Orthopedic Prometric MCQs - Chapter 3 Part 46

Orthopedic Prometric MCQs - Chapter 3 Part 46
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
When using the tibial external rotation test on a patient, increased external rotation at 30° and 90° of knee flexion is indicative of:
Explanation
Question 2
The recommended treatment for an acute combined anterior cruciate ligament and complete posterolateral corner disruption in a young athlete is:
Explanation
Question 3
The ideal timing for repair of an acute posterolateral corner knee injury is:
Explanation
Question 4
Which of the following exercises must be delayed for up to 3 months after posterolateral corner repair or reconstruction of the knee:
Explanation
Question 5
For patients who sustain a knee dislocation, the role of clinical history, physical examination, and magnetic resonance imaging (MRI) is:
Explanation
Question 6
After high velocity knee dislocations, there is serious injury to the popliteal vessels in approximately what percentage of patients:
Explanation
Question 7
After high velocity knee dislocations, there is serious injury to the peroneal nerve in approximately what percentage of patients:
Explanation
Question 8
The strongest bundle in the posterior cruciate ligament is the:
Explanation
Question 9
In the posterior cruciate ligament the anterolateral bundle is tight in __ and the posteromedial bundle is tight in ____:
Explanation
Question 10
When applying valgus stress, over which arc of motion is the anterior band of the anterior oblique component of the ulnar collateral ligament of the elbow under tension:
Explanation
Question 11
When applying valgus stress, over which arc of motion is the posterior band of the anterior oblique component of the ulnar collateral ligament of the elbow under tension:
Explanation
Question 12
Which of the following structures is the main stabilizer of the elbow to valgus stress:
Explanation
Question 13
Disruption of which of the following ligaments represents the primary lesion in posterolateral rotatory instability of the elbow:
Explanation
Question 14
Elbow injury usually occurs during which phase of throwing:
Explanation
Question 15
Which of the following structures is the most important dynamic stabilizer of the elbow to valgus stresses during throwing:
Explanation
Question 16
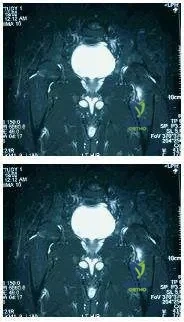
The following is a hip magnetic resonance image (MRI) of a 28-year-old male triathlete who has noticed progressive activityrelated left hip pain. Recommended treatment includes:

Explanation
Question 17
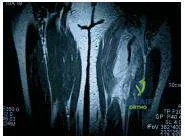
The following radiographs are of a 19-year-old female collegiate distance runner who complained of pain in her right distal tibia. She reports having shin splints 2 years earlier that affected her right proximal tibia. She has been unable to run secondary to symptoms for 3 weeks. She reports being amenorrheic for approximately the last 3 years. Which of the following should be included in her initial treatment regimen:
Explanation
Question 18
The following figure is the magnetic resonance image (MRI) of a 40-year- old avid female water-skier who felt a pop in her left hip as she was pulled over the front of her ski. Recommended treatment includes:
Explanation
Question 19
During which phase of throwing is the flexor-pronator muscle mass most electrically active:
Explanation
Question 20
Which of the following is a risk factor for anterior cruciate ligament (AC L) injury in noncontact athletes:
Explanation
Question 21
Which of the following structures constitute the primary static stabilizers of the posterolateral corner (PLC) of the knee?
Explanation
Question 22
During the tibial external rotation (dial) test, a patient exhibits 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side, but normal external rotation at 90 degrees. This finding is most indicative of an isolated injury to which of the following?
Explanation
Question 23
A 22-year-old athlete undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Which of the following is the most frequently reported complication associated with this specific graft choice?
Explanation
Question 24
Which of the following clinical tests is most specific for diagnosing a posterolateral corner (PLC) deficiency in the knee?
Explanation
Question 25
A 30-year-old male presents after a high-energy dashboard injury resulting in a knee dislocation that spontaneously reduced. His pedal pulses are palpable. What is the most appropriate initial screening tool to evaluate for an occult popliteal artery injury?
Explanation
Question 26
The posterior cruciate ligament (PCL) consists of two main functional bundles. Which of the following statements regarding the anterolateral (AL) bundle is correct?
Explanation
Question 27
A 25-year-old soccer player sustains an acute combined Grade III femoral-sided medial collateral ligament (MCL) tear and an anterior cruciate ligament (ACL) rupture. What is the most widely accepted treatment strategy for this injury pattern?
Explanation
Question 28
A 28-year-old skier presents with a swollen knee after a twisting fall. Radiographs demonstrate a small avulsion fracture of the lateral tibial plateau.
This radiographic finding (Segond fracture) is virtually pathognomonic for an injury to which of the following structures?
Explanation
Question 29
A 10-year-old boy falls from his bicycle and sustains a Meyers and McKeever Type III tibial eminence fracture. What is the most appropriate definitive management?
Explanation
Question 30
Which of the following arteries provides the primary blood supply to the anterior cruciate ligament (ACL)?
Explanation
Question 31
During the evaluation of a patient with a suspected knee ligament injury, the quadriceps active test is performed. The knee is flexed to 90 degrees, and the patient is asked to slide their foot forward against resistance. An anterior shift of the tibia is noted. This finding indicates a deficiency of the:
Explanation
Question 32
A 24-year-old male sustains a traumatic knee dislocation resulting in a combined ACL, PCL, and posterolateral corner (PLC) injury. He is noted to have foot drop on the affected side. Injury to which of the following nerves is most likely?
Explanation
Question 33
In the posteromedial corner of the knee, which structure serves as the primary restraint to valgus stress and internal rotation when the knee is near full extension?
Explanation
Question 34
A clinical examination of a knee shows increased external rotation of the tibia at 30 degrees of flexion that normalizes at 90 degrees.
To reconstruct the primary deficient structures in this specific injury pattern, grafts should be routed to replicate the functions of which anatomical structures?
Explanation
Question 35
A 35-year-old man presents with chronic medial knee pain months after a valgus injury. Radiographs reveal a linear calcification adjacent to the medial femoral condyle. What is the eponymous name for this radiographic sign?
Explanation
Question 36
While femoral-sided Grade III MCL tears are typically managed nonoperatively when combined with an ACL tear, a tibial-sided Grade III MCL avulsion requires surgical repair. Why is operative intervention specifically indicated for this variant?
Explanation
Question 37
According to the Schenck classification of knee dislocations (KD), a patient who sustains tears to both the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL), with intact collateral ligaments, is classified as:
Explanation
Question 38
A patient presents with a knee injury. The dial test shows >10 degrees of external rotation asymmetry at 30 degrees of knee flexion, but symmetric rotation at 90 degrees. Which structure is most likely injured?
Explanation
Question 39
In evaluating a patient with a suspected posterolateral corner injury, the reverse pivot shift test is performed. During the test, a clunk is felt as the knee is brought from flexion into extension. This clunk represents:
Explanation
Question 40
A 35-year-old male presents with chronic posterolateral knee instability and varus malalignment following an old injury. He is scheduled for a posterolateral corner (PLC) reconstruction. What is the most appropriate initial surgical management?
Explanation
Question 41
Which of the following nerves is most frequently injured in the setting of a severe posterolateral corner (PLC) injury or knee dislocation?
Explanation
Question 42
A patient suffers a high-velocity knee dislocation. Following closed reduction, the Ankle-Brachial Index (ABI) is measured at 0.85. What is the next best step in management?
Explanation
Question 43
A 25-year-old athlete sustains a valgus blow to the knee. MRI reveals a complete rupture of the superficial and deep medial collateral ligament (MCL) with the distal end of the superficial MCL displaced superficial to the pes anserinus. What is the recommended treatment?
Explanation
Question 44
When reconstructing the anterior cruciate ligament (ACL), the surgeon must identify the lateral intercondylar ridge (resident's ridge). What is the anatomical relationship of the native ACL footprint to this ridge?
Explanation
Question 45
What is the primary restraint to posterior tibial translation at 90 degrees of knee flexion?
Explanation
Question 46
A patient presents with a chronic grade III isolated PCL injury treated non-operatively 15 years ago. Which compartments of the knee are at the highest risk for developing secondary osteoarthritis?
Explanation
Question 47
During a physical examination for a suspected knee ligament injury, the examiner actively flexes the patient's quadriceps while the knee is held at 90 degrees of flexion. The tibia is observed to translate anteriorly. This finding is pathognomonic for an injury to which structure?
Explanation
Question 48
Which of the following anatomical structures forms the primary static restraint to varus opening at 0 and 30 degrees of knee flexion?
Explanation
Question 49
A 22-year-old football player sustains a Schenck KD-III knee dislocation. To minimize the risk of compartment syndrome from fluid extravasation during arthroscopic multiligamentous reconstruction, what is the generally recommended optimal timing for surgery if no vascular injury is present?
Explanation
Question 50
The meniscofemoral ligaments of the knee are intimately associated with the posterior cruciate ligament (PCL). Which of the following correctly describes their anatomical relationship?
Explanation
Question 51
A 45-year-old female presents with chronic medial knee pain. Radiographs reveal a calcification near the medial femoral epicondyle.
What is the eponymous name for this radiographic finding?
Explanation
Question 52
During a posterolateral corner (PLC) reconstruction using an anatomical technique (e.g., LaPrade), three main structures are reconstructed. Which of the following is NOT one of the three primarily reconstructed structures?
Explanation
Question 53
An isolated posterolateral corner injury is diagnosed. Which physical exam finding would most accurately differentiate an isolated PLC injury from a combined PLC and PCL injury?
Explanation
Question 54
A patient sustains an avulsion fracture of the anterolateral proximal tibia.
This finding is considered pathognomonic for a tear of which major knee ligament?
Explanation
Question 55
The superficial medial collateral ligament (sMCL) has distinct femoral and tibial attachments. Where is its primary distal (tibial) attachment located?
Explanation
Question 56
A patient is evaluated for a knee dislocation. Which specific knee dislocation classification implies a tear of the anterior cruciate ligament, posterior cruciate ligament, and medial collateral ligament, while the posterolateral corner remains intact?
Explanation
Question 57
A 30-year-old male undergoes a single-bundle anterior cruciate ligament (ACL) reconstruction. To optimally control both anterior translation and rotational instability, where is the most appropriate location for the femoral tunnel within the native footprint?
Explanation
Question 58
A 25-year-old male is brought to the emergency department after a high-speed motorcycle accident. Clinical examination reveals a grossly deformed knee that is reduced under sedation. Post-reduction Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 59
Which of the following structures form the primary static stabilizing complex of the posterolateral corner (PLC) of the knee?
Explanation
Question 60
During physical examination of a patient with a suspected multiligamentous knee injury, the dial test reveals 15 degrees of increased external tibial rotation compared to the contralateral side at 30 degrees of knee flexion. At 90 degrees of flexion, the side-to-side difference in external rotation is 2 degrees. What is the most likely injury pattern?
Explanation
Question 61
A patient sustains a high-energy knee dislocation. On examination, there is a transverse skin furrow (dimple sign) over the medial joint line, and the knee cannot be closed-reduced. What structure is most likely interposing and preventing reduction?
Explanation
Question 62
The posterior cruciate ligament (PCL) consists of two main functional bundles. Which statement best describes the biomechanical properties of the anterolateral (AL) bundle?
Explanation
Question 63
Review the radiograph demonstrating a small cortical avulsion fracture from the medial aspect of the proximal tibia (Reverse Segond fracture).
This radiographic finding is virtually pathognomonic for which of the following combined injuries?
Explanation
Question 64
During surgical reconstruction of the posterolateral corner (PLC) using a fibular-based technique, a surgeon must be extremely careful to protect the common peroneal nerve. Where is this nerve most vulnerable during the approach?
Explanation
Question 65
According to the Schenck classification of knee dislocations, a patient with an MRI confirming complete tears of the ACL, PCL, and the posterolateral corner (PLC), with an intact medial collateral ligament (MCL), is classified as:
Explanation
Question 66
A 28-year-old male presents with recurrent instability 2 years after an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Clinical examination reveals an intact ACL graft on Lachman testing but significant varus thrust during gait and a positive reverse pivot shift. Failure to address which of the following at the index procedure most likely caused this outcome?
Explanation
Question 67
A 22-year-old collegiate football player sustains an acute combined grade III anterior cruciate ligament (ACL) tear and grade III medial collateral ligament (MCL) tear. Assuming non-operative treatment of the MCL is chosen, what is the most widely accepted management strategy?
Explanation
Question 68
The posteromedial corner of the knee provides primary restraint against valgus forces in full extension and anteromedial rotatory instability. Which of the following structures is the most crucial static component of this complex?
Explanation
Question 69
Which type of knee dislocation is most strongly associated with a stretch or complete rupture injury to the common peroneal nerve?
Explanation
Question 70
During normal knee kinematics, the popliteus muscle plays a vital role in initiating knee flexion from a fully extended position. What is its primary biomechanical action during this phase?
Explanation
Question 71
An isolated rupture of the posterolateral corner (PLC) is suspected in a 25-year-old athlete. During the Dial test, what are the expected physical examination findings that differentiate an isolated PLC injury from a combined PLC and posterior cruciate ligament (PCL) injury?
Explanation
Question 72
Which of the following anatomic structures is considered the primary restraint to varus opening at 30 degrees of knee flexion?
Explanation
Question 73
A 25-year-old athlete sustains an acute traumatic knee dislocation. In the emergency department, the Ankle-Brachial Index (ABI) is measured at 0.8. A CTA confirms a popliteal artery intimal tear. The vascular surgeon repairs the artery via a posterior approach. What is the most appropriate next orthopedic step?
Explanation
Question 74
What is the primary anatomical and biomechanical rationale for utilizing a tibial inlay technique over a standard transtibial technique during posterior cruciate ligament (PCL) reconstruction?
Explanation
Question 75
Which of the following physical examination tests is most specific for evaluating posterolateral corner (PLC) rotatory instability?
Explanation
Question 76
A 35-year-old patient presents with a chronic posterolateral corner (PLC) deficiency and a noticeable varus thrust during gait. Radiographs show medial compartment narrowing and significant mechanical varus alignment. What is the most appropriate initial surgical management?
Explanation
Question 77
A 28-year-old football player presents with acute knee pain and lateral swelling after a direct blow to the anteromedial tibia. A radiograph is obtained.
Based on the classical significance of the "arcuate sign" shown, what associated structural injury is almost certainly present?
Explanation
Question 78
During a single-bundle posterior cruciate ligament (PCL) reconstruction, which specific bundle is typically reconstructed, and at what angle of knee flexion should the graft be tensioned?
Explanation
Question 79
A patient is diagnosed with a grade III MCL tear combined with an ACL rupture. MRI reveals the distal MCL has avulsed from its tibial insertion and retracted superficial to the pes anserinus (Stener-like lesion of the knee). What is the recommended management strategy?
Explanation
Question 80
Which neurological structure is at highest risk during an acute posterolateral corner injury, and what specific clinical finding dictates the poorest prognosis for conservative recovery?
Explanation
Question 81
A 22-year-old female skier presents after a twisting knee injury. Radiographs reveal the finding shown.
This classical fracture (Segond fracture) represents an avulsion of which structure and strongly correlates with which associated injury?
Explanation
Question 82
When performing an anatomical posterolateral corner (PLC) reconstruction, at what knee position should the fibular collateral ligament (FCL) graft be properly tensioned?
Explanation
Question 83
The popliteofibular ligament (PFL) plays a crucial role in posterolateral knee stability. Which of the following best describes its primary anatomical origin and insertion?
Explanation
Question 84
A 40-year-old male presents with a suspected posterior cruciate ligament (PCL) injury. On examination, a positive posterior sag sign is noted. Which radiographic view is most accurate for quantifying the exact degree of posterior tibial translation?
Explanation
Question 85
A 50-year-old patient presents with acute posteromedial knee pain after deep flexion. MRI demonstrates the lesion shown.
If left untreated, a complete posterior horn medial meniscal root tear is biomechanically equivalent to which of the following?
Explanation
Question 86
During an anatomical posterolateral corner (PLC) reconstruction, tunnels must be placed accurately in the lateral femoral condyle. What is the spatial relationship of the normal fibular collateral ligament (FCL) femoral attachment relative to the popliteus tendon attachment?
Explanation
None
