Mastering Distal Femoral Replacement in Revision TKA: An Intraoperative Guide

Key Takeaway
This masterclass provides an exhaustive, real-time guide to distal femoral replacement in revision total knee arthroplasty. We'll navigate complex bone loss scenarios, emphasizing meticulous surgical anatomy, precise intraoperative techniques, and critical decision-making. Fellows will gain insights into advanced reconstruction strategies, from augments to bulk allografts, ensuring optimal outcomes for challenging revision cases.
Comprehensive Introduction and Patho-Epidemiology
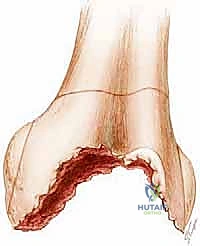
The management of massive distal femoral bone loss in the setting of revision total knee arthroplasty (TKA) represents one of the most formidable challenges in adult reconstructive orthopedics. As the aggregate volume of primary TKA procedures continues to rise globally, a proportional and inevitable increase in the revision burden follows. We are no longer merely addressing isolated polyethylene wear or aseptic loosening with well-preserved host bone; contemporary revision arthroplasty frequently entails catastrophic structural failure. This necessitates a transition from standard revision systems to complex reconstructive paradigms, including Distal Femoral Replacement (DFR). If left untreated, the continued generation of particulate debris and the micromotion between loose components and the host bone will precipitate escalating, irreversible osteolysis, culminating in complete loss of the metaphyseal and diaphyseal structural integrity.
The pathogenesis of severe distal femoral bone loss is multifactorial, driven by a combination of mechanical insult, biologic response, and iatrogenic factors during index implant extraction. Bone loss is nearly unavoidable during the explantation of a failed femoral component. The extraction of previous implants, whether fixed via polymethylmethacrylate (PMMA) cement or porous biological ingrowth, demands meticulous dissection at the implant-bone interface. Even with the judicious use of microsaws, flexible osteotomes, and ultrasonic extraction tools, the space-occupying nature of these instruments inherently incurs a finite volumetric loss of host bone. Aggressive extraction without establishing a clear, circumferential plane between the metal and the bone can lead to catastrophic avulsion of one or both femoral condyles—an intraoperative pitfall that immediately escalates the complexity of the reconstruction. Furthermore, correcting the malrotation of a previously implanted femoral component will obligatorily result in further bone sacrifice anteriorly and posteriorly as the new component is reoriented to the true epicondylar axis.
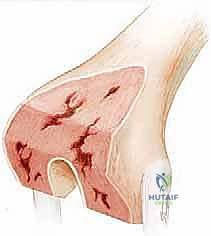
Beyond the mechanical trauma of extraction, the biological environment of a failed TKA plays a dominant role in bone attrition. Stress-shielding of the periprosthetic femur, a predictable consequence of rigid intramedullary or massive metaphyseal implant loading, leads to profound regional osteopenia. This is frequently compounded by macrophage-mediated osteolysis secondary to wear debris particles (polyethylene, metal, or cement). This insidious biological cascade generates expansive cavitary and segmental lesions that completely undermine the structural columns of the distal femur. Preoperative plain radiographs, while foundational to our diagnostic workup, notoriously underestimate the true three-dimensional extent of this osteolysis.
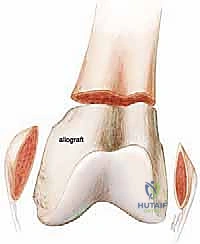
Consequently, the reconstructive surgeon must invariably prepare for a worst-case scenario. When the metaphyseal host bone is insufficient to support standard revision stems and metaphyseal cones or sleeves—typically corresponding to Anderson Orthopaedic Research Institute (AORI) Type III defects—the paradigm shifts toward structural allografts or modular mega-prostheses. Severe distal femoral bone loss, if inadequately addressed with under-sized or under-supported implants, will inevitably lead to early mechanical failure, subsidence, gross varus/valgus instability, and potentially catastrophic periprosthetic fracture. Our ultimate objective is to bypass this compromised bone, achieve rigid diaphyseal fixation, restore the anatomical joint line, and provide a durable, functional construct for the patient.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the distal femoral anatomy and its intricate relationship with the surrounding neurovascular structures and musculature is non-negotiable for safe and effective revision surgery. The osteology of the metaphyseal femur is characterized by its fluted geometry and cancellous architecture, which, in a primary setting, provides an excellent environment for implant fixation. However, in the setting of a massive revision, this cancellous bed is frequently obliterated. The medial and lateral epicondyles remain our most critical osseous landmarks. The surgical transepicondylar axis dictates the rotational alignment of the femoral component, while the epicondyles themselves serve as the origins for the medial collateral ligament (MCL) and the lateral collateral ligament (LCL)/popliteus complex. In DFR, these epicondyles are often resected or rendered incompetent, mandating the use of a rotating hinge construct to substitute for the lost collateral stability.

Understanding the muscular intervals and attachments is critical for both exposure and postoperative function. The primary approach relies on a medial parapatellar arthrotomy, navigating the quadriceps femoris complex. Mobilizing the extensor mechanism in a multiply operated knee with severe arthrofibrosis requires meticulous technique to avoid patellar tendon avulsion. The adductor magnus insertion at the adductor tubercle is a reliable landmark for approximating the joint line when the epicondyles are distorted. Posteriorly, the medial and lateral heads of the gastrocnemius originate from the posterior aspects of the femoral condyles. During DFR, these origins are typically detached, which can lead to a dead space posteriorly and necessitates careful soft tissue management to prevent hematoma formation and protect the neurovascular bundle.
Neurovascular vigilance must be absolute during these extensive reconstructions. The femoral artery and vein transition to the popliteal artery and vein as they traverse the adductor hiatus, coming to lie directly posterior to the distal femur and posterior capsule. Extensive posterior dissection, aggressive curettage of posterior osteophytes, or the use of oscillating saws in the posterior compartment are high-risk maneuvers. The sciatic nerve, while generally proximal, and its terminal branches (particularly the common peroneal nerve) are at risk during aggressive retraction or when correcting severe valgus deformities. The peroneal nerve is highly sensitive to stretch; thus, restoring the joint line and correcting alignment must be done with careful consideration of nerve tension.

From a biomechanical perspective, a distal femoral replacement fundamentally alters the load-transfer mechanism of the lower extremity. Standard condylar implants transfer load through the metaphyseal bone. In contrast, a DFR bypasses the metaphysis entirely, transferring axial, torsional, and bending forces directly to the femoral diaphysis via the intramedullary stem. This creates a significant stress riser at the host-implant junction, predisposing the patient to periprosthetic fractures. Furthermore, because the collateral ligaments are typically sacrificed or incompetent, the implant relies on a rotating hinge mechanism. This hinge must dissipate torsional forces to protect the diaphyseal fixation; a fixed hinge would rapidly transmit these forces to the cement-bone interface, leading to premature aseptic loosening.
Exhaustive Indications and Contraindications
The decision to proceed with a Distal Femoral Replacement in a non-oncologic setting is complex and should be reserved for scenarios where traditional reconstructive techniques are unfeasible. The primary indication is an AORI Type III defect of the distal femur, characterized by massive, uncontained segmental bone loss that precludes the stable fixation of a revision femoral component, even with the addition of metaphyseal cones, sleeves, or custom augments. This degree of bone loss is frequently encountered in the setting of multiple prior revisions, severe stress shielding, or massive osteolysis secondary to polyethylene wear.

Another major indication is the management of complex periprosthetic distal femoral fractures, specifically highly comminuted Vancouver Type B3 fractures in the elderly, osteoporotic patient. In these cases, attempting internal fixation or standard revision is often fraught with a high risk of nonunion or construct failure. DFR allows for immediate weight-bearing and rapid mobilization, which is critical for minimizing morbidity and mortality in the geriatric population. Additionally, DFR is indicated in cases of profound collateral ligament incompetence combined with significant bone loss, where a rotating hinge knee is mandatory, but the remaining metaphyseal bone cannot support the bulky housing of the hinge mechanism.
Despite its utility as a salvage procedure, DFR carries strict contraindications. The most absolute contraindication is the presence of an active, uncontrolled periprosthetic joint infection (PJI). Implanting a massive mega-prosthesis in a contaminated bed guarantees failure. Such cases mandate a two-stage approach: aggressive debridement, placement of an articulating or static antibiotic-loaded cement spacer, and a prolonged course of targeted intravenous antibiotics prior to definitive DFR. Relative contraindications include a severely compromised soft tissue envelope that cannot provide adequate coverage for the massive implant, requiring preliminary or concurrent plastic surgery intervention (e.g., gastrocnemius flap).
Furthermore, patients who are medically unfit to tolerate a prolonged surgical procedure with significant potential for blood loss should be carefully evaluated. In some instances, a permanent antibiotic spacer or above-knee amputation may be the more prudent, life-saving choice. The table below outlines the specific indications and contraindications for DFR in revision TKA.
| Category | Specific Condition | Rationale / Clinical Context |
|---|---|---|
| Indications | AORI Type III Femoral Defect | Metaphyseal bone is insufficient for cone/sleeve fixation. |
| Vancouver B3 Periprosthetic Fracture | Comminuted fracture with loose implant and poor bone stock. | |
| Massive Osteolysis / Stress Shielding | Uncontained defects precluding standard augment use. | |
| Severe Ligamentous Incompetence | Requires a hinged construct; bone cannot support hinge housing. | |
| Post-Tumor Resection | Primary indication in orthopedic oncology. | |
| Contraindications | Active Periprosthetic Joint Infection | High risk of persistent infection; requires 2-stage revision. |
| Inadequate Soft Tissue Envelope | High risk of wound breakdown and secondary infection. | |
| Severe Neuropathic Joint (Charcot) | High risk of mechanical failure and dislocation. | |
| Medically Unstable Patient | Cannot tolerate prolonged surgery or massive blood loss. | |
| Young, High-Demand Patient (Relative) | High likelihood of eventual aseptic loosening and mechanical failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Flawless execution of a complex distal femoral replacement hinges entirely on exhaustive preoperative planning. The diagnostic workup must begin with high-quality, comprehensively positioned radiographs. True lateral views of the knee, obtained at exactly 90 degrees of knee flexion, are paramount for assessing the anterior and posterior condylar bone stock and the position of the existing implant. Full-length, weight-bearing hip-to-ankle radiographs are mandatory to assess the overall mechanical axis, identify any extra-articular deformities, and evaluate the diaphyseal bowing of the femur, which will dictate the radius of curvature required for the long intramedullary stem.
Advanced imaging modalities are frequently required. Computed Tomography (CT) scans utilizing Metal Artifact Reduction Sequences (MARS) provide an invaluable three-dimensional map of the osteolysis and remaining host bone. This allows the surgeon to accurately classify the defect and determine exactly where the viable diaphyseal bone begins. Concurrently, the exclusion of deep periprosthetic joint infection is non-negotiable. The diagnostic algorithm must include serum inflammatory markers (ESR, CRP), and an image-guided joint aspiration for synovial fluid cell count, differential, alpha-defensin, and aerobic/anaerobic/fungal/AFB cultures. Any suspicion of infection mandates a staged approach.
Templating is a rigorous exercise in anticipating the reconstruction. Using digital templating software, the surgeon must estimate the level of the required femoral resection, the diameter and length of the diaphyseal stem required for rigid fixation (aiming for at least 2 cortical diameters of diaphyseal engagement), and the size of the segmental augments needed to restore the leg length. It is critical to plan for the restoration of the joint line, which is typically located 25-30 mm distal to the adductor tubercle or 10-15 mm proximal to the fibular head. The surgical team must coordinate with implant representatives to ensure that a comprehensive modular mega-prosthesis system, including various stem lengths, diameters, and segmental body sizes, is available in the operating theater.
Patient positioning sets the stage for intraoperative success. The patient is placed supine on a radiolucent operating table to facilitate intraoperative fluoroscopy. A firm bump is placed under the ipsilateral hemipelvis to prevent external rotation of the limb, ensuring the patella points directly toward the ceiling. A rigid leg-holding device, such as a Stulberg footrest, is utilized to meticulously control knee flexion and extension throughout the procedure, which is vital for exposure and assessing gap kinematics. While some surgeons utilize a proximal thigh tourniquet, many experienced revision surgeons prefer to operate without one. Avoiding a tourniquet allows for continuous assessment of tissue perfusion, minimizes ischemic damage to already compromised soft tissues, and permits dynamic evaluation of hemostasis prior to closure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach must be carefully planned to navigate existing scar tissue while maximizing exposure. When faced with multiple previous incisions, the most laterally based viable incision is generally preferred to preserve the vascular supply to the anterior skin flap. A standard medial parapatellar arthrotomy is the workhorse approach. However, in the setting of severe arthrofibrosis or patella baja, extensile measures must be anticipated. A quadriceps snip is a highly effective, low-morbidity extension. If further exposure is required, a tibial tubercle osteotomy (TTO) provides unparalleled access to the diaphysis while protecting the patellar tendon; however, it requires meticulous repair and alters postoperative weight-bearing protocols. Crucially, patellar eversion should be strictly avoided to prevent avulsion of the extensor mechanism; lateral subluxation is preferred.
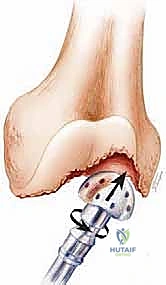
Implant extraction is the most perilous phase of the procedure. The interface between the failed component and the host bone must be systematically disrupted. Flexible osteotomes, pencil burrs, and ultrasonic extraction devices are utilized to break the cement mantle or disrupt porous ingrowth. The surgeon must resist the temptation to lever the implant out prematurely, as this will inevitably result in catastrophic condylar avulsion. Once the femoral component is removed, the true extent of the osseous defect is revealed. Radical debridement of all necrotic bone, fibrous tissue, and residual PMMA is performed until healthy, bleeding cortical bone is encountered.
Preparation of the host bone begins with identifying the true anatomical axis of the femur. Progressive flexible or rigid reaming is performed up the femoral canal to determine the appropriate stem diameter. The level of the femoral resection is then determined based on preoperative templating and intraoperative assessment of bone viability. A transverse cut is made through the diaphysis in healthy cortical bone. It is imperative to meticulously measure the distance from the resected bone edge to the native joint line (referencing the adductor tubercle, fibular head, or inferior pole of the patella) to accurately select the modular segmental components and restore equal leg lengths.
Trialing is an iterative and exacting process. The trial stem, segmental body, and hinge mechanism are assembled and inserted. The surgeon must assess the stability of the construct, the restoration of leg length, and the kinematics of the knee. Because the collateral ligaments are absent, gap balancing is less about soft tissue releases and more about selecting the appropriate polyethylene bearing thickness and hinge bumper to prevent hyperextension and ensure smooth tracking. Once the trials are finalized, the definitive implant is assembled on the back table. Fixation of the diaphyseal stem can be achieved via cemented or cementless techniques. Cemented stems provide immediate fixation and allow for the delivery of local antibiotics, while fully porous-coated cementless stems offer the potential for long-term biologic fixation, provided there is a tight diaphyseal scratch fit.

Complications, Incidence Rates, and Salvage Management
Distal femoral replacement in the setting of revision TKA is inherently a salvage procedure, and surgeons must counsel patients extensively regarding the high complication profile. The magnitude of the surgery, combined with the compromised local biology and the biomechanical demands placed on the mega-prosthesis, results in a complication rate that significantly eclipses that of standard revision arthroplasty. The most devastating and frequent complication is Periprosthetic Joint Infection (PJI). The extensive dead space, prolonged operative time, and poor soft tissue envelope create an ideal environment for bacterial colonization. Management of PJI in a DFR is incredibly challenging; while acute infections may occasionally be salvaged with Debridement, Antibiotics, and Implant Retention (DAIR), chronic infections almost universally require a grueling two-stage revision or, in cases of severe bone loss and soft tissue compromise, an above-knee amputation.
Aseptic loosening and mechanical failure represent the second major category of complications. The rotating hinge mechanism, while necessary to dissipate torsional forces, is subject to significant wear. Bushing wear and axle failure can occur over time, leading to instability and metallosis. Furthermore, the massive stress riser at the junction of the rigid intramedullary stem and the host diaphyseal bone predisposes the patient to periprosthetic fractures. If a fracture occurs at the tip of the stem, it often necessitates an even more extensive revision with total femoral replacement. Stem subsidence can also occur, particularly with cementless designs if initial rigid fixation is not achieved.
Extensor mechanism complications are also disproportionately common. The multiple prior surgeries, combined with the extensive exposure required for DFR, place the patellar tendon and quadriceps tendon at high risk for rupture. An extensor mechanism disruption in the presence of a DFR is a catastrophic event that severely limits ambulation. Salvage options include reconstruction with synthetic mesh (e.g., Marlex mesh) or a complete extensor mechanism allograft, though both techniques have high failure rates. The table below summarizes the most common complications, their approximate incidence rates based on current literature, and standard salvage management strategies.
| Complication | Approximate Incidence | Salvage Management Strategy |
|---|---|---|
| Periprosthetic Joint Infection (PJI) | 10% - 20% | DAIR (acute); 2-Stage Revision with spacer; Suppressive antibiotics; Amputation (severe cases). |
| Aseptic Loosening / Stem Subsidence | 5% - 12% | Revision to a longer/thicker stem; Impaction grafting; Conversion to Total Femoral Replacement. |
| Periprosthetic Fracture | 4% - 8% | Open Reduction Internal Fixation (ORIF) with cables/plates; Revision to longer stem bypassing fracture. |
| Extensor Mechanism Failure | 5% - 10% | Marlex mesh reconstruction; Extensor mechanism allograft; Gastrocnemius flap for coverage. |
| Hinge Mechanism Failure / Bushing Wear | 3% - 7% | Modular exchange of polyethylene bushings and axle; Revision of hinge housing if damaged. |
| Wound Necrosis / Dehiscence | 5% - 15% | Negative pressure wound therapy; Surgical debridement; Medial/Lateral gastrocnemius rotational flaps. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a distal femoral replacement must be meticulously phased and customized to the specific intraoperative findings, particularly the method of stem fixation and the integrity of the extensor mechanism. Unlike primary TKA, where rapid and aggressive mobilization is the universal standard, DFR rehabilitation requires a delicate balance between preventing arthrofibrosis and protecting the massive reconstructive construct and vulnerable soft tissues.

In the immediate postoperative phase (Days 0 to 14), the primary goals are wound healing, deep vein thrombosis (DVT) prophylaxis, and early, safe mobilization. If a cemented diaphyseal stem was utilized and the extensor mechanism remains intact, patients are generally allowed weight-bearing as tolerated (WBAT) with an assistive device. However, if a cementless, diaphyseal-engaging stem was used, the surgeon may elect to restrict weight-bearing (e.g., toe-touch weight-bearing) for 6 weeks to facilitate biologic osteointegration. Range of motion (ROM) exercises are initiated immediately, typically utilizing continuous passive motion (CPM) machines or active-assisted techniques, aiming for 0 to 90 degrees of flexion before hospital discharge. If a tibial tubercle osteotomy or extensor mechanism repair was performed, the knee is locked in extension in a hinged brace for ambulation, and flexion is strictly limited and gradually advanced over 6 to 8 weeks.
The intermediate phase (Weeks 2 to 6) focuses on progressive strengthening and improving gait mechanics. Physical therapy emphasizes quadriceps activation, straight leg raises, and closed-chain exercises, provided there are no extensor mechanism precautions. Because the rotating hinge implant provides inherent coronal and sagittal stability, therapy can focus more on functional mobility rather than proprioceptive ligamentous retraining. Patients are transitioned from a walker to a cane as their balance and strength improve. Pain management and swelling control remain critical during this phase to allow for effective participation in physical therapy.
The late phase (Weeks 6 to 12 and beyond) aims to maximize the functional outcome and return the patient to activities of daily living (ADLs). Advanced strengthening, stationary cycling, and aquatic therapy are highly beneficial. It is imperative that the surgeon and physical therapist set realistic expectations for the patient. A knee with a DFR will never feel or function like a native knee or even a well-functioning primary TKA. Patients must be permanently counseled to avoid high-impact activities, running, jumping, and heavy lifting, as these activities will exponentially accelerate bushing wear and increase the risk of aseptic loosening or periprosthetic fracture. Lifelong clinical and radiographic surveillance is mandatory.
Summary of Landmark Literature and Clinical Guidelines
The evolution of Distal Femoral Replacement from a niche procedure in orthopedic oncology to a vital tool in the armamentarium of the revision arthroplasty surgeon is well-documented in the orthopedic literature. Historically, mega-prostheses were reserved exclusively for limb salvage following tumor resection. However, as the complexity of non-oncologic revisions increased, pioneers began adapting these massive implants for severe bone loss. Landmark studies by Springer et al. and Berend et al. in the early 2000s demonstrated that while DFR in non-oncologic revision TKA carried a higher complication rate than standard revisions, it offered a viable, limb-saving alternative to amputation, with acceptable mid-term survivorship.
Current clinical guidelines emphasize the critical distinction between fixed-hinge and rotating-hinge designs. Early fixed-hinge implants were plagued by catastrophic aseptic loosening because they rigidly transmitted all torsional forces to the cement-bone interface. The universal adoption of the rotating-hinge concept, which allows
