Operative Management of Ingrown Toenails: A Comprehensive Surgical Guide

Key Takeaway
Onychocryptosis, commonly known as an ingrown toenail, is a painful condition driven by extrinsic pressure and improper nail trimming. Management depends on clinical staging, ranging from conservative cotton-mesh elevation in Stage I to partial or total nail plate avulsion with matrixectomy in Stages II and III. This guide details the relevant nail anatomy, biomechanics, and step-by-step surgical techniques required to achieve definitive resolution and minimize recurrence.
Comprehensive Introduction and Patho-Epidemiology
Ingrown toenail, medically designated as onychocryptosis or unguis incarnatus, represents one of the most ubiquitous and frequently mismanaged nail disorders encountered by orthopedic surgeons, foot and ankle specialists, and general practitioners alike. Despite its prevalence, it is often erroneously relegated to the category of a minor podiatric ailment. However, improper or inadequate management frequently leads to chronic, debilitating pain, recurrent soft-tissue infections, and significant functional morbidity. In vulnerable patient populations—particularly those with poorly controlled diabetes mellitus, peripheral neuropathy, or profound peripheral arterial disease—a seemingly innocuous ingrown toenail can rapidly precipitate deep space infections, osteomyelitis of the distal phalanx, and ultimately necessitate partial or complete digital amputation. Therefore, a rigorous, evidence-based approach to this pathology is an absolute requirement for the practicing orthopedic surgeon.
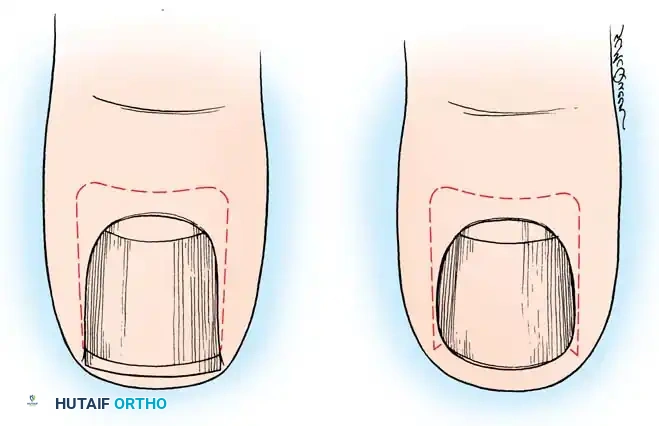
The precise pathophysiology of onychocryptosis is multifaceted, representing a complex interplay between intrinsic anatomical predispositions and extrinsic biomechanical forces. The term "ingrown toenail" is itself a mechanistic misnomer; it incorrectly implies that the nail plate actively alters its growth trajectory to invade the adjacent soft tissues. In reality, the pathology is predominantly a soft-tissue disorder characterized by the hypertrophy and medialization of the lateral nail fold, which is subsequently driven into the sharp, unyielding lateral margin of the nail plate. This condition is exceedingly rare in barefoot populations, highlighting the profound pathogenic role of extrinsic pressure exerted by constrictive, modern footwear. Within the restrictive confines of a narrow or improperly sized shoe toe box, the hallux is forcibly deviated laterally toward the second toe. This generates sustained pressure against the lateral border of the nail, while the medial aspect of the shoe toe box exerts a simultaneous counter-pressure on the medial nail fold.

When this extrinsic biomechanical pressure forces the hypertrophic nail fold into the sharp edge of an improperly trimmed nail plate, the epidermal barrier is breached. This micro-laceration serves as a portal of entry for the normal, yet opportunistic, bacterial and fungal flora of the foot, predominantly Staphylococcus aureus, Streptococcus species, and various dermatophytes. The introduction of these pathogens into the highly vascularized perionychial tissues initiates a robust and aggressive inflammatory cascade. As eloquently described by Lapidus, this pathological sequence creates a "bottlenecked, poorly draining abscess." The localized environment becomes characterized by intense erythema, profound edema, hyperhidrosis, and exquisite point tenderness along the affected nail border.
As the inflammatory process transitions from an acute to a chronic phase, the body's frustrated attempt at wound healing results in the exuberant formation of hypertrophic granulation tissue. This highly vascular, friable tissue proliferates rapidly, spilling over the lateral nail plate and further occluding any potential avenues for spontaneous purulent drainage. The presence of this granulation tissue establishes a vicious, self-perpetuating cycle: the increased soft-tissue bulk exacerbates the extrinsic pressure from footwear, which in turn drives the nail plate deeper into the nail fold, thereby worsening the laceration and fueling further inflammation and tissue hypertrophy. Breaking this cycle requires definitive surgical intervention aimed at either removing the offending portion of the nail plate and its generative matrix, or excising the hypertrophic soft tissues that have encroached upon the nail.
Detailed Surgical Anatomy and Biomechanics
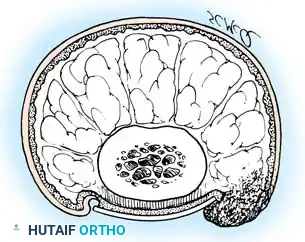
To execute effective surgical ablation, minimize the risk of iatrogenic deformity, and definitively prevent recurrence, the orthopedic surgeon must possess an intimate, three-dimensional understanding of the perionychial anatomy. The normal nail complex is not a singular structure but rather a highly specialized, integrated unit composed of several distinct anatomical and functional components. The nail root represents the proximal portion of the nail plate that lies deeply embedded beneath the proximal skin fold. The nail body is the exposed, visible portion of the nail plate, composed of dense, compacted, and longitudinally oriented keratinocytes. The nail walls, or labia ungues, are the cutaneous margins that overhang and border the two lateral edges of the nail body, forming the lateral nail grooves. The eponychium, commonly referred to as the proximal nail fold, is the distal extension of the stratum corneum of the skin that covers the nail root, while the cuticle is the distal, acellular edge of the eponychium that forms a critical, waterproof seal between the skin and the nail plate.
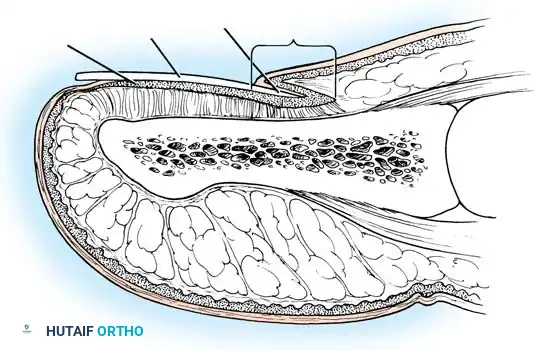
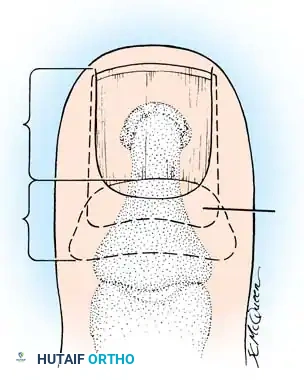
The generative center of the nail complex is the matrix, which consists of several highly active layers of cells derived from the stratum germinativum. Functionally and anatomically, the matrix is divided into two distinct components: the sterile matrix and the germinal matrix. The sterile matrix lies distal to the lunula and is tightly adherent to the overlying nail plate, contributing minimally to its longitudinal growth but significantly to its adherence and thickness. In stark contrast, the germinal matrix is the primary engine of longitudinal nail plate production. In the skeletally mature foot, the germinal matrix extends from just distal to the lunula to approximately 5 to 8 millimeters proximally, lying deep to the eponychium and resting directly upon the periosteum of the distal phalanx. Macroscopically, it appears smoother and distinctly paler than the highly vascular sterile matrix.
A critical anatomical nuance that dictates surgical success is the morphology of the proximal-lateral extents of the germinal matrix, known as the lateral horns. The germinal matrix does not end abruptly at the visible lateral margins of the nail root; rather, it sends microscopic, sweeping projections proximally and laterally deep into the adjacent soft tissues of the proximal nail fold. Failure to meticulously identify, expose, and completely excise or chemically ablate these lateral horns is the single most common cause of recurrent nail spicule formation following partial or total matrixectomy. The surgeon must aggressively pursue these lateral extensions during any definitive ablative procedure, often requiring a dedicated proximal incision through the eponychium for adequate visualization.

The vascular supply and innervation of the nail complex are robust, reflecting its high metabolic demand and sensory function. Arterial inflow is provided by the terminal branches of the proper plantar digital arteries, which form a rich, anastomotic subungual glomus network that is highly sensitive to temperature and pressure changes. Venous drainage is primarily dorsal. Innervation is supplied predominantly by the proper plantar digital nerves, with supplementary contributions to the proximal perionychium from the dorsal sensory branches of the superficial peroneal nerve. This dual innervation necessitates a comprehensive ring block at the base of the digit to achieve profound surgical anesthesia, as a simple dorsal or volar block will inevitably leave the patient with residual nociception during deep matrix dissection.
Exhaustive Indications and Contraindications
The management algorithm for onychocryptosis is rigorously dictated by the clinical stage of the disease, the patient's underlying physiological status, and the chronicity of the presentation. Clinical staging, often based on the Heifetz or Mozena classification systems, divides the pathology into three distinct phases. Stage I (the Inflammatory Stage) is characterized by mild erythema, localized swelling, and tenderness along the lateral nail fold, with the epidermal barrier largely intact and no purulent drainage present. Stage II (the Abscess Stage) represents a progression wherein the lateral nail fold bulges over the nail plate, accompanied by intense hyperhidrosis, severe pain, and active drainage that rapidly transitions from serous to purulent and fetid due to polymicrobial colonization. Stage III (the Granulation Stage) is the most advanced chronic phase, defined by the presence of exuberant, hypertrophic granulation tissue that completely covers the lateral nail fold, inhibiting free drainage and often epithelizing over the nail plate.
Operative intervention is strictly indicated based on these clinical stages. Nonoperative management—consisting of cotton-pledget elevation, warm water soaks, and footwear modification—is highly effective in Stage I and can occasionally salvage early Stage II lesions if acute inflammation is aggressively managed with broad-spectrum oral antibiotics. However, once hypertrophic granulation tissue develops (Stage III), or if a Stage II lesion proves refractory to conservative measures, nonoperative management yields rapidly diminishing returns and is associated with unacceptably high recurrence rates. Surgical management, therefore, becomes the definitive standard of care. The specific operative procedure—ranging from simple partial avulsion to definitive matrixectomy or radical soft-tissue resection—is tailored to the severity of the deformity, the presence of concurrent infection, and the patient's history of prior interventions.


While surgical intervention is frequently required, the surgeon must be acutely aware of absolute and relative contraindications, particularly in the lower extremity where vascular compromise can lead to catastrophic outcomes. Absolute contraindications to elective operative management include severe, un-optimized peripheral arterial disease (PAD) with an ankle-brachial index (ABI) less than 0.5, absent palpable pedal pulses without non-invasive vascular clearance, and active, uncontrolled systemic sepsis originating from the digit. In patients with profound ischemia, even minor surgical trauma to the nail fold can precipitate non-healing ulcerations, dry gangrene, and the eventual need for major limb amputation. In such scenarios, vascular surgery consultation and revascularization must precede any elective podiatric or orthopedic intervention.
Relative contraindications require nuanced clinical judgment and meticulous perioperative optimization. These include poorly controlled diabetes mellitus (HbA1c > 9.0%), active localized cellulitis extending proximally beyond the metatarsophalangeal joint, and severe immunosuppression. In the presence of advancing cellulitis, it is prudent to initiate culture-directed intravenous or high-dose oral antibiotics and delay definitive matrixectomy until the surrounding soft-tissue erythema has receded, thereby minimizing the risk of disseminating the infection or experiencing wound dehiscence. Furthermore, the use of chemical matrixectomy agents (such as 89% phenol or sodium hydroxide) is relatively contraindicated in patients with significant microvascular disease, as these caustic agents induce a severe chemical burn that relies on robust local tissue perfusion for adequate healing.
| Indication / Contraindication Category | Specific Clinical Scenarios | Management Implications |
|---|---|---|
| Absolute Surgical Indications | Stage III (Granulation), Refractory Stage II, Recurrent Onychocryptosis | Proceed with operative management (Partial Matrixectomy/Winograd). |
| Relative Surgical Indications | Early Stage II failing 2 weeks of conservative care, Severe pain limiting ambulation | Trial of antibiotics/soaks, followed by surgery if no rapid improvement. |
| Absolute Contraindications | Severe PAD (ABI < 0.5), Acute systemic sepsis, Uncorrectable coagulopathy | Defer elective surgery; obtain vascular consult; manage medically. |
| Relative Contraindications | Proximal spreading cellulitis, HbA1c > 9.0%, Active immunosuppressive therapy | Optimize medically; delay matrixectomy until local infection is controlled. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with a meticulous clinical evaluation of the affected digit and the patient's overall lower extremity vascular and neurological status. The surgeon must palpate the dorsalis pedis and posterior tibial pulses; if any deficit is noted, Doppler ultrasound or formal non-invasive arterial studies are mandatory. Neurological assessment using a 10-gram Semmes-Weinstein monofilament is essential to document pre-existing peripheral neuropathy, which will dictate post-operative wound care protocols and weight-bearing restrictions. While routine plain radiography is not strictly required for a straightforward ingrown toenail, multi-planar radiographs of the hallux should be obtained if there is clinical suspicion of underlying osteomyelitis (indicated by a chronically draining sinus tract or a "sausage digit" appearance) or a subungual exostosis, which can mimic the pain and nail plate elevation seen in recurrent onychocryptosis.
Achieving profound, reliable anesthesia is the cornerstone of a successful and humane surgical procedure. A digital block is the anesthetic technique of choice. The surgeon should utilize a 1% to 2% solution of lidocaine or mepivacaine, often mixed with 0.5% bupivacaine for prolonged post-operative analgesia. Classically, orthopedic teaching dictates that these agents must be used without epinephrine to avoid vasospasm and potential digital ischemia. While recent literature has challenged this dogma, demonstrating the safety of epinephrine in healthy digits, it remains prudent to avoid vasoconstrictors in patients with known microvascular disease. The injection is performed using a small-gauge needle (25G or 27G) introduced approximately 1 cm distal to the first web space. The surgeon must systematically block the proper plantar digital nerves and the dorsal sensory branches of the superficial peroneal nerve, ensuring circumferential anesthesia before proceeding with any tissue manipulation.

A completely bloodless surgical field is absolutely critical for the precise identification and complete extirpation of the germinal matrix, particularly the elusive lateral horns. Even minor capillary bleeding will obscure the pale, glistening tissue of the matrix, leading to incomplete resection and guaranteed recurrence. Hemostasis is achieved through the application of a digital tourniquet at the base of the proximal phalanx. This can be accomplished using a sterile 1/4-inch Penrose drain tightly wrapped and secured with a hemostat, or a commercially available elastic digital tourniquet ring. The surgeon must meticulously exsanguinate the digit by elevating it and applying distal-to-proximal pressure before engaging the tourniquet. The time of tourniquet application must be strictly recorded, and it should rarely exceed 20 to 30 minutes for these procedures to prevent ischemic neuropraxia.



Patient positioning is straightforward but requires attention to ergonomics to facilitate precise surgical technique. The patient is placed in the supine position on the operating table or a specialized podiatric procedure chair. The affected lower extremity is externally rotated slightly to provide direct, orthogonal visual access to the medial or lateral aspect of the hallux, depending on the site of pathology. A sterile field is established utilizing standard chlorhexidine or povidone-iodine preparation, extending from the mid-foot to the distal tuft. The surgeon should be seated comfortably at the foot of the table, utilizing adequate overhead surgical lighting or a sterile headlamp. The instrument tray should be pre-templated with a Freer or nasal elevator, heavy straight nail scissors (English anvil action), a #15 scalpel blade, a small curette, and fine toothed forceps, ensuring all necessary tools are immediately accessible once the tourniquet is inflated.
Step-by-Step Surgical Approach and Fixation Technique
The operative treatment of ingrown toenails is broadly categorized based on two divergent philosophical approaches regarding the primary etiology of the disease: either the nail plate itself is deemed the primary offender (necessitating nail and/or matrix removal), or the hypertrophic soft tissues are considered the primary pathology (requiring aggressive soft-tissue resection while sparing the nail). The selection of the specific surgical technique must be tailored to the chronicity of the lesion, the extent of soft-tissue hypertrophy, and the patient's anatomical variations.
Total and Partial Nail Plate Avulsion
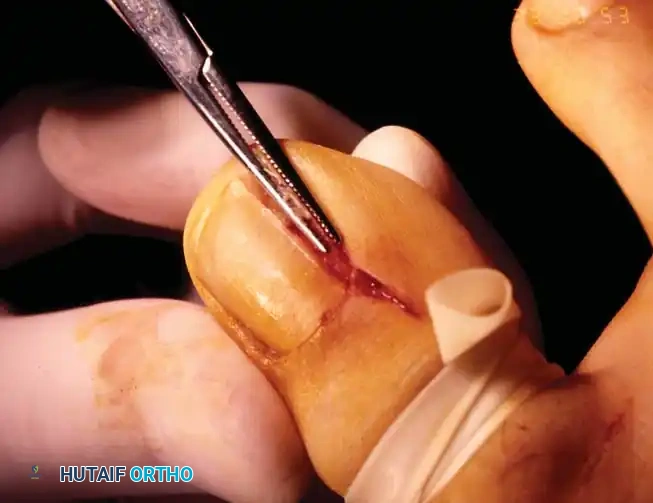
Total nail plate removal without concomitant matrixectomy is rarely indicated as a definitive, standalone procedure due to unacceptably high recurrence rates, historically reported between 32% and 78%. It is primarily reserved as a temporizing or decompressive measure for severe, circumducting subungual abscesses that involve both lateral folds and the proximal eponychium, where a partial removal would fail to provide adequate purulent drainage. Following adequate anesthesia and exsanguination, the surgeon passes a straight, thin hemostat or a small, flat nasal elevator beneath the nail plate in the midline. Starting at the hyponychium, the instrument is advanced proximally to several millimeters beneath the eponychial fold, adjacent to the lunula. The surgeon must avoid sweeping the instrument back and forth, which can lacerate the underlying sterile matrix. Instead, the elevator is withdrawn and re-inserted in a similar longitudinal manner beneath each lateral margin. Once sufficiently loosened, a firm, steady distal pull is applied with a heavy hemostat to extract the plate.
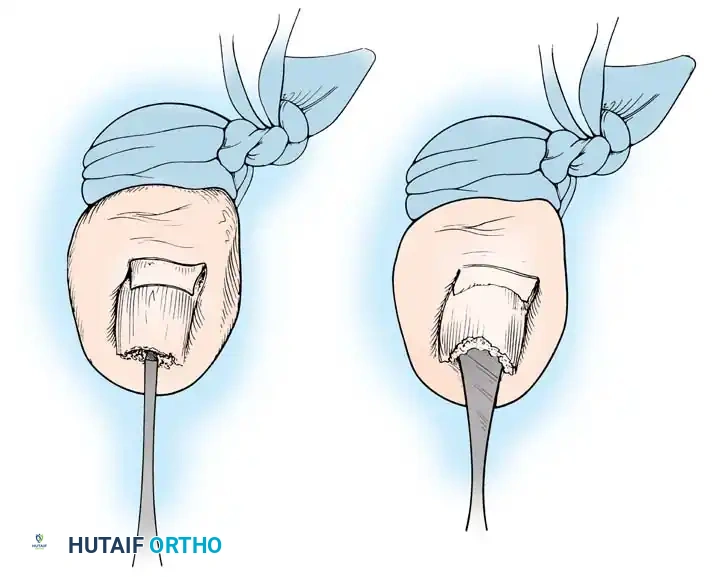

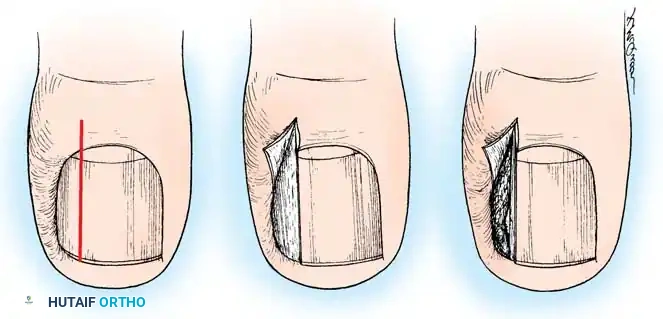
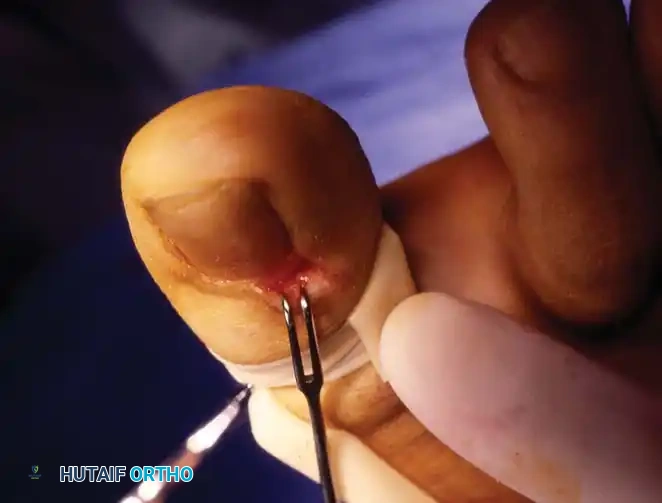
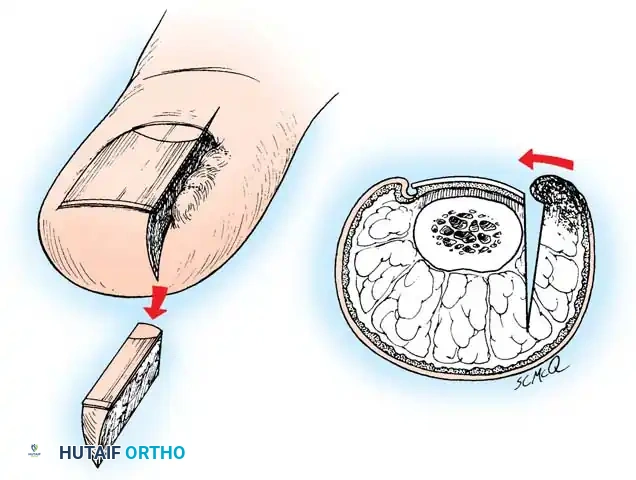
Partial nail plate removal is a significantly less morbid alternative, particularly attractive in pediatric and adolescent populations where permanent alteration of the nail's aesthetic appearance is undesirable. However, similar to total avulsion, the recurrence rate remains high if the underlying generative matrix is not simultaneously addressed. The technique involves lifting only the affected lateral fourth of the nail from its bed using a small, angled probe. Using heavy, straight scissors, the surgeon cuts the nail plate longitudinally while maintaining upward traction on the lateral segment. It is imperative that this longitudinal incision extends to the absolute proximal end of the nail plate, deep beneath the eponychium. The offending lateral nail spike is then grasped and extracted with a rolling motion toward the midline to ensure no distal spicules break off and remain embedded in the lateral recess.


Following either total or partial avulsion without matrixectomy, the exposed, highly sensitive nail bed must be meticulously protected. A nonadherent, single-layer dressing, such as Adaptic or Xeroform, is applied directly to the exposed sterile matrix, followed by a gently wrapped, bulky compression bandage. The patient must be explicitly forewarned that the nail requires 4 to 6 months to regenerate completely. Furthermore, the surgeon must counsel the patient that multiple, repeated nail avulsions significantly increase the risk of developing a permanent upward-turned deformity of the distal nail bed and digital pulp, a complication resulting from the loss of the rigid, stabilizing counter-pressure normally provided by the intact nail plate.


The Winograd Procedure (Partial Matrixectomy)
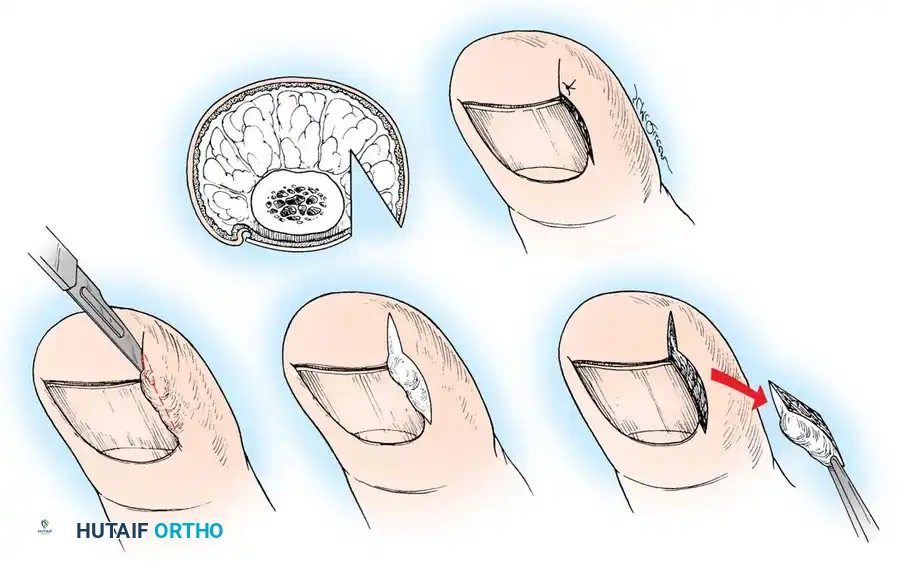
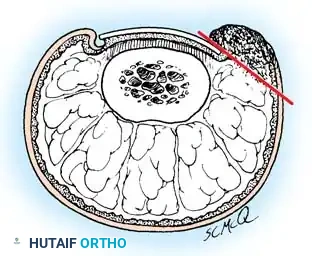
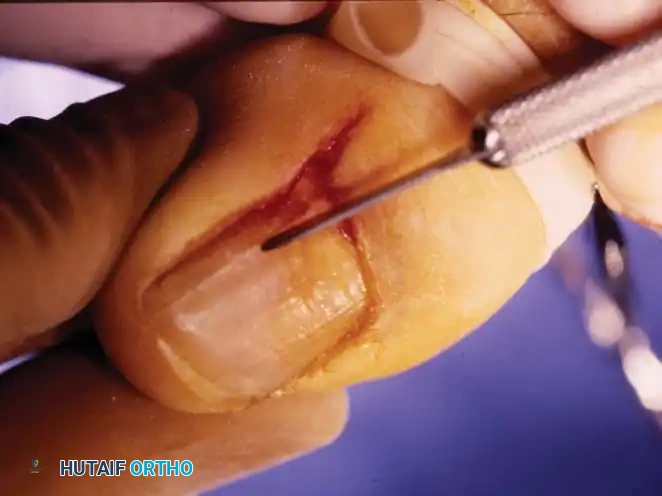
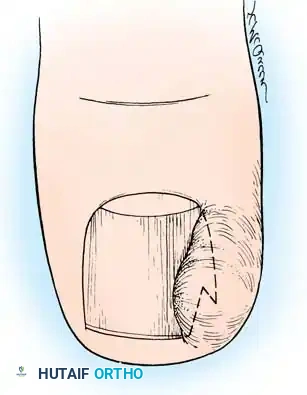
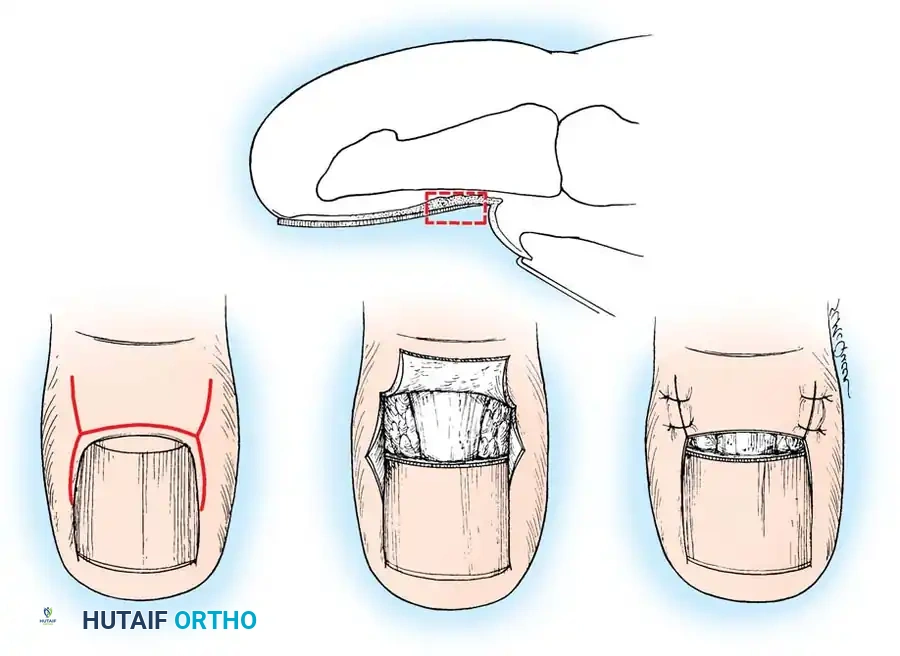
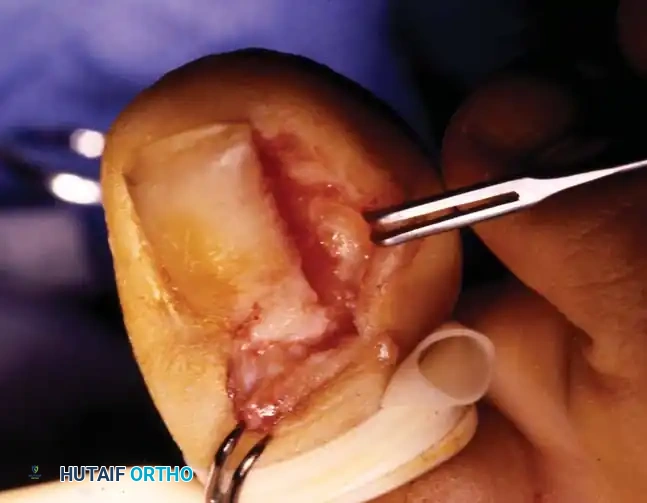
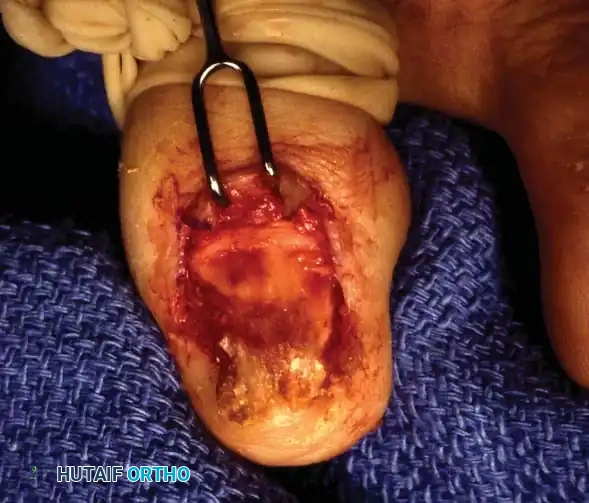
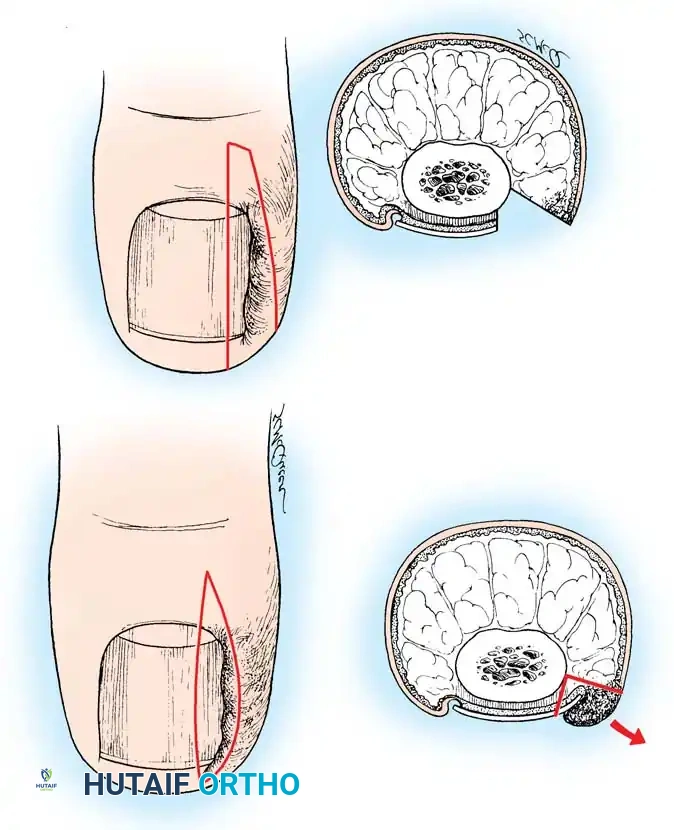
Described by Winograd in 1929, the partial nail plate avulsion combined with surgical matrixectomy remains the gold standard for the definitive management of Stage II and Stage III ingrown toenails. By mechanically excising the lateral horn of the germinal matrix, the longitudinal growth of the offending nail border is permanently arrested, resulting in a slightly narrower but functionally normal nail plate. Under tourniquet control, the procedure begins with a longitudinal incision through the nail plate, approximately 3 to 4 mm from the affected lateral border. This incision is extended proximally through the eponychium using a #15 scalpel blade to fully expose the nail root and the underlying matrix.


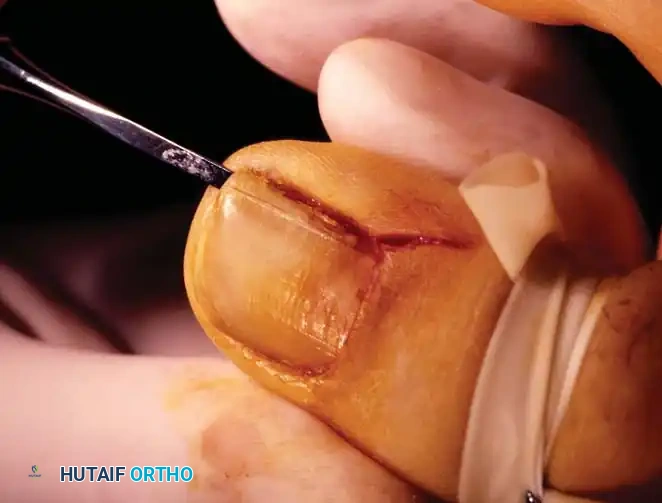
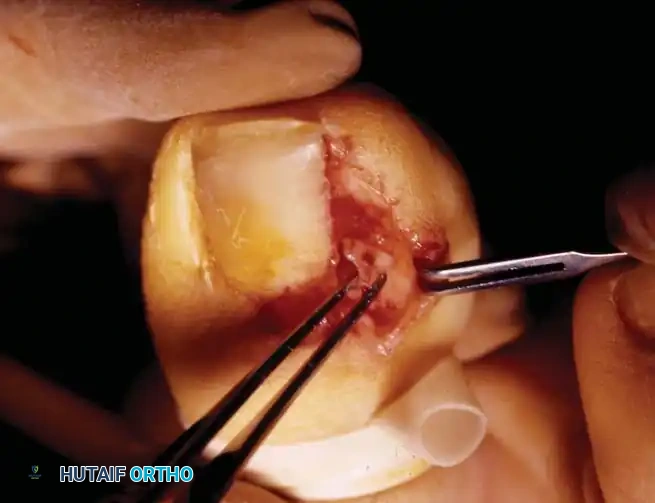
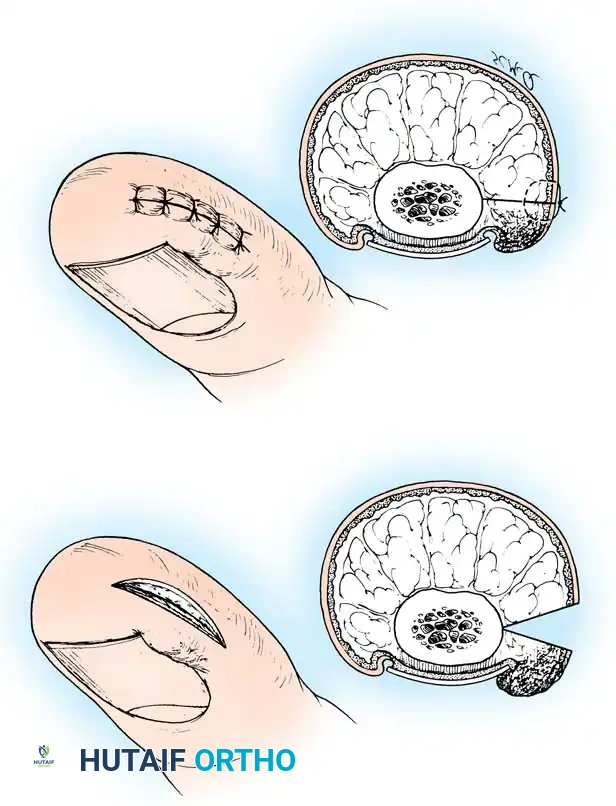
Once the proximal nail fold is incised and retracted, a second, elliptical incision is made to excise the hypertrophic lateral nail fold and the adjacent granulation tissue en bloc. The surgeon then meticulously dissects down to the periosteum of the distal phalanx. The critical step is the complete identification and excision of the germinal matrix, including its deep lateral horn. The matrix appears as a pale, glistening tissue layer distinct from the overlying dermis and underlying periosteum. Using a small curette or the tip of a #15 blade, the surgeon aggressively scrapes the base of the lateral recess and the proximal-lateral corner to ensure no matrix cells remain.
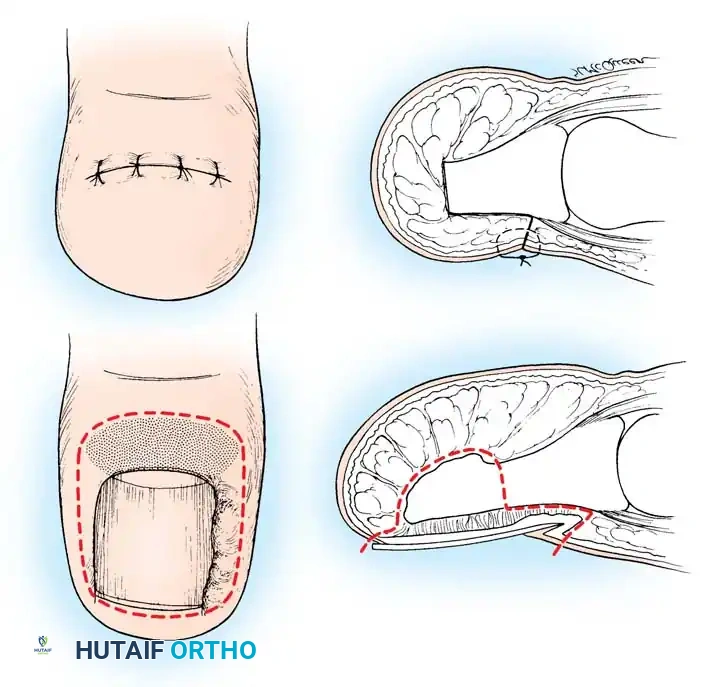
After thorough curettage, the tourniquet is released, and meticulous hemostasis is achieved using localized pressure or minimal electrocautery. The wound is copiously irrigated with sterile saline. The eponychial incision and the lateral soft-tissue defect are then approximated. While some surgeons prefer to leave the defect open to heal by secondary intention, primary closure using 4-0 or 5-0 non-absorbable nylon sutures (often in a mattress configuration to evert the skin edges) provides a superior cosmetic result and faster time to epithelialization. The sutures are placed through the remaining nail plate and the lateral skin flap, securely anchoring the soft tissues away from the newly created nail margin.


Chemical Matrixectomy and Soft-Tissue Resection
Chemical matrixectomy, utilizing 89% aqueous phenol or 10% sodium hydroxide, is a highly effective alternative to sharp surgical excision and is favored for its lower post-operative pain profile and reduced risk of iatrogenic nail bed laceration. Following partial nail avulsion, the surgical field must be completely bloodless, as blood rapidly neutralizes phenol. A sterile cotton-tipped applicator is dipped in the chemical agent and aggressively massaged into the proximal lateral recess, targeting the lateral horn of the germinal matrix. The application is typically performed in three successive 30-to-45-second intervals. Following the final application, the area is copiously irrigated and neutralized with isopropyl alcohol (for phenol) or dilute acetic acid (for sodium hydroxide) to prevent collateral chemical burns to the adjacent healthy tissues.
Conversely, the soft-tissue resection paradigm, championed by Vandenbos and Bowers in 1959, posits that the nail plate is inherently normal and the pathology lies entirely within the hypertrophic soft tissues. The Vandenbos procedure involves a radical, elliptical excision of the lateral nail fold and the hyperplastic tissue, deliberately sparing the nail plate and the matrix entirely. An incision is made 3 to 5 mm proximal to the base of the nail, curving laterally and distally to encompass the entire hypertrophic fold, extending deep to the periosteum.