Comprehensive Surgical Management of Bunionette (Tailor’s Bunion)

Key Takeaway
A bunionette, or Tailor’s bunion, is a painful bony prominence on the lateral aspect of the fifth metatarsal head. Often associated with splay foot or hallux valgus, it results from chronic pressure and mechanical overload. Conservative management includes shoe modifications and orthotics. When refractory, surgical intervention is indicated. Options range from partial lateral condylectomy for localized prominences to distal chevron or diaphyseal osteotomies for severe metatarsus quintus valgus, ensuring biomechanical restoration and symptom relief.
Comprehensive Introduction and Patho-Epidemiology
The bony prominence on the lateral aspect of the fifth metatarsal head is classically referred to within orthopedic literature as a "tailor’s bunion" or bunionette. This specific nomenclature originates from the historical cross-legged sitting position favored by tailors, a posture that forced the lateral border of the foot against the unyielding floor. This chronic, repetitive mechanical overload led to localized tissue ischemia, microtrauma, and the subsequent formation of an adventitial bursa over the lateral condyle. While the occupational hazard has largely vanished in modern society, the condition remains highly prevalent, predominantly driven by extrinsic footwear constraints and intrinsic biomechanical abnormalities of the forefoot.
In contemporary orthopedic practice, a bunionette is frequently observed not merely as an isolated osseous anomaly, but rather as a constituent of a broader, more complex forefoot pathology. Most notably, it is associated with the splay foot deformity, often presenting concomitantly with hallux valgus and central metatarsalgia. The etiology of the bunionette is definitively multifactorial, encompassing genetic predispositions, ligamentous laxity, and altered foot kinematics. The primary structural abnormalities include a congenitally or traumatically enlarged fifth metatarsal head (Type I deformity), an abnormal lateral angulation of the distal diaphysis (Type II deformity), or a pathological widening of the fourth-fifth intermetatarsal angle (Type III deformity), all of which render the fifth metatarsal head excessively prominent and susceptible to external pressure.

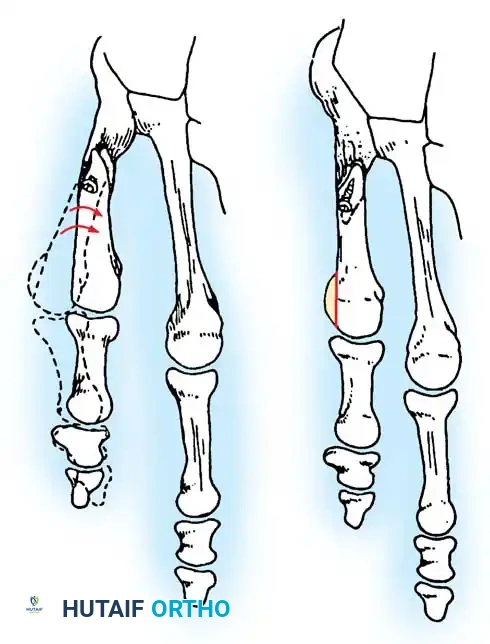
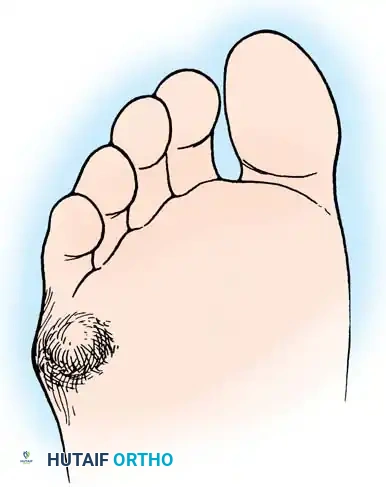
Fig. 80-30 A and B, Bunionette with metatarsus quintus valgus and fifth toe varus.
Constricting, narrow-toe-box footwear remains the primary extrinsic source of discomfort and exacerbation in modern patient populations. Continuous, unrelenting pressure over this lateral bony prominence incites a cascade of chronic inflammatory responses. This friction leads to the development, and subsequent hypertrophy, of an adventitial bursa, which can become acutely inflamed, erythematous, and exquisitely tender to palpation. If this pathological mechanical environment is left untreated, ischemic ulceration of the overlying skin may ensue. Furthermore, an intractable plantar keratosis (IPK) or a dense lateral hyperkeratotic callus frequently develops over the prominent bunionette due to unyielding shoe pressure and altered shear forces during the terminal stance phase of gait.

Fig. 80-31 Bunionette–hallux valgus–splay foot complex. Note lateral angulation of shaft of fifth metatarsal at distal third (arrows).
🚨 Clinical Warning: The Neuropathic Foot
In patients with diabetes mellitus, advanced Charcot-Marie-Tooth disease, or specific types of spinal dysraphism associated with poor sensibility, a neglected bunionette complication can be catastrophic. Ulceration and subsequent deep space infection can rapidly result in osteomyelitis, leading to the loss of the entire fifth ray or even necessitating a major lower extremity amputation.
In addition to a symptomatic bursa over the lateral aspect of the prominent fifth metatarsal head, a diffuse callus or localized intractable keratosis can develop beneath the plantar aspect of the fifth metatarsal head. This is particularly prevalent if a rigid extension deformity is present at the fifth metatarsophalangeal (MTP) joint, which drives the metatarsal head plantarward during weight-bearing, severely disrupting the normal distribution of plantar pressures across the forefoot parabola.

Fig. 80-32 Bunionette deformity with bursa formation.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the surgical anatomy and biomechanics of the lateral column of the foot is an absolute prerequisite for executing successful interventions for bunionette deformities. The fifth metatarsal is anatomically distinct from the lesser metatarsals, possessing a unique structural morphology characterized by a prominent tuberosity proximally, a dorsolaterally bowed diaphysis, and an asymmetrical metatarsal head. The lateral condyle of the fifth metatarsal head is naturally more prominent than its medial counterpart, predisposing it to external pressure. The articular surface extends further plantarward and laterally, accommodating the multi-planar motion of the fifth MTP joint, which inherently possesses a greater degree of mobility in the sagittal and transverse planes compared to the central rays.
The ligamentous and capsular structures surrounding the fifth MTP joint are critical for dynamic stability. The joint capsule is reinforced by collateral ligaments that originate from the dorsal tubercles of the metatarsal head and insert onto the plantar-medial and plantar-lateral aspects of the proximal phalanx. The plantar plate, a dense fibrocartilaginous structure, resists hyperextension forces and serves as an insertion site for the plantar aponeurosis. The abductor digiti minimi (ADM) tendon, inserting onto the lateral aspect of the proximal phalanx base, exerts a strong lateral and plantar deforming force. When the fifth metatarsal head deviates laterally, the ADM gains a mechanical advantage, exacerbating the varus deformity of the fifth toe and further exposing the lateral condyle to shoe wear friction.

General Surgical Diagram illustrating the lateral prominence and planned resection.
Neurovascular anatomy demands meticulous attention during surgical exposure. The dorsolateral cutaneous branch of the sural nerve invariably crosses the operative field, typically coursing over the dorsal aspect of the fifth metatarsal diaphysis before arborizing to supply sensation to the lateral aspect of the fifth toe. Iatrogenic injury to this nerve can result in a debilitating neuroma, often causing more morbidity than the original bunionette. Plantarward, the proper digital branch of the lateral plantar nerve must be protected, particularly during plantar condylectomy or deep capsular releases. The vascular supply to the fifth metatarsal head is derived from an extraosseous arterial ring formed by branches of the lateral plantar and dorsal metatarsal arteries, necessitating careful subperiosteal dissection to preserve capsular attachments and prevent avascular necrosis of the metatarsal head following osteotomy.
Biomechanically, the lateral column of the foot (comprising the calcaneus, cuboid, and fourth and fifth metatarsals) functions as a mobile adapter during the early stance phase of gait and transitions into a rigid lever for propulsion during terminal stance. The fifth ray bears approximately 10% to 15% of the body's weight during normal ambulation. In the presence of a bunionette deformity, particularly those associated with an increased fourth-fifth intermetatarsal angle (Type III), the lateral column becomes hypermobile. This hypermobility leads to an inefficient transfer of forces, causing the fifth metatarsal head to roll laterally and plantarward, thereby concentrating shear forces on the overlying skin and subcutaneous tissues, culminating in the classic clinical presentation of an intractable plantar keratosis and adventitial bursitis.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for a bunionette deformity must be predicated on a thorough clinical evaluation, radiographic assessment, and, most importantly, the documented failure of exhaustive conservative management. Non-operative modalities—including the utilization of wide toe-box footwear, custom-molded semirigid orthotics with specific lateral and plantar reliefs, metatarsal pads, and targeted corticosteroid injections for acute bursitis—must be trialed for a minimum of three to six months. Surgery is indicated only when these conservative measures fail to alleviate debilitating pain, when the deformity progressively worsens, or when impending skin breakdown threatens the viability of the lateral foot, particularly in at-risk populations.
The specific surgical procedure chosen is dictated by the Fallat and Buckholz classification system, which categorizes the pathoanatomy based on radiographic parameters. Type I deformities (isolated lateral condylar hypertrophy) are typically managed with a lateral condylectomy. Type II deformities (lateral bowing of the diaphysis) necessitate a distal or midshaft osteotomy to realign the articular surface. Type III deformities (widened fourth-fifth intermetatarsal angle, typically >8 degrees) require a more proximal osteotomy or a robust diaphyseal translation to adequately narrow the forefoot. Failure to match the surgical procedure to the specific pathoanatomic type is the leading cause of recurrent deformity and persistent postoperative pain.
| Category | Specific Clinical Scenarios |
|---|---|
| Absolute Indications | - Chronic, debilitating pain at the 5th MTP joint refractory to >6 months of conservative care. - Recurrent ulceration over the lateral eminence in a sensate foot. - Severe splay foot deformity causing secondary central metatarsalgia. - Intractable plantar keratosis (IPK) directly beneath the 5th metatarsal head unresponsive to offloading. |
| Relative Indications | - Progressive cosmetic deformity causing severe psychological distress (with concomitant pain). - Difficulty accommodating standard footwear despite professional shoe stretching. - Concomitant hallux valgus surgery where lateral column balancing is required to achieve a functional forefoot. |
| Absolute Contraindications | - Severe peripheral arterial disease (PAD) with inadequate perfusion (ABI < 0.5 or absent palpable pulses without Doppler flow). - Active soft tissue infection or acute osteomyelitis at the operative site. - Uncontrolled diabetes mellitus with severe peripheral neuropathy (Charcot neuroarthropathy) and lack of protective sensation. - Medically unstable patients unfit for regional or general anesthesia. |
| Relative Contraindications | - Heavy tobacco use (significantly increases the risk of delayed union or nonunion in osteotomies). - Patient non-compliance or inability to adhere to strict postoperative weight-bearing restrictions. - Purely cosmetic concerns in an entirely asymptomatic foot. - Severe, generalized hypermobility syndromes where recurrence is highly probable without arthrodesis. |
Contraindications must be rigidly respected to avoid catastrophic postoperative complications. Vascular compromise is the most critical absolute contraindication; any surgical incision on the lateral border of an ischemic foot is highly likely to result in wound dehiscence, chronic ulceration, and potential amputation. Neuropathy presents a complex challenge; while an impending ulcer in a neuropathic patient may necessitate prophylactic exostectomy, complex osteotomies requiring prolonged periods of protected weight-bearing are fraught with risks of Charcot exacerbation, hardware failure, and nonunion. In such scenarios, if surgery is unavoidable, it must be combined with prolonged rigid immobilization (e.g., total contact casting) and aggressive multidisciplinary management.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful bunionette correction. The clinical examination must assess the entire lower extremity kinetic chain, focusing on the flexibility of the deformity, the presence of Achilles tendon or gastrocnemius contractures (which can exacerbate forefoot overload), and the specific location of hyperkeratotic lesions. A lateral callus suggests a pure transverse plane deformity, whereas a plantar-lateral or purely plantar IPK indicates a significant sagittal plane component (plantarflexed fifth metatarsal) that must be addressed, often requiring an elevating osteotomy rather than a simple lateral condylectomy.
Radiographic evaluation is mandatory and must include standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. On the AP view, the surgeon must calculate the fourth-fifth intermetatarsal angle (IMA), which is normally between 6 and 8 degrees. An IMA exceeding 8 to 10 degrees defines a Type III deformity. The lateral bowing angle of the fifth metatarsal is also measured; normal is less than 3 degrees, and an increase signifies a Type II deformity. The fifth MTP joint must be scrutinized for signs of degenerative joint disease, subluxation, or frank dislocation, which would preclude joint-sparing osteotomies and necessitate salvage procedures such as resection arthroplasty.

Pre-operative templating demonstrating measurement of the 4-5 Intermetatarsal Angle.
Radiographic evaluation of lateral bowing and condylar hypertrophy.
Digital templating is strongly recommended to determine the optimal level and geometry of the osteotomy. For distal chevron osteotomies, the apex of the cut should be planned within the metaphyseal bone to ensure adequate healing potential, while allowing for sufficient medial translation (typically 3 to 5 mm) to correct the IMA without causing lateral cortical overhang. For diaphyseal or proximal osteotomies, the surgeon must template the degree of angular correction required and select appropriate internal fixation devices, such as low-profile titanium plates or intramedullary compression screws, ensuring they will not cause secondary soft tissue irritation beneath the thin lateral integument.
Patient positioning is standardized for lateral column forefoot surgery. The patient is placed in the supine position on the operating table. A significant bump (sandbag or gel pad) is placed beneath the ipsilateral hip to internally rotate the lower extremity, bringing the lateral aspect of the foot into a directly superior, easily accessible orientation for the surgeon. A well-padded pneumatic tourniquet is applied to the proximal thigh or calf, depending on surgeon preference and patient vascular status. Regional anesthesia, specifically a popliteal sciatic nerve block combined with a saphenous nerve block, is highly preferred, providing excellent intraoperative muscle relaxation and profound postoperative analgesia, thereby reducing the need for systemic opioids.
Step-by-Step Surgical Approach and Fixation Technique
If conservative treatment fails and surgical intervention becomes necessary, the procedure must be meticulously tailored to the specific pathoanatomy. The primary surgical choices range from partial resection of the lateral condyle to complex diaphyseal osteotomies. Complete resection of the fifth metatarsal head is considered a salvage procedure and is rarely indicated as a primary intervention due to the high risk of transfer metatarsalgia and profound weakness during the push-off phase of gait.
Partial Resection of the Lateral Condyle (Lateral Condylectomy)
Partial resection of the lateral condyle of the fifth metatarsal head is historically the most commonly utilized procedure for Type I deformities. It effectively relieves pressure symptoms and allows the patient a slightly greater variety of shoe wear. However, the cosmetic correction regarding the overall width of the foot is minimal, and patients must be counseled accordingly.
💡 Surgical Pearl: Managing Patient Expectations
The patient must be explicitly warned before surgery that only the painful bony prominence will be removed. The overall width of the forefoot will not be altered appreciably. If forefoot narrowing is the primary goal to address a splay foot, an osteotomy is absolutely required.
Causes of failure in lateral condylar resection include inadequate resection of the prominence, secondary MTP joint subluxation due to over-resection of the collateral ligament attachments, and progressive forefoot splaying over time. Furthermore, if there is a painful callosity beneath the metatarsal head, the plantar aspect of the condyle must also be resected to prevent persistent plantar pain.
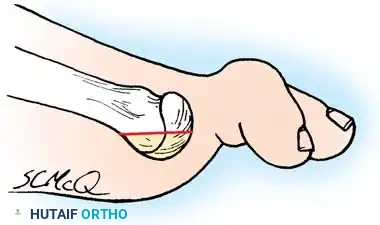
Fig. 80-35 Plantar aspect of fifth metatarsal head should be removed in addition to lateral flare if a plantar callus coexists.
🔪 Surgical Technique 80-13: Bunionette Excision
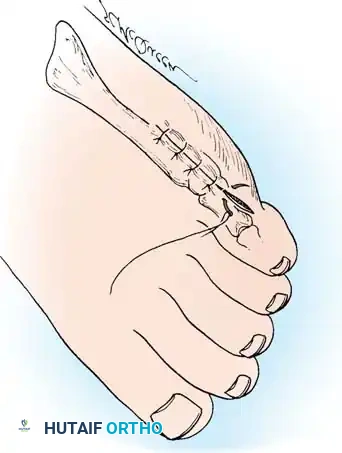
- Incision: Execute a straight lateral (preferred) or dorsolateral longitudinal incision extending from the junction of the middle and distal thirds of the fifth metatarsal shaft to the midshaft of the proximal phalanx. Incise only the epidermis and dermis initially to avoid inadvertent nerve injury.
- Nerve Protection: Meticulously identify and protect the dorsolateral cutaneous branch of the sural nerve. The straight lateral incision should pass safely between this nerve dorsally and the proper digital branch of the lateral plantar nerve to the fifth toe plantarward. Retract these structures with blunt, atraumatic retractors.

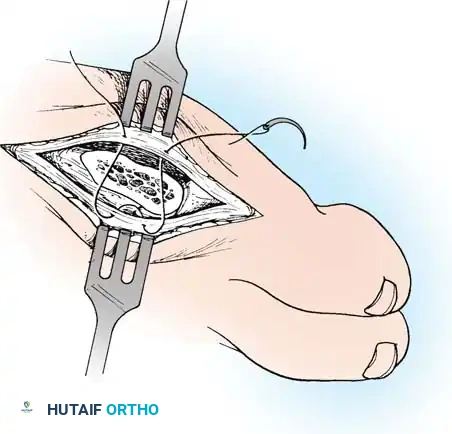
Fig. 80-36A Skin incision.
- Capsular Exposure: The tendon of insertion of the abductor digiti minimi passes just plantar to the midline of the lateral aspect of the fifth metatarsal head. Make the periosteal and capsular incision in a straight line 2 or 3 mm dorsal to the midline to preserve this tendon and the plantar capsular structures.
- Joint Delivery: By sharp dissection, elevate the capsule dorsally and plantarward until the fifth metatarsal head can be completely visualized by delivering it laterally as the proximal phalanx is pushed medially. Ensure the entire lateral flare and the distal articular surface are exposed.
⚠️ Surgical Pitfall: Over-resection
More metatarsal head can be removed than is intended if the medial edge of the articular cartilage is not adequately exposed and utilized as a landmark. Approximately 35% to 40% of the metatarsal head is usually removed to excise the bony prominence. A thin osteotome or a small sagittal saw blade is mandatory to prevent iatrogenic fracture of the metaphysis or excessive bone loss leading to joint instability.
- Osteotomy Cut: Score the proximal margin of the proposed osteotomy at the anatomic neck. Direct the saw cut in a dorsal-distal to plantar-proximal direction, ensuring the cut is parallel to the weight-bearing surface of the foot to avoid creating a sharp plantar spike.


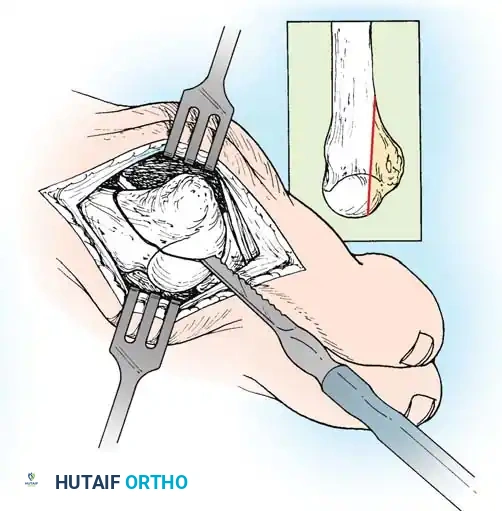
Fig. 80-36B Excision of lateral prominence of fifth metatarsal head to include 40% of articular surface.
- Phalangeal Contouring: Reduce the phalanx over the remaining part of the fifth metatarsal head, and palpate the lateral flare of the base of the phalanx. If this produces a projecting bony prominence that may cause impingement against the shoe, excise the prominence with a rongeur or bone-biter.
- Plantar Condylectomy: Before closing the capsule, round off all sharp bone edges with a power rasp or hand file. If a plantar callus coexists beneath the metatarsal head, angle the saw blade to resect the plantar-lateral condyle, effectively elevating the functional weight-bearing surface of the metatarsal head.
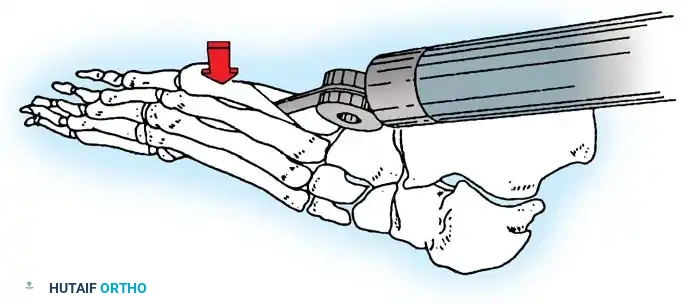
Distal Chevron Osteotomy for Type II and III Deformities
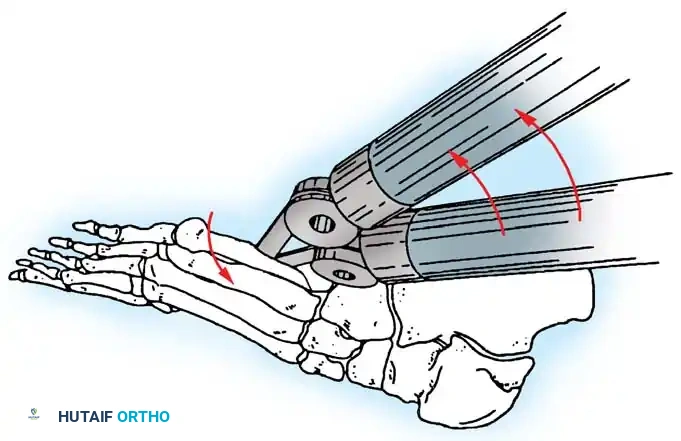
For patients with a widened IMA or lateral bowing, a distal chevron osteotomy is the workhorse procedure. The approach is identical to the condylectomy. Once the head is exposed, a V-shaped osteotomy with the apex pointing distally is created in the metaphysis. The angle of the chevron should be approximately 60 degrees. The capital fragment is then translated medially by up to 50% of the shaft width.
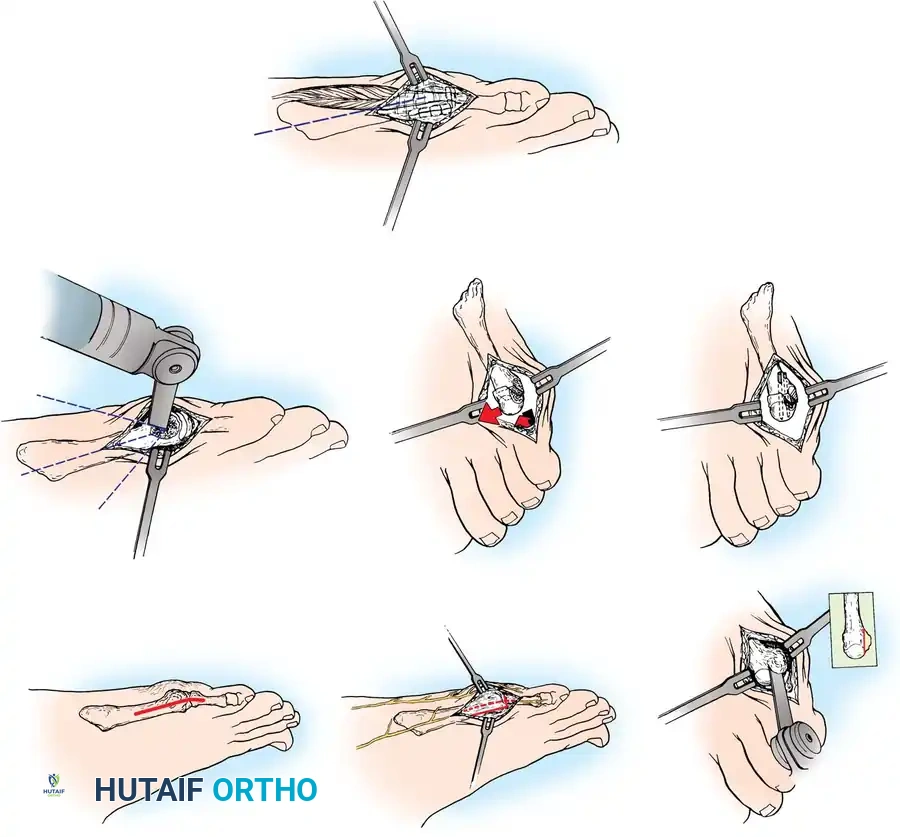
Distal Chevron Osteotomy translation and temporary K-wire fixation.
Once the desired medial translation is achieved, the osteotomy is provisionally fixed with a smooth 0.045-inch Kirschner wire. Definitive fixation is typically achieved with a single 2.0 mm or 2.4 mm cannulated headless compression screw or a low-profile threaded K-wire. The overhanging lateral cortical bone of the proximal shaft is then resected flush with the translated metatarsal head. The capsule is closed under tension (capsulorrhaphy) to pull the fifth toe out of varus and stabilize the MTP joint.

Final fixation of the distal osteotomy.
Post-operative radiographic appearance of internal fixation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following bunionette surgery can occur and range from minor superficial wound issues to catastrophic hardware failure and nonunion. The surgeon must be adept at recognizing these complications early and implementing appropriate salvage strategies.
| Complication | Estimated Incidence | Etiology & Pathophysiology | Management & Salvage Strategies |
|---|---|---|---|
| Sural Nerve Injury / Neuroma | 5% - 10% | Iatrogenic transection or aggressive retraction of the dorsolateral cutaneous nerve during exposure. | Initial management includes gabapentinoids and localized corticosteroid injections. Refractory neuromas require surgical excision and proximal burying of the nerve stump into intrinsic musculature. |
| Recurrence of Deformity | 8% - 15% | Failure to address a widened IMA (performing a simple condylectomy for a Type III deformity), or failure of capsulorrhaphy. | Revision surgery with a more proximal osteotomy (diaphyseal or basal) to ensure adequate medial translation. Aggressive soft tissue re-balancing. |
| Transfer Metatarsalgia | 5% - 12% | Excessive dorsal elevation of the 5th metatarsal head during osteotomy fixation, transferring load to the 4th metatarsal. | Conservative: Custom orthotics with a 4th ray offload. Surgical: Plantarflexing Weil osteotomy of the 4th metatarsal or revision plantarflexing osteotomy of the 5th. |
| Delayed Union / Nonunion | 2% - 5% | Thermal necrosis from saw blades, excessive periosteal stripping disrupting blood supply, or patient non-compliance (smoking, early weight-bearing). | Prolonged immobilization and bone stimulators for delayed union. Frank nonunion requires revision open reduction, autologous bone grafting, and rigid plate osteosynthesis. |
| Over-resection / MTP Instability | 3% - 6% | Resecting >50% of the metatarsal head, destroying the collateral ligament origins, leading to medial subluxation of the toe. | Soft tissue reconstruction is often inadequate. Salvage may require syndactylization to the 4th toe or, in severe cases, 5th MTP joint arthroplasty/resection. |
| Deep Infection | < 2% | Contamination during surgery, poor wound healing in patients with compromised vascularity or poorly controlled diabetes. | Aggressive surgical debridement, hardware removal if stability is compromised, and targeted intravenous antibiotic therapy. Severe osteomyelitis may necessitate 5th ray amputation. |
Salvage Management: Fifth Metatarsal Head Resection
Complete resection of the fifth metatarsal head is strictly reserved as a
Clinical & Radiographic Imaging Archive