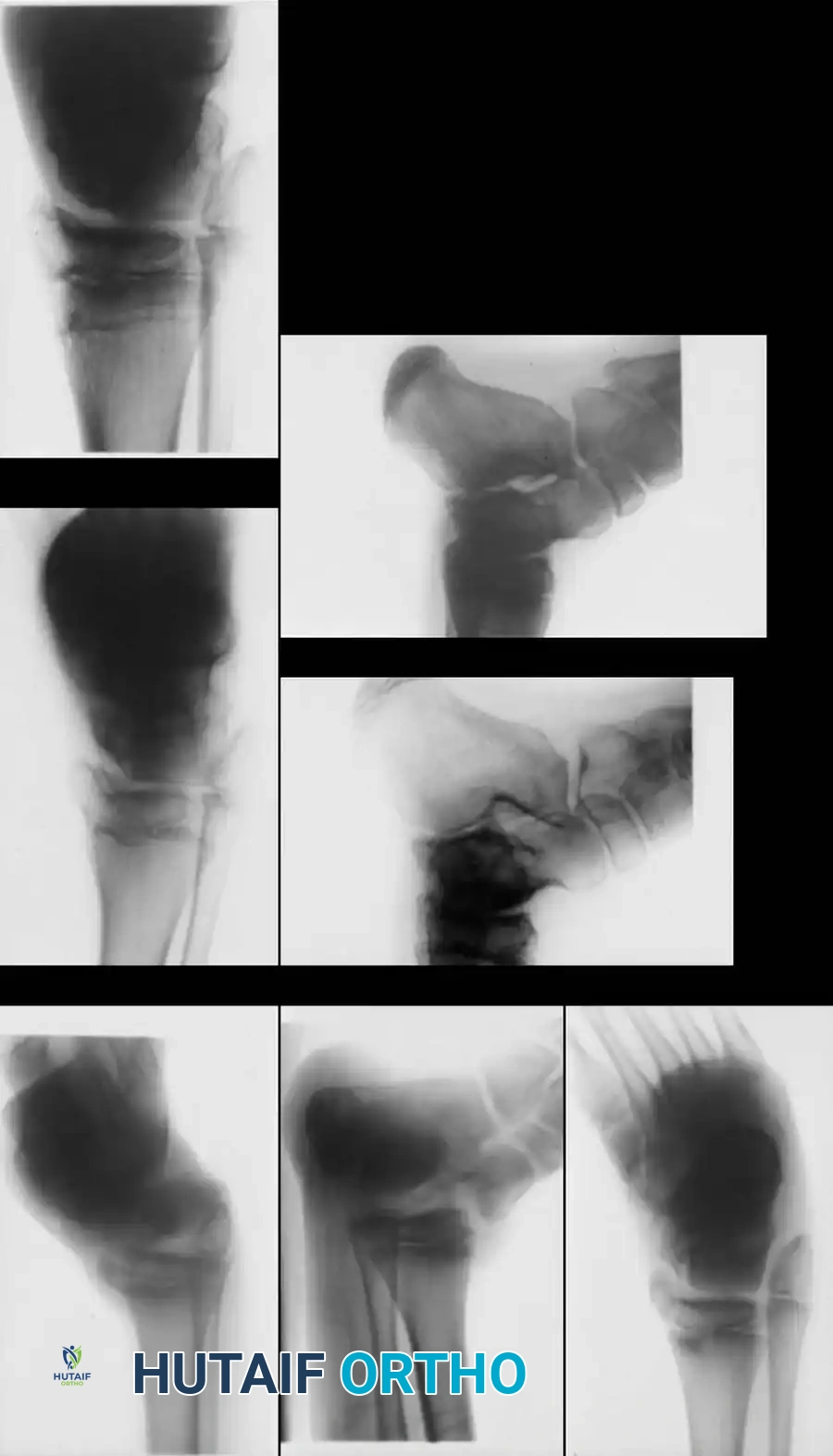
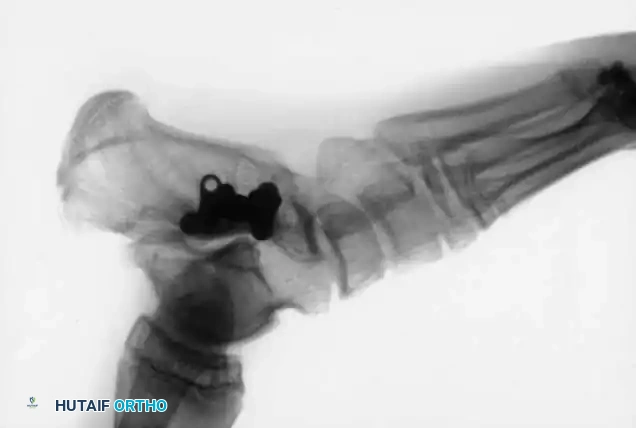
Thorough pre-operative planning is the cornerstone of successful talar fracture management. The complex, multi-planar geometry of the talus renders standard radiographic evaluation insufficient for definitive surgical templating. While standard anteroposterior (AP), lateral, and mortise views of the ankle are required as the initial baseline, the Canale view is absolutely essential for evaluating the talar neck for subtle varus comminution or displacement.
To obtain the Canale view, the foot is placed directly under the x-ray tube, and the ankle is placed in maximal equinus—the usual position after the reduction of a talar neck fracture. This position can be maintained more easily by maximal flexion of the hip and knee. The foot is pronated 15 degrees, and the x-ray tube is directed cephalad at a 75-degree angle from the horizontal tabletop. This specialized technique enables the surgeon to look directly down the axis of the talar neck, detecting any subtle offset, comminution, or varus deformity that would otherwise be obscured by the overlapping shadows of the distal tibia and calcaneus.
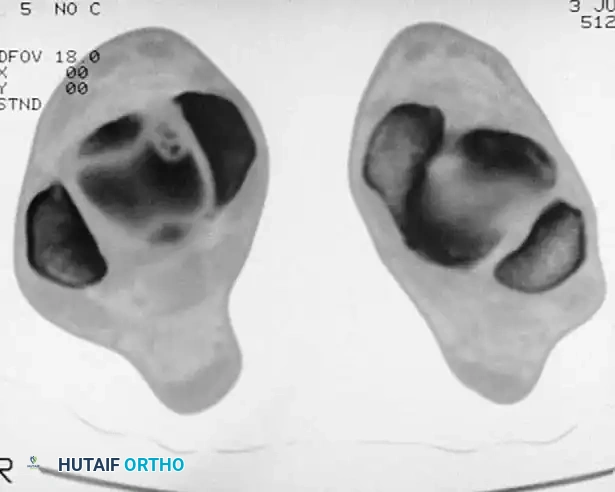
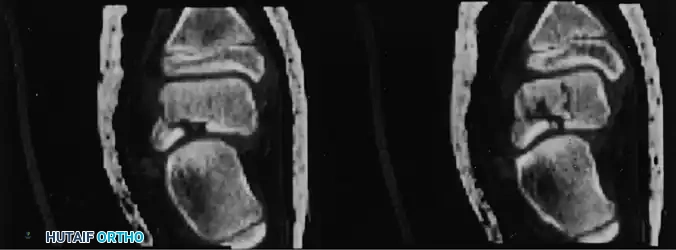
Despite the utility of the Canale view, Computed Tomography (CT) with fine 1mm cuts and multi-planar reconstructions (coronal, sagittal, and 3D) has become the gold standard and an absolute requirement for pre-operative planning. Standard radiographs often fail to accurately locate the lesion's anterior-to-posterior position or the true extent of articular comminution. CT scanning defines the exact location, size, and depth of the fracture lines, which is critical for planning the surgical approach and hardware trajectory.


Patient positioning in the operating room must be tailored to the planned surgical approach and the anticipated trajectory of fixation. For standard anteromedial and anterolateral approaches, the patient is placed supine with a bump under the ipsilateral hip to allow for neutral rotation of the leg. A radiolucent triangle may be utilized to position the knee in flexion, relaxing the gastrocnemius-soleus complex and facilitating reduction. If a posterior-to-anterior (PA) screw trajectory is planned—which offers biomechanically superior compression—the patient may need to be positioned in the lateral decubitus or prone position. The surgeon must ensure that fluoroscopy can freely access the AP, lateral, and Canale views without obstruction from the operating table.

Step-by-Step Surgical Approach and Fixation Technique
The surgical management of displaced talar neck and body fractures demands meticulous soft tissue handling to preserve the remaining tenuous blood supply. A dual-incision technique—utilizing both anteromedial and anterolateral approaches—is strongly advocated to allow direct visualization of both cortices, ensuring absolute anatomical reduction and preventing the dreaded varus malunion.
The anteromedial approach is executed by making an incision medial to the tibialis anterior tendon, beginning at the anterior aspect of the medial malleolus and extending distally toward the navicular tuberosity. The neurovascular bundle must be carefully identified and retracted laterally. The capsule of the talonavicular joint is incised, exposing the medial talar neck. The anterolateral approach is performed via an incision centered over the sinus tarsi, extending from the Chaput tubercle toward the base of the fourth metatarsal. The extensor digitorum brevis muscle belly is elevated, and the lateral aspect of the talar neck and the subtalar joint are exposed. Crucially, the surgeon must strictly avoid stripping the dorsal periosteum of the talar neck, as this harbors the critical superior neck vessels.
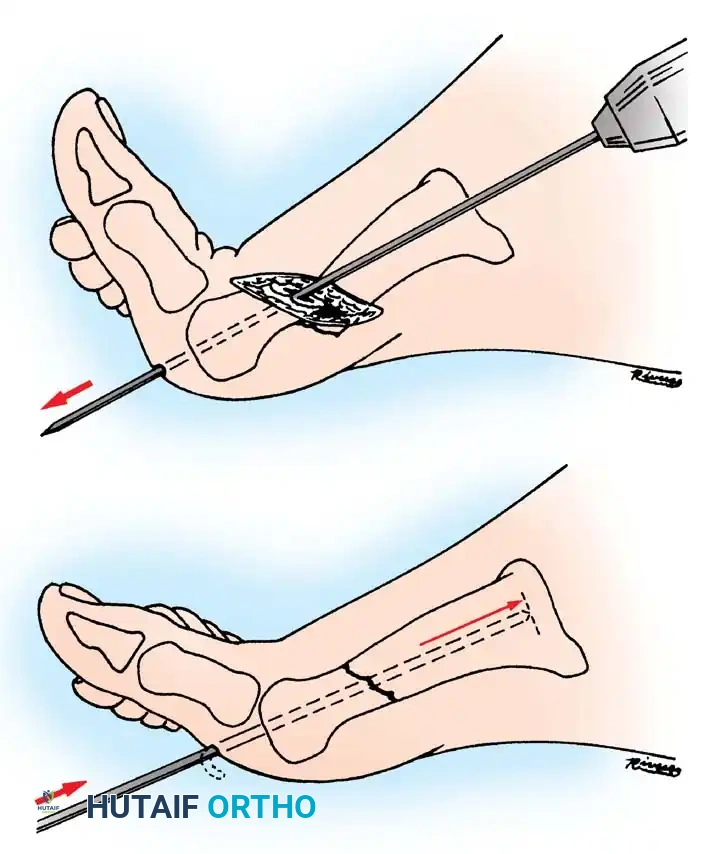
Once the fracture is debrided of hematoma and interposed soft tissue, anatomical reduction is achieved using specialized reduction forceps. Temporary fixation is secured with Kirschner wires. For definitive fixation, the biomechanically superior construct involves cancellous lag screws inserted percutaneously from posterior to anterior. This requires a posterolateral approach, taking extreme care to protect the sural nerve and the flexor hallucis longus (FHL) tendon. Posterior-to-anterior screws cross the fracture site perpendicular to the primary fracture plane, offering enhanced compression and utilizing the denser bone of the posterior talar body for screw purchase.

In cases of severe medial comminution, standard lag screw fixation may lead to iatrogenic shortening and varus deformity. In such instances, the utilization of mini-fragment plates (2.0mm or 2.4mm) applied as neutralization or buttress plates along the medial talar neck is imperative to maintain column length. Headless compression screws are frequently utilized for articular fragments to allow for countersinking beneath the cartilage surface.

For Osteochondral Lesions of the Talus (OLT), the surgical approach depends on the lesion's location as defined by the pre-operative CT. Anterolateral lesions can typically be accessed via anterior arthroscopy with the ankle in plantarflexion. Posteromedial lesions may require a medial malleolar osteotomy for perpendicular access. A critical clinical pearl involves identifying the "floating" fragment. If an osteochondral fragment appears on radiographs to be floating in its crater and riding high, with a flake of bone proximally that appears to be in the joint, the fragment is likely inverted in the crater. This means the subchondral bone is facing the joint space, and the cartilage is facing the bony crater. In this position, biological healing is impossible, and surgical excision with base microfracture is absolutely indicated.
Complications, Incidence Rates, and Salvage Management
The complication profile following talar fractures is extensive and potentially devastating, directly correlating with the initial energy of the trauma and the quality of the surgical reduction. The most feared complication is osteonecrosis (avascular necrosis) of the talar body. The risk correlates directly with the degree of displacement and dislocation as defined by the Hawkins Classification: Type I fractures carry a 0-10% risk, Type II a 20-50% risk, Type III a 70-100% risk, and Type IV fractures almost universally result in osteonecrosis.
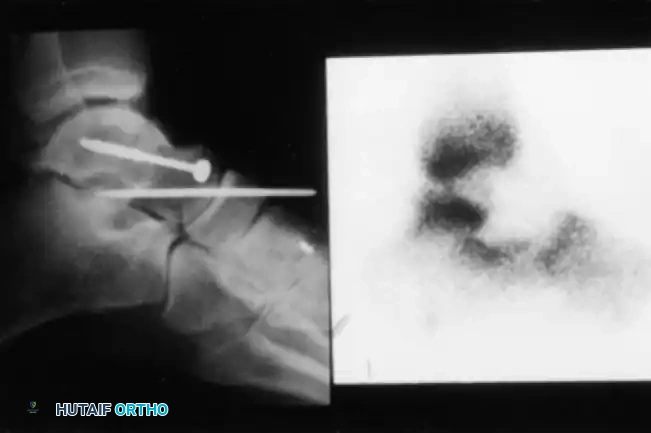
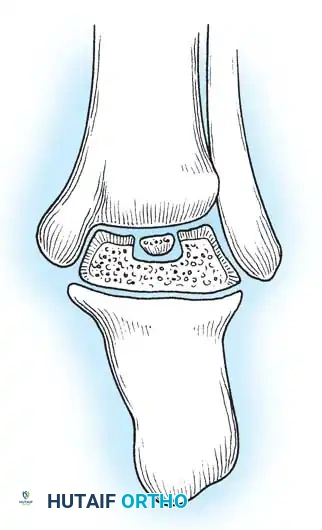
A critical prognostic indicator for talar viability is the Hawkins sign—a subchondral radiolucency present in the talar dome 8 to 12 weeks after injury. This lucency represents subchondral osteopenia secondary to active hyperemia, indicating that the talar body remains vascularized and is undergoing active bone resorption and remodeling. A positive Hawkins sign at 12 weeks is a highly reliable indicator that osteonecrosis will not occur. Conversely, the lack of a subchondral lucency at 3 months strongly indicates that osteonecrosis has occurred, leaving a dense, sclerotic talar dome on radiographs.

If standard radiographs are equivocal, bone scanning or Magnetic Resonance Imaging (MRI) may be utilized. Decreased radiotracer uptake on a technetium-99m bone scan or altered signal intensity (loss of normal fatty marrow signal on T1-weighted images) on MRI confirms the avascular state.
Malunions of talar fractures are frequent in adults treated nonoperatively or with inadequate surgical fixation. Malunion usually occurs with the distal fragment dorsiflexed or in a varus position, causing the fibula to rotate more anteriorly than normal. This forces the patient to bear an excessive amount of weight on the lateral side of the foot, rapidly leading to traumatic arthritis in the ankle and subtalar joints. Infection is another devastating complication, particularly following open fractures. Because the talus is composed almost entirely of cancellous bone, established osteomyelitis of the talus is highly resistant to systemic antibiotic treatment.
| Complication | Estimated Incidence Rate | Pathophysiological Mechanism | Salvage Management Options |
|---|---|---|---|
| Osteonecrosis (AVN) | 10% (Type I) to 100% (Type IV) | Disruption of retrograde extraosseous blood supply | Patellar tendon-bearing brace, Core decompression, Blair fusion, TTC arthrodesis |
| Varus Malunion | 20% - 30% (if single incision used) | Medial comminution collapse, inadequate visualization | Medial opening wedge osteotomy, Triple arthrodesis for end-stage arthritis |
| Post-Traumatic Arthritis | 50% - 90% (Subtalar > Ankle) | Initial cartilage impact damage, joint incongruity | Subtalar arthrodesis, Tibiotalar arthrodesis, Total Ankle Arthroplasty (if AVN absent) |
| Deep Infection / Osteomyelitis | 5% - 15% (Higher in Open Fx) | Poor soft tissue envelope, avascular bone acting as sequestrum | Aggressive debridement, Talectomy with primary tibiocalcaneal fusion |
Surgical warnings dictate that repeated sequestrectomy or attempted excision and drainage of a sinus tract are generally contraindicated in established osteomyelitis of the talus. The results of simple talectomy without fusion have been historically poor, leaving a painful, unstable limb. The preferred treatment for fractures of the talus complicated by intractable infection or severe symptomatic avascular collapse is excision of the affected bone followed by rigid arthrodesis. Salvage operations include tibiocalcaneal fusion utilizing an intramedullary nail, Blair fusion (sliding anterior tibial graft to the talar neck), or a formal triple arthrodesis depending on the extent of joint involvement.
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following operative management of talar fractures is a protracted process, requiring immense patient compliance and close radiographic monitoring. The primary objective during the initial post-operative phase is the protection of the fragile fixation construct and the preservation of the compromised soft tissue envelope.
Phase I: Maximum Protection (Weeks 0-6)
Immediately post-operatively, the patient is placed in a bulky, well-padded posterior splint with the ankle in neutral dorsiflexion. Strict non-weight-bearing (NWB) status is absolutely mandatory. Elevation of the limb above the level of the heart is critical to mitigate severe peritalar edema, which can compromise wound healing. At 2 weeks, sutures are removed, and the patient is transitioned to a rigid short-leg cast or a locked controlled ankle motion (CAM) boot. NWB status is maintained. If wound healing is optimal, gentle, active range of motion (ROM) of the toes, knee, and hip is encouraged to prevent proximal atrophy.
Phase II: Early Mobilization and Vascular Assessment (Weeks 6-12)
At the 6-to-8-week mark, critical radiographic evaluation is performed. Standard AP, lateral, and Canale views are obtained to assess for the presence of the Hawkins sign. If subchondral lucency is observed, indicating intact vascularity, the patient may begin progressive, active, and active-assisted ROM of the ankle and subtalar joints out of the CAM boot. Weight-bearing remains strictly prohibited. Aggressive physical therapy focuses on restoring dorsiflexion and plantarflexion, though inversion and eversion (subtalar motion) must be introduced cautiously to avoid stressing the talar neck fracture site.
Phase III: Progressive Weight-Bearing and Strengthening (Weeks 12-24)
By 12 weeks, clinical and radiographic signs of fracture consolidation should be evident. If union is progressing and there is no evidence of avascular collapse, the patient is transitioned to partial weight-bearing (PWB) in a CAM boot, advancing by 25% of body weight weekly. In cases where osteonecrosis is suspected or confirmed (absence of Hawkins sign, sclerosis on plain films), a prolonged period of NWB or the use of a custom patellar tendon-bearing (PTB) brace is instituted. The PTB brace unloads the talus, transferring axial forces from the patellar tendon directly to the shoe, allowing the talus to undergo creeping substitution without mechanical collapse. Strengthening exercises for the peroneals, tibialis posterior, and gastroc-soleus complex are aggressively pursued during this phase.
Summary of Landmark Literature and Clinical Guidelines
The modern operative management of talar fractures is built upon a foundation of landmark orthopedic literature that has defined our understanding of talar vascularity, fracture classification, and biomechanical fixation.
L.G. Hawkins' seminal 1970 paper, "Fractures of the Neck of the Talus," remains the bedrock of talar trauma management. Hawkins not only provided the prognostic classification system that bears his name but also first described the subchondral radiolucency (Hawkins sign) as a reliable indicator of talar viability. His observation that the degree of initial displacement directly correlates with the disruption of the retrograde blood supply fundamentally shifted the paradigm toward early, anatomical reduction.
Canale and Kelly, in their 1978 publication "Fractures of the Neck of the Talus: Long-Term Evaluation of Seventy-One Cases," further refined the management protocols. They introduced the Type IV classification (talonavicular dislocation) and, crucially, described the "Canale view" radiograph. Their work highlighted the devastating consequences of varus malunion, demonstrating that even a few degrees of malalignment result in profound subtalar stiffness and early degenerative joint disease.
In the realm of osteochondral lesions, Berndt and Harty's 1959 study, "Transchondral Fractures (Osteochondritis Dissecans) of the Talus," established the morphological staging system still utilized today. They definitively proved the traumatic etiology of lateral lesions through cadaveric impact studies, distinguishing them from the more complex etiology of medial lesions.
Modern clinical guidelines, supported by recent biomechanical studies (e.g., Swanson et al., Journal of Orthopaedic Trauma), strongly advocate for the use of dual incisions (anteromedial and anterolateral) to ensure absolute visualization of the talar neck, thereby minimizing the risk of varus
