What to Expect: Ankle Surgery Postoperative Care & Instructions
Key Takeaway
This topic focuses on What to Expect: Ankle Surgery Postoperative Care & Instructions, Postoperative care and instructions following ankle arthrodesis emphasize patient education regarding altered gait. Patients should expect walking will not return to normal, experiencing reduced speed and increased energy expenditure. Achieving optimal fusion position—0° dorsiflexion, 0°-5° valgus, 5°-10° external rotation—is crucial for recovery, guiding rehabilitation strategies and managing long-term functional expectations.
Comprehensive Introduction and Patho-Epidemiology
The management of complex ankle pathology represents one of the most dynamic and rapidly evolving domains within contemporary orthopedic surgery. Unlike the hip and knee, where primary osteoarthritis predominates, the vast majority of end-stage ankle arthritis is post-traumatic in etiology, often afflicting a significantly younger and more active patient demographic. This unique epidemiological profile necessitates surgical interventions that not only alleviate debilitating pain but also withstand the rigorous biomechanical demands of decades of weight-bearing activity. The transition from conservative management to surgical intervention marks a critical juncture in patient care, requiring an exhaustive understanding of both the operative techniques and the stringent postoperative protocols necessary to ensure optimal outcomes.
Historically, ankle arthrodesis has been heralded as the gold standard for end-stage tibiotalar arthropathy. However, the last two decades have witnessed a paradigm shift with the advent of refined total ankle arthroplasty (TAA) systems, advanced ankle arthroscopy techniques, and sophisticated soft-tissue reconstructions for Achilles and peroneal tendinopathies. As surgical indications expand, the orthopedic surgeon must navigate a complex algorithmic approach to patient selection. The decision matrix must account for the patient's physiological age, bone stock, coronal and sagittal plane deformities, neurovascular status, and their capacity to adhere to rigorous postoperative rehabilitation regimens.
Postoperative care and instructions are not merely an afterthought; they are intrinsically linked to the surgical intervention's success. The physiological healing of bone and soft tissue in the distal lower extremity is notoriously unforgiving due to the tenuous vascular envelope, limited soft-tissue coverage, and the immense sheer forces transmitted through the foot and ankle during the gait cycle. A meticulously executed ankle arthrodesis or tendon reconstruction can easily be compromised by premature weight-bearing, inadequate immobilization, or failure to recognize early signs of wound breakdown. Therefore, the surgeon must approach postoperative care with the same level of precision and vigilance applied in the operating theater.
This definitive chapter provides an exhaustive exploration of the surgical management of the ankle, synthesizing detailed operative techniques with comprehensive postoperative care paradigms. By examining the intricacies of ankle arthrodesis, arthroplasty, arthroscopy, and major tendinous reconstructions, this text aims to equip the orthopedic surgeon, resident, and medical student with the evidence-based knowledge required to optimize patient outcomes. The integration of patho-epidemiology, biomechanics, and phased rehabilitation protocols will serve as a foundational reference for navigating the multifaceted challenges of ankle surgery.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of ankle anatomy and its complex biomechanics is the cornerstone of successful surgical intervention and postoperative rehabilitation. The ankle joint, or talocrural joint, is a highly congruent, modified hinge joint formed by the articulation of the distal tibia, the medial and lateral malleoli, and the talar dome. The inherent stability of the ankle is derived from its unique osseous architecture—often described as a mortise and tenon configuration—and a robust network of ligamentous restraints. The talar dome is wider anteriorly than posteriorly, meaning that the joint is most stable in maximal dorsiflexion when the widest portion of the talus is wedged into the mortise. Conversely, the joint relies heavily on ligamentous stability in plantarflexion.
The normal physiological range of motion (ROM) of the ankle joint is critical for a fluid, energy-efficient gait. Normal dorsiflexion ranges from 0° to 20°, while normal plantarflexion ranges from 0° to 45°. During the stance phase of walking, a minimum of 10° of dorsiflexion is required to allow the tibia to translate smoothly over the plantigrade foot. Deficits in this range of motion, whether due to osteophyte formation, soft tissue contracture, or an improperly positioned arthrodesis, will inevitably lead to compensatory kinematics at the midfoot, subtalar joint, and knee, predisposing these adjacent segments to accelerated degenerative changes.
Ligamentous support is divided into the lateral collateral complex and the medial deltoid complex. The lateral complex comprises the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is the primary restraint to anterior translation of the talus and is the most frequently injured ligament in the human body. The medial deltoid ligament is a stout, multifascicular structure that provides primary resistance to valgus tilting and lateral talar excursion. Surgically, understanding the footprint of these ligaments is vital during approaches for ankle arthroscopy or when balancing a total ankle arthroplasty.
The tendinous anatomy surrounding the ankle is equally paramount, particularly when addressing tendinopathies. The Achilles tendon, the largest and strongest tendon in the body, lacks a true synovial sheath, relying instead on a highly vascularized paratenon. Its watershed area, located 2 to 6 centimeters proximal to its calcaneal insertion, is notoriously prone to degeneration and rupture. Laterally, the peroneal tendons (longus and brevis) traverse posterior to the lateral malleolus, secured by the superior peroneal retinaculum (SPR). Pathology here, such as longitudinal splits or subluxation, requires meticulous surgical repair and specific postoperative immobilization to prevent recurrence.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the ankle requires a meticulous evaluation of the patient's pathology, symptomatology, and functional demands. For end-stage ankle arthritis, the indications for ankle arthrodesis remain robust, particularly for patients who are not candidates for arthroplasty. The primary indication is severe arthropathy that has failed exhaustive conservative management, including bracing, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid or biologic injections. Arthrodesis is also the salvage procedure of choice for a failed total ankle arthroplasty, where bone loss and soft tissue compromise preclude revision arthroplasty.
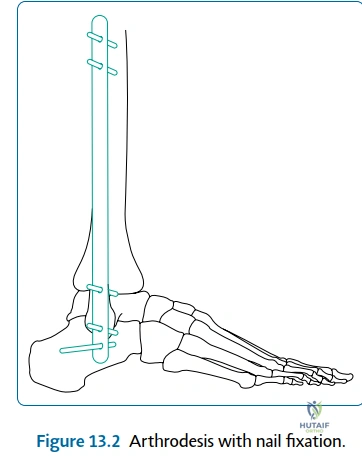
Further indications for ankle arthrodesis include complex tumor reconstruction, where massive resection of the distal tibia or talus necessitates rigid stabilization. Sequelae of chronic infection, particularly tuberculous arthritis, often result in profound joint destruction that is best managed with a solid fusion once the infection is eradicated. Avascular necrosis (AVN) of the talus, especially following high-energy talar neck fractures (Hawkins type III or IV), frequently leads to talar dome collapse and requires tibiotalocalcaneal (TTC) arthrodesis. Additionally, neuropathic joints (Charcot arthropathy) and neurological conditions resulting in a flail or severely deformed joint (e.g., polio, severe cerebral palsy) are classic indications for rigid internal fixation and fusion to provide a stable, plantigrade foot.
Conversely, total ankle arthroplasty (TAA) is indicated for older, lower-demand patients with end-stage osteoarthritis, post-traumatic arthritis, or inflammatory arthritis, provided they have adequate bone stock, minimal coronal plane deformity (typically less than 10-15 degrees), and competent ligamentous stability. Surgery for Achilles and peroneal tendinopathies is indicated when conservative measures fail, presenting as chronic pain, weakness, or tendon subluxation that limits activities of daily living. Ankle arthroscopy is indicated for the management of osteochondral lesions of the talus (OCLT), anterior impingement syndrome, and the removal of loose bodies.
Contraindications to these procedures must be strictly respected to avoid catastrophic postoperative complications. Active infection is an absolute contraindication to both arthroplasty and internal fixation for arthrodesis. Severe peripheral vascular disease, profound neuropathy (relative for arthrodesis, absolute for arthroplasty), and inadequate soft tissue envelopes are critical barriers to successful surgery. Furthermore, patient non-compliance, active smoking, and uncontrolled diabetes mellitus significantly elevate the risk of nonunion and wound necrosis, necessitating extensive preoperative optimization.
| Pathology / Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Ankle Arthrodesis | Arthropathy failing conservative care, failed arthroplasty, tumor reconstruction, sequelae of infection (TB), AVN of talus, Charcot joint, severe neurological flail joint. | Active local infection, severe uncorrectable vascular ischemia. | Active smoking, uncontrolled diabetes (HbA1c > 8.0%), severe osteoporosis. |
| Ankle Arthroplasty | End-stage OA/RA in low-demand patients, preserved bone stock, functional ROM. | Active infection, Charcot arthropathy, AVN of talus (>50%), severe peripheral neuropathy. | High physical demands/heavy labor, severe coronal deformity (>15°), young age (<50). |
| Ankle Arthroscopy | Osteochondral lesions of the talus, anterior impingement, loose bodies, synovitis. | Local soft tissue infection, severe joint space narrowing (precluding instrument access). | Severe edema, tenuous vascular status. |
| Tendon Reconstruction | Chronic Achilles/peroneal tendinopathy failing non-operative care, acute ruptures in active patients, recurrent subluxation. | Active infection, critical limb ischemia. | Poor soft tissue envelope, sedentary lifestyle (for acute rupture repair). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful ankle surgery, dictating the intraoperative workflow and anticipating potential pitfalls. The clinical evaluation must include a comprehensive neurovascular assessment, documenting pedal pulses, capillary refill, and protective sensation. The soft tissue envelope must be scrutinized for previous surgical incisions, venous stasis changes, and overall skin quality. Weight-bearing anteroposterior, lateral, and mortise radiographs of the ankle are mandatory. For complex deformities or when assessing bone stock for arthrodesis or arthroplasty, a computed tomography (CT) scan is invaluable for three-dimensional spatial understanding and identifying subchondral cysts. Magnetic resonance imaging (MRI) is the modality of choice for evaluating tendinous pathology and osteochondral lesions.
Templating is particularly critical for ankle arthrodesis and arthroplasty. For arthrodesis, the surgeon must plan the trajectory of the fixation constructs, whether utilizing large fragment crossing screws, an anterior locking plate, or a retrograde intramedullary nail for TTC fusions. The goal of templating is to ensure rigid compression across the prepared joint surfaces while avoiding neurovascular structures. For arthroplasty, templating determines the appropriate implant size, the level of the tibial cut, and the axis of rotation, ensuring the restoration of the mechanical axis and avoiding overstuffing the joint.

Patient positioning is dictated by the chosen surgical approach. For an anterior approach to the ankle (commonly used for arthroplasty and anterior plating arthrodesis), the patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position, bringing the foot pointing straight up. This allows excellent visualization of the anterior neurovascular bundle (deep peroneal nerve and anterior tibial artery). For a transfibular approach to arthrodesis, the patient is placed in the lateral decubitus position, allowing direct access to the lateral malleolus, which is often resected and used as a biologic bone graft.
For Achilles tendon surgery, the patient is positioned prone. Careful padding of all bony prominences, particularly the contralateral knee and bilateral upper extremities, is essential to prevent perioperative neuropraxias. A thigh tourniquet is generally preferred over a calf tourniquet for ankle procedures to allow unhindered access to the distal leg and to avoid tethering the gastrocnemius-soleus complex, which can artificially alter resting ankle tension during tendon repairs or balancing procedures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an ankle arthrodesis demands meticulous attention to joint preparation and the spatial orientation of the fusion. The optimal position of arthrodesis is universally accepted as: 1. Neutral flexion (0° of dorsiflexion/plantarflexion), 2. 0°-5° of valgus, and 3. 5°-10° of external rotation (matching the contralateral limb's tibial torsion). Fusing the ankle in plantarflexion results in a devastating recurvatum thrust at the knee during the stance phase, while excessive varus locks the transverse tarsal joints, creating a rigid, painful midfoot.
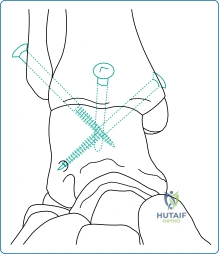
Once the joint is exposed—whether via an anterior, lateral transfibular, or arthroscopic approach—the remaining articular cartilage must be aggressively debrided down to bleeding subchondral bone. The subchondral plate is then fenestrated or "feathered" using a high-speed burr or osteotome to expose the highly vascular cancellous bone, which contains the mesenchymal stem cells necessary for osteogenesis. Fixation is typically achieved using two or three large-fragment (6.5mm or 7.3mm) cannulated screws. The "home run" screw is directed from the posterior aspect of the distal tibia into the neck of the talus, maximizing thread purchase in the dense talar bone. Additional crossing screws are placed to provide rotational stability and rigid interfragmentary compression.
For Achilles tendinopathy, the surgical approach involves a longitudinal incision placed slightly medial to the midline of the tendon to avoid the sural nerve laterally. The paratenon is carefully incised and preserved for later closure. The diseased, mucinoid degenerative tissue is excised. If a Haglund's deformity (a prominent posterosuperior calcaneal tuberosity) is present, it is resected using an osteotome or burr to prevent mechanical impingement. If more than 50% of the tendon is debrided, augmentation with a flexor hallucis longus (FHL) tendon transfer is highly recommended to restore plantarflexion power and provide a robust vascular bed for healing.

Surgery for peroneal tendinopathy typically utilizes a retromalleolar approach. The sural nerve is identified and protected. The superior peroneal retinaculum (SPR) is incised, and the tendons are inspected. Longitudinal tears in the peroneus brevis are common; these are debrided and tubularized using a running non-absorbable suture. If the tendon is irreparably damaged, a tenodesis of the brevis to the intact peroneus longus is performed. The SPR must be meticulously repaired to prevent postoperative subluxation, often requiring osseous anchors into the fibula if the retinaculum is attenuated.
Ankle arthroscopy is performed using standard anteromedial and anterolateral portals. The anteromedial portal is established just medial to the tibialis anterior tendon, while the anterolateral portal is placed lateral to the peroneus tertius. Extreme caution must be exercised during the creation of the anterolateral portal to avoid iatrogenic injury to the superficial peroneal nerve (SPN). Transillumination and superficial dissection with a hemostat ("nick and spread" technique) are mandatory. Arthroscopy allows for excellent visualization of the joint for debridement of osteophytes, microfracture of osteochondral lesions, and synovectomy, with significantly reduced postoperative morbidity compared to open arthrotomy.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, ankle surgery carries a distinct profile of potential complications. The most dreaded complication following ankle arthrodesis is nonunion, with reported incidence rates ranging from 5% to 12% in the general population, but skyrocketing to over 30% in patients with uncontrolled diabetes, active tobacco use, or avascular necrosis of the talus. Nonunion typically presents as persistent pain with weight-bearing and progressive hardware failure (screw breakage or backing out). Salvage management requires a revision operation, removal of broken hardware, aggressive debridement of the fibrous nonunion, and stabilization with a more rigid construct, often an anterior locking plate or a TTC nail, supplemented with autologous bone graft or orthobiologics (e.g., BMP-2).
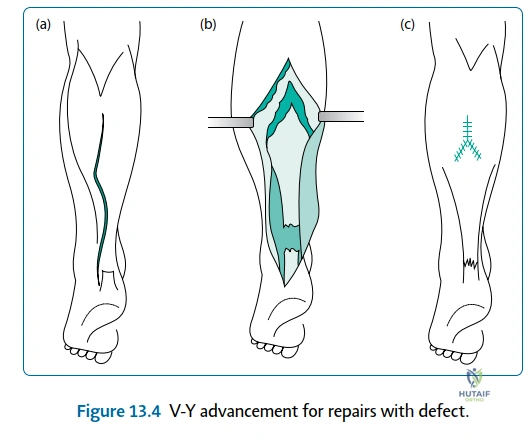
Wound complications are particularly prevalent in ankle surgery due to the thin soft tissue envelope. Anterior approaches to the ankle and posterior approaches for the Achilles tendon are at high risk for delayed healing, dehiscence, and superficial infection. The incidence of wound complications can approach 15% in high-risk cohorts. Superficial infections are managed with targeted oral antibiotics and local wound care. However, deep space infections involving the hardware or the joint space require emergent surgical irrigation and debridement, hardware retention if the construct is stable, and prolonged intravenous antibiotics. If the infection cannot be eradicated, hardware removal and placement of an antibiotic spacer may be necessary.
Adjacent segment disease is an inevitable long-term consequence of ankle arthrodesis. By eliminating the 0°-20° of dorsiflexion and 0°-45° of plantarflexion at the tibiotalar joint, immense stress is transferred to the subtalar and talonavicular joints. Up to 50% of patients will develop radiographic evidence of subtalar arthritis within 10 years of an ankle fusion, though not all will be symptomatic. When conservative measures fail, salvage management involves extending the fusion to include the subtalar joint (tibiotalocalcaneal arthrodesis).
Nerve injury is a significant risk, particularly to the superficial peroneal nerve during anterolateral portal placement or lateral approaches, and to the sural nerve during Achilles or peroneal tendon surgery. Neuromas can be highly debilitating. Management begins with desensitization therapy, gabapentinoids, and diagnostic blocks. Refractory neuromas may require surgical excision and burying of the proximal nerve stump into deep muscle or bone to prevent recurrence.
| Complication | Incidence Rate | Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Nonunion (Arthrodesis) | 5% - 12% (up to 30% in high-risk) | Smoking, diabetes, AVN, inadequate fixation, infection. | Revision fixation (plate/nail), autogenous bone grafting, orthobiologics, strict NWB. |
| Wound Dehiscence / Necrosis | 5% - 15% | Anterior/posterior incisions, vascular disease, smoking, tourniquet time. | Local wound care, negative pressure wound therapy (VAC), local rotational flaps (sural flap). |
| Deep Infection | 1% - 4% | Immunosuppression, prolonged operative time, prior surgery. | Emergent I&D, IV antibiotics, hardware removal if loose, potential amputation in severe cases. |
| Adjacent Segment Arthritis | 30% - 50% (at 10 years) | Malposition of fusion (varus/plantarflexion), high BMI. | NSAIDs, bracing, corticosteroid injections, extension of fusion (TTC arthrodesis). |
| Nerve Injury (Neuroma) | 2% - 7% | Retraction injury, aberrant anatomy (SPN, sural nerve). | Gabapentinoids, targeted nerve blocks, surgical excision and deep burial of proximal stump. |
Phased Post-Operative Rehabilitation Protocols
The postoperative care and rehabilitation following ankle surgery are as critical as the surgical execution itself. The overarching goal of the postoperative protocol is to protect the surgical repair or fusion site while mitigating the risks of deep vein thrombosis (DVT), muscle atrophy, and complex regional pain syndrome (CRPS). Rehabilitation is generally divided into four distinct phases, though the timeline varies significantly based on the specific procedure performed.
Phase 1: Maximum Protection (Weeks 0-2)
Immediately postoperatively, the patient is placed in a well-padded, bulky Jones splint or a short leg cast. The primary objectives during this phase are wound healing, edema control, and pain management. Strict non-weight-bearing (NWB) status is mandatory for arthrodesis, arthroplasty, and major tendon repairs. Patients are instructed to keep the operative limb elevated above the level of the heart for 23 hours a day to minimize swelling, which is the primary antagonist to wound healing. DVT prophylaxis, typically low-molecular-weight heparin or a direct oral anticoagulant, is initiated based on the patient's risk stratification. At the two-week mark, sutures are removed, and clinical wound healing is assessed.
Phase 2: Early Mobilization and Protected Weight Bearing (Weeks 2-6)
For patients undergoing ankle arthroscopy or simple debridement, this phase marks the transition to weight-bearing as tolerated in a controlled ankle motion (CAM) boot, with the initiation of active range of motion (AROM) exercises. However, for ankle arthrodesis and major tendon reconstructions, strict NWB status is maintained. The patient is transitioned from a splint to a rigid fiberglass cast or a locked CAM boot. For Achilles tendon repairs, the foot is typically immobilized in 15°-20° of plantarflexion to remove tension from the anastomosis. Isometric exercises of the proximal musculature (quadriceps, hamstrings, gluteals) are encouraged to prevent profound deconditioning.

Phase 3: Progressive Weight Bearing and Strengthening (Weeks 6-12)
At the six-week mark, weight-bearing radiographs are obtained for arthrodesis patients to assess for early trabecular consolidation across the fusion site. If clinical and radiographic signs of healing are present, the patient begins a progressive weight-bearing protocol in a CAM boot, advancing from 25% to 100% weight-bearing over 4 weeks. Physical therapy is formally initiated. For tendon repairs, the plantarflexion angle is gradually reduced to neutral. Therapy focuses on restoring proprioception, normalizing gait mechanics within the boot, and gentle concentric strengthening. Passive stretching of repaired tendons is strictly avoided to prevent elongation and subsequent weakness.
Phase 4: Return to Function and Advanced Rehabilitation (Months 3-6+)
Once solid clinical and radiographic union is achieved (typically 10-12 weeks for arthrodesis), or the tendon repair has matured, the patient is weaned out of the CAM boot into a supportive athletic shoe, often utilizing an ankle-foot orthosis (AFO) or a rigid lace-up brace for transitional support. Physical therapy intensifies, focusing on eccentric strengthening, advanced proprioceptive drills (BAPS board, single-leg stance), and work-specific or sport-specific functional training. Patients are counseled that maximal medical improvement (MMI) following complex ankle surgery often takes 12 to 18 months. Swelling after prolonged standing or activity is expected and managed with compression garments and elevation.
Summary of Landmark Literature and Clinical Guidelines
The evolution of ankle surgery and its associated postoperative care is deeply rooted in landmark orthopedic literature. The biomechanical imperative of the "golden position" for ankle arthrodesis was famously elucidated by Buck et al., who demonstrated that neutral dorsiflexion, slight valgus, and external rotation optimize the kinematics of the transverse tarsal joints and reduce the oxygen cost of walking. Deviation from this position, particularly into plantarflexion, exponentially increases stress on the midfoot, accelerating adjacent segment degeneration.
In the realm of joint preservation versus sacrifice, the work of Glazebrook and the Canadian Orthopaedic Foot and Ankle Society (COFAS) has provided critical insights. Their multicenter studies comparing ankle arthrodesis to total ankle arthroplasty have shown that while TAA provides superior functional scores and a more symmetric gait pattern in the short to medium term, arthrodesis remains the most durable and reliable procedure for pain relief, particularly in younger, high-demand patients. These findings heavily influence preoperative counseling and patient expectation management.
Regarding postoperative care, the American Orthopaedic Foot & Ankle Society (AOFAS) guidelines emphasize the critical nature of prolonged immobilization for arthrodesis and the careful, staged introduction of tension in tendon repairs. Recent literature has also strongly advocated for the use of early functional rehabilitation protocols following acute Achilles tendon ruptures, demonstrating that protected, early weight-bearing in a functional orthosis yields equivalent rerupture rates to traditional cast immobilization, but with superior early functional outcomes and earlier return to work. Furthermore, the implementation of standardized DVT prophylaxis protocols in foot and ankle surgery, guided by the Caprini risk assessment model,
Clinical & Radiographic Imaging Archive
